
Abstract
Introduction
Tibial torsion can be measured by various clinical and radiological methods. Computed tomography (CT) scan measurement is currently the investigation of choice. The purpose of our study was to compare the clinical and CT scan methods to reveal malrotation after nailing of tibia and also to find out if leg position for distal locking has any influence on incidence of malrotation.
Materials and methods
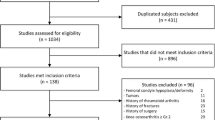
We have included 106 patients (21–68 years) of tibia nailing, and categorised them as category A (figure of four position n = 54) and category B (knee straight position n = 52) based on limb position for distal locking. The plumb line measurement, Thigh Foot Axis (TFA) and CT scan measurement (using new reference line) were documented and compared with the uninjured limb.
Results
We observed plumb line measurement to be the most inaccurate method followed by TFA method. CT scan measurement was the most accurate method showing external rotations (> 10º) in 32 cases (30.1%) and internal rotation (> − 10º) in five cases (4.71%). The TFA method had a sensitivity of 44% and specificity of 86% in identifying malrotations. The interobserver reliability for CT scan measurement was 0.96. Even though statistically not significant (P value), figure of four position for distal locking leads to larger number of malrotations (both external and internal rotation).
Conclusion
CT scan is the most accurate method of measuring malrotation. The new reference line used in our study provides accurate measurement of malrotation. The two different positions of leg for distal locking do not have a statistically significant influence on incidence of malrotation.




Similar content being viewed by others


References
Mullaji, A. B., & Sharma, A. K. (2008). Tibial torsion in non-arthritic Indian adults: A computer tomography study of 100 limbs. Indian Journal of Orthopaedics, 42, 309–313.
Staheli, L. T., Corbett, M., Wyss, C., & King, H. (1985). Lower-extremity rotational problems in children. Normal values to guide management. The Journal of Bone and Joint Surgery, 67, 39–47.
Kahn, K. M., & Beals, R. K. (2002). Malrotation after locked intramedullary tibial nailing: Three case reports and review of the literature. Journal of Trauma, 53, 549–552.
Jend, H. H., Heller, M., Dallek, M., & Schoettle, H. (1981). Measurement of tibial torsion by computer tomography. Acta Radiologica Diagnosis, 22, 271–276.
Reikaras, O., & Hoiseth, A. (1989). Torsion of the leg determined by computed tomography. Acta Orthopaedica Scandinavica, 60, 330–333.
Yoshioka, Y., Siu, D. W., Scudamore, R. A., & Cooke, T. D. (1989). Tibial anatomy and functional axes. Journal of Orthopaedic Research, 7, 132–137.
Hutter, C. G., Jr., & Scott, W. (1949). Tibial torsion. Journal of Bone and Joint Surgery. American Volume, 31, 511–518.
Clementz, B. G. (1989). Assessment of tibial torsion and rotational deformity with anew fluoroscopic technique. Clinical Orthopaedics and Related Research, 245, 199–209.
Schneider, B., Laubenberger, J., Jemlich, S., Groenek, K., Weber, H. M., & Larger, M. (1997). Measurement of femoral antetorsion and tibial torsion by magnetic resonance imaging. British Journal of Radiology, 70, 575–579.
Hudson, D., Roger, T., & Richards, J. (2006). Ultrasound measurements of torsions in the tibia and femur. Journal of Bone and Joint Surgery. American Volume, 88, 138–143.
Jakob, R. P., Haertel, M., & Stussi, E. (1980). Tibial torsion calculated by computerized tomography and compared to other methods of measurement. Journal of Bone and Joint Surgery. British Volume, 62, 238–242.
Lee, S. Y., Choi, K. S., Jeung, I. S., Lee, J. E., Yang, S. M., & Lee, S. M. (2011). Physical examination and computed tomography in children with toe-in gait. Journal of Korean Academy of Rehabilitation Medicine, 35, 61–66.
Stuberg, W., Temme, J., Kaplan, P., Clarke, A., & Fuchs, R. (1991). Measurement of tibial torsion and thigh-foot angle using goniometry and computed tomography. Clinical Orthopaedics and Related Research, 272, 208–212.
Valmassy, R., & Stanton, B. (1989). Tibial torsion. Normal values in children. Journal of the American Podiatric Medical Association, 79, 432–435.
King, H. A., & Staheli, L. T. (1984). Torsional problems in cerebral palsy. Foot Ankle., 4, 180–184.
Milner, C. E., & Soames, R. W. (1998). A comparison of four in vivo methods of measuring tibial torsion. Journal of Anatomy, 193, 139–144.
Eckhoff, D. G., & Johnson, K. K. (1994). Three-dimensional computed tomography reconstruction of tibial torsion. Clinical Orthopaedics and Related Research, 302, 42–46.
Strecker, W., Keppler, P., Gebhard, F., & Kinzl, L. (1997). Length and torsion of the lower limb. Journal of Bone and Joint Surgery. British Volume, 79, 1019–1023.
Moussa, M. (1994). Rotational malalignment and femoral torsion in osteoarthritic knees with patellofemoral joint involvement: A CT scan study. Clinical Orthopaedics and Related Research, 304, 176–183.
Lang, L. M., & Volpe, R. G. (1998). Measurement of tibial torsion. Journal of the American Podiatric Medical Association, 88, 160–165.
Takai, S., Sakakida, K., Yamashita, F., Suzu, F., & Izuta, F. (1985). Rotational alignment of the lower limb in osteoarthritis of the knee. International Orthopaedics, 9, 209–215.
Yagi, T. (1994). Tibial torsion in patients with medial-type osteoarthrotic knees. Clinical Orthopaedics and Related Research, 302, 52–56.
Turner, M. S. (1994). The association between tibial torsion and knee joint pathology. Clinical Orthopaedics and Related Research, 302, 47–51.
Rosen, H., & Sandick, H. (1955). The measurement of tibio fibular torsion. Journal of Bone and Joint Surgery. American Volume, 37, 847–855.
Bonnevialle, P., Andrieu, S., Bellumore, Y., Challé, J. J., Rongières, M., & Mansat, M. (1998). Torsional abnormalities and length discrepancies after intramedullary nailing for femoral and tibial diaphyseal fracture. Computerized tomography evaluation of 189 fractures. Revue de Chirurgie Orthopedique et Reparatrice de l’appareil Moteur, 84, 397–410.
Court-Brown, C. M., Christie, J., & McQueen, M. M. (1990). Closed intramedullary tibial nailing. Its use in closed and type I open fractures. The Journal of Bone and Joint Surgery. British Volume, 72, 605–611.
Puno, R. M., Vaughan, J. J., Stetten, M. L., & Johnson, J. R. (1991). Long-term effects of tibial angular malunion on the knee and ankle joints. Journal of Orthopaedic Trauma, 79, 371–383.
Puloski, S., Romano, C., Buckley, R., & Powell, J. (2004). Rotational malalignment of the tibia following reamed intramedullary nail fixation. Journal of Orthopaedic Trauma, 18, 397–402.
Terry Canale, S., & James, B. (2013). Chapter 54—Fractures of the lower extremity. In: Campbell, Editor. Campbell’s operative Orthopaedics, 12th edition,Tennessee, p 2645.
Prasad, C. V., Khalid, M., McCarthy, P., & O’Sullivan, M. E. (1999). CT assessment of torsion following locked intramedullary nailing of tibial fractures. Injury, 30, 467–470.
Jafarinejad, A. E., Bakhshi, H., Haghnegahdar, M., & Ghomeishi, N. (2012). Malrotation following reamed intramedullary nailing of closed tibial fractures. Indian Journal of Orthopaedics, 46, 312–316.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standard statement
This study involved patients with fracture both bones of leg, who were managed in a tertiary care centre with multidisciplinary approach. We have performed only established and time tested procedures on these patients. We have not employed any new experimental methods (including surgical, pharmacological and radiological methods) on these patients. Every procedure was explained in detail to the patient, including the post operative CT scan for measurement of malrotation. We have exercised utmost care to follow the international principles of medical ethics in all our patients. We have also obtained informed consent for surgical aspects as well as for using their clinical and radiological images for scientific study purpose. As a corresponding author, I hold the full responsibility for any ethical related issues in this study.
Informed consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ramprasath, D.R., Chezian, S.V. & Surendar, V. Identification of Tibial Malrotation After Nailing Using Unique CT Scan Reference Line, and Influence of Position of Leg for Distal Locking on Rotation. JOIO 55, 662–668 (2021). https://doi.org/10.1007/s43465-020-00307-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43465-020-00307-z