
Abstract
Introduction
Young people in Iraq are exposed to conflict and trauma, and to alcohol references in uncensored international TV and media. Previous regional reviews indicate that alcohol is the least studied substance in Arab countries and no data on young people in Iraq were identified. Accordingly, we re-examined the scope of available literature on alcohol and Iraqi young people, including in studies where alcohol was not the primary focus.
Methods
Five major international databases (MEDLINE (OVID), Embase (OVID), PsycINFO (OVID), Scopus, Web of Science) and one local Iraqi database (Iraqi Academic Scientific Journals (IASJ)) were systematically searched for published articles up to 16 September 2019. Original articles that included any alcohol data on general Iraqi young or student samples were included.
Results
Thirteen articles met the inclusion criteria from a total of 3374 results. All studies were cross-sectional and quantitative. Most alcohol data were incidental rather than the focus of the studies. All but two studies used face-to-face or pen-and-paper surveys. Each study reported on alcohol differently—with most not using validated tools. A wide range of drinking prevalence was reported (2.2%–23.7%). Studies reported a relatively high rate (12.2–56%) of alcohol misuse among those that drink. Alcohol was associated with risky behaviour in the two studies that reported on this measure.
Conclusion
Results suggest a low prevalence of drinking compared to non-Muslim Majority Countries (non-MMCs), and a relatively high prevalence of risk amongst drinkers. More research is needed using study methods and validated screening or diagnostic tools tailored for the local Iraqi context.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Globally, alcohol is the leading risk factor for people aged between 15 and 49 [1]. Harmful alcohol use has been associated with conflict exposure [2, 3] and other mental health conditions such as post-traumatic stress disorder (PTSD) [4]. Iraq is a nation that has been exposed to international and civil war for the past four decades. Most of Iraq’s population is under the age of 24 [5], and exposed to civil war, directly or through family or community involvement [6]. In addition, Iraqi young people are influenced by conflicting principles and cultures—that of their home cultures and religions and that which they are exposed to with no censorship on television, social and mass media [6]. For example, local Iraqi traditions prohibit alcohol use while alcohol is commonly presented as a positive and sophisticated commodity in international entertainment channels and by social media users online. Although each of these challenges may be present in other Muslim majority countries (MMCs), the combination of these factors in Iraq is unique—especially given the diversity inherent in its deep cultural tradition [6].
Alcohol is legal to consume, import and trade in Iraq on a federal level—with restrictions on the religion of the licensee, hours of operation and proximity to mosques, hospitals and schools. There have been several prohibition orders or other restrictions on a local or provincial level, however alcohol is still sold in pubs, clubs and alcohol stores around the country—mainly in large metropolitan areas that have non-Muslim minorities such as Baghdad and Erbil. For example, Erbil’s Ainkawa district with a majority Christian population has several alcohol stores, pubs and clubs. Major hotel chains and five-star establishments in Erbil also serve alcohol to their clients. In more conservative areas, alcohol is either forbidden legally or harder to access due to religious and cultural prohibition [7].
Little is known about alcohol use in MMCs, especially within the Eastern Mediterranean region. However, despite being known for their the low prevalence of alcohol use, the last World Health Organization pattern of drinking score in 2006 listed Muslim Middle Eastern countries as having the second riskiest pattern of drinking after the former Soviet countries of Eastern Europe [8]. Similarly, in 2016, among drinkers, the highest alcohol per capita consumption was in the Eastern Mediterranean region [9]. In Arab countries, research about alcohol was less than research about other substances including illicit and abused prescription drugs [10]. Previous reviews have investigated alcohol policy approaches in MMCs [11] as well as prevalence of drinking in the Eastern Mediterranean [12] and Arab gulf region [13]. In Iraq specifically, a previous review has investigated alcohol’s place in Iraq’s history, cultures, and societies [6]. However, none of these reviews outline the scope of existing academic literature around alcohol use, misuse, and policy in Iraq—including in relation to young people. For example, Ghandour, Chalak, El-Aily, Yassin, Nakkash, Tauk, El Salibi, Heffron, Afifi [12] found no study matching their inclusion criteria that describes alcohol use among young people or students in Iraq. This may be for several reasons—firstly, data about alcohol may be found in studies that focus on other research areas such as smoking, risky behaviours, and other mental health conditions. These articles may employ a general sample, not specified by age or student status. Finally, other studies may be published in local journals which may not always be identified in general academic searches.
To remedy these gaps, we conducted a systematic scoping review to identify all articles about alcohol use, misuse or attitudes among young people or students in Iraq. Our objective was to identify what is known about attitudes towards alcohol and prevalence of drinking among young people in Iraq. To meet this objective, this review will consider:
-
1.
What studies on the prevalence of alcohol consumption or attitudes of young people towards alcohol have been undertaken in Iraq?
-
2.
What definitions, questionnaires, tests, diagnostic processes, and outcomes did the studies employ?
-
3.
When and if available, how were influencing factors (such as war, globalisation, etc.) assessed in relation to alcohol use?
-
4.
What, and if available, when, preventative strategies have been implemented and evaluated that address the issues related to alcohol in this population?
2 Methods
This systematic scoping review [14] intends to describe the available literature about alcohol in young populations in Iraq. This will include any literature regarding alcohol—including quantitative and qualitative studies that explore alcohol awareness or attitudes to alcohol, and prevalence of use, misuse, and dependence. By selecting a wide scope, we aim to capture as much as possible of the scarce literature about this topic.
This review utilised the condition, context, population (CoCoPop) approach instead of the traditional approach: population, intervention, condition, outcome (PICO) [15]. PICO is typically used in studies that investigate an intervention and outcome. This study’s main objective however is to assess the prevalence of alcohol use and misuse and it does not asses any interventions or outcomes.
Condition:Prevalence of drinking/Attitude towards alcohol.
Context:Iraq.
Population:Young/Student populations in Iraq.
2.1 Identifying the relevant studies
In keeping with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement [16], a systematic search of six major health and multi-discipline databases was undertaken (see Additional file 1: Appendix S1 for PRISMA checklist). Five major international databases and one local Iraqi database were searched for published articles up until the literature search was conducted on 13th of September 2019. These databases were MEDLINE (OVID), Embase (OVID), PsycINFO (OVID), Scopus, Web of Science, and Iraqi Academic Scientific Journals (IASJ). No earliest year of publication was included in this search. The search terms were Iraq AND alcohol* OR substance *use OR drinking. The asterisk denotes the inclusion of any iteration of “alcohol” and “use” including alcoholism, misuse and abuse. A detailed search strategy is included in the appendix (Additional file 2: Appendix S2). The breadth of this search was purposely selected to identify any literature that included alcohol data.
Further hand-searched articles, identified via consultation with academics and the reference lists of the included articles, were also screened for eligibility.
Only English literature was searched. This is because English is the main language of medical research and education in Iraq. Arabic and Kurdish sources either do not exist, are limited or not accessible.
2.2 Study selection
Original peer-reviewed journal articles conducted in Iraq with an Iraqi general or student sample containing alcohol-specific data provided by age or student status were included (Table 1).
2.3 Charting the data
The aims, methods, and results of each included article were described in a spreadsheet. This included: the main focus, data collection year, sample identifiers (size, type, sampling method), setting (university, school, clinic, etc.), method of data-collection (online, pen-and-paper, etc.), tools and any criterion (AUDIT, etc.), lifetime or past-year prevalence and any other relevant quantitative or qualitative results (if any).
2.4 Patient and public involvement statement
There was no patient or public involvement in this research.
3 Results
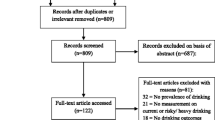
The search resulted in 3374 articles, of which 1668 were duplicates. None of the papers found in IASJ were indexed in the other databases. After a title and abstract screen, 64 articles remained and were included in the full-text screen. Eight of these studies met the inclusion criteria. Five hand-searched articles also met the criteria (Fig. 1), resulting in a total of 13 included studies.

PRISMA flow chart for literature search
3.1 Study descriptions
3.1.1 Research topics
Descriptions of the studies are reported in Table 2. Of the included studies, only four were alcohol specific [17,18,19,20]; two were about substance use [21, 22] and two about health risk behaviours [23, 24]; one each was primarily focused on mental health disorders [25], smoking [26], novel psychoactive drugs [27], risky driving [28], and sleep disorders [29]. No literature was found that related to preventative strategies in relation to alcohol.
3.1.2 Study years
Although no earliest year limits were placed in the search, all the papers were published between 2009 and 2018 with data collected from 2005 to 2017.
3.1.3 Study settings and data collection
Only one study recruited a sample from more than one province [25]. Four studies recruited from Baghdad [19,20,21, 27] and Erbil [17, 22, 23, 28]. Two recruited students from Karbala [18, 26]. Kirkuk [24] and Dohuk [29] were the recruitment sites of one study. Figure 2 identifies provinces where recruitment occurred on the Iraqi map.
All studies were cross-sectional and quantitative. Nine studies were self-administered surveys [17,18,19, 23, 24, 26,27,28,29]—eight of these were paper-and-pen and one online [27]. Three studies used face-to-face interviews [21, 22, 25] and one used autopsy blood samples [20]. Eight studies were conducted in school or college [17,18,19, 23, 24, 26, 28, 29], two at home [22, 25], one each at a youth centre [21], online [27] and at a forensics laboratory [20].
Three of the four alcohol-specific studies were self-administered pen-and-paper surveys conducted in school/college and the fourth was a post-mortem blood alcohol concentration (BAC) study.

Provinces where student/youth specific alcohol data are reported in peer-reviewed original articles. No data has been reported from unshaded (white) provinces (n = 13). The five shaded provinces have had alcohol/youth specific alcohol data. The darker the shade, the more studies conducted in that province (see key in top left of Fig. 2) [map sourced from https://d-maps.com/carte.php?num_car=26317&lang=en]
3.1.4 Alcohol screening and diagnostic processes
Only four of the eleven studies reporting alcohol prevalence or patterns data reported using validated alcohol screening or diagnostic tools. Two used the Composite International Diagnostic Interview [21, 25, 30], one used the Alcohol Use Disorders Identification Test (AUDIT) [18, 31], and one the Mini International Neuropsychiatric Interview (MINI) [22, 32]. One study utilised blood alcohol concentration at autopsy [20]. The other studies did not report how alcohol questions were asked.
3.1.5 Samples
Ten of the studies reported randomised recruitment with varying levels of detail. Ten studies included a student sample: four were general university samples [17,18,19, 26], three were medical students [27,28,29], two secondary school [23, 24] and one did not specify [22]. Although Ali, Sabir [17] defined their sample as medical college students, it included students studying medicine, dentistry, pharmacy and nursing. Similarly, Al-Ameri, Abd Al-Badri, Lafta [19] defined medical students as those studying medicine, dentistry or pharmacy. Of the other three studies, one was a general household sample [25], one a youth centre sample [21] and the third a sample of general autopsies [20].
Two samples were male only [23, 24], two had a majority male sample [17, 21] and six a majority female sample [18, 19, 26,27,28,29]. The other three studies did not provide gender breakdown for young or student subsamples.
3.2 Prevalence and patterns of alcohol use
3.2.1 Lifetime drinking
Alcohol-related results of each study are reported in Table 3. There was a wide variation in reported prevalence of drinking between studies. Two studies reported prevalence of lifetime alcohol use at 7.6% and 9.7% [19, 24]. Al-Ameri, Abd Al-Badri, Lafta [19] provides a breakdown by gender, showing the vast majority of those that drink are males (19.7% vs 0.8%). On multivariable analysis, lifetime alcohol users more likely lived away from family (prevalence ratio [PR] 2.7; 95% CI 1.8–4.1); p < 0.001 vs. those who lived with family) and were non-medical students [PR 2.6; 95% CI 1.4–4.7; p 0.002 vs. medical students (medicine, dentistry or pharmacy)] [19].
Baker, Al-Doski [23] and Al-Imam, Al-Mukhtar, Shafiq, Irfan [27] also provide alcohol use prevalence (6.6% and 0.9% respectively) without specifying if the figure is for current or lifetime drinking. Although Baker and Al-Doski’s total sample is 500 students, they only provide the drinking prevalence for the 296 students who reported any risk behaviours. Age of onset of drinking for a student or age-specific sample was only reported by one secondary school study: 12 years old (unspecified if mode, median or mean) [24].
3.2.2 Current drinking
Similarly, the prevalence of current drinking varied widely, from 2.2% [18] to 23.7% [17]. Each study reporting current drinking recruited individuals from a different setting and used different methods for data collection. The two Kurdistan studies, conducted in Erbil and Dohuk, had the highest prevalence at 23.7% and 11.9%, respectively [17, 29]. In contrast, the study in Karbala, a conservative Arab city in central Iraq, reported 2.2% [18]. Al-Qazzaz, Al-Saffar, Al-Rubai, Al-Qazzaz [20] reported the post-mortem blood alcohol levels in 14–34-year-old Iraqis who were sent for autopsy in Baghdad. A twelfth (8.5%) of the sample had a blood alcohol concentration of more than 40 mg/100 mL (0.04 g/dL).
In their study about sleep, Abdulah, Piro [29] report that evening drinking was a predictor of emotional disturbance (p = 0.034) and restless legs syndrome during the night (p = 0.003).
3.2.3 Alcohol misuse including abuse and dependence
Five studies reported data on alcohol misuse, with four using validated screening or diagnostic tools. Al Mousawi [18] reports that the majority (56%) of drinking students who completed AUDIT scored above eight (0.8% of entire sample).Footnote 1 A third (36%) of drinkers who completed AUDIT were hazardous drinkers (8–15), a tenth (10.7%) risky drinkers (16–19) and a tenth (9.3%) were high-risk or dependent (20+). Al Mousawi [18] comments that items 7 (guilt) and 10 (others concerned about your drinking) of the AUDIT may be interpreted differently in the Iraqi context. This is because guilt is common as a reaction to breaking a religious or cultural taboo. Similarly, any drinking in this context will typically make other people worried about the drinker’s behaviour even if it does not necessarily represent high-risk or dependence.
Al-Ameri, Abd Al-Badri, Lafta [19] reported that 1.2% (12.2% of drinkers) of the Baghdad student sample were heavy/high risk drinkers (consumed 3 + standard drinks [10 g ethanol] per day/7 + per week for women; 4 + per day/14 + per week for men). Similarly, A fifth (19.8%) of the student drinkers in Karbala consumed more than 4 drinks per drinking day [18]. Almost half (46%) of the fifty students who answered AUDIT question 3 in Karbala reported consuming 6 + drinks on a weekly or daily basis [18].
Despite the occurrence of episodic heavy drinking among drinkers, reported prevalence of “alcohol use disorders” among the whole population is low. A national household study from 2006, the Iraqi Mental Health Survey (IMHS), showed only 0.7% of those aged 18–34 met DSM-IV lifetime criteria for alcohol abuse and 0.3% met criteria for dependence [25]. Similarly, in Baghdad, Al-Imam, Al-Mukhtar, Shafiq, Irfan [27] reported that 0.4% (50% of drinkers) had alcohol use disorder (criteria not provided). In contrast, in Erbil, six students (6.2% of students) met the DSM-IV criteria for past-12-month alcohol abuse and two (2.5%) for dependence [22]. In a youth centre sample in Baghdad, 20.1% of 18–35-year-olds met DSM-IV criteria for lifetime alcohol abuse (no female reported drinking) [21]. Although the article does not provide specific details about the nature of the youth centre attendees, this higher figure suggests that this was most likely a high-risk group, and not representative of the general population.
3.2.4 Reliability and validity analysis of alcohol screening/survey tools
Al Mousawi [18] is the only study that conducted an internal reliability test of its alcohol screening tool in an Iraqi sample. The AUDIT had a Cronbach’s α of 0.66. However, when the guilt question was removed, the reliability increased to α = 0.73.
The Shabila et al. (2015) survey showed good internal consistency (α = 0.78 to 0.82) for a broad range of risky driving behaviours. Abdulah, Piro [29] reported the internal consistency of SLEEP-50 (a survey in relation to sleep consisting of 50 items, that only includes one alcohol question) in previous non-Iraqi international studies. Other studies did not measure internal consistency of their survey tools.
3.3 Patterns/locations
3.3.1 Frequency of drinking
Drinkers in Iraq mostly reported consuming alcohol infrequently. Student drinkers mostly reported drinking ‘occasionally’ in Erbil (81.5%) [17] and Baghdad (64%) [19]. Neither study defined what is meant by ‘occasional’ drinking. Al Mousawi [18] reports that 40.8% of drinking students in Karbala had alcohol once monthly or less often. A minority (5.8%) of students in Kirkuk reported regular drinking (frequency undefined) [24].
3.3.2 Drinking locations
The only study to report on drinking locations was from Erbil. Students most frequently consumed alcohol in bars or restaurant (44.5%) followed by outdoor settings (25.9%). Only 7.6% of current drinkers drank at home [17].
3.4 Attitudes, behaviours, and motives
3.4.1 Attitudes
Only one, smoking-focused study reported on attitudes to alcohol. Two percent of the students had positive attitudes to alcohol (compared with 2% to illicit drugs and 10% to smoking). Smokers had more positive attitudes to drinking (p < 0.001) [26]. An overall negative attitude towards alcohol is also seen with half of student drinkers in Karbala reporting guilt about their drinking (54.4%) or that people expressed concern about their drinking (49.1%) [18].
3.4.2 Motives
Only one study reported on the motive for drinking. Most students (51.9%) reported they drink for pleasure while 44.4% drink to get relief from stress [17].
3.4.3 Behaviours
Alcohol-related risk behaviours were reported by two studies. The first reported that most students perceived either driving after ‘mild to moderate’ drinking (80.1%) or drunk driving (72.5%) to be the riskiest driving behaviours. Despite this, some students reported driving after drinking (after a ‘mild to moderate intake of alcohol’ 4.5%; or whilst drunk, 6.4%). Further, almost a tenth reported finding driving under the influence of alcohol enjoyable [28]. In Kirkuk, Saeed [24] reports 6.5% of the student sample had ridden more than once in a car driven by someone who has consumed alcohol. About one third (30.6%) of the secondary school students have also driven a vehicle while drinking alcohol.
This latter statement however is internally inconsistent with the reported 7.6% lifetime use of alcohol in the same study. The abstract of this study also contains a statement that more than half (52.5%) of the students were in a vehicle driven by a drinking person. However, these results are not included in the paper itself. Saeed [24] also reported that alcohol is associated with carrying a weapon (n = 15, p 0.014) and physical fighting (n = 20, p < 0.001).
4 Discussion
This systematic scoping review is the first review on prevalence, patterns, and attitudes of alcohol use in Iraq and to our knowledge, is the first review of student or youth drinking in any MMC. The search methods employed identified alcohol-related data on young Iraqis in local and international peer-reviewed academic literature. Thirteen articles were included. Most had a non-alcohol focus and reported alcohol data incidentally.
A wide range of prevalence was reported for lifetime and current alcohol use and misuse. Less than half the studies employed validated tools to assess alcohol use. Most articles did not document how they asked about alcohol. Similarly, most authors either do not report whether they asked about lifetime or current drinking, or how they determined that participants had “alcohol use disorders” or were “heavy/binge” users and what pattern of drinking each of these terms represents. This makes these results harder to interpret. Accordingly, no clear pattern of drinking can be discerned in these Iraqi young and student samples. However, generally, a higher prevalence of alcohol use was reported by samples from Kurdistan (North Iraq). This is consistent with data from Iraq’s 2015 household survey that found alcohol consumption is highest in the Northern governorates and lowest in the South [33].
All included studies reporting prevalence of consumption by sex, showed a significantly higher prevalence of alcohol use or misuse by male participants—with two studies indicating no female use. The prevalence of female consumption is also low in other Iraqi general population studies with self-report data including the national household surveys [34, 35]. In contrast, the one study employing the objective measure of post-mortem blood alcohol concentration shows a higher percent of females overall with BAC of over 40 mg/100 mL (12.2% vs 8.4% males with BAC above 40 mg/100 mL) [20]. In this sample, there were 1136 males and only 139 females, and 91.4% of the females had died from a traumatic event (vs 78.4% of males). One explanation for this discrepancy could be that Iraqis, by observation, are more protective of their female relatives—and some may be less likely to consent for their female relatives to undergo post-mortem examination except where it is legally required. It is possible that the study has an over-representation of females who have either been victims of abuse and trauma or who are abandoned by their families. Nonetheless, it reveals that female consumption of alcohol exists in Iraq and is associated with harms including death. In the study, there was a significant relation between traumatic death and higher consumption (p = 0.007) [20].
Studies assessing drinking in this context to date have mostly used in-home or in-class self-reported pen-and-paper surveys or face-to-face interviews. The sensitivity of alcohol use in MMCs makes it particularly difficult for young people or females to disclose behaviours or attitudes that go against societal norms. Previous studies have indicated under-reporting of alcohol consumption in MMCs and particularly in Iraq [34]. A systematic review and meta-analysis of 62 prevalence studies from neighbouring Iran also indicates a large variance in reported lifetime drinking by different studies (0.03% to 68.0%; mean: 13%) – all showing higher consumption by male participants. These variations have been similarly attributed to differences in study designs, methods and samples [36].
Although prevalence of alcohol use is low in Iraq compared to some other MMCs such as Lebanon [37] and non-MMCs such as Australia [38], the prevalence of alcohol misuse is high among those who drink. This is clear in all studies that report on both alcohol use and misuse. Most strikingly, the IMHS [25] showed only 0.7% of those aged 18–34 had an alcohol use disorder and 0.3% had dependence. However, among drinkers of all ages, 45.7% met criteria for ICD-11 alcohol use disorders, with 32.1% harmful use and 13.7% dependence (compared to 33.3%, 26.6% and 6.8% respectively in Australia) [39]. In keeping with these findings, the 2015 Survey of Substance Abuse in Iraq (SSAI) showed that 71% of current drinkers met criteria for dependence on the Severity of Dependence Scale (SDS) [33]. Interestingly, Iraq had the highest prevalence of AUDs among drinkers from all ten countries included in WHO’s World Mental Health Surveys [39]. This is in line with the World Health Organization pattern of drinking score that showed Muslim countries in the Middle East have the second riskiest pattern of drinking after the former Soviet countries of Eastern Europe [8] and that the Eastern Mediterranean region has the highest alcohol per capita consumption among drinkers globally [9].
These high prevalence of dependence among drinkers are worrying. However, Al Mousawi [18] highlighted the potential for screening or diagnostic tools to be culturally biased. For example, items 7 (guilt) and 10 (worry of others about your drinking) of AUDIT may be more highly endorsed by Muslim respondents. This is most likely because of religious, social, and cultural prohibition. Drinkers may feel guilty and trigger the worry of family and friends even if they consume alcohol in only small amounts. Similarly, the SDS includes items such as “How much did you worry about your use of the drug?” which may also provide false positive results for dependence. This illustrates the importance of tailoring tools and interventions for MMCs.
Ali, Sabir [17] reported that students used alcohol for pleasure (51.9%) or to relieve stress (44.4%) and Al Mousawi [26] reported 2% of students view alcohol positively (with no further details). Other than these two studies, there is no data on influencing factors, attitudes towards alcohol or preventative strategies. Given Iraq’s history of exposure to globalisation and war, an understanding of factors influencing drinking is key to understand and predict trends among young Iraqis.
No study reported on harm-reduction or treatment initiatives and measures in Iraq. Iraq has no clear written or implemented alcohol policy, strategy or harm reduction initiatives [6, 11]. This is despite at least three studies from diverse cities showing young people dying or placing themselves and others at risk while under the influence of alcohol [20, 24, 28]. This is another area that warrants further investigation.
All studies other than the national IMHS [25] report no funding. This is because medical and health research only began after 2003 and there are no current major government grant cycles. Most funded research such as the IMHS or SSAI are either directly managed and funded by the Ministry of Health or externally funded by international organisations [25, 34]. However, because Iraq is now a high-middle income country, it is no longer eligible for most international government and non-governmental organisational funding initiatives. In addition, recent wars in Iraq have had a major impact on the national burden of disease. These factors impede Iraq’s ability to further progress in health research especially in areas such as alcohol.
4.1 Limitations
This study was limited to only include studies in English. Although, to our knowledge, there are no alcohol-specific data published in the Arabic language because English is the main language of medical and scientific research in Iraq. A meta-analysis of the data could not be conducted because each study reported on alcohol differently (most using their own measures). We were limited in our ability to compare figures for specific demographics because the studies did not describe their sample adequately. Because this is a scoping review, limited assessment was made on the quality of the included studies. Despite this, clear weakness of the methods and reporting of some studies were noted in this review. This study was limited to original journal articles published in peer-reviewed academic journals—this meant that age-specific data for the SSAI was not included as these had been published in a report, but not in refereed journals. Although the Al-Qazzaz, Al-Saffar, Al-Rubai, Al-Qazzaz [20] paper fits within our scope and was included, the sample differed from the other included studies as it was based on blood samples of autopsies.
4.2 Conclusion
Alcohol research is limited in all MMCs, including Iraq. This review shows that most alcohol data is incidental rather than the focus of the studies. No clear picture of the prevalence of drinking or attitudes towards alcohol among young Iraqis can be drawn. However, the results indicate that Iraq is not immune to health concerns resulting from alcohol use. The high rates of heavy use and misuse among those who consume alcohol as well as the alcohol-related risk behaviour among students are cause for concern. More research is needed, particularly to understand the concerns, needs and experiences of young people and their relationship with alcohol, and ways to effectively prevent or intervene for AUDs. To achieve this effectively, study methods, screening or diagnostic tools, preventive and therapeutic interventions should be tailored for the local Iraqi context.
Notes
An AUDIT score above 8 indicates risky drinking. This could range from hazardous use through to high-risk or likely dependence (Babor, 2001).
References
GBD 2016 Alcohol Collaborators. Alcohol use and burden for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2018;392(10152):1015–1035.
Lo J, Patel P, Shultz JM, Ezard N, Roberts B. A systematic review on harmful alcohol use among civilian populations affected by armed conflict in low- and middle-income countries. Subst Use Misuse. 2017;52(11):1494–510.
Roberts B, Ezard N. Why are we not doing more for alcohol use disorder among conflict-affected populations? Addiction. 2015;110(6):889–90.
Debell F, Fear NT, Head M, et al. A systematic review of the comorbidity between PTSD and alcohol misuse. Soc Psychiatry Psychiatr Epidemiol. 2014;49(9):1401–25.
UNDESA. World Population Prospects: The 2017 Revision, Key Findings and Advance Tables. 2017.
Al Ansari M, Dawson A, Conigrave K. Alcohol: from Mesopotamia to Modern Iraq. J Ethn Subst Abuse. 2019;9:1–23.
Al AM. Attitudes of Youth Towards Alcohol in Muslim Majority Countries: Insights from Iraq. Sydney: University of Sydney School of Public Health, The University of Sydney; 2020.
WHO. Interpersonal Violence and Alcohol. Geneva: WHO; 2006.
WHO. Global status report on alcohol and health. Geneva; 2018.
Sweileh WM, Zyoud SH, Al-Jabi SW, Sawalha AF. Substance use disorders in Arab countries: research activity and bibliometric analysis. Substance Abuse Treat Prevent Policy. 2014;9:33.
Al-Ansari B, Thow A-M, Day CA, Conigrave KM. Extent of alcohol prohibition in civil policy in muslim majority countries: the impact of globalization. Addiction. 2015;111(10):1703–13.
Ghandour L, Chalak A, El-Aily A, et al. Alcohol consumption in the Arab region: What do we know, why does it matter, and what are the policy implications for youth harm reduction? Int J Drug Policy. 2016;28:10–33.
AlMarri TSK, Oei TPS. Alcohol and substance use in the Arabian Gulf region: a review. Int J Psychol. 2009;44(3):222–33.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Munn Z, Stern C, Aromataris E, Lockwood C, Jordan Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Methodol. 2018;18(1):5–5.
Moher D, Liberati A, Tetzlaff J, Altman DG, Then PG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. PLOS Med. 2009;6(7):e1000097.
Ali S, Sabir J. Prevalence of alcohol use among medical college students in Hawler Medical University. Zanko J Med Sci. 2009;13(1):17–23.
Al MA. Alcohol use disorder identification test use in Muslim countries. IJPTSUD. 2015;1(3–4):79–92.
Al-Ameri R, Abd Al-Badri HJ, Lafta RK. Prevalence of alcohol consumption among university students in Baghdad: a cross-section survey from Iraq. Epidemiol Biostat Public Health. 2016;13(4):8.
Al-Qazzaz MA, Al-Saffar AJ, Al-Rubai HK, Al-Qazzaz EM. Evaluation of alcohol concentrations in samples referred to the forensic Laboratory in Baghdad. Egypt J Forensic Sci. 2017;7(1):27.
Al-Hemiary N, Hashim M, Al-Diwan J, Abdul RE. Alcohol and drug abuse in post-conflict Iraq. J Fac Med. 2015;57(4):291–5.
Rahim TA. Rate of alcohol and substance use disorders among the journalists in Erbil City. Arab J Psychiatry. 2010;21(1):50–60.
Baker JMA, Al-Doski NAS. Health risk behaviors among male students in secondary schools in Erbil city. Zanco J Med Sci. 2016;20(1):1199–205.
Saeed HM. Assessment of the health risk behavior in young adulthood: a school-based health study in Kirkuk City / Iraq. Med J Tikrit University. 2016;21(2):172–81.
Alhasnawi S, Sadik S, Rasheed M, et al. The prevalence and correlates of DSM-IV disorders in the Iraq Mental Health Survey (IMHS). World Psychiatry. 2009;8(2):97–109.
Al MA. The prevalence of smoking among karbala/iraq university students in iraq in 2005. Tobacco Use Insights. 2014;7:9–14.
Al-Imam A, Al-Mukhtar F, Shafiq A, Irfan M. Knowledge and (Ab)use in connection with novel psychoactive substances: a cross-sectional analysis of Iraqi medical students. Global J Health Sci. 2017;9(11):61.
Shabila NP, Ismail KH, Saleh AM, Al-Hadithi TS. Risky driving behaviours among medical students in Erbil Iraq. Sultan Qaboos Univ Med J. 2015;15(3):e390–7.
Abdulah DM, Piro RS. Sleep disorders as primary and secondary factors in relation with daily functioning in medical students. Ann Saudi Med. 2018;38(1):57–64.
Kessler RC, Üstün TB. The world mental health (WMH) survey initiative version of the world health organization (WHO) composite international diagnostic interview (CIDI). Int J Methods Psychiatr Res. 2004;13(2):93–121.
Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care. Geneva: World Health Organization; 2001.
Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (MINI): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;8:89.
US Department of State, Bureau of International Narcotics and Law Enforcement Affairs, Iraqi Society of Addiction Medicine, University of California LA, Center for Human Services. Survey of Substance Abuse in Iraq. Bethesda; 2015.
Al-Hemiery N, Dabbagh R, Hashim MT, et al. Self-reported substance use in Iraq: findings from the Iraqi National Household Survey of Alcohol and Drug Use, 2014. Addiction. 2017;112(8):1470–9.
WHO. Iraq Mental Health Survey 2006/7. Baghdad: World Health Organization; 2009.
Chegeni M, Kamel Khodabandeh A, Karamouzian M, Shokoohi M, Abedi L, Khalili M, Rajaei L, Ardalan G, Sharifi H (2020) Alcohol consumption in Iran: a systematic review and meta-analysis of the literature. Drug Alcohol Rev 39(5):525–538. https://doi.org/10.1111/dar.13093
Karam EG, Maalouf WE, Ghandour LA. Alcohol use among university students in Lebanon: prevalence, trends and covariates: The IDRAC University Substance Use Monitoring Study (1991 and 1999). Drug Alcohol Depend. 2004;76(3):273–86.
AIHW. Alcohol, tobacco & other drugs in Australia. Canberra: Australian Institute of Health Welfare; 2020.
Degenhardt L, Bharat C, Bruno R, et al. Concordance between the diagnostic guidelines for alcohol and cannabis use disorders in the draft ICD-11 and other classification systems: analysis of data from the WHO’s World Mental Health Surveys. Addiction. 2019;114(3):534–52.
Acknowledgements
We would like to thank Elaine Tam, Academic Liaison Librarian at the University of Sydney for her help with the literature search for this paper.
Author information
Authors and Affiliations
Contributions
MA conducted the systematic literature search, analysis and write up of the manuscript under supervision of authors KC and AD. All authors contributed to the discussion and reviewed the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
There are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Additional file 1.
PRISMA checklist.
Additional file 2.
Detailed search strategy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Al Ansari, M., Dawson, A. & Conigrave, K. Alcohol among young people in Iraq: a systematic scoping review. Discov Psychol 2, 16 (2022). https://doi.org/10.1007/s44202-022-00024-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44202-022-00024-8