
Abstract
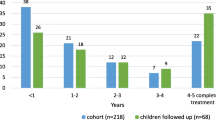
The Ponseti method of clubfoot treatment has revolutionized the clubfoot treatment. Participation of non-government organizations (NGOs) has helped expand the reach of clubfoot treatment and improve the outcomes. Establishing new clubfoot clinics may have their teething problems, which need to be anticipated and addressed for their efficient functioning. This retrospective observational study was performed using records of children enrolled in the initial 4 years of an NGO supported clubfoot clinic at a teaching public hospital. Patient details were analyzed to act as surrogate indicators of the challenges faced in the efficient delivery of care at this new clubfoot clinic. Furthermore, the authors’ suggestions would help other clinicians in starting a clubfoot clinic more effectively. Three hundred eighty-four children were enrolled in the initial 4 years. Two hundred ninety-seven children completed their cast treatment. Two hundred four (53.12%), which was more than half of all the enrolled children, had received some prior treatment. Only 86 (22.4%) children followed up for 4 years or more. A high dropout rate at different stages of treatment and follow-up was also noticed. The high dropout rate with the knowledge that most of the enrolled children had some prior treatment points to the clinicians’ and counselors’ failure to educate the parents. Electronic instead of manual data entry would play a role in tracing children in the setting of a new clubfoot clinic. A dedicated team of clinicians and counselors right from the beginning would help in gaining parental trust. Field visits by volunteers might be a useful additional strategy in improving the follow-up and the overall results.
Similar content being viewed by others
Data Availability
The data in the form of an Excel sheet can be made available on request.
References
Owen RM, Capper B, Lavy C. Clubfoot treatment in 2015: a global perspective. BMJ Glob Health. 2018;3(4):e000852. https://doi.org/10.1136/bmjgh-2018-000852.
van Bosse HJ. Ponseti treatment for clubfeet: an international perspective. Curr Opin Pediatr. 2011;23(1):41–5. https://doi.org/10.1097/MOP.0b013e328342112a.
Shabtai L, Specht SC, Herzenberg JE. Worldwide spread of the Ponseti method for clubfoot. World J Orthop. 2014;5:585–90. https://doi.org/10.5312/wjo.v5.i5.585.
Sharma P, Verma R, Gohiya A, Gaur S. Analysis of the effectiveness of a non- governmental organization in supporting clubfoot clinic at a tertiary care center. SICOT-J. 2015;1:8–10. https://doi.org/10.1051/sicotj/2015008.
Morin ML, Hoopes DM, Szalay EA. Positive communication paradigm decreases early recurrence in clubfoot treatment. J Pediatr Orthop. 2014;34(2):219–22. https://doi.org/10.1097/BPO.0000000000000080.
Owen RM, Penny JN, Mayo A, Morcuende J, Lavy CB. A collaborative public health approach to clubfoot intervention in 10 low-income and middle-income countries: 2- year outcomes and lessons learnt. J Pediatr Orthop B. 2012;21(4):361–5. https://doi.org/10.1097/BPB.0b013e3283504006.
Johnson RR, Friedman JM, Becker AM, Spiegel DA. The Ponseti method for clubfoot treatment in low and middle-income countries: a systematic review of barriers and solutions to service delivery. J Pediatr Orthop. 2017;37(2):e134–9. https://doi.org/10.1097/BPO.0000000000000723.
Poudel RR, Kumar VS, Tiwari V, Subramani S, Khan SA. Factors affecting compliance to hospital visit among clubfoot patients: a cross-sectional study from a tertiary referral clubfoot clinic in the developing country. J Orthop Surg. 2019;27(1):2309499019825598. https://doi.org/10.1177/2309499019825598.
Gadhok K, Belthur MV, Aroojis AJ, Cook T, Oprescu F, Ranade AS, et al. Qualitative assessment of the challenges to the treatment of idiopathic clubfoot by the Ponseti method in urban India. Iowa Orthop J. 2012;32:135–40.
Agarwal A, Gupta N. Does initial Pirani score and age influence number of Ponseti casts in children? Int Orthop. 2014;38(3):569–72. https://doi.org/10.1007/s00264-013-2155-3.
Acknowledgments
The authors want to acknowledge CURE India for their continued support in counseling services and free of cost braces for children with clubfeet.
Author information
Authors and Affiliations
Contributions
Study conceptualization was by VG and PB. Initial literature search was by PB, AJ, and NM. Data extraction from the records was done by PB, AJ, and NM. Data analysis was done by PB and VG. Manuscript preparation was done by PB. VG, AJ, and NM did proof reading and manuscript editing. All the authors approved the manuscript before its submission.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they no conflicts of interest.
Ethics Approval
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. As the study involved review of medical records, formal ethical approval was waived off by the departmental review board.
Consent to Participate
Informed consent was obtained from the parents of the children enrolled in the clinic.
Consent for Publication
Informed consent for use of data for scientific purposes was obtained from the parents of the children enrolled in the clinic.
Code Availability
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Surgery
Rights and permissions
About this article

Cite this article
Behera, P., Gupta, V., Mishra, N. et al. Challenges in Establishing a New Clubfoot Clinic at a Public Hospital: an Appraisal of the Initial 384 Cases. SN Compr. Clin. Med. 3, 632–636 (2021). https://doi.org/10.1007/s42399-021-00747-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42399-021-00747-0