
Abstract
This paper presents a method for collecting core body temperature data via a temperature sensor integrated into a powered toothbrush. The purpose is to facilitate the collection of temperature data without any extended effort from the user. Twelve participants use a powered toothbrush with a temperature sensor mounted on the brush head twice daily for two months. The obtained values are compared with those from a conventional fever thermometer approved for intraoral use. The results show that the temperature sensor–integrated powered toothbrush can measure the core body temperature and provide values comparable to those provided by a traditional oral thermometer. The use of the device can facilitate disease monitoring, fertility control, and security solutions for the elderly.
Article highlights
-
The body temperature can be measured using a powered toothbrush with an integrated temperature sensor.
-
The values obtained from a temperature sensor–integrated powered toothbrush was comparable to those obtained from a traditional oral thermometer.
-
The implication of the study is a way to facilitate the collection of temperature data, but the design of the temperature sensor’s integration in the brush head needs to be further developed, and the possibility of transferring the obtained data directly to a central server using WIFI must be explored.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
The core body temperature has long been used as a disease or metabolic-change indicator. What is considered normal body temperature and what is considered fever were determined by Wunderlich [1] as early as 1869. Natural variations in the core body temperature are found during the day [1] and cyclical changes vary between individuals[2]. However, the concept of fever is being re-evaluated [3]. It has previously been said that a fever is a 38 °C core body temperature or higher, but it has been shown that the normal core body temperature differs between individuals, meaning that some individuals can be ill and have a fever even if their core body temperature is lower than 38 °C. It is also known that older individuals in general, and sometimes individuals with neurocognitive illnesses have a lower normal body temperature and may therefore be underdiagnosed regarding fever. A new definition suggests that fever is defined as an increase of 1.0-1.5 °C from the individual´s normal body temperature, along with malaise [4]. The use of the temp brush method is beneficial because it continuously checks the body temperature and can thus determine an individual’s normal body temperature measured from the same site [5]. This allows quick detection when something is wrong and thus taking action long before the temperature has risen to 38 °C. Regular monitoring of the core body temperature in an easy way can be beneficial for individuals in different life situations.
In Sweden, as in many other parts of the world, life expectancy is increasing, and many healthy elderly, or disabled adults, live alone. They may lack relatives or have them far away. This could create a feeling of insecurity. Using a method of monitoring the body temperature while tooth brushing not affecting daily life or autonomy may be beneficial for them. Such a method can monitor the core body temperature and thus detect the need for medical consultation and care at an early stage of the disease. Previous studies have shown that a powered toothbrush is a well-functioning tool used by older individuals with mild cognitive impairment even when their cognitive levels decrease [6]. There is also a described method for the wireless transmission of data from intelligent powered toothbrushes for storage and analysis [7]. The aim of increasing older people’s opportunities for good health and quality of life is not diminished by this method’s broader opening to other uses, such as fertility planning. Several digital aids based on measuring body temperature rise after ovulation are available. However, they require traditional rectal or vaginal temperature measurements, and the obtained data are entered manually into an application. This affects the user’s daily life and is inconvenient to use. There is also a risk of committing errors when reading and entering data, which can cause gaps in the frequency of use of such aids [8].
Using the increase in body temperature occurring after ovulation to plan or avoid pregnancy has long been of great interest [9], [10], and a device that enables the automatic transfer of body temperature data from a toothbrush to a computer application or server can be beneficial. Another possible use of such a device is for monitoring and detecting diseases such as hypothyroidism. The rapid development of digital health support functions and artificial intelligence applications has increased the need for different types of body sensors. In addition, today’s active people may not want to spend time collecting data but would rather like this to happen in the background. Being able to collect body temperature data while the individual is brushing their teeth would meet such requirements.
The present study aimed to evaluate whether a temperature sensor integrated into a powered toothbrush could provide body temperature data equivalent to those provided by the traditional mouth thermometer. This paper is organized into seven parts and Sect. 2 contains Materials, Methods, and Statistics. In the following Sect. 3, the Results are reported followed by the Discussion and Conclusion in Sect. 4. In Sect. 5 Ethics are discussed and Abbreviations described, and Sect. 6 contains the References. Finally in Sect. 7 Statements and Declarations are presented.
2 Material, methods, and statistics
2.1 Materials and methods
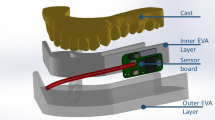
For this study, 12 participants (10 females, 2 males) aged 34–61 (mean age: 48.25) were recruited from the Department of Health at Blekinge Institute of Technology (Table 1). The inclusion criteria were the presence of at least twenty teeth and not taking any medications regularly. The present study follows the ethical rules for the research described in the World Medical Association (WMA), Declaration of Helsinki[11]. All participants received individual oral and written information about the study and their right to cancel participation at any time without a specific reason. Participants signed informed consent before the start of the study. At baseline, the participants received an intelligent powered toothbrush [12] equipped with a temperature sensor mounted on the brush head connected to a digital min/max [13] thermometer display via wire as well as a traditional digital fever thermometer [14] approved for intraoral use The reference value, in the form of the conventional thermometer, indicates the highest temperature obtained that remains unchanged during a predetermined measurement time The brush thermometer’s maximum value is used after the recommended brushing time of two minutes.
The minimum value only signals the ambient temperature at the beginning of brushing and increases during the brushing session to the maximum temperature value, which is reached when the temperature sensor is on the floor of the mouth under the tongue.
The mobile application associated with the powered toothbrush was downloaded to the participants’ mobile phones and the brushes were synchronized with the application for measuring average brush time. Accurate information and instructions about the use of brush and thermometer were given. Participants were asked to first measure their body temperature in the morning and evening with the traditional fever thermometer (T). Then brush their teeth with the powered toothbrush for at least two minutes without rinsing the brush or mouth in the meantime. The maximum temperature achieved during the brush session and the temperature from T were noted in the tables obtained in addition to any temporary illness or the use of antipyretic drugs. The study continued for 60 days.
During analyze of the data, the normal distribution of the material was controlled. Furthermore, the material was analyzed in MATLAB where curves for T and the brush thermometer (B T) morning and evening for all participants were produced. To the observation values from the B T, the mean value of the difference between T and B T was added to be able to compare the curves. The Bland-Altman[15] plot was then performed. Eleven participants answered, after the study, the following questions. (Table 1)
How many days did it take to get used to the brush thermometer?
Did you have any problems using the equipment? If yes, briefly describe the problems.
Did you find it positive to have regular control over your body temperature?
Eight B T and eight T were validated by simultaneously immersing them for two minutes in a water bath at 36.4 degrees Celsius, which was the average temperature of the fever thermometers in all observations.
2.2 Statistics
One sample T-test, calculations, and analysis of data as well as the construction of curves and plots have been performed in Statistical Package for Social Science, version 28 (SPSS Inc., NY, USA) [16] and MATLAB [17].
3 Results
All 12 participants completed the study period. Gender and age distribution as well as the participants’ user opinions are shown in Table 1.
For the eleven participants who shared their experiences, it took an average of 2.4 days (SD 1.87) to get used to the new toothbrush. 82% of the participants stated that they had no problems using the equipment. Of the 18% who stated that they had problems using the tool, it was due to the size of the prototype. All participants experience the positive effects of having control over their body core temperature (BCT).
T was used as the golden standard. The definition of fever is generally described as a body temperature ≥ 38 °C [18]. A daily mean value calculated on the participants’ morning and evening temperature measured orally with the T gave a mean value for the morning temperature of 36.4 °C and the evening temperature of 36.44 °C. The thermometers were validated in a 36.4 C water bath. The mean value for BT was 36.61 (SD 0.134) and for T 36.95 (SD 0.054). For the 12 participants, mean values, median, CI, and standard deviation for the gap between the observations for T and B T are presented in Table 2.
The normal distribution of the material was checked for each participant and the total number of observations using Kolmogorov-Smirnov, Shapiro-Wilk, Normal Q-Q Plot, Detrended Normal Q-Q plot, Histogram, and Boxplot. The gap between T and the B T shows a good normal distribution both on an individual basis and for the total number of observations. Thirty-six morning observations and six evening observations were unavailable representing 3% of the 1440 observation occasions. Figure 1 illustrates the histogram, Q-Q plot, and box plot for total ID 1–12, in the morning.

Histogram, Q-Q plot, and box plot for ID 1–12 morning
To compare the compliance of the two measurement methods, the individual difference (diff) between T and B T must be neutralized. This is done by adding the mean diff from Table 2 to the values for B T for the morning and evening of the respective ID. The procedure is visually shown in Fig. 2a and b for the morning values of ID 12.

a Morning measured values T and BT for ID12. b Morning measured values T and BT + mean diff for ID12
The Bland-Altman plot (Fig. 3) was used to compare the two measurement methods and to evaluate whether proportional bias occurs. The agreement limits are defined as T – BT + - SD * 1.96. Suppose the values between the limits have no clinical significance. In that case, it is ensured that 95% of the differences lie within the span and are interchangeable with each other allowing for identifying and ignoring extreme values. The Bland-Altman plot shows that the observations in this study, in addition to identified extreme values, are within the limits of agreement and will contain 95% of future measurements with the two methods.
Table 3 shows the data used for the Bland-Altman plot
When the diff of evening observations T and B T, for ID1-12, was analyzed by one-sample T-test the difference was statistically significant. This indicates that the bland-Altman plot is uncertain (Fig. 4). Despite this, as in the plot for the morning observations, it shows a slight tendency to proportional bias so that T shows higher values than B T at low temperatures and vice versa. However, this was within the limits of agreement.

Bland-Altman plot morning and evening for ID 4

Bland-Altman plot morning and evening for ID 1–12
Illustrated in Fig. 5 are the brush patterns of the different individuals which are seen as well-distinguishable clusters. The standard deviation of the participants’ average brushing time over two months is between 0 and 9 s.

All measured values T and BT for ID 1–12
4 Discussion and conclusion
4.1 Discussion
We have investigated if it is possible to measure core body temperature during toothbrushing with a temperature sensor on the brush head of a powered toothbrush. Furthermore, if the data obtained is equivalent to that from an orally used fever thermometer.
The intended user groups are many and include individuals of different ages and cognition levels. The experimental group in this pilot study was chosen to obtain as good observation data and feedback as possible referring to the temperature measurement. In this study, it was not investigated clinically or via questionnaire/interview whether the sensor equipment affected the brushing result or the comfort when used. The goal is to carry out larger research studies aimed at different target groups.
One limitation of the study is the primitively designed experimental device. A few participants reported having difficulties using the prototypes due to their size. This may have resulted in unreliable metrics for one participant throughout the study. In a larger population, this problem could be significant. However, a better design and integration of the sensor in the brush head are planned for future studies. Another limitation is that the participants were all healthy during the study period. A febrile control group had been an asset to the study and should be considered for future research.
Both individual and systematic differences exist between the two measurement methods. The individual differences depend, for example, on the users’ different brushing patterns and whether the mouth is open or closed during brushing. At the same time, the differences within the individuals are small. The participants’ mean brushing times over two months have a standard deviation between 0 and 9 s. Figure 5 shows how the difference between T and BT differs between the participants, while each participant’s measurements are quite conformal during the trial period, which shows up as clearly observable clusters in the figure. The systematic differences are shown in generally lower measurement values and higher standard deviation from the BT measurements. Without correction, these discrepancies would have made it impossible to use the tested method for diagnostics. By taking the mean value of the difference between the measured values for T and BT and adding it to the value for BT, the mean difference becomes zero in each measurement, which makes it possible to compare the methods. A strength of this study is the large number of observations collected over a relatively long period and using a powered toothbrush as a carrier of temperature sensor has the advantage of not requiring any extra effort from the user. Similar studies have been performed with a temperature sensor in a patch on the abdominal skin which is compared with IR measurement of temperature on the forehead [19]. Another study uses bracelets to obtain, among other things, body temperature [20]. These studies show good acceptance from users but have short trial periods, 24 and 72 h. Unlike the present study, they measure skin temperature which is affected by several external factors such as ambient temperature and sweating which gives an uncertain measurement and a weak correlation between the measurement methods. Core body temperature is the temperature of structures deep within the body. There are several accepted methods to measure core body temperature, e.g., rectal, oral, and by ear canal for tympanic membrane temperature. They all have pros and cons regarding accessibility and convenience [5]. The rectal measurement method is often used as the golden standard, as the values vary slightly with repeated measurements in the same individual and occasion. The disadvantages are that it carries a risk of infection and rupture of the mucous membrane if performed incorrectly and that the method can be perceived as unpleasant and embarrassing for the user. Oral measurement has the advantage of being easy to perform but the method is sensitive to the correct placement of the thermometer. Temperature measurement at the tympanic membrane with an IR thermometer is fast, hygienic, and painless, though even this method is sensitive to incorrect handling. In this study, we have used oral measurement with a digital oral thermometer as the golden standard as it measures in the same site as the BT method. Other measurement methods have shown lower values and increased SD compared to rectal measurement. Previous studies that compared different measurement methods have determined the importance of always measuring at the same place, not comparing values from different measurement sites, and not converting values to correspond to values from rectal measurement [21]. As previously mentioned, the definition of fever is reevaluated from a fixed value of 38 °C to an individual-related value based on malaise together with an increased core body temperature of 1-1.5 °C is a fever. Accordingly, knowing the normal temperature becomes essential. Using a temperature sensor integrated into the brush head of a powered toothbrush that can transfer the data to a computer application or a central server provides a database for calculating the person´s normal temperature and allows for the detection of changes in body temperature patterns.
In the present study, the Bland-Altman plot is used to compare a new measurement method with a golden standard [15], [22] and showed good agreement between the two measurement methods.
The future potential lies in fully integrating the temperature sensor in the brush head and transmitting the data via WIFI and/ or Bluetooth together with other brush data. This is technically and design-wise feasible as the sensors are small and relatively inexpensive and thus allow a smooth design. This study has shown the way for a powered toothbrush as a carrier of a temperature sensor.
4.2 Conclusion
The feasibility of using an intelligent powered toothbrush to carry a sensor for measuring the core body temperature during toothbrushing is good.
5 Ethical considerations and abbreviation
5.1 Ethical considerations
The present study follows the ethical rules for the research described in the World Medical Association (WMA), Declaration of Helsinki [11].
An ethical trial has not been implemented as this feasibility study does not process sensitive personal data according to the Swedish Integration Agency (IMY). Nor does the study involve any physical intervention or intention to affect the participants physically or mentally. No biological material is collected but only temperature data from the oral cavity. That it is voluntary to participate is obvious to the participants who are healthy adults and are not in a position of dependence on the authors.
5.2 Consent to participate and consent for publication
The participants received both oral and written information about the study plan and the possibility of terminating their participation at any time without stating a reason. All participants provided written informed consent about participating and their awareness of the publication of the results before entering the studies. The participant’s identity is coded so that all incoming data is de-personalized.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- BCT:
-
Body Core Temperature
- T:
-
Fever thermometer
- BT:
-
Brush thermometer
- Diff:
-
Difference
References
Wunderlich CA (1871) On the temperature in diseases: a manual of medical thermometry. New Sydenham Society, London
”Non-invasive monitoring of core body temperature rhythms over 72 h in 10 bedridden elderly patients with disorders of consciousness in a Japanese hospital: a pilot study | Elsevier Enhanced Reader” (2022). https://reader.elsevier.com/reader/sd/pii/S0167494313001027?token=EFC363CCF6B2E10E9D0F2991CDA06165852A4EB72C1D87EC562989172E7C44DCD8FA193331F1F4984B63D84187908452&originRegion=eu-west-1&originCreation=20220315130123
”Forskare slår hål på myter om feber”. https://www.vardfokus.se/nyheter/forskare-slar-hal-pa-myter-om-feber/ (åtkomstdatum 19 april 2022)
Levander Och MS, Grodzinsky E (2017) Variation in normal ear temperature. Am J Med Sci 354(4):370–378. https://doi.org/10.1016/j.amjms.2017.05.013
Sund-Levander M, Grodzinsky OE (2013) Assessment of body temperature measurement options. Br J Nurs 22(6):942–950
Flyborg J, Renvert S, Sanmartin Berglund J, Anderberg OP (2022) ”Use of a powered toothbrush to improve oral health in individuals with mild cognitive impairment. Gerodontology. https://doi.org/10.1111/ger.12619
Aeddula O, Flyborg J, Larsson T, Anderberg P, Sanmartin Berglund J, Och Renvert S, (2021) A solution with bluetooth low energy technology to support oral healthcare decisions for improving oral hygiene. In: Presenterad vid 5th international conference on medical and informatics H. vol 1 ICMHI, Kyoto, Japan, p 134–139. http://urn.kb.se/resolve?urn=urn:nbn:se:bth-22249
Shopov M, Kakanakova I, Kakanakov N, Mateev OB, (2019) An mHealth application for female fertility assistance. In: 4th international conference on smart and sustainable technologies (SpliTech). https://doi.org/10.23919/SpliTech.2019.8783086
Shilaih M, Goodale BM, Falco L, Kübler F, Clerck DV, Leeners OB (2018) Modern fertility awareness methods: wrist wearables capture the changes in temperature associated with the menstrual cycle. Biosci Rep. https://doi.org/10.1042/BSR20171279
Stanford JB, Willis SK, Hatch EE, Rothman KJ, Wise OLA (2019) Fecundability in relation to use of fertility awareness indicators in a North American preconception cohort study. Fertil Steril 112(5): 892-899. https://doi.org/10.1016/j.fertnstert.2019.06.036
”World Medical Association Declaration of Helsinki (2001) Ethical principles for medical research involving human subjects. Bull World Health Organ 79(4):373–374
”Oral -B Genius 8000 N Silver eltandborste | Oral-B” (2021). https://www.oralb.se/sv-se/produkter/eltandborstar/oral-b-genius-8000n-silver-eltandborste (åtkomstdatum 14 april 2021)
”156d04d 4-3c2a-4111-aca1-7ea66fcc2703.pdf”. Åtkomstdatum: 10 februari 2022. [Online]. Tillgänglig vid: https://docs.biltema.com/v2/documents/file/sv/156d04d4-3c2a-4111-aca1-7ea66fcc2703
Köp Telfo febertermometer, 1 st | Apoteket.se (2022). https://www.apoteket.se/produkt/telfo-febertermometer-1-st-344912/ (åtkomstdatum 10 februari 2022)
Bland Och JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1(8476):307–310
SPSS Statistics | IBM (2022). https://www.ibm.com/products/spss-statistics
MATLAB - MathWorks (2022)
Moran DS, Mendal OL (2002) Core temperature measurement. Sport Med, 32(14):879–885. https://doi.org/10.2165/00007256-200232140-00001
Kim H (2021) Smart patch for skin temperature: preliminary study to evaluate psychometrics and feasibility. Sensors. https://doi.org/10.3390/s21051855
Durán-Vega LA (2019) An IoT system for remote health monitoring in elderly adults through a wearable device and mobile application. Geriatrics. https://doi.org/10.3390/geriatrics4020034
Sund-Levander M, Grodzinsky E, Loyd D, Wahren OLK (2004) Errors in body temperature assessment related to individual variation, measuring technique and equipment. Int J Nurs Pract 10(5):216–223
Hanneman SK (2008) Design, analysis and interpretation of method-comparison studies. AACN Adv Crit Care 19(2):223–234. https://doi.org/10.1097/01.AACN.0000318125.41512.a3
Acknowledgment
This study was supported by grants from the Blekinge Institute of Technology and Kristianstad University. The powered toothbrushes used in the study were generously provided by Proctor & Gamble.
Funding
Open access funding provided by Blekinge Institute of Technology. This study was supported by grants from the Blekinge Institute of Technology and Kristianstad University. The powered toothbrushes were generously provided by Proctor & Gamble.
Author information
Authors and Affiliations
Contributions
JF, SR, and JSB planned the project. JF performed the data collection. JF and UI managed the data collected. JF and UI analyzed the data. JF led the writing. SR, JSB, and PA participated in the final manuscript production. All authors revived and accepted the final manuscript.
Corresponding author
Ethics declarations
Competing of interest
The authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Flyborg, J., Renvert, S., Anderberg, P. et al. Measurement of body temperature in the oral cavity with a temperature sensor integrated with a powered toothbrush. SN Appl. Sci. 5, 22 (2023). https://doi.org/10.1007/s42452-022-05250-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s42452-022-05250-2