
Abstract
Myocarditis is an inflammatory disease of the myocardium with either focal or diffuse involvement and usually gives rise to chest pain, dyspnea, palpitations, and fatigue. In severe cases, arrythmias, syncope, and cardiogenic shock may occur. Acute myocarditis is most commonly caused by a variety of viruses with cardiotropic properties. Rare causes of myocarditis include bacterial infections. We, herein, describe a case of acute myocarditis caused by the intracellular bacterium Francisella tularensis. A young and previously healthy male in Northern Sweden was referred to the emergency department due to intense upper-chest pain and dyspnea. ECG exhibited minimal ST-segment elevations and laboratory parameters revealed pathological levels of high-sensitivity cardiac troponin and C-reactive protein. Radiological imaging showed increased metabolism in enlarged lymph nodes in the chest and signs that could be compatible with increased metabolism in the left ventricular of the heart. The combination of acute myocarditis and enlarged lymph nodes was believed to be caused by the intracellular bacterium Francisella tularensis, endemic in the Northern Sweden, and was verified with positive serology. The patient showed full recovery after antimicrobial treatment. As this is the fifth published case of myocarditis associated with Francisella tularensis, we suggest considering tularemia in acute myocarditis in tularemia-endemic area.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Myocarditis is an inflammatory disease of the myocardium with either focal or diffuse involvement [1]. In acute myocarditis, the patient typically presents with chest pain, dyspnea, palpitations, fatigue, and in more severe cases also arrhythmias, syncope, and cardiogenic shock [2]. Acute myocarditis has been estimated to cause 12% of sudden cardiac death in young adults [3, 4]. It is predominantly a disease of patients under the age of 50 years, and 3 out of 4 patients are males [5]. The gold standard for a definitive diagnosis of myocarditis relies on an endomyocardial biopsy (EMB) using the Dallas criteria, which is based on traditional histological stains [6]. The invasive nature of an EMB, combined with the Dallas criteria’s limited diagnostic accuracy and sensitivity, have implied a limited use of EMB [7]. In medical practice, myocarditis is more often diagnosed based on a combination of clinical features, laboratory analysis, and imaging findings [8].
Community-acquired myocarditis is often a result from common viral infections causing an inflammatory response in the endomyocardium, either directly or indirectly [1]. Less common causes of myocarditis include toxins, medications, autoimmune phenomena, and bacterial infections [9]. The gram-negative intracellular bacterium Francisella tularensis, highly contagious, is found in Europe as well as in North America causing the infection tularemia in humans and other mammals. Tularemia can be transmitted to humans from invertebrates, mammals and birds by various routes of transmission and F. tularensis is regarded a potential biological threat agent for warfare or bioterrorism by the Center for Disease Control and Prevention in the USA and by the European Medicines Agency [10,11,12]. In Europe, the less virulent of two main subspecies is present [12]. Flu-like symptoms such as fever, myalgia, arthralgia, and headache usually develop after an incubation period of 3–5 days (range 1–21 days) [13]. Systemic complications may arise, especially if the infection is left untreated, including respiratory disease and lymphadenopathy with abscesses. Pericarditis is unusual in tularemia and myocardium involvement and acute myocarditis are considered very rare complications [14, 15]. To the best of our knowledge, four cases of tularemia-induced myocarditis have been described in the literature. Herein, we describe an additional case of myocarditis in a young male adult who presented at the emergency clinic with symptoms mimicking an acute coronary syndrome.
Case Presentation
A 29-year-old, otherwise healthy, male was referred to an emergency department (ED) in Northern Sweden in the beginning of October due to an intense upper chest pain, Numerical Rating Scale (NRS) 9, with a sudden onset and with radiation up to his jaw. He had suffered from progressive respiratory difficulties and a short of breath during physical exercise beginning 2 weeks earlier. Six days prior to admission, he had suffered from a fatigue, episodes of excessive sweating, subfebrility, and headache. Four days prior to admission, a progressive discomfort in his upper chest evolved, with radiation to his jaw and left forearm. The chest pain intensified, especially when being physically active, and was accompanied by nausea, and prompted him to seek medical attention. The patient lived in a semi-rural area but did not have any domestic animals or pets and had not been abroad. He did not recall any lymphadenopathy or infected wounds.
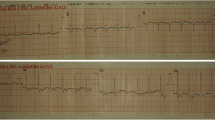
His initial vital parameters (body temperature, pulse oximetry saturation, respiratory rate, and blood pressure) upon arrival to the ED were all normal. He had no heart murmurs, and his physical examination was without any remarks. Laboratory testing, however, showed elevated high sensitivity (Hs) troponins and a slightly increased level of C-reactive protein (CRP) (Table 1). His ECG showed non-significant ST-elevations in most precordial electrodes (Fig. 1). The transthoracic echocardiogram (TTE) was found normal, but pro B-type natriuretic peptide (proBNP) was elevated (354 ng/l) indicating increased filling pressure in the heart.

Patient ECG. ECG registered upon the patient’s arrival to the emergency department. A Extremity leads, and B precordial leads. ST-elevations up to 2 mm of height can be seen in I, -aVR, II, and V2-V6
On the first day after admission—a fortnight after the first symptoms arose—a CT scan of the chest showed enlarged lymph nodes, one with central necrosis, in the right hilum pulmonalis. There was also a moderately enlarged lymph node centrally in the mediastinum. These enlarged masses were further investigated with a full-body fluorodeoxyglucose (FDG)-positron emission tomography (PET)/computer tomography (CT) (from here on referred to as PET/CT) and showed increased metabolism in lymph nodes next to the trachea, the carina, and the hilum pulmonalis, all on the right side (Fig. 2). The latter showed signs compatible with necrotic tissue. Additional enlarged lymph nodes with increased metabolism were found next to the vena cava, vena porta, and the aorta (Fig. 3). There was an unspecific metabolism in the myocardium (Fig. 4), and the patient had moderate splenomegaly.

Trans axial PET/CT (left) and CT (right). FDG-uptake in a necrotic right sided hilar lymph node (open arrow) and in a subcarinal lymph node (filled arrow)

Coronal PET/CT of the upper abdomen. FDG-uptake in paraaortic /paracaval and paraportal lymph nodes

Coronal PET/CT of the chest. FDG-uptake in right sided hilar and mediastinal lymph nodes. Whether the high cardiac FDG-uptake (i.e., glucose metabolism) is physiological or due to myocarditis is not possible to assess, since imaging is not performed with a heart protocol (after low carbohydrate diet and prolonged fasting)
These radiological findings combined with the initial symptoms of respiratory difficulties and subfebrility raised the suspicion of tularemia, which is endemic in Northern Sweden. Blood sampling for F. tularensis-serology was performed the first day after admission but came back negative. F. tularensis-specific antibodies in blood were assayed using a rapid immunochromatographic test for IgM, IgA, and IgG (VIRapid® TULAREMIA, Vircell, Granada, Spain) and an ELISA for semi-quantitative and highly sensitive detection of IgM and IgG antibodies (Protocol A.5.2 in the WHO guidelines on tularaemia) [16]. Three days later, however, a new blood sample was drawn, and this time the rapid immunochromatography test, as well as the ELISA, provided weak signals classified as indeterminate by the laboratory (Table 2). At this time, troponin had started to decrease, and the patient was feeling better and was discharged, but at the suspicion of tularemia was given doxycycline (100 mg twice daily) for 14 days. On day 11 after admission, a new blood sample was taken for analysis of F. tularensis-specific antibodies and this time both the rapid immunochromatographic test and the semi-quantitative ELISA assay provided clearly positive results verifying seroconversion diagnostic for acute tularemia (Table 2). A follow-up blood-sample taken 45 days after admission further verified that this was an acute disease episode of tularemia showing decrease of IgM and increase in IgG (Table 2). After 14 days with doxycycline the patient still reported fatigue and a short of breath. The treatment was prolonged for another 10 days using ciprofloxacin (500 mg twice daily) and the patient fully recovered. A CT scan of the thorax with intravenous contrast did not show any pathological findings and all laboratory tests were normal.
Discussion
Acute myocarditis is an inflammatory disease commonly associated with a variety of viruses, even though other causative agents also exist [1]. The pathogenesis of acute myocarditis, however, is still incompletely understood. We, herein, describe an unusual case of acute myocarditis in a young and previously healthy male in Northern Sweden with a disease history of 14 days, which turned out to be caused by the intracellular bacterium F. tularensis. The patient presented at the emergency clinic with symptoms of an acute coronary syndrome, although an underlying coronary artery disease seemed quite unlikely due to his young age and spotless medical record. Due to this, a CT coronary angiography was not performed. ECG showed minimal ST-segment elevations in most precordial electrodes, and he had elevated troponins indicating cardiac pathology. A TTE showed normal cardiac function despite a slightly increased pro-BNP, and a PET/CT showed unspecific metabolism in the myocardium, which could be either physiological or compatible with an inflammatory response. Cardiac magnetic resonance imaging was not performed but would have been informative to address this.
Findings of enlarged pulmonary, mediastinal, and abdominal lymph nodes next to the big blood vessels on the CT scan and PET/CT could be due to a malign neoplasia, e.g., lymphoma, or sarcoidosis. These findings, however, raised the concern of tularemia, which is endemic in Northern Sweden. Serology for F. tularensis was initially negative, but already at day 3 after admission, the laboratory reported levels that were indeterminate (i.e., between negative and positive), and at day 11, the patient had seroconverted and fulfilled diagnostic criteria for recent F. tularensis infection [16].
The present patient case lacked radiological signs of pneumonia but illustrates extensive lymph tissue involvement in the mediastinum, a feature that is typical in tularemia patients with pneumonia that has been acquired by inhalation of F. tularensis-aerosols, for example, from dust contaminated by infected rodents [17]. Such mediastinal engagement may be indistinguishable from malignancy on CT scans making differential diagnosis challenging [15]. Tularemia, like some other infections caused by intracellular bacteria including tuberculosis and brucellosis, can also be missed due to the unspecific symptoms and clinical mimicry. Further increasing the challenge, a diagnostic seroconversion can take up to 14–21 days to occur [18]. PCR detection of the bacterium is increasingly used for respiratory samples in patients with suspected pneumonia, and for samples from wound secretions in clinical presentations after tick or insect bites. In the present patient’s case, however, there was no suspicion of pneumonia and no wound secretion, and therefore, no such diagnostic attempts performed. With regard to clinical chemistry parameters, the present history is typical for tularemia with generally lower levels of CRP than expected for an invasive bacterial disease [17]. In this case, CRP peaked at 40 mg/L.
Because F. tularensis is well-known for tropism with macrophages, dendritic cells, and in addition some epithelial cells but not tropism with myocardial cells, we hypothesize that the infection indirectly triggered acute myocarditis by activating the immune system. This would resemble the pathophysiology of acute myocarditis from some lymphotropic viruses that are believed to cause cardiac injury by triggering a cytokine storm or a cellular immune response [1]. To put this hypothesis to test a first step would be to obtain an EMB in accordance with the diagnostic procedure that is gold standard for acute myocarditis [19]. A definitive diagnosis of myocarditis requires an EMB but most patients do nevertheless not undergo this invasive procedure. This is partly due to low sensitivity, but also due to the often self-limiting nature of myocarditis hampering the incentive for an invasive procedure [20, 21]. According to the latest Expert Consensus Document, an EMB is recommended in a limited number of clinical scenarios, including hemodynamically compromised patients, and patients suffering from life-threatening arrhythmias. In our case, with a hemodynamically stable patient showing spontaneous recovery, an EMB was not performed.
From 1992 to 2012, more than 18,300 human cases of tularemia were reported to the ECDC database, with the highest average incidence in Sweden and Finland. The most common transmission route in these countries is by a mosquito bite [22]. The patient lived in a semi-rural setting but had not been exposed to vertebrates known to transmit F. tularensis. Inhaled, contaminated aerosols or transmission via a mosquito bite are the two most probable scenarios of transmission in this case [22].
Conclusions
Tularemia can easily be missed due to unspecific symptoms and clinical presentation. It is, therefore, important to bear this infectious disease in mind in tularemia-endemic areas when assessing patients with inflammation of organs within the chest cavity combined with radiological signs of lymphadenopathy. Cardiac magnetic resonance imaging may provide important information when a suspicion is raised. As this is the fifth published case of myocarditis associated with F. tularensis, we suggest considering tularemia in acute myocarditis in tularemia-endemic areas. Timely treatment with appropriate antibiotics provides a favorable prognosis in tularemia.
Data Availability
All medical data and materials are kept in the electronic medical record of the patient and can only be accessed by health personnel taking part in the patient’s medical care. Please contact the corresponding author to request details regarding this case.
Code Availability
Not applicable.
Abbreviations
- CRP:
-
C-reactive protein
- CT:
-
Computer tomography
- EMB:
-
Endomyocardial biopsy
- ED:
-
Emergency Department
- FDG:
-
Fluorodeoxyglucose
- Hs:
-
High sensitivity
- NRS:
-
Numerical Rating Scale
- PET:
-
Positron emission tomography
- ProBNP:
-
Pro B-type natriuretic peptide
- TTE:
-
Transthoracic echocardiogram
References
Tschope C, et al. Myocarditis and inflammatory cardiomyopathy: current evidence and future directions. Nat Rev Cardiol. 2021;18(3):169–93.
Kociol RD, et al. Recognition and initial management of fulminant myocarditis: a scientific statement from the American Heart Association. Circulation. 2020;141(6):e69–92.
Doolan A, Langlois N, Semsarian C. Causes of sudden cardiac death in young Australians. Med J Aust. 2004;180(3):110–2.
Fabre A, Sheppard MN. Sudden adult death syndrome and other non-ischaemic causes of sudden cardiac death. Heart. 2006;92(3):316–20.
Fu M, et al. Trends in myocarditis incidence, complications and mortality in Sweden from 2000 to 2014. Sci Rep. 2022;12(1):1810.
Aretz HT, et al. Myocarditis. A histopathologic definition and classification. Am J Cardiovasc Pathol. 1987;1(1):3–14.
Baughman KL. Diagnosis of myocarditis: death of Dallas criteria. Circulation. 2006;113(4):593–5.
Pollack A, et al. Viral myocarditis–diagnosis, treatment options, and current controversies. Nat Rev Cardiol. 2015;12(11):670–80.
Hang W, et al. Fulminant myocarditis: a comprehensive review from etiology to treatments and outcomes. Signal Transduct Target Ther. 2020;5(1):287.
European Medicines Agency. EMA/CHMP Guidance document on use of medicinal products for the treatment and prophylaxis of biological agents that might be used as weapons of bioterrorism. European Medicines Agency; 2014.
Rathjen NA, Shahbodaghi SD. Bioterrorism. Am Fam Physician. 2021;104(4):376–85.
Ellis J, et al. Tularemia. Clin Microbiol Rev. 2002;15(4):631–46.
Tarnvik A, Chu MC. New approaches to diagnosis and therapy of tularemia. Ann N Y Acad Sci. 2007;1105:378–404.
Evans ME, et al. Tularemia: a 30-year experience with 88 cases. Medicine (Baltimore). 1985;64(4):251–69.
Frischknecht M, et al. Tularemia: an experience of 13 cases including a rare myocarditis in a referral center in Eastern Switzerland (Central Europe) and a review of the literature. Infection. 2019;47(5):683–95.
World Health Organization. WHO Guidelines on tularaemia. World Health Organization: Geneva; 2007. https://apps.who.int/iris/handle/10665/43793
Tärnvik A, Berglund L. Tularaemia. Eur Respir J. 2003;21(2):361–73.
Maurin M. Francisella tularensis, Tularemia and serological diagnosis. Front Cell Infect Microbiol. 2020;10: 512090.
Ammirati E, et al. State-of-the-art of endomyocardial biopsy on acute myocarditis and chronic inflammatory cardiomyopathy. Curr Cardiol Rep. 2022;24(5):597–609.
Felker GM, et al. The spectrum of dilated cardiomyopathy. The Johns Hopkins experience with 1,278 patients. Medicine (Baltimore). 1999;78(4):270–83.
Cooper LT, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. J Am Coll Cardiol. 2007;50(19):1914–31.
Hestvik G, et al. The status of tularemia in Europe in a one-health context: a review. Epidemiol Infect. 2015;143(10):2137–60.
Acknowledgements
The authors would like to thank Dr. Jan Axelsson at Diagnostic Radiology, Department of Radiation Sciences at Umeå University, Umeå, Sweden for his kind support in creating the radiological images.
Funding
Open access funding provided by Umea University.
Author information
Authors and Affiliations
Contributions
ATB and AE were responsible for the patient’s medical care during admission to the hospital and analyzed and interpreted the patient data. ATB wrote the manuscript with support from CF, AE, and AJ. AE provided senior cardiological expertise. CF interpreted the radiological examinations and provided senior radiological expertise. AJ provided senior expertise in infectious medicine with a particular focus on tularemia. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
The written informed consent for publication of the case and images was obtained from the patient.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Medicine
Learning Points
- Myocarditis is an inflammatory disease of the myocardium and can be caused by a variety of agents, most commonly cardiotropic viruses.
- Tularemia is a multi-host, highly contagious, vector-borne disease caused by Francisella tularensis, which can cause a wide range of symptoms in humans and therefore be difficult to recognize.
- Acute myocarditis is a very rare complication to tularemia and can mimic other cardiac manifestations such as acute coronary syndrome or Takotsubo’s cardiomyopathy.
- Left untreated, tularemia has high morbidity but can be successfully treated with non-beta-lactamase antibiotics.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bäck, A.T., Flygare, C., Eriksson, A. et al. Acute Myocarditis Caused by Francisella tularensis: a Case Report. SN Compr. Clin. Med. 5, 105 (2023). https://doi.org/10.1007/s42399-023-01436-w
Accepted:
Published:
DOI: https://doi.org/10.1007/s42399-023-01436-w