
Abstract
Rural youth suicide represents a major source of mental health inequity in the United States (US). School-based suicide prevention programs may provide an effective avenue to address this mental health crisis among rural youth. This study’s primary goal is to demonstrate the feasibility and acceptability of a novel implementation approach (utilizing teachers from a neighboring school) for delivering the Youth Aware of Mental Health (YAM) program, an evidence-based, universal youth suicide prevention curriculum, to high school students in rural Montana. We will recruit approximately 1300 9th grade student in four Montana schools. Using a non-inferiority design, we will randomize classrooms in each school to be instructed by a teacher from another school (YAM-TE; experimental) or a traditional external instructor (YAM-EXT; control). We will assess program fidelity of both YAM training and implementation via independent observer and instructor-reporter ratings. Youth will complete measures of acceptability at post-YAM and outcome measures at pre-YAM, post-YAM, and 12 month follow-up. Standard and mixed linear and logistic regression models will be used to test the main hypothesis that the YAM-TE does not differ from YAM-EXT regarding fidelity (teachers) and acceptability (teachers and youth). Exploratory analyses will test moderation of the intervention effect (e.g., sex, poverty) and the mediating effect of mental health literacy, belongingness, and perceived burdensomeness on the intervention effect. Results of this pilot study will inform the development of subsequent, fully powered noninferiority trials. Our long-term goal is to scale YAM-TE for implementation across rural US communities or, if culturally appropriate, more globally.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
1 Introduction
1.1 Suicide prevalence and risk among United States rural youth
Youth suicide is a growing mental health problem and rural youth suicide represents a major source of mental health inequity in the United States (US). Suicide is second only to accidental deaths in causing fatality in US youth aged 12–18 years, and rates have increased nationwide over the past 20 years [1,2,3,4]. Rural youth are especially at risk [5,6,7], with nearly twice the rates of suicides compared to their urban peers [8, 9]. For example, in Montana (MT), the suicide rate among 12- to 18-year-olds of 17.9 per 100,000 well exceeds the national average 6.4/100,000 [1]. Suicide-related thoughts or behaviors also are more common in rural youth; for example, consistently, over the past decade (and as illustrated using the latest available data, YRBSS 2019 [10]), more MT youth than youth across the US reported that they had seriously considered suicide (23.4 vs. 18.8%, p < 0.001), made a suicide plan (19.5 vs. 15.7%, p < 0.001), or attempted suicide (10 vs. 8.9%, n.s.) in the past 12 months [11,12,13]. Prevalence of these reports of suicide intent or attempts have increased both nationally and in MT over the past few years. Finally, “feeling sad or hopeless to a degree that affected some usual daily activities,” a strong predictor of suicidal ideation and attempts, has been reported by a large (and growing) number of youth [14, 15]. For example, the prevalence rose from 26.1% in 2009 to 36.7% in 2019 in the total US sample and from 27.3 to 36.7% in the MT sample [10].
Various theories have been proposed to explain risk for suicide across diverse age and racial/ethnic groups and across geographic locations, all describing risk as multifactorial across multiple risk domains (individual characteristics, familial or interpersonal, social or cultural [16,17,18,19,20]), and emphasizing negative intrapersonal states (e.g., negative emotions; feeling socially disconnected or a sense of thwarted belongingness; perceiving oneself as unduly burdensome [17]) and adverse life events (e.g., parental loss; maltreatment [21]) as risk-, and positive social norms and relationships as protective factors [22, 23]. Mental health problems are significantly associated with suicide and most decedents with a current mental health problem experienced depression [23, 24]. Connecting at-risk individuals to mental health resources is a key element of suicide prevention [6]. Yet only a minority of those in need do access care, and low mental health literacy and stigma are commonly noted barriers [25,26,27,28].
Rural youth face increased suicide risk (beyond common risk factors they share with their urban counterparts), including low mental health literacy [29], high mental health stigma [30, 31], lack of mental health services, social isolation [5, 32], poverty, and a pessimistic outlook on the future. Lower mental health literacy among rural vs. urban populations may impede recognition of emotional distress or psychopathology as concerns that warrant treatment [29, 31, 33, 34]. Self-stigmatization and fear of being stigmatized for seeking mental health care may be particularly acute in small communities where “everyone is in everyone else’s business” and where self-reliance is highly valued [34,35,36,37]. Many rural states are mental health services “deserts;” for example, in 2019, all MT counties were “Mental Health Care Professional Shortage Areas [38]. In rural states, the combination of vast geographic expanses with low population density, of long distances to and limited availability of mental health services [39], mean that rural youth live in under-resourced settings and represent an under-served population [6, 40]. Prevalent household poverty further exacerbates rural youth’s challenges [41] arising from physical and social isolation due to large distances between homes or lack of transportation; from feeling socially or politically excluded due to poverty or minority group status; and from lack of job prospects creating a sense of feeling trapped and hopeless about the future [42]. Individuals residing in rural communities also have been shown to have greater access to lethal means, increasing the likelihood that a suicide attempt will result in death [42,43,44,45,46].
These scientific advances in identifying suicide risk and protective factors notwithstanding, research has yielded only modest success in predicting suicide attempts [47,48,49,50,51]. Therefore, experts have called for “upstream,” developmentally tailored suicide prevention programs that strengthen coping and resilience [52] and readily reach youth [53,54,55,56]. In under-resourced communities with under-served populations in the US, schools often are the one public institution accessible to all.
1.2 School-based universal prevention programs are well-suited for addressing rural youth suicide risk
There is expert consensus that school-based universal suicide prevention efforts are needed to complement targeted or treatment approaches for several reasons [55,56,57,58,59,60]. One, schools have high reach even in rural or frontier communities: School attendance until age 16 is free and mandatory in all US states, with some states requiring students to remain in school until 17 or 18 years of age [61]; and school districts typically provide free transportation to students for whom walking to school is not an option for health or safety reasons. Therefore, neither poverty nor geographic location should prevent students from school attendance. Two, there is synergy between schools’ educational mission and focus on healthy child development and the goals of suicide prevention curricula [55,56,57,58,59, 62, 63]. Moreover, offering a suicide prevention program as part of the regular school curriculum on health and mental health topics ensures efficient and cost-effective intervention access for most youth, even in resource-poor communities [64]. Rural schools often face budgetary challenges that preclude offering a full suite of suicide intervention programs (e.g., targeted prevention or treatment of youth who attempted suicide). Therefore, school authorities favor a universal approach when facing budget constraints [65, 66]. Three, in many rural US communities, schools serve as a location for providing mental health care to youth and their families [40, 42]. Adolescents are reluctant to seek mental health care [67, 68], and those who do access medical care are unlikely to receive mental health care [69, 70]. Hence, school-based universal programs have high reach by not requiring that students access care (unlike suicide screening in primary care) or self-identify symptoms such as depression as problems requiring treatment (as would be the case for targeted prevention). And four, by being offer to all students, universal prevention programs avoid the potential risk of stigmatization arising from targeted prevention [59, 71].
Despite these advantages of school-based universal suicide prevention programs, knowledge gaps remain. Systematic reviews of psychosocial youth suicide prevention studies have noted that, overall, few studies have focused on universal interventions [58], and while there have been studies of interventions designed for elementary school children (e.g., the Good Behavior Game [72, 73] or the Promoting Alternative Thinking Strategies curriculum [74]), research of school-based universal suicide prevention programs for adolescents is limited. Moreover, except for small pilot efforts, there have been no studies of such programs when implemented in rural schools [59]. We propose to evaluate the effectiveness of an evidence-based universal suicide prevention program (Youth Aware of Mental Health, YAM) when adapted for implementation in low-resource, rural schools.
1.3 Why YAM is a promising universal youth suicide prevention program for rural youth
YAM [75] is a manualized, universal suicide prevention curriculum designed for delivery during regular school classes by trained instructors and assistants who are not part of the school staff [75,76,77]. The YAM program comprises 5 modules, including an initial didactic lesson followed by highly interactive sessions including small group work and role plays that draw upon students’ personal experiences. The rationale for using external instructors and assistants rather than school staff for program delivery is that students may be more open to participate fully in interactive class activities (e.g., role plays involving sensitive topics) without fear that revealing personal information might impact how school staff would interact with or evaluate student in the future.
YAM was found superior both in reducing suicide attempts and in cost-effectiveness versus other school-based universal suicide prevention programs in a large European cluster-randomized clinical trial. Specifically, the “Saving and Empowering Young Lives in Europe” (SEYLE) study randomized schools in 10 European countries to one of three youth suicide prevention interventions or a control condition. The sample comprised ~ 11,000 9th graders. Only the YAM program was found superior to the control condition: Students receiving the YAM program showed significantly reduced suicidality, including 55% fewer incident suicide attempts and 50% fewer cases of severe suicidal ideation, over one year [75, 76]. Using a payer’s perspective and modeling costs of the three active intervention programs and the control group, YAM had the lowest incremental cost per 1% incidence reduction of suicide attempts or ideation and per quality adjusted life year gained [64]. The high scientific rigor of SEYLE and the promising outcomes suggest that YAM is a prime intervention candidate for universal school-based youth suicide prevention.
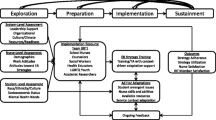
Beyond its proven efficacy [60], there also are compelling conceptual reasons for selecting YAM as the intervention approach for rural schools. The conceptual model underpinning YAM addresses well some of the needs of rural youth. As illustrated in Fig. 1, YAM embraces a strength-based, youth empowerment approach (i.e., is consistent with rural cultures’ ethos of self-reliance), yet also corrects stigmatizing beliefs about psychiatric symptoms (e.g., that feeling depressed or anxious in response to stressful experiences is a sign of weakness) and teaches students how to access help when needed. YAM seeks to reduce risk by teaching emotional awareness and emotion regulation skills; positive peer relationships (improving problem solving and decision-making and skills when facing common conflicts or problems); and mental health literacy (recognizing in self or others the need for help; identifying resources; reaching out for help). (YAM implementation details are described in the Method section.)

Model of action: from skills-building curricular targets to positive youth outcomes
1.4 Studies support the feasibility and acceptability of YAM as adapted for rural US youth
Evidence supports the feasibility and acceptability of YAM for rural youth in MT and Texas (TX). In a key step toward adapting YAM for US youth and in consultation with the developers of the YAM program [77], Lindow et al. [78] solicited qualitative feedback from two groups of 5 students each who had received the original, European YAM curriculum by certified instructors. Informed by the qualitative work, Lindow and colleagues adapted the training and course materials for US settings (e.g., incorporating idioms and examples based on local events or custom and replacing several role-play scenarios to be culturally suitable to US youth). This culturally adapted YAM version was evaluated in 11 high schools (81.3% school participation) in TX and MT for feasibility and acceptability [78] and for effectiveness in improving mental health literacy and reducing stigma [79]. YAM was delivered to 1,878 students (9th grade: 91.7%) during regular classes by trained instructors and assistants. Satisfaction surveys among school staff (N = 49), parents (N = 59) and students (N = 398) found that YAM was well-received. Moreover, mental health knowledge and help seeking for depression or suicidal ideation increased, and stigma scores decreased in students who received YAM in the MT/TX study [79].
The MT/TX study team conducted a subsequent feasibility study in 10 small MT schools, changing the delivery format by using trained land-grant Extension agents instead of the original model of external instructors and assistants [80]. Feasibility was measured as the percentage of schools willing to offer the program and acceptability was measured using student ratings. Results suggested that YAM is feasible and acceptable in rural schools. Specifically, 77% of invited schools participated and student ratings were highly favorably: 89.1% of youth rated “agree” or “strongly agree” to “it is a good idea to provide young people with a mental health and risk behavior prevention program in schools;” 70.3% reported they were pleased with YAM; 70.7% thought YAM should be suggested for other schools and 70.1% of youth thought students would find the program appropriate. Future studies should gather more detailed information from students about opportunities for program improvements.
These US-based offerings of YAM were supported by state funding for implementation expenses, enabling schools to offer the curriculum without costs to schools for the recruitment and training of the YAM instructors/assistants or for their time spent delivering the prevention intervention. Our team collected informal feedback from superintendents and school principals about their budgetary resources for picking up implementation costs. The resounding feedback was that the resources required for recruiting and training external YAM staff were unduly burdensome. Instead, school officials expressed a strong preference for their own staff to be trained as YAM program instructors/assistants. Yet, the YAM developers have been firm in their belief that the efficacy of YAM may be undermined if students are being taught by their own teachers. The opportunity for youth to share and utilize their personal stories as the basis of discussions and roleplay scenarios without concern that a teacher may in future interactions (e.g., grading; letters of recommendation, etc.) relate differently to students who divulged potentially sensitive personal information is deemed central to students’ engagement with and the efficacy of YAM. To resolve this dilemma, we propose a pilot study to lay the groundwork for a subsequent, fully-powered RCT study testing the efficacy of a novel implementation model for YAM, teacher exchanges (YAM-TE) versus the standard model involving external instructors/assistants (YAM-EXT).
1.5 Study aims: exploring the feasibility and acceptability of a teacher exchange model and collecting preliminary outcome data for YAM-TE versus YAM-EXT
Our long-range goal is to conduct an RCT study testing the efficacy of implementing YAM using a teacher exchange model (TE) rather than the standard model involving external instructors (EXT). Specifically, we propose to develop an implementation strategy involving neighboring schools exchanging teachers for teaching the YAM curriculum. In each participating school, teachers would be trained to serve as YAM instructors/assistants, but the instructional staff from one school would deliver the curriculum in the designated partner school, and vice versa. Embedding YAM instructors within schools is consistent with expert recommendations for making prevention interventions scalable and sustainable [81].
We believe the teacher exchange model would be suitable for communities with more than one middle- or high school or with like schools in close-by (≤ 30 miles) communities. These characteristics apply to a substantial number of MT communities: There are 15/15 Class AA schools (≥ 825 pupils) and 17/22 Class A schools (≥ 340–825 pupils) where exchanges could occur in the same town; there are 18/40 Class B schools (> 120–340 pupils) that could partner with near-by town. We envision that the primary targets for YAM-TS would be Schools AA-B. If proven feasible in our pilot study, the YAM-TE model could be implemented across MT and similar states in the US.
Before embarking on a fully-powered trial, pilot work is needed to answer questions about the feasibility of the proposed implementation strategy, as well as about the feasibility of methodological components such as recruitment and retention of research participants, randomization, assessment procedures, and training protocols. As recommended in a seminal paper on pilot studies [82], because they are by definition underpowered, pilot studies should not use control groups for the primary purpose of testing the differential efficacy of the novel versus original intervention. Rather, inclusion of a control group is advantageous for examining whether different interventions are associated with differential recruitment or attrition, whether randomization procedures can be implemented, and other aspects pertaining to the ultimate implementation of both intervention conditions. A primary focus of pilot studies is feasibility, i.e., whether a study protocol be executed or needs to be modified because some or all elements are unacceptable (e.g., participants decline participation or drop out; participants fail to complete assessments) or do not work (e.g., training fails to result in competent instruction of the program) which can be quantified as described below. Using a non-inferiority design, our pilot study will randomly assign classes to YAM-TE or YAM-EXT to address three aims, described next.
1.5.1 Aim 1: examine the feasibility and acceptability of the teacher exchange model, YAM-TE.
The proximal outcomes are fidelity (can TE staff deliver the YAM curriculum as competently as EXT?) and the number of YAM sessions taught as scheduled (are TE staff as adherent to the teaching schedule, i.e., available to teach the class, as the EXT staff?). The primary outcomes are acceptability of YAM-TE to students (do students exposed to TE rate acceptability at comparable levels to students exposed to EXT?) and teachers (are teachers willing to endorse the TE model after completion of the pilot study?).
1.5.2 Aim 2: examine the feasibility and acceptability of the research methods
We will quantify feasibility of (a) randomization as the number of classes who receive the assigned YAM implementation format/the number of randomized classes; (b) recruitment as the number of students who agree to provide assessment data (have parental consent and student assent and attend assessment sessions)/the number of students invited to participate; (c) retention as the number of students who completed subsequent assessments (post-YAM; 12 months)/ the number of students who provided baseline data; and (d) assessment procedures as the number of students enrolled in the study with at least 90% of item completion, at each assessment point.
1.5.3 Aim 3: gather preliminary outcome data
A proximal primary outcome (measured at end of the YAM program) is willingness to seek help, and distal primary outcomes (measured at a 12 month follow-up) include suicidal ideation and attempts. Secondary proximal outcomes include changes in students’ mental health literacy, help seeking, and psychosocial functioning. We also will measure potential moderators (e.g., sex; family poverty [83]) and potential mechanisms [84] explaining YAM distal primary outcomes (increased: help seeking; belongingness; coping; reduced: perceived burdensomeness; depression [85,86,87]). We expect non-inferiority of YAM-TE versus YAM-EXT on all outcomes; all analyses regarding our feasibility study’s third aim are exploratory.
2 Method
2.1 Overview and study design
We will employ a noninferiority design (combining implementation and effectiveness methods) [88] and randomize (at each school) course sections to receive YAM-TE (experimental group) or YAM-EXT (control group). As shown in Fig. 2, students will be asked to complete a baseline assessment the week prior to receiving the YAM curriculum. YAM will be taught in 5 class periods (60 min each), spread across 3 weeks. Post-assessments will be performed upon completion of the final YAM lesson; longer-term program impact will be measured at 12 month follow-up.

Timeline of program delivery and youth assessments
2.2 YAM curriculum and training
2.2.1 YAM program
YAM is a manualized school-based universal prevention program designed to raise students’ awareness about risk and protective factors associated with suicide; teach them a basic understanding of mental disorders, dispel myths and stigma about mental illness, and educate students about healthcare resources and help seeking; and help students enhance coping skills and emotional resiliency to deal with adverse life events, stress, and suicidal risk [75]. YAM comprises five lessons taught by a trained instructor (aided by an assistant) during regular (60 min) class periods [89]; an instruction booklet for students within which the core program themes are reinforced; and colorful posters for display in the classroom for the duration of the program that highlight each session’s core messages. YAM seeks to empower students to think about, verbalize, and discuss their stressors and mental health concerns, using active learning strategies (e.g., small group work and role-plays) and focusing on real-world scenarios that are meaningful to them. Key topics and pedagogical approaches are shown in Fig. 3. The proposed study will utilize an instructors’ manual reflecting adaptations reflective of experiences of and the language used by US youth [78].

YAM Session Content and Primary Teaching Mode
2.2.2 Instructor training and supervision
YAM is taught by a trained instructor with support of an assistant who helps manage the class and lead small-group discussions. All instructors will receive the instructors’ manual, student booklet, and classroom posters. In separate workshops, TE and EXT instructors (5-day training) and assistants (1-day training) will be taught by two trainers (certified by the YAM developers and following the YAM training model). In brief, the training involves a combination of lectures, discussion and role-plays covering common psychopathology experienced by youth and how to detect and understand youth psychopathology; youth suicide risk factors; barriers to seeking care; how to create a supportive class environment for discussion of student concerns or interpersonal problems; teaching coping skills and problem solving (stop, think, act, evaluate); handling participation issues such as overly shy students or disruptions; and safely managing at-risk students consistent with school safety protocols and following study protocols such as responding to and reporting adverse events. During YAM implementation, all instructors will participate in bi-weekly supervision meetings (separate for TE or EXT) via videoconference and may request, as needed, consultation with a trainer.
2.3 Participants and recruitment
2.3.1 Participating schools and randomization
We will invite four public high schools in MT that reflect the type of rural school most likely suited for the proposed implementation model: schools need to be large enough to have an adequately sized pool of teaching staff interested in becoming trained YAM instructors and geographically close enough to another school for switching instructors, thus preserving the YAM requirement that instructors do not teach students from their own school. At each school, the entire 9th grade will be organized into sections of 20–25 students based on the grade’s course schedule. Given current enrollments, we expect to offer 10–12 sections (5–6 YAM-TE, 5–6 YAM-EXT), per school. Sections will be randomized such that at each school, approximately half of the students will be exposed to YAM-TE (i.e., program delivery by two trained teaching staff employed by another school) and about half of the students will be exposed to the standard YAM delivery format (i.e., two external, trained instructors). By randomizing at the level of section within a school rather than at the level of school, we control for seasonal factors that might affect implementation (e.g., weather related school delays; seasonal effects on mood or health behaviors; etc.).
2.3.2 Students
At each school, all 9th-grade students will receive the YAM curriculum as part of their health curriculum during regular school periods and be invited to participate in the feasibility study. Of the approximately 1300 pupils eligible for study inclusion, we expect a minimum response rate (receipt of both parental/guardian consent and student assent) of 55%, for a total study sample of ~ 715 youth. There are several reasons for targeting 9th grade students: (1) the original YAM program was designed for and tested among 14–16 year-old youth in the 9th grade; (2) developmentally 9th grade is a stressful transition period for youth in the United States as they are entering high school [90, 91]; and (3) 12-month median prevalence estimates of depression in mid-to-late adolescence are much higher than in childhood (4–5% vs. < 1%, respectively) and cumulative probability rising from 5% in early adolescence to 20% at the start of emerging adulthood [92].
2.4 Instruments and procedures
Our implementation outcome measures [76, 77] are informed by the SELYE study [76], literature on implementing school-based curricula [93], and theoretical protective and risk factors for suicide among rural youth [6, 18, 42, 94, 95]. Given our emphasis on feasibility and acceptability of the novel implementation model, we propose fewer distal outcome measures than the original YAM to accommodate participating schools’ concerns about the study taking up too much class time.
2.4.1 Instructor assessment of the feasibility of YAM-TE versus YAM-EXT
We will ask instructors about their experience both post-training and post-program delivery the following questions on a 5-point Likert scale (strongly disagree to strongly agree): “The YAM training was worth my time” (post-training) and “Teaching the YAM program was worth my time” (post-YAM) [96]. Additionally, we will ask instructors to answer these open-ended questions (3 post-training and 4 post-YAM implementation): “What did you like the most about the YAM training?” “What did you like the least about the YAM training? “What are your recommendations to improve the YAM training?” “What did you like the most about teaching the YAM program? “What did you like the least about teaching the YAM program? “What are your recommendations to improve the YAM program?” “What could be done to better support you in your role as YAM instructor?” [89].
Fidelity will be measured via classroom observation and instructors’ self-report, using checklists. Classroom observations will be conducted by trainers during 5 randomly selected YAM sessions per YAM-TE or YAM-EXT. Observers will be a neutral presence in the classroom; they will use the Fidelity Checklist (same as self-report checklist, below) to assess key components of the session as well as rating the quality of implementation. Observers will not provide feedback to instructors at the time of observation; rather, instructors will receive summary reports upon completion of the study. No youth will be identified on the Fidelity Checklist. After each YAM class, TE and EXT instructors will complete a fidelity self-report checklist, indicating (yes/no) whether core YAM content or activities comprising a session was covered (e.g., session 1: “clearly reviewed symptoms of depression, giving examples for each”). In an open text box next to each checklist item, instructors may comment on student engagement in discussion around the curriculum; how adequately prepared instructors felt to lead the discussion; and whether (and if so why) any topics were not covered. On a standard form, instructors will record any changes made to key components during sessions and any issues or barriers they experienced implementing session content. Self-assessments should take no more than five minutes/YAM session to complete.
2.4.2 Youth assessments of the acceptability of YAM-TE versus YAM-EXT
Upon completing the YAM program, youth will be asked to rate six items (using a 5-point Likert scale), asking whether they thought YAM was helpful; added to their understanding of mental health; enhanced their knowledge and skills; was respectful of their cultural background; whether they trusted the instructor; and whether the instructor was skilled at teaching YAM. Via two open-ended questions, youth will be asked to report two things they liked about YAM and what, if anything, they would change about the program.
2.4.3 Youth demographic characteristics, assessments of outcomes
Youth will complete baseline, post-YAM (outcomes/mediators only), and 12 month assessments in a computer lab or using iPADs during health class. Based on pilot work, we expect youth assessments to take about 30 min.
2.4.3.1 Demographic questionnaire
Youth will be asked to report age; sex (male, female, nonbinary); race/ethnicity, receipt of free school lunch during the current school year, and a question concerning family food insecurity adapted from the USDA Food Security Survey Model [97] (“In the previous 12 months was there any time your family has run out of food and not been able to purchase more?”). We will use Goodman et al.’s adaptation of the “MacArthur ladders” to assess socioeconomic status. The MacArthur ladders have been found to be reliable across culturally diverse samples of children [98]. Youth indicate “at this time,” on which rung of the pictorial 10-rung ladder they believe their family stands relative to other families in the US society (subjective SES). Anchor points are provided at 10 (“at the top are the people who are the best off– have the most money, the highest amount of schooling; and the jobs that bring the most respect”) and at 1 (“at the bottom are the people who are the worst off—they have the least money, little or no education, and no job or the jobs that no one respects”) [99, 100]. To measure perceived social status among their school peers, students will be presented with another ladder (“Now assume that the ladder is a way of picturing your school”) and asked to place themselves relative to other students. Rung 10 represents “the people in your school with the most respect, the highest grades, and the highest standing,” and rung 1 represents “the people no one respects, no one wants to hang around with, and have the worst grades.” In a large adolescent community sample, each of the ladders and the ladders combined explained about 10% of unique variance of adolescents’ depression scores [99].
2.4.3.2 Depression and suicidal behaviors
Three standardized Youth Risk Behavior Survey questions (response choices: yes/no) will be included: “During the past 12 months, did you ever feel so sad and hopeless almost every day for two weeks or more in a row, that you stopped doing some usual activities?”; “Have you ever seriously thought about killing yourself?”; “Have you ever tried to kill yourself?” [101].
2.4.3.3 Psychological risk factors for youth suicide, behavioral health problems, and impairment
We will use 8 items of the Interpersonal Needs Questionnaire [102] to measure Thwarted Belongingness (e.g., “These days, I feel like I belong”) and Perceived Burdensomeness (e.g., “These days, I feel like a burden on the people in my life”), each rated on a 4-point scale (1 = Not at all true for me to 4 = Very true for me). We will use the 25-item Strengths and Difficulties Questionnaire (SDQ) [103] to measure emotional symptoms, conduct problems, hyperactivity and/or inattention, peer relationship problems and pro-social behavior. The SDQ has been validated extensively [104] and was used in the YAM trial [75, 105]. We will measure past-12-month impairment due to a mental (item 1) or alcohol/drug (item 2) problem; sleep disturbance using 4 items from the PROMIS Pediatric Disturbances Item Bank, which was validated for youth ages 8 to 17 years [106]; and subjective well-being using the 5-item WHO Well-being Scale (WHO-5) (0 = worst possible to 5 = best possible quality of life) and has been shown to provide reliable assessment of adolescents’ subjective well-being [77, 107, 108]. We will use the 4-item subscales “Cognitive Decision Making” (e.g., “You thought about what would happen before you decided what to do”), “Direct Problem Solving” (e.g., “You tried to make things better by changing what you did”), “Control” (e.g., “You told yourself you could handle whatever happens”), and “Optimism” (e.g., “You told yourself that things would get better”) of the Children’s Coping Strategies Checklist–Revised (CCSC-R) [109, 110]. Youth will be asked to rate how often they usually use a strategy to solve their problems or make themselves feel better within the past month on a 4-point scale (1 = Never to 4 = Most of the time). The CCSC-R has been used to assess coping behaviors in youth ages 9–15 years from various demographic backgrounds and participating in youth mental health interventions [52, 111].
2.4.3.4 Mental health literacy, help seeking confidence and behaviors
We will use 7 items from the Depression Knowledge Test [112] to measure students’ knowledge acquisition related to core content of YAM and one open-ended question about knowledge of local mental health resources. We will assess youth’s confidence to seek help, using a 5-point Likert scale (1 = Not confident at all to 5 = Very confident), asking “How confident are you to seek help if you had (a) an alcohol or drug problem, (b) depression, anxiety, or another emotional problem, and (c) thoughts about killing yourself?” [113]. We will ask 3 questions about help seeking (yes/no): “In the past 12 months, have you talked to a medical doctor or other professional (psychologists, counselors, nurse, other healing professionals) about (a) problems with feeling depressed or anxious problems, (b) drinking alcohol or taking drugs, or (c) thinking about killing yourself or having made an attempt to kill yourself?”.
2.5 Data analysis plan
2.5.1 Preliminary data evaluation
Prior to analysis, the data will be audited for quality and completeness, including missing data patterns and evaluation of distributions. The equivalence of the random assignment of groups will be assessed by comparison of intervention groups on demographic and clinical characteristics. Should groups differ on any characteristics, these variables will be used as covariates in the analyses.
2.5.2 Analysis of primary hypotheses
To date, there have been no RCT studies evaluating the use of TE instructors to deliver the YAM program. Hence, there is no historical evidence for determining a noninferiority margin (M1) to test the hypothesis that the YAM-TE does not differ from the standard YAM-EXT regarding fidelity (teachers) and acceptability (teachers and youth). In the absence of statistical evidence, we will use Cohen’s [114] recommendations for a moderate effect size to define M1. For quantitative outcomes, M1 will be Cohen’s d = 0.5 (YAM-TE performs worse than YAM-EXT), and for binary outcomes, M1 will be relative risk (RR) = 1.90 (YAM-TE performs worse than YAM-EXT). The results of these pilot study analyses will inform the development of a statistically informed M1 for the YAM-TE compared to YAM-EXT in a future fully powered noninferiority trial.
Linear (continuous outcomes) and logistic (binary outcomes) regression analyses will be used to test hypotheses for teacher outcomes. Separate regression models will be tested to estimate unadjusted intervention effects and intervention effects adjusted for potential confounding variables (e.g., sex). Parameter estimates from these analyses will be used to calculate effect sizes and 95% confidence intervals for the difference between the YAM-TE and YAM-EXT groups. If the 95% confidence interval for the effect size exceeds M1, that is, the effect size for the inferiority of the YAM-TE relative to the YAM-EXT is greater than Cohen’s d = 0.5 or RR = 1.90, this would suggest that the YAM-TE is inferior to the YAM-ETX, and we cannot reject the null hypothesis that the YAM-TE does not differ from the YAM-EXT on the outcomes.
Mixed linear and logistic regression analysis will be used to test hypotheses for youth outcomes, adjusting for clustering of students within teacher/trainer. Separate regression models for post-intervention student acceptability will be tested to estimate unadjusted intervention effects and intervention effects adjusted for potential confounding variables (e.g., gender, ethnicity). Models evaluating other student outcomes will adjust for pre-intervention variables, in addition to potential confounding variables (e.g., sex, ethnicity). The parameter estimates from these analyses will be used to calculate effect sizes and 95% confidence intervals for the difference between the YAM-TE and YAM-ETX groups. If the 95% confidence interval for the effect size exceeds the non-inferiority margin, that is, the effect size for the inferiority of the YAM-TE relative to the YAM-EXT is greater than Cohen’s d = 0.5 or RR = 1.90, this would suggest that the YAM-TE is inferior to the YAM-EXT, and we cannot reject the null hypothesis that the YAM-TE does not differ from the YAM-EXT.
Exploratory analyses will include testing moderation of the intervention effect by potential modifier variables (e.g., sex, family poverty). Hierarchical mixed models will be used to test the mediating effect of mental health literacy, belongingness, and perceived burdensomeness on the intervention effect. Additional exploratory analyses may involve incorporating teacher/trainer outcomes in the mixed models as predictors of youth outcomes, as well as teacher/trainer outcomes, by intervention group interactions to evaluate the potential moderating effect of teacher/trainer characteristics on intervention group differences in student outcomes.
2.6 Ethical considerations
The study will not commence until approved by the Institutional Review Board (IRB) of the participating university and by the local school district’s superintendent office. A draft IRB protocol is provided in Supplement A. Past studies have shown that asking about suicide does not increase risk for self-harm [115, 116]; and the two questions we will ask student are taken from a widely-used youth suicide risk assessment tool already given to students in the four participating schools [11]. Safety will be measured by TE and EXT instructors’ completion of an adverse event checklist after each YAM class.
3 Discussion
We expect our study to expand the science of youth suicide prevention by targeting an as-yet under-served study population, rural youth, and evaluating a teaching model that preserves the goal of providing YAM by instructional staff unfamiliar to the students, yet that may be superior regarding sustainability for resource-strapped rural communities (YAM-TE). Our study is designed to collect feasibility and acceptability data concerning all aspects of the prevention trial: program delivery format, recruitment, and assessment strategies and measures. It also will generate pilot data concerning proximal (end of program) and distal outcomes.
3.1 Limitations and future directions
Several limitations warrant consideration. One, the YAM curriculum is designed to engage all youth in a classroom to share their perspective or provide specific examples of challenges they encounter in their daily lives. As such, the proposed study will not endeavor to create separate adaptations by ethnic group, but rather will maintain YAM’s universal prevention approach. That said, for interventions in states such as MT, we believe that developing and testing a cultural adaptation of YAM for implementation in Native American reservation schools represents an important goal but exceeds the scope of our study and warrants being the focus of a separate study. Related, in US states with other ethnic or racial minorities (e.g., African American youth or Latinx youth), studies are needed to examine the cultural appropriateness and efficacy of YAM. Two, the TE delivery model is envisioned to work in communities where neighboring schools are located close enough for exchanging teachers without undue time burdens of transportation costs. For geographically more isolated schools, the standard EXT model may still be the better option; alternatively, in states with land-grant universities, the Extension model may be a sustainable option. Three, generalizability of findings will depend in part on robust student participation. We believe that the feasibility study approach is invaluable for gathering information about optimizing strategies for securing parental consent and student assent. While the proposed study will be carried out in one rural US state (MT), if proven feasible and based on pilot data promising to be effective, we believe the YAM-TE model can be applied in other US states and may ultimately offer a model for other countries.
References
Centers for disease control and prevention. WISQARS: Fatal injury data. 2019.
Miron O, Yu KH, Wilf-Miron R, Kohane IS. Suicide rates among adolescents and young adults in the United States, 2000–2017. JAMA. 2019;321(23):2362–4.
Curtin SC, Heron M. Death rates due to suicide and homicide among persons aged 10–24: United States, 2000–2017. NCHS Data Brief. 2019;352:1–8.
Ballesteros MF, Webb K, McClure RJ. A review of CDC’s web-based injurys statistics query and reporting system (WISQARS): planning for the future of injury surveillance. J Safety Res. 2017;61:211–5.
Hirsch JK, Cukrowicz KC. Suicide in rural areas: an updated review of the literature. J Rural Ment Health. 2014;38(2):65.
Centers for Disease Control and Prevention. Suicide policy brief: preventing suicide in rural America 2020. https://www.cdc.gov/ruralhealth/suicide/policybrief.html.
Hirsch JK. A review of the literature on rural suicide: risk and protective factors, incidence, and prevention. Crisis. 2006;27(4):189–99.
Fontanella CA, Hiance-Steelesmith DL, Phillips GS, Bridge JA, Lester N, Sweeney HA, et al. Widening rural-urban disparities in youth suicides, United States, 1996–2010. JAMA Pediatr. 2015;169(5):466–73.
Singh GK, Siahpush M. Widening rural-urban disparities in all-cause mortality and mortality from major causes of death in the USA, 1969–2009. J Urban Health. 2014;91(2):272–92.
Centers for Disease Control and Prevention. High School YRBSS: Montana 2019 and United States 2019 Results 2019. https://nccd.cdc.gov/Youthonline/App/Results.aspx?SID=HS&QID=H28&LID=MT&YID=2019&COL=S&QP=G.
Centers for Disease Control and Prevention. High School Youth Risk Behavior Surveillance System (YRBSS) (2017). Unintentional injuries: Suicide-related behaviors: Attempted suicide 2019. https://nccd.cdc.gov/youthonline/App/QuestionsOrLocations.aspx?CategoryId=C01.
Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance Survey Montana Mental Health Results 1999–2018 2020. file:///C:/Users/Ruth%20Weissman/Documents/CMHRR/YAM/MT%20mental%20health%20data%20through%202019.pdf.
Centers for Disease Control and Prevention. YRBSS Explorer 2019. https://yrbs-explorer.services.cdc.gov/#/.
Price JH, Khubchandani J. Latina adolescents health risk behaviors and suicidal ideation and suicide attempts: results from the national youth risk behavior survey 2001–2013. J Immigr Minor Health. 2017;19(3):533–42.
Qiao N, Bell TM. Indigenous adolescents’ suicidal behaviors and risk factors: evidence from the national youth risk behavior survey. J Immigr Minor Health. 2017;19(3):590–7.
Van Meter AR, Paksarian D, Merikangas KR. Social functioning and suicide risk in a community sample of adolescents. J Clin Child Adolesc Psychol. 2019;48(2):273–87.
Chu C, Buchman-Schmitt JM, Stanley IH, Hom MA, Tucker RP, Hagan CR, et al. The interpersonal theory of suicide: a systematic review and meta-analysis of a decade of cross-national research. Psychol Bull. 2017;143(12):1313–45.
Cha CB, Franz PJ, Guzmán ME, Glenn CR, Kleiman EM, Nock MK. Annual research review: Suicide among youth - epidemiology, (potential) etiology, and treatment. J Child Psychol Psychiatry. 2018;59(4):460–82.
De Beurs D, Fried EI, Wetherall K, Cleare S, Connor DB, Ferguson E, et al. Exploring the psychology of suicidal ideation: a theory driven network analysis. Behav Res Therapy. 2019;120:103419.
Kasen S, Chen H. Social context and change in suicide ideation in a community sample of youths. Soc Psychiatry Psychiatr Epidemiol. 2020;55(3):319–27.
Thompson MP, Kingree JB, Lamis D. Associations of adverse childhood experiences and suicidal behaviors in adulthood in a U.S. nationally representative sample. Child Care Health Dev. 2019;45(1):121–8.
Whitlock J, Wyman PA, Moore SR. Connectedness and suicide prevention in adolescents: pathways and implications. Suicide Life Threat Behav. 2014;44(3):246–72.
Nock MK, Green JG, Hwang I, McLaughlin KA, Sampson NA, Zaslavsky AM, et al. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: results from the National Comorbidity Survey Replication Adolescent Supplement. JAMA Psychiat. 2013;70(3):300–10.
Ertl A, Sheats KJ, Petrosky E, Betz CJ, Yuan K, Fowler KA. Surveillance for violent deaths-National Violent Death Reporting System, 32 States, 2016. MMWR Surveill Summ. 2019;68(9):1–36.
Hom MA, Stanley IH, Joiner TE Jr. Evaluating factors and interventions that influence help-seeking and mental health service utilization among suicidal individuals: a review of the literature. Clin Psychol Rev. 2015;40:28–39.
Michelmore L, Hindley P. Help-seeking for suicidal thoughts and self-harm in young people: a systematic review. Suicide Life Threat Behav. 2012;42(5):507–24.
Rowe SL, French RS, Henderson C, Ougrin D, Slade M, Moran P. Help-seeking behaviour and adolescent self-harm: a systematic review. Aust N Z J Psychiatry. 2014;48(12):1083–95.
Kutcher S, Wei Y, Costa S, Gusmao R, Skokauskas N, Sourander A. Enhancing mental health literacy in young people. Eur Child Adolesc Psychiatry. 2016;25(6):567–9.
Jorm AF. Why we need the concept of “mental health literacy.” Health Communnicat. 2015;30(12):1166–8.
Bellamy GR, Bolin JN, Gamm LD. Rural Healthy People 2010, 2020, and beyond: the need goes on. Fam Community Health. 2011;34(2):182–8.
Monteith LL, Smith NB, Holliday R, Dorsey Holliman BA, LoFaro CT, Mohatt NV. “We’re afraid to say suicide”: Stigma as a barrier to implementing a community-based suicide prevention program for rural veterans. J Nervous Mental Dis. 2019;208:371–6.
Zamora-Kapoor A, Nelson LA, Barbosa-Leiker C, Comtois KA, Walker LR, Buchwald DS. Suicidal ideation in American Indian/Alaska Native and White adolescents: the role of social isolation, exposure to suicide, and overweight. Am Indian Alsk Native Ment Health Res. 2016;23(4):86–100.
Kennedy AJ, Brumby SA, Versace VL, Brumby-Rendell T. Online assessment of suicide stigma, literacy and effect in Australia’s rural farming community. BMC Public Health. 2018;18(1):846.
Heitkamp T, Nielsen, S., Schroeder, S. Promoting positive mental health in rural schools 2019 https://mhttcnetwork.org/centers/mountain-plains-mhttc/product/promoting-positive-mental-health-rural-schools.
Miller B, Baptist J, Johannes E. Health needs and challenges of rural adolescents. Rural Remote Health. 2018;18(3):4325.
Varia SG, Ebin J, Stout ER. Suicide prevention in rural communities: perspectives from a community of practice. J Rural Mental Health. 2014;38:109–15.
Ibrahim N, Amit N, Shahar S, Wee LH, Ismail R, Khairuddin R, et al. Do depression literacy, mental illness beliefs and stigma influence mental health help-seeking attitude? A cross-sectional study of secondary school and university students from B40 households in Malaysia. BMC Public Health. 2019;19(Suppl 4):544.
Rural Health Information Hub. Health Professional Shortage Areas: Mental Health, by County 2019. https://www.ruralhealthinfo.org/data-explorer?id=209&state=MT.
Kaiser Family Foundation. Mental Health Care Health Professional Shortage Areas 2018. https://www.kff.org/other/state-indicator/mental-health-care-health-professional-shortage-areas-hpsas/?currentTimeframe=0&selectedRows=%7B%22states%22:%7B%22montana%22:%7B%7D%7D%7D&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
Blackstock JS, Chae KB, Mauk GW, McDonald A. Achieving access to mental health care for school-aged children in rural communities: a literature review. The Rural Educator. 2018;39(1):12–5.
Singh GK, Daus GP, Allender M, Ramey CT, Martin EK, Perry C, et al. Social determinants of health in the United States: addressing major health inequality trends for the nation, 1935–2016. Int J MCH AIDS. 2017;6(2):139–64.
Stark CR, Riordan V, O’Connor R. A conceptual model of suicide in rural areas. Rural Remote Health. 2011;11(2):1622.
Anestis MD, Houtsma C. The association between gun ownership and statewide overall suicide rates. Suicide Life Threaten Behav. 2018;48(2):204–17.
Wertz J, Azrael D, Miller M. Americans who become a new versus a former gun owner: implications for youth suicide and unintentional firearm injury. Am J Public Health. 2019;109(2):212–4.
Nestadt PS, Triplett P, Fowler DR, Mojtabai R. Urban-rural differences in suicide in the State of Maryland: the role of Ffrearms. Am J Public Health. 2017;107(10):1548–53.
Hanlon TJ, Barber C, Azrael D, Miller M. Type of firearm used in suicides: findings from 13 states in the National violent death reporting system, 2005–2015. J Adolesc Health. 2019;65(3):366–70.
Ribeiro JD, Huang X, Fox KR, Franklin JC. Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br J Psychiatry. 2018;212(5):279–86.
Glenn CR, Kleiman EM, Cha CB, Deming CA, Franklin JC, Nock MK. Understanding suicide risk within the Research Domain Criteria (RDoC) framework: a meta-analytic review. Depress Anxiety. 2018;35(1):65–88.
Huang X, Ribeiro JD, Musacchio KM, Franklin JC. Demographics as predictors of suicidal thoughts and behaviors: a meta-analysis. PLoS ONE. 2017;12(7): e0180793.
Bentley KH, Franklin JC, Ribeiro JD, Kleiman EM, Fox KR, Nock MK. Anxiety and its disorders as risk factors for suicidal thoughts and behaviors: a meta-analytic review. Clin Psychol Rev. 2016;43:30–46.
Franklin JC, Ribeiro JD, Fox KR, Bentley KH, Kleiman EM, Huang X, et al. Risk factors for suicidal thoughts and behaviors: a meta-analysis of 50 years of research. Psychol Bull. 2017;143(2):187–232.
O’Hara KL, Sandler IN, Wolchik SA, Tein JY. Coping in context: The effects of long-term relations between interparental conflict and coping on the development of child psychopathology following parental divorce. Develop Psychopathol. 2019;31(5):1695–713.
Wyman PA. Developmental approach to prevent adolescent suicides: research pathways to effective upstream preventive interventions. Am J Prev Med. 2014;47(3 Suppl 2):S251–6.
Franklin JC, Huang X, Fox KR, Ribeiro JD. What suicide interventions should target. Curr Opin Psychol. 2018;22:50–3.
Zalsman G, Hawton K, Wasserman D, van Heeringen K, Arensman E, Sarchiapone M, et al. Evidence-based national suicide prevention taskforce in Europe: a consensus position paper. Eur Neuropsychopharmacol. 2017;27(4):418–21.
Zalsman G, Hawton K, Wasserman D, van Heeringen K, Arensman E, Sarchiapone M, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry. 2016;3(7):646–59.
Wilcox HC, Wyman PA. Suicide prevention strategies for improving population health. Child Adolesc Psychiatr Clin N Am. 2016;25(2):219–33.
Calear AL, Christensen H, Freeman A, Fenton K, Busby Grant J, van Spijker B, et al. A systematic review of psychosocial suicide prevention interventions for youth. Eur Child Adolesc Psychiatry. 2016;25(5):467–82.
Robinson J, Bailey E, Witt K, Stefanac N, Milner A, Currier D, et al. What works in youth suicide prevention? A systematic review and meta-analysis. EClinicalMedicine. 2018;4–5:52–91.
Mann JJ, Michel CA, Auerbach RP. Improving suicide prevention through evidence-based strategies: a systematic review. Am J Psychiatry. 2021;178(7):611–24.
National Center for Education Statistics. Compulsory school attendance laws, minimum and maximum age limits for required free education, by state: 2017 2017. https://nces.ed.gov/programs/statereform/tab5_1.asp.
Substance Abuse and Mental Health Services Administration. National strategy for suicide prevention implementation assessment report 2017. https://store.samhsa.gov/system/files/sma17-5051.pdf.
Centers for Disease Control and Prevention. State suicide prevention planning: A CDC research brief. https://www.cdc.gov/violenceprevention/pdf/state-suicide-prevention-planning-brief.pdf.
Ahern S, Burke LA, McElroy B, Corcoran P, McMahon EM, Keeley H, et al. A cost-effectiveness analysis of school-based suicide prevention programmes. Eur Child Adolesc Psychiatry. 2018;27(10):1295–304.
Miller DN, Eckert TL, DuPaul GJ, White GP. Adolescent suicide prevention: acceptability of school-based programs among secondary school principals. Suicide Life Threat Behav. 1999;29(1):72–85.
Schorr M, Van Sant W, Jameson JP. Preventing suicide among students in rural schools. In: Michael KD, Jameson JP, editors. Handbook of rural school mental health: Springer International Publishing/Springer Nature, Cham; 2017. p. 129–45, Chapter xxix, 390 Pages.
Cotter P, Kaess M, Corcoran P, Parzer P, Brunner R, Keeley H, et al. Help-seeking behaviour following school-based screening for current suicidality among European adolescents. Soc Psychiatry Psychiatr Epidemiol. 2015;50(6):973–82.
Hardin HK, McCarthy VL, Speck BJ, Crawford TN. Diminished trust of healthcare providers, risky lifestyle behaviors, and low use of health services: a descriptive study of rural adolescents. J Sch Nurs. 2018;34(6):458–67.
Avenevoli S, Swendsen J, He JP, Burstein M, Merikangas KR. Major depression in the national comorbidity survey-adolescent supplement: prevalence, correlates, and treatment. J Am Acad Child Adolesc Psychiatry. 2015;54(1):37-44.e2.
Costello EJ, He JP, Sampson NA, Kessler RC, Merikangas KR. Services for adolescents with psychiatric disorders: 12-month data from the National Comorbidity Survey-Adolescent. Psychiatr Serv. 2014;65(3):359–66.
Klimes-Dougan B, Klingbeil DA, Meller SJ. The impact of universal suicide-prevention programs on the help-seeking attitudes and behaviors of youths. Crisis. 2013;34(2):82–97.
Ialongo NS, Domitrovich C, Embry D, Greenberg M, Lawson A, Becker KD, et al. A randomized controlled trial of the combination of two school-based universal preventive interventions. Dev Psychol. 2019;55(6):1313–25.
Embry DD. The Good Behavior Game: a best practice candidate as a universal behavioral vaccine. Clin Child Fam Psychol Rev. 2002;5(4):273–97.
Humphrey N, Hennessey A, Lendrum A, Wigelsworth M, Turner A, Panayiotou M, et al. Public Health Research. The PATHS curriculum for promoting social and emotional well-being among children aged 7–9 years: a cluster RCT. Southampton (UK): NIHR Journals Library; 2018.
Wasserman D, Hoven CW, Wasserman C, Wall M, Eisenberg R, Hadlaczky G, et al. School-based suicide prevention programmes: the SEYLE cluster-randomised, controlled trial. Lancet. 2015;385(9977):1536–44.
Wasserman D, Carli V, Wasserman C, Apter A, Balazs J, Bobes J, et al. Saving and empowering young lives in Europe (SEYLE): a randomized controlled trial. BMC Public Health. 2010;10:192.
Carli V, Wasserman C, Wasserman D, Sarchiapone M, Apter A, Balazs J, et al. The saving and empowering young lives in Europe (SEYLE) randomized controlled trial (RCT): methodological issues and participant characteristics. BMC Public Health. 2013;13:479.
Lindow JC, Hughes JL, South C, Gutierrez L, Bannister E, Trivedi MH, et al. Feasibility and acceptability of the Youth Aware of Mental Health (YAM) intervention in US adolescents. Archiv Suicide Res. 2019;24:1–16.
Lindow JC, Hughes JL, South C, Minhajuddin A, Gutierrez L, Bannister E, et al. The youth aware of mental health intervention: impact on help seeking, mental health knowledge, and stigma in U.S. adolescents. J Adolesc Health. 2020;67(1):101–7.
Bailey SJ, Oosterhoff B, Lindow JC, Robecker T, Bryan B, Byerly MJ. Feasibility, acceptability, and fidelity: extension agents teaching youth aware of mental health. J Rural Mental Health. 2021;46:88.
Tolan PH. Scaling up evidence-based interventions within the US Public Health Market. Prev Sci. 2019;20(8):1169–72.
Leon AC, Davis LL, Kraemer HC. The role and interpretation of pilot studies in clinical research. J Psychiatr Res. 2011;45(5):626–9.
Musci RJ, Kharrazi H, Wilson RF, Susukida R, Gharghabi F, Zhang A, et al. The study of effect moderation in youth suicide-prevention studies. Soc Psychiatry Psychiatr Epidemiol. 2018;53(12):1303–10.
Insel TR. The NIMH experimental medicine initiative. World Psychiatry. 2015;14(2):151–3.
Silverman WK, Pettit JW. Developmental window of opportunity: implications of parent-child psychotherapy for early childhood depression treatment. Am J Psychiatry. 2018;175(11):1051–3.
López R Jr, Brick LA, Defayette AB, Whitmyre ED, Wolff J, Frazier E, et al. Depressive symptom severity mediates the association between avoidant problem-solving style and suicidal ideation. J Affect Disord. 2020;274:662–70.
Hill RM, Pettit JW. Pilot randomized controlled trial of LEAP: A selective preventive intervention to reduce adolescents’ perceived burdensomeness. J Clin Child Adolesc Psychol. 2019;48(sup1):S45-s56.
Landes SJ, McBain SA, Curran GM. An introduction to effectiveness-implementation hybrid designs. Psychiatry Res. 2019;280: 112513.
Wasserman C, Hoven CW, Wasserman D, Carli V, Sarchiapone M, Al-Halabi S, et al. Suicide prevention for youth–a mental health awareness program: lessons learned from the Saving and Empowering Young Lives in Europe (SEYLE) intervention study. BMC Public Health. 2012;12:776.
Benner AD, Boyle AE, Bakhtiari F. Understanding students’ transition to high school: demographic variation and the role of supportive relationships. J Youth Adolesc. 2017;46(10):2129–42.
Benner AD. The transition to high school: current knowledge, future directions. Educ Psychol Rev. 2011;23(3):299–328.
Thapar A, Collishaw S, Pine DS, Thapar AK. Depression in adolescence. Lancet. 2012;379(9820):1056–67.
Stein BD, Kataoka SH, Hamilton AB, Schultz D, Ryan G, Vona P, et al. School personnel perspectives on their school’s implementation of a school-based suicide prevention program. J Behav Health Serv Res. 2010;37(3):338–49.
Pettit JW, Buitron V, Green KL. Assessment and management of suicide risk in children and adolescents. Cogn Behav Pract. 2018;25(4):460–72.
Hill RM, Pettit JW. Perceived burdensomeness and suicide-related behaviors in clinical samples: current evidence and future directions. J Clin Psychol. 2014;70(7):631–43.
Padmanathan P, De Silva MJ. The acceptability and feasibility of task-sharing for mental healthcare in low and middle income countries: a systematic review. Soc Sci Med. 2013;97:82–6.
Carlson SJ, Andrews MS, Bickel GW. Measuring food insecurity and hunger in the United States: development of a national benchmark measure and prevalence estimates. J Nutr. 1999;129(2S Suppl):510s-s516.
Amir D, Valeggia C, Srinivasan M, Sugiyama LS, Dunham Y. Measuring subjective social status in children of diverse societies. PLoS ONE. 2019;14(12): e0226550.
Goodman E, Adler NE, Kawachi I, Frazier AL, Huang B, Colditz GA. Adolescents’ perceptions of social status: development and evaluation of a new indicator. Pediatrics. 2001;108(2):E31.
Goodman E, Huang B, Schafer-Kalkhoff T, Adler NE. Perceived socioeconomic status: a new type of identity that influences adolescents’ self-rated health. J Adolesc Health. 2007;41(5):479–87.
Centers for Disease Control and Prevention. Youth risk behavioral surveillance survey 2017. https://nccd.cdc.gov/youthonline/App/Results.aspx?LID=MT.
El-Behadli AF, Beitra D, Zullo L, Mbroh H, Stewart SM. Measuring thwarted belongingness and perceived burdensomeness in clinically depressed and suicidal youth: refinement and reduction of the Interpersonal Needs Questionnaire. Suicide Life Threaten Behavior. 2019;49(5):1463–72.
Goodman R, Meltzer H, Bailey V. The strengths and difficulties questionnaire: a pilot study on the validity of the self-report version. Eur Child Adolesc Psychiatry. 1998;7(3):125–30.
Fajardo-Bullon F, Rasskin-Gutman I, Leon-Del Barco B, RibeiroDosSantos EJ, Iglesias GD. International and Spanish findings in scientific literature about minors’ mental health: predictive factors using the strengths and difficulties questionnaire. Int J Environ Res Public Health. 2019;16(9):1603.
Barzilay S, Apter A, Snir A, Carli V, Hoven CW, Sarchiapone M, et al. A longitudinal examination of the interpersonal theory of suicide and effects of school-based suicide prevention interventions in a multinational study of adolescents. J Child Psychol Psychiatry. 2019;60(10):1104–11.
Forrest CB, Meltzer LJ, Marcus CL, de la Motte A, Kratchman A, Buysse DJ, et al. Development and validation of the PROMIS pediatric sleep disturbance and sleep-related impairment item banks. Sleep. 2018;41(6):zsy054.
Allgaier AK, Pietsch K, Fruhe B, Prast E, Sigl-Glockner J, Schulte-Korne G. Depression in pediatric care: is the WHO-Five Well-Being Index a valid screening instrument for children and adolescents? Gen Hosp Psychiatry. 2012;34(3):234–41.
Balazs J, Miklosi M, Kereszteny A, Hoven CW, Carli V, Wasserman C, et al. Comorbidity of physical and anxiety symptoms in adolescent: Functional fmpairment, self-rated health and subjective well-being. Int J Environ Res Public Health. 2018;15(8):1698.
Sandler IN, Tein JY, Mehta P, Wolchik S, Ayers T. Coping efficacy and psychological problems of children of divorce. Child Dev. 2000;71(4):1099–118.
Ayers TS, Sandler IN, West SG, Roosa MW. A dispositional and situational assessment of children’s coping: testing alternative models of coping. J Pers. 1996;64(4):923–58.
Boring JL, Sandler IN, Tein JY, Horan JJ, Velez CE. Children of divorce-coping with divorce: a randomized control trial of an online prevention program for youth experiencing parental divorce. J Consult Clinical Psycholol. 2015;83(5):999–1005.
Berg M, Rozental A, Johansson S, Liljethorn L, Radvogin E, Topooco N, et al. The role of knowledge in internet-based cognitive behavioural therapy for adolescent depression: Results from a randomised controlled study. Internet Interv. 2019;15:10–7.
Lubman DI, Berridge BJ, Blee F, Jorm AF, Wilson CJ, Allen NB, et al. A school-based health promotion programme to increase help-seeking for substance use and mental health problems: study protocol for a randomised controlled trial. Trials. 2016;17:393.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd edition ed. Hillsdale: Laurence Erlbaum Associates; 1988.
DeCou CR, Schumann ME. On the Iatrogenic Risk of assessing suicidality: a meta-analysis. Suicide Life Threat Behav. 2018;48(5):531–43.
Blades CA, Stritzke WGK, Page AC, Brown JD. The benefits and risks of asking research participants about suicide: a meta-analysis of the impact of exposure to suicide-related content. Clin Psychol Rev. 2018;64:1–12.
Author information
Authors and Affiliations
Contributions
RSW, BGS, and HW developed the research aims and study design; JSR developed the analysis plan; KE contributed to the development of the assessment battery and YAM training materials, the protection of human subjects plan, and Figs. 1, 2, 3. MK helped develop the research aims and liaised with the Youth Aware of Mental Health developers; All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Weissman, R.S., Scott, B.G., Edwards, K. et al. Adapting a youth suicide prevention program for rural communities in the United States: a feasibility study. Discov Psychol 4, 27 (2024). https://doi.org/10.1007/s44202-024-00140-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44202-024-00140-7