
Abstract
Purpose
Many autistic individuals experience sensory features that impact participation in healthcare. In this study, we aimed to identify the needs of autistic children during healthcare participation and, based on the findings, generate solutions to improve participation in healthcare.
Methods
A design-thinking approach with qualitative methods was used. First, observation of the environment and journey mapping were completed as part of the empathy stage of design thinking. Next, six parents of autistic children completed semi-structured interviews. The interviews were transcribed, and thematic analysis was used to identify themes. Next, healthcare providers participated in a group session to discuss experiences caring for autistic children. These data were also analyzed using qualitative methods, and themes emerged. Finally, healthcare providers and five interior design and architecture professionals reviewed the themes from both groups and the best available literature. They participated in a brainstorming session where solutions were collaboratively generated.
Results
Four main themes emerged from the parent's interviews, and three themes emerged from the healthcare provider’s input. Several solutions were identified during the brainstorming session, including a prototype for a sensory adaptive environment, sensory adaptations during medical procedures, and training for providers on sensory features in autism.
Conclusion
The design thinking method was appropriate to identify the problem and potential solutions to improve participation in healthcare for autistic children.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Autism Spectrum Disorder (ASD) is the most common neurodevelopmental disorder in childhood [4]. Up to 84% of autistic persons experience sensory features [5]. These include hyper- or hypo-reactivity to sensations such as touch, smell, movement, and sounds, unusual interest in the sensory aspects of objects and the environment, and difficulty integrating two or more sensory experiences simultaneously [5, 26, 27]. Participation in healthcare is essential to maintain optimal health and well-being. However, healthcare can be an overwhelming experience for autistic persons experiencing sensory features [11]. Stimuli in a healthcare setting, such as bright lights, sounds, smells, touch, and even pain, can generate discomfort and induce sensory overload, anxiety, and trigger stress responses that can cause unsafe behaviors and interactions [10, 30]. Further, the demands of multiple, simultaneous integration of stimuli can create challenges in understanding and following directions and other aspects of participation in healthcare. As a result, some autistic individuals and their families refrain from medical care to prevent negative behaviors and experiences, leading to poor health outcomes [30].
Most healthcare settings do not provide an environment that accommodates and supports the autistic population’s unique sensory needs [10]. Furthermore, most healthcare providers do not thoroughly understand sensory features and their impact on behavior and thus do not provide needed accommodations. This can place autistic children, their families, and providers at risk for ineffective service delivery [10].
One strategy utilized to address sensory features and improve participation in activities is the implementation of sensory adaptative environments. These adaptations are designed to allow children with sensory needs to have control of the environment and assist with self-regulation [12, 20, 21, 30]. Adaptations are thoughtfully designed and include adaptations to an existing environment or the development of a new sensory adaptive environment [9]. There is no “one-size-fits-all” solution, but rather adaptations that meet the individual’s and the facility's needs.
Wood et al. [30] and Cermak et al. [7] found that sensory adaptations in the physical environment improved participation in the emergency room and dental office settings, respectively. They discovered that adaptations such as a quiet room equipped with sensory-friendly elements, including dim lights, soothing sounds, and opportunities for pressure touch (i.e., a weighted butterfly cocoon worn during the dental visit), rocking chairs, and a variety of small manipulative hand toys, can positively impact participation and interaction. Furthermore, Cermak et al. [7] found that using this sensory-adapted equipment improved participation in dental healthcare for this population and decreased sensory discomfort and behavioral distress.
Sensory adaptations can be implemented in a variety of settings and in a variety of different ways. In their study, Wood et al. [30] implemented environmental adaptations to assist autistic individuals with sensory needs as soon as they arrived at the emergency room. These included adaptations such as alternative sitting options (ball, mat, stretcher, mat on the floor), showing a picture list of available sensory toys, and offering devices like a white noise machine during medical procedures. These feasible and low-cost adaptations helped patients safely complete medical procedures [30]. Litwin and Sellen [15] implemented sensory kits in a pediatric emergency room using a sound machine, a tablet with calming photos, small hand toys, and multiple transportable items for all sensory systems. They found a substantial need for these sensory adaptations, particularly in crowded environments and during waiting periods, and parents and participants indicated high satisfaction with the adaptations implemented during the visits.
Collaboration among stakeholders is critical for implementing sensory adaptations [7, 30]. Often, occupational therapists and interior design experts help develop unique environmental adaptations and can contribute to more successful outcomes, including increased participation in healthcare and decreased stress, anxiety, and stereotyped behaviors [21]. Design Thinking (DT) is an innovative approach that uses multidisciplinary collaboration to solve problems by generating empathy for clients [2, 8]. It is rooted in participatory design [16, 28]. DT has now been adopted in healthcare and is a preferred method for stakeholder engagement because of its collaborative, iterative process and its value for diversity to generate meaningful solutions [23, 25]. DT seeks to understand the needs through the engagement of stakeholders [2, 25]. The goal of DT is to solve complex problems efficiently, innovatively, and collaboratively to develop client-centered, meaningful solutions [2, 25].
This project aimed to identify the needs of autistic children during healthcare participation using a collaborative, innovative approach and use these data to generate solutions to improve participation during healthcare visits. The findings from this study serve as guidance to address the needs of autistic children in various settings beyond healthcare.
1 Methods
1.1 Ethical approval
Ethics approval for this project was granted by the Thomas Jefferson University Institutional Review Board in accordance with the guidelines of the Declaration of Helsinki. Informed consent was obtained from all individual participants in the study.
1.2 Study design
The project utilized qualitative methodology with a design-thinking (DT) approach to engage stakeholders in a collaborative, interactive process. Following DT methodology, which included observations of the existing environment, interviews with families, and discussion and brainstorming with the healthcare providers and design experts. Qualitative analysis was used to identify themes from parent interviews and professional discussions. This process allowed for an opportunity to collect data from multiple sources and develop responsive solutions.
1.3 Setting
This study occurred in 2021 at an autism center, part of a children’s healthcare network, and in collaboration with a large urban university. The autism center opened in late 2018 and provides pediatric developmental, psychological, and psychiatric care. The professionals at the center work closely with other specialists, such as physical, occupational, speech, and assistive technology, to create customized care plans to manage the child’s needs and promote independence [3]. The center was designed to accommodate autistic children’s needs with a visually appealing environment, clutter-free, and way-finding makers throughout. The center provides some sensory adaptations, such as adaptive seating in the waiting room and lighting adjustments, but was seeking ideas to improve participation in healthcare for the autistic population. Most of the meetings for this project took place remotely due to the COVID-19 pandemic, except for the journey map (described below), which was completed in person by the first author in collaboration with the autism center medical director.
1.4 Participants
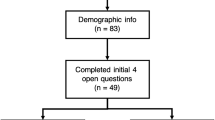
Participants included parents or caregivers of autistic children attending the autism center (n = 6), healthcare professionals (n = 15), and professionals in design and architecture (n = 5). Parents were recruited via convenience sampling from the autism center’s patient pool. Individuals received an email with the study information in English and Spanish. Interested individuals replied to the email and completed a phone screening in their preferred language to determine eligibility and to set up an interview time. Verbal informed consent of eligible participants was obtained before the interview and stored in a university password-protected file following the Institutional Review Board (IRB) standards. Parents were eligible if they had a child with a diagnosis of autism between the ages of 3 and 10 years old and were currently receiving services at the center. Autism diagnoses were made by professionals at the center who are trained and qualified in autism diagnosis. Six individuals were eligible and agreed to participate. Three identified as Caucasian, one as Black/African American, and two as Hispanic/Latino. Four participants completed interviews in English and two in Spanish.
Convenience sampling was used to recruit healthcare providers, interior designers, and architects. An email was sent, and those who replied to the email were screened, provided an overview of the project, and consented. Nine occupational therapists, three medical doctors, one nurse, one psychologist, one child life specialist, three interior designers, and two architects were eligible and agreed to participate.
1.5 Procedures
As shown in Fig. 1 below, the project followed the DT phases: Empathize, understands the user and the challenges; Define, frames the problem and the desired outcome; Ideate, seeks to generate as many solutions as possible to address the problem; Prototype, crafts potential solutions to make them tangible for testing and Test, implements the solutions identified and evaluates the effectiveness [2, 25]. In this paper, we present phase one of a two-phased project presenting findings from the stages of empathizing, defining, ideating, and prototyping. The testing phase will be part of the project's second phase and will be implemented in the future.

Design thinking approach
During the empathize stage, a journey map was developed to understand the child’s and parent’s healthcare experience. Journey mapping is a technique utilized to visualize the process one goes through to complete an activity or a goal [13]. The journey map was developed in collaboration with autism center staff to visually represent the process of the healthcare visit. The map was created using photos of the center’s physical environment and describing the usual healthcare visit steps. The journey map is shown in the results section.
Also, during the empathize stage, parent interviews were conducted via phone in English and Spanish, according to the participant’s selected preferred language. Interviews followed a semi-structured format with questions designed to learn about the experiences of participation. After learning about the child’s age, diagnosis, and frequency of visits, questions focused on learning about their experiences obtaining health care at the center. Questions such as Can you describe a typical visit? Does the visit present any challenges? Do you use any strategies when presented with a challenge? How does the experience influence your child’s behavior? Lastly, as part of this stage, the healthcare providers discussed experiences during service delivery to autistic children at the center. This group meeting occurred before the brainstorming session and differed from the parent interviews completed individually.
During the define stage, thematic analysis of the parent interview data and the provider group discussion data were completed (see data analysis for more detail). Additionally, a literature review was conducted on autism, sensory features, and participation in healthcare to inform the process further.
In the ideate stage, 15 healthcare providers, three designers, and two architects met via Zoom [31]. All professionals were English speakers. They were presented with the themes identified from the parent interviews, the themes identified by the providers, and the result of the literature review. Further, the group watched training videos on sensory integration and sensory interventions to understand sensory needs.
Collaborative brainstorming occurred in the same group session and with the same members. Two design-thinking experts guided this. One expert was the director of the design lab at an urban university, and the second expert was a member of this lab. The goal of brainstorming was to generate as many potential solutions as possible using the information available. Participants used an online collaborative whiteboard platform [17] to add pictures, use sticky notes with ideas, and make drawings.
Lastly, in the prototype stage, the DT experts guided the group through a ranking process of the ideas and solutions, discussed desirability, feasibility, and viability, and created a final prototype with the solutions.
1.6 Data analysis
Thematic analysis was used for the parent interviews and the healthcare provider group session following recommendations from Castleberry et al. [6] and Nowell et al. [18]. Interview recordings were transcribed using specialized software (Otter.ai) [19]. Transcripts were reviewed for accuracy and uploaded to the NVivo platform, a software program to organize the information, develop codes, and identify themes [29]. Data were reviewed multiple times. The rigor of the qualitative analysis was accomplished through data triangulation (implementing various sources to analyze and understand the data) [14]. Peer debriefing (a presentation and discussion of the data with a peer not involved in the project) was completed to obtain objective input [14]. Bias was reduced following the process of reflexivity [14, 18], by recording reflections on the personal views of the primary researcher and acknowledging bias.
2 Results
2.1 The journey map
The journey map is depicted below (Fig. 2). Journey mapping showed a typical visit follows six steps: (1) Transition from the home to the center. For children with sensory differences, transitions from the house to the car or public transportation to the center require preparation and can be overwhelming. (2) Arrival at the center. This is where patients sign in and wait in a waiting room area with bright lighting, a television, and a small table. Families with their children must stay in the waiting area until they are called to the vitals room. (3) Vital signs. Taking vital signs occurs in a room with two adult-size chairs, a treatment table, and adjustable lighting. Usually, toys are available in this room, but they were removed to protect sanitation during the pandemic. (4) Transition to the treatment room. In this next step, children transition to a brightly lit treatment room (lights can be dimmed if needed) with one or two tables and regular office chairs. (5) Further treatment or testing. Additional testing and intervention that may be needed are provided in the same visit for some children. This means they must transition to another treatment room with similar physical characteristics. (6) Leaving the center. In the last step, children and their families leave the room, walk through long hallways following the colored lines leading to the exit, stop at the check-out desk, and leave the center.

Journey Map. 1. Pictures taken by PI at Swank Autism Center in Wilmington, DE, 2021
2.2 Parent/caregiver themes
Four themes emerged from the parent interviews
Environment challenges in the physical and social environment interfere with participation in healthcare. About the physical environment, data revealed that additional adaptations are needed to address the unique sensory needs of autistic children. Statements such as “Bright lights [in the center] bother my son and so [it triggers unwanted behaviors]” and “The rooms are too bright, and he is sensitive to light.” indicate how physical environment features interfere with sensory needs and affect healthcare participation.
Parents identified that environmental modifications were needed to improve participation. Specific suggestions included an area with sensory items for children to take a break or self-regulate, a large variety of sensory toys and interactive objects in the exam room, and offering different colors and more natural light. “a quiet room with different color lights and bubble walls”; “Maybe if there were more sensory items available to occupy his attention while I was talking to the doctor, that would be helpful”; “They need different kinds of sensory toys to interact in the rooms.” Specific types of equipment were also identified as strategies, such as rocking and calming chairs. “they need to offer cocoon chairs and gel pads.”
Regarding the social environment, parents noted that there needs to be more training among some clinical staff on sensory differences and strategies to address them.
A second theme was regarding medical procedures. Data revealed that procedures such as measuring vital signs can be challenging and influence the appointment's course and future care. Parents expressed that “taking the temperature or blood pressure makes him react, and he can become aggressive, and he is not able to participate in the rest of the visit”; “The temperature and blood pressure and all that stuff, like that is uncomfortable for her to do”; “The blood pressure cuff starts squeezing her too hard, and she does not like that, affecting the full visit.” indicating the challenge autistic children and their families experience during the medical visit and expressing the need for adaptations to meet their unique sensory needs and complete medical procedures successfully and safely.
A third theme is specific to sensory needs. Families expressed that their children experience unique sensory needs that can interfere with a successful healthcare visit. Some of those needs include “he cannot be around people; I have to ask them for a room that is quiet,”; “sounds bother him and can make the visit difficult,”; “he is very much like a sensory seeker,” and [needs frequent stimulatory input]; “he needs frequent oral input” [to stay regulated].
The last theme was related to timing. For some parents, implementing strategies before the visit helped with self-regulation, such as “I give him my phone so that he can relax [before taking vitals].” for others, implementing strategies during the visit worked best. “I have a bag of toys with me, so I try to bring stuff to the appointments [and provide it prior to each transition].” However, for some parents, strategies worked best after the visit, such as giving the child sensory rewards for positive participation, “I use a system of [sensory-related] rewards; I tell him, okay, if you sit still during the appointment, I will buy you a pack of gum.”
2.3 Themes from healthcare provider participation
Data collected from the provider’s session was analyzed using the same qualitative approach followed by the parent interviews. The following themes were identified.
Procedures, providers expressed the importance of routine procedures such as obtaining vital signs. However, they stated experiencing challenges due to sensory sensitivities and, in some cases, decreased understanding of the medical procedures. Some statements supporting this theme include: “Taking vitals is a trigger, and the child becomes overwhelmed, making the visit very difficult”; “I need vital signs, but it makes the patient unhappy; they have difficulty understanding why certain things are happening.” All healthcare professionals agreed that sensory differences significantly interfere with procedures and the course of the visit.
Additionally, providers indicated that “long wait times can be unpredictable,” resulting in the patient having to wait longer and potentially becoming overwhelmed. Providers also indicated that “time constraints” can impact their ability to deliver additional adaptations during medical procedures or to address sensory challenges.
Providers agreed that more resources to address the sensory needs could positively impact participation. These included the “availability of more sensory-friendly seating” and “sensory strategies.” Of note, some sensory-friendly seating options were available at the center, but they were stored and out of sight during the pandemic. The providers stated that there is a “spectrum of needs,” meaning that every child has different sensory needs, and a potential variety of sensory materials and adaptations is needed for improved outcomes in healthcare visits. They also expressed the need for more staff education about the sensory features of autism and potential challenges for those providing care.
Providers agreed that modifications in the environment were necessary to improve health outcomes, describing solutions such as “having a separate and quiet space” for those who have decreased tolerance to public spaces or “a sensory adapted environment with sensory toys that are easy to clean” so children can freely interact and meet their unique needs and “dynamic lighting with varied controls” in multiple healthcare spaces. Participants also suggested adaptations to medical procedures as an essential step to improve participation and decrease negative experiences. Some suggested that “creating a social story” may prepare the child for the sensory experiences they would encounter during the medical visit. (The center was creating a social story at the time, but it had not yet been implemented). Others suggested that “asking families about triggers when taking vitals” would be a helpful strategy or “having a family member model vitals” could provide a visual model to help children understand the process of the medical procedures needed.
Further, providers expressed that communication is essential to improve care for autistic children. Some highlighted that “communication is key” to learning more about the child’s sensory needs. Others highlighted communication as being essential for healthcare providers and staff to “learn effective communication techniques” when delivering care to families of autistic children. Providers also reflected on the importance of “learning about the family’s values and goals” to deliver client-centered care that meets the child’s sensory needs and expectations for successful outcomes.
2.4 Prototype development
During the brainstorming session, three main solutions emerged: a Sensory Adaptive Environment (SAE), sensory adaptations during medical procedures, aiming vital signs (blood pressure, temperature, heart rate, weight, and height measurements), and training for providers on sensory features in autism. For the SAE, the team identified that it should be implemented in an available room near the waiting room area. Participants with a background in interior design and architecture worked with the group to provide specific suggestions on the design and accessibility. Occupational therapists who are experts on environmental adaptations and sensory integration provided input on sensory equipment and potential activities to be incorporated into the SAE. Some suggestions were also developed using the literature presented during the session. Equipment suggestions were added using pictures of the equipment on the Miro platform. Other healthcare providers provided input on feasibility and use. A final SAE prototype emerged consisting of three different zones: (1) the calming/passive zone, (2) the active/exploratory zone, (3) and the midzone/transitioning zone, as described below and shown in Fig. 3. These zones were named and described by the team during the prototype stage.

Sensory Adaptive Environment Prototype
2.4.1 The calming zone
The calming zone is designed for individuals who typically experience hyper-reactivity to sensations, mainly when presented with unfamiliar environments. The purpose of this zone is to provide a calming and relaxing environment. In this zone, the child will have access to equipment identified to provide calming sensations to facilitate self-regulatory experiences. Suggested equipment for this zone includes a lycra snuggle swing, a cushioned bubble tube base with visual elements such as fish and jellyfish, a bean bag chair, a weighted disc blanket, a fiber optic cascade, and fiber optic ceiling tiles.
2.4.2 The active/exploratory zone
This zone is designed for children who may benefit from more active participation in sensory experiences and who usually seek sensory input. The purpose of this zone is to provide an exploratory environment. Children in this zone can interact with various equipment that provides the unique sensations they seek, intending to improve self-regulation and participation in healthcare. Suggested equipment for this zone includes rocking chairs, large marble panels, activity panels, a small trampoline, a climbing wall, and a swing.
2.4.3 The midzone/transition zone
This zone is designed to be in the middle of the room with equipment that can provide calming or exploratory experiences. This zone also serves as a transition zone when children first enter the room to guide their needs and transition between the two other zones. Equipment for this zone includes a fiber optic tunnel, touch light panels, cocoon chairs, and other elements available, such as canceling headphones, tactile objects, a bin with toys (dinosaurs and cars were highly suggested by parents), and chewy tubes.
3 Discussion
Participation in healthcare can be an overwhelming experience for autistic individuals and their families due to the sensory needs of the child and the sensory features of the environment. This study aimed to use stakeholder input to learn about autistic children’s experiences when participating in healthcare and to design solutions to improve participation. We followed a design thinking approach to empathize with the participant's experiences, engage in multidisciplinary collaboration, and ultimately design innovative, human-centered solutions. The solutions identified were responsive to the user’s needs and were specific to the local autism center where the study took place. However, the identified solutions may also apply to other settings and environments. For this setting, participants noted that environmental supports and adaptations to address sensory features could make the healthcare process more successful, and three specific solutions emerged: a SAE, sensory adaptations during medical procedures, and training for providers on sensory features in autism and how they may affect healthcare delivery.
DT was a successful, innovative approach to address this problem and develop meaningful solutions. DT has been recently used in healthcare to generate creative solutions to challenging healthcare issues. The engagement of a multidisciplinary team in an innovative way can improve the utilization and acceptability of the solutions identified, increase adherence, improve outcomes, and empower stakeholders toward greater participation in research and evidence-based interventions [24]. The engagement of stakeholders in this interactive process ensured that voices were heard and that the solutions generated were responsive to the stakeholders' concerns and needs [25]. The design-thinking process provides a model for others interested in finding innovative solutions to complex and multifaceted problems.
Although there is ample literature describing the challenges of autistic individuals related to their sensory features, there is a paucity of literature describing specific environmental interventions to address these challenges for improved healthcare participation. This study detailed specific strategies and solutions that could address these sensory challenges during healthcare for this center. Importantly, each environment and setting should be considered individually, as solutions will vary based on the setting, population, and site needs. For example, a SAE with specific zones to address sensory needs may be useful in some environments but not in others. Further, it is important to have a professional, such as an occupational therapist with expertise in sensory integration, knowledgeable about the adverse effects of sensory experiences. Many autistic individuals experience both hyper-reactivity and hypo-reactivity to sensations that may influence behavior [5]. Professional support can facilitate positive outcomes and assist with transitioning from this environment back to a clinic.
Our findings are consistent with Wood et al. [30], Litwin and Sellen [15], and Cermak et al. [7], who explored adaptations to the physical and social environment to improve participation in emergency departments or dental exams for autistic individuals. They found that immediate, short-term solutions such as sensory tool kits or carts can be helpful. Similarly, our study found that implementing these adaptations was a potential solution to address the sensory needs of this population. One unique feature of the current study is that a more permanent, long-term solution was generated—creating a prototype for a permanent SAE room. This important finding might be considered in other healthcare facilities with the space and resources.
SAEs are being implemented in a variety of settings beyond medical environments. Park et al. [21] designed an SAE in a public high school with successful results. Similarly, many sports stadiums and airports now have SAE available to improve the experience of autistic children and their families in these environments [1, 22]. Given that the SAE designed in this study emerged directly from stakeholders' input by engaging them in an interactive process, it has direct relevance for the setting in which it was created. It is essential to acknowledge that each type of setting may have different goals, and the children they serve will have different sensory needs. Thus, it will be essential to design SAE according to these needs, and methods such as DT, which informs design through understanding stakeholder needs, may be an ideal approach. It may be helpful to complete a pre-visit screening with each child to identify the types of sensory activities or adaptations best suited for their sensory needs and then guide them accordingly.
One additional recommendation that emerged from the data was the importance of education for providers on sensory features and the sensory differences that many autistic persons experience. This finding is consistent with Wood et al. [30], who implemented a training program for the hospital staff introducing the concept of “sensory-informed care” for providers to learn about the sensory needs of this population as a basis for implementing strategies to address the needs. After the training, they found that providers felt more knowledgeable of their autistic patients’ sensory needs and the environmental adaptations or modifications that could support them. Thus, they reported the implementation of sensory-adapted strategies with better success. Also important is the knowledge that SAEs differ from sensory treatment rooms that trained occupational therapists use to implement individually tailored sensory-motor interventions.
4 Conclusions
Gaps persist in understanding and addressing the sensory features of autistic individuals during healthcare, and these often impact their receipt of needed healthcare services. Increased awareness of environmental adaptations and innovative approaches, such as design thinking, could substantially improve these outcomes. We share the results of this project as a valuable model for engaging stakeholders to create positive sensory experiences that can improve participation in healthcare and other essential activities.
4.1 Limitations
Limitations include that the study was conducted during the COVID-19 pandemic, limiting the availability and use of sensory items previously offered to the patients by the center. Also, the parent interviews were conducted by phone. The parents completed the interviews but did not participate in the ideate and prototype stages where the solutions were crafted. All the group meetings were conducted online. Although most participants were comfortable interacting in a virtual space, it is possible that it may have impacted some participants’ willingness to speak up. In addition, the sample of parents who participated in the interviews was small due to time constraints, which may impact generalizability. All healthcare providers were English speakers, and information was not collected on their years of experience. Finally, by design, the project was specific to the healthcare facility where the study took place. Although this increases the utility of the findings for this site, it may decrease the appropriateness for other sites.
Data availability
The data supporting this study's findings can be available upon request from the corresponding author [LRV]. The data is not publicly available because it contains information that could compromise the privacy of the research participants.
References
Allegheny County Airport Authority. Pittsburgh International Airport opens first-of-its-Kind sensory-friendly space that includes real plane cabin and seating. Fly Pittsburgh; 2019. https://flypittsburgh.com/acaa-corporate/newsroom/news-releases/pittsburgh-international-airport-opens-first-of-its-kind-sensory-friendly-space-that-includes-real-plane-cabin-and-seating/.
Altman M, Huang TT, Breland JY. Design thinking in health care. Prevent Chron Dis. 2018. https://doi.org/10.5888/pcd15.180128.
Autism Center, Delaware Valley. Nemours Children's Health. 2023. https://www.nemours.org/services/swank-autism-center.html.
Baio J, Wiggins L, Christensen DL, Maenner MJ, Daniels J, Warren Z, Kurzius-Spencer M, Zahorodny W, Robinson C, Rosenberg White T, Durkin MS, Imm P, Nikolaou L, Yeargin-Allsopp M, Lee L, Harrington R, Lopez M, Fitzgerald RT, et al. Prevalence of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites United States 2014. MMWR Surveill Summ. 2018;67(6):1–23. https://doi.org/10.15585/mmwr.ss6706a1.
Ben-Sasson A, Gal E, Fluss R, Katz-Zetler N, Cermak SA. Update of a meta-analysis of sensory symptoms in ASD: a new decade of research. J Autism Dev Disord. 2019;49(12):4974–96. https://doi.org/10.1007/s10803-019-04180-0.
Castleberry A, Nolen A. Thematic analysis of qualitative research data: is it as easy as it sounds? Curr Pharm Teach Learn. 2018;10(6):807–15. https://doi.org/10.1016/j.cptl.2018.03.019.
Cermak SA, Stein Duker LI, Williams ME, Dawson ME, Lane CJ, Polido JC. Sensory adapted dental environments to enhance oral care for children with autism spectrum disorders: a randomized controlled pilot study. J Autism Dev Disord. 2015;45(9):2876–88. https://doi.org/10.1007/s10803-015-2450-5.
Design thinking in health care. 2019. Centers for Disease Control and Prevention. https://www.cdc.gov/pcd/issues/2018/18_0128.htm.
Essary J, Park G, Adams L, Nanda U. Making a sensory cocoon: translating discrete sensory needs into a built solution with emerging digital fabrication workflows. Technol|Archit + Des. 2020;4(1):80–91. https://doi.org/10.1080/24751448.2020.1705717.
Gabriels RL, Agnew JA, Beresford C, Morrow MA, Mesibov G, Wamboldt M. Improving psychiatric hospital care for pediatric patients with autism spectrum disorders and intellectual disabilities. Autism Res Treat. 2012;2012:1–7. https://doi.org/10.1155/2012/685053.
Gurney JG, McPheeters ML, Davis MM. Parental report of health conditions and health care use among children with and without autism. Arch Pediatr Adolesc Med. 2006;160(8):825. https://doi.org/10.1001/archpedi.160.8.825.
Hill L, Trusler K, Furniss F, Lancioni G. Effects of multisensory environments on stereotyped behaviors as maintained by automatic reinforcement. J Appl Res Intellect Disabil. 2012;25(6):509–21. https://doi.org/10.1111/j.1468-3148.2012.00697.x.
Howard T. Journey mapping. Commun Des Q. 2014;2(3):10–3. https://doi.org/10.1145/2644448.2644451.
Johnson RB, Christensen L. Educational research: quantitative, qualitative, and mixed approaches. Thousand Oaks: SAGE Publications; 2019.
Litwin S, Sellen K. Designing a sensory kit to improve the environment for children with autism spectrum disorder in the pediatric emergency department. J Autism Dev Disord. 2022. https://doi.org/10.1007/s10803-022-05651-7.
Milroy JJ, Oakes LR, Hickerson BD. Design thinking: assessing the health needs of college students with intellectual and/or developmental disabilities. J Appl Res Intellect Disabil. 2021;34(6):1408–20. https://doi.org/10.1111/jar.12882.
Miro The Visual Workspace for Innovation. 2021. https://miro.com/.
Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis. Int J Qual Methods. 2017;16(1):160940691773384. https://doi.org/10.1177/1609406917733847.
Otter. (n.d.). Otter.ai [Computer software]. Retrieved March 16, 2021, from https://otter.ai/.
Pares N, Masri P, Van Wolferen G, Creed C. Achieving dialogue with children with severe autism in an adaptive multisensory interaction: the "Mediate’ project. IEEE Trans Visual Comput Graph. 2005;11(6):734–43. https://doi.org/10.1109/tvcg.2005.88.
Park G, Nanda U, Adams L, Essary J, Hoelting M. Creating and testing a sensory well-being hub for adolescents with developmental disabilities. J Inter Des. 2020;45(1):13–32. https://doi.org/10.1111/joid.12164.
Philadelphia Eagles. Eagles build state-of-the-art sensory room at Lincoln financial Field. Philadelphia Eagles; 2019. https://www.philadelphiaeagles.com/news/eagles-build-state-of-the-art-sensory-room-at-lincoln-financial-field.
Ramos AK, Trinidad N, Correa A, Rivera R. Partnering for health with Nebraska’s Latina immigrant community using design thinking process. Prog Community Health Partnersh Res Educ Act. 2016;10(2):311–8. https://doi.org/10.1353/cpr.2016.0022.
Redante RC, De Medeiros JF, Vidor G, Cruz CM, Ribeiro JL. Creative approaches and green product development: Using design thinking to promote stakeholders’ engagement. Sustain Prod Consump. 2019;19:247–56. https://doi.org/10.1016/j.spc.2019.04.006.
Roberts JP, Fisher TR, Trowbridge MJ, Bent C. A design thinking framework for healthcare management and innovation. Healthcare. 2016;4(1):11–4. https://doi.org/10.1016/j.hjdsi.2015.12.002.
Robertson CE, Baron-Cohen S. Sensory perception in autism. Nat Rev Neurosci. 2017;18(11):671–84. https://doi.org/10.1038/nrn.2017.112.
Singh JS, Bunyak G. Autism disparities: a systematic review and meta-ethnography of qualitative research. Qual Health Res. 2018;29(6):796–808. https://doi.org/10.1177/1049732318808245.
Van der Westhuizen D, Conrad N, Douglas TS, Mutsvangwa T. Engaging communities on health innovation: experiences in implementing design thinking. Int Q Community Health Educ. 2020;41(1):101–14. https://doi.org/10.1177/0272684x19900880.
Walsh M. Teaching qualitative analysis using QSR NVivo. Qual Rep. 2015. https://doi.org/10.46743/2160-3715/2003.1890.
Wood EB, Halverson A, Harrison G, Rosenkranz A. Creating a sensory-friendly pediatric emergency department. J Emerg Nurs. 2019;45(4):415–24. https://doi.org/10.1016/j.jen.2018.12.002.
Zoom Video Communications Inc. 2021. https://zoom.us/.
Acknowledgements
Thank you to the parents, providers, and design experts who participated in the study. Also, thanks to the Jefferson Autism Center of Excellence team for supporting this project and the Nemours Inpatient Rehabilitation team from the Delaware Valley for their collaborations.
Funding
Roseann C. Schaaf has received grant funding from internal and external agencies, including the National Institutes of Health and the Nancy Lurie Marks Foundation to study sensory features in autism.
Author information
Authors and Affiliations
Contributions
LRV, RD, DTD, MF, and RS participated in the study's conception and design. LRV, DTD, MF, and RS participated in the implementation of the study. LRV, AC, MF, and RS completed data analysis. LRV, AC, and RS disseminated the results. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rios-Vega, L., Carroll, A., Dumont, R. et al. Designing sensory adaptive environments to enhance participation in healthcare for autistic children. Discov Psychol 4, 22 (2024). https://doi.org/10.1007/s44202-024-00118-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44202-024-00118-5