
Key summary points
To investigate individual major comorbid diseases as predictors of infection after hip fracture surgery.
AbstractSection FindingsInfection risk was higher among patients having any comorbid disease compared to patients without comorbid disease. The most important predictors of infection after hip fracture surgery were renal disease, depression/anxiety, and chronic pulmonary disease.
AbstractSection MessageComorbid diseases varied in importance as predictors of infection after hip fracture surgery.
Abstract
Purpose
Comorbidity level is a predictor of infection in the first 30 days after hip fracture surgery. However, the roles of individual comorbid diseases as predictors of infection remain unclear. We investigated individual major comorbid diseases as predictors of infection after hip fracture surgery.
Methods
We obtained Danish population-based medical registry data for patients undergoing hip fracture surgery (2004–2018). Information was obtained on 27 comorbidities, included in various comorbidity indices, 5 years before surgery. The primary outcome was any hospital-treated infection within 30 days after surgery. Cumulative incidence of infection was calculated by considering death as competing risk. We used logistic regression to compute mutually adjusted odds ratios with 95% confidence interval for infection.
Results
Of 92,239 patients with hip fracture, 71% were women, and the median age was 83 years. The most prevalent comorbidities were hypertension (23%), heart arrhythmia (15%), and cerebrovascular disease (14%). The 30-day incidence of infection was 15% and 12% among the total cohort and among patients with no record of comorbidities, respectively. Infection incidence was highest among patients with renal disease (24%), depression/anxiety (23%), and chronic pulmonary disease (23%), and lowest among patients with metastatic solid tumor (15%). Adjusted odds ratios of infection ranged from 0.94 [0.80–1.10] for metastatic solid tumor to 1.77 [1.63–1.92] for renal disease.
Conclusion
Most comorbid diseases were predictors of infection after surgery for hip fracture. Awareness of patients’ comorbidity profiles might help clinicians initiate preventive measures or inform patients of their expected risk.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hip fracture is a serious and frequent injury. The global annual incidence of hip fracture was 14 million in 2019 [1] and is predicted to continue to increase until 2050 with the aging of the world’s population [2].
The global average total cost of healthcare and social care 1 year after hip fracture has been estimated to be $43,669 per patient [3]. In addition, the 1-year mortality has been reported to be approximately 30% [4, 5]. Complications are frequent after hip fracture surgery and have been associated with diminished health status and quality of life, high healthcare and social costs, and elevated mortality [3, 4, 6]. Infections, including pneumonia and urinary tract infection, are among the most frequent complications and highly associated with mortality after hip fracture surgery [7, 8]. From 2005 to 2016, the infection risk increased among patients with hip fractures, whereas a similar trend was not observed in the general population of the same age and sex [9]. This finding is of major concern, because the 30-day mortality among patients with hip fractures with any infection is more than twice that of infection-free patients with hip fractures [10]. Thus, accurate identification of patients with hip fractures at high infection risk is of increasing importance.
Comorbidity level, as measured by the Charlson comorbidity index (CCI) [11], is associated with elevated infection risk after surgery for hip fracture [12]. However, the CCI does not include potentially important predictors of infection, such as depression [13] or thyroid disease [14]. Furthermore, the CCI was developed for predicting mortality in a population of patients with breast cancer [11]. Therefore, the assigned weights used to calculate the CCI summary score may overestimate or underestimate the importance of the individual comorbid diseases in the context of infection in patients with hip fracture.
Relying on the comorbidity indices may mask the potential important effects of individual comorbid diseases, thus hindering stratified preventive interventions. However, relative and absolute measures of infection after hip fracture surgery based on individual comorbid diseases are rare in the current literature, although both measures are highly clinically relevant for evaluating effects on healthcare systems and patients. Several studies in patients with hip fracture have reported an association between selected comorbid diseases and the risk of specific infections [15,16,17,18,19], but with conflicting results [16,17,18]. Those studies have been hindered by methodological problems including small sample sizes [15,16,17,18,19], potential selection bias [15,16,17,18,19], and loss to follow-up [19]. Furthermore, few comorbid diseases or comorbidity measures have been evaluated [15,16,17,18,19].
Therefore, we investigated a wide selection of prevalent major comorbid diseases and their roles as predictors of infection within 30 days after hip fracture, using data from Danish health registries.
Method
Setting and data sources
This study was set in Denmark, which has approximately 5.9 million residents [20]. The tax supported Danish healthcare is universally accessible and includes general practitioners and hospitals. We obtained data from the following nationwide medical registries: 1) the Danish Multidisciplinary Hip Fracture Registry (DMHFR), which has recorded information on patient characteristics, surgery, quality indicators, and prognostic factors for all patients with hip fractures ≥ 65 years of age since 2004 [21, 22]; 2) the Danish Civil Registration System, which has recorded information on vital and civil status, and residence for all Danish residents since 1968, using a unique personal identifier assigned to all Danish residents enabling linkage between all Danish medical registries on individual level [23]; 3) the Danish National Patients Registry [24], which has recorded information on in-hospital treatments and surgical procedures performed, as well as 1 primary and as many as 19 secondary discharge diagnoses, since 1977, and information on outpatient clinic discharges and emergency department visits since 1995. The discharge diagnoses have been coded according to the International Classification of Diseases 10th Edition (ICD-10) since 1994.
Study cohort
The study cohort was identified from the DMHFR and included 92,239 patients treated surgically for a first unilateral hip fracture between January 2004 and October 2018.
Comorbid diseases
Comorbidity indices including the CCI [11], the Elixhauser Comorbidity Index [25], the Rx-risk Comorbidity Index [26], and the Nordic Multimorbidity Index [27] guided the selection and definition of chronic comorbid diseases, for example diabetes, and other comorbid conditions, for example anemia, as potential predictors. This was done to improve the comparability of our results to that of other studies using these indices. Information on comorbid diseases was obtained for each patient from the ICD-10 diagnosis codes recorded in the Danish National Patient Registry in the 5 years before the date of hip fracture surgery. Both primary and secondary diagnoses from in-hospital and outpatient clinic visits were used. Diagnosis codes recorded at emergency department visits were excluded, because of potentially low validity, given that non-specific symptom-based diagnoses are the most frequent diagnoses in Danish emergency department visits [28]. As comorbid diseases accumulate in patients over time, the prevalence increases with an increasing length of the lookback period. However, the length of the lookback period has been shown to have minimal effects on the ability of the comorbidity indices to predict infections among patients with hip fractures [29]. A lookback period of 5 years was chosen to ensure applicability in clinical practice, aiming to identify most patients’ comorbidity diagnoses, under the assumption that past information on diagnoses would become harder to collect in clinic with prolonged lookback period. To ensure statistical precision and clinical relevance, we included only comorbid diseases with a prevalence > 1%; consequently, comorbid diseases, such as HIV/AIDS (prevalence 0.02%) and hemiplegia (prevalence 0.2%), were not included. In total, 27 comorbid diseases were evaluated. For two diseases, a distinction was made by severity: patients with diabetes were categorized as either having uncomplicated or complicated diabetes, and patients with solid tumors were categorized by metastasis status, as having either no or any metastatic solid tumors. Further details, including diagnosis codes and descriptions of the diagnoses for each of the 27 comorbid diseases, are provided in Online Resource 1.
Infection
The primary outcome was defined as any hospital-treated infection recorded in the Danish National Patient Registry. These infections included common and serious viral and bacterial infections, such as pneumonia, urinary tract infection, skin infection, surgical-site infection, or gastrointestinal infection, as well as rarer infections, parasitic or mycotic infections. The primary outcome was identified as primary and secondary discharge diagnoses of any type of infection during in-hospital and outpatient clinic visits. Infection diagnosis codes recorded during emergency department visits were also included, on the basis of the assumption that infection is an acute disease easily diagnosed in acute settings, according to characteristic symptoms (e.g., fever and cough) and readily accessible paraclinical tests (e.g., chest X-ray, or urine and blood samples), and can be treated in an emergency department setting [30]. The primary outcome of any hospital-treated infection is important from a patient perspective since any infection after hip fracture surgery is a serious complication associated with poorer prognosis [10]. Secondary outcomes of pneumonia and urinary tract infection were also identified because these infections are prevalent and are among the most common causes of death in patients with hip fracture and thus are of particularly high clinical relevance [7, 8]. Lists of diagnosis codes used for the definition of outcomes in this study are available in the Online Resource 1.
Variables
Information on surgery date was collected from the DMHFR. From the Danish Civil Registration system, patient age and sex were collected at the surgery date, whereas dates of death or emigration were collected within the study period. Age was categorized into three groups: 65–74, 75–84, and ≥ 85 years.
Statistical analysis
The number and prevalence of baseline characteristics were reported for the total cohort.
For both primary and secondary infection outcomes, patients were followed from baseline, defined as the date of surgery, until the date of infection, migration, death, or 30 days after surgery, whichever came first.
Numbers of incident infection cases and the cumulative incidence of infection, considering death a competing risk, were calculated for the total cohort, stratified by each selected comorbid disease, and for patients with no record of comorbid diseases [31].
Using logistic regression, we estimated crude odds ratios (ORs) for infection according to each of the selected comorbid diseases, comparing patients with each selected comorbid disease (i.e., exposed) to patients without the selected comorbid disease (i.e., unexposed) in 27 bivariate models. The ORs at baseline can be interpreted as the odds of infection within the first 30 days after surgery among exposed patients compared with unexposed patients (e.g., patients with vs. without a record of renal disease) [32].
In addition, a multivariate model including all 27 selected comorbid diseases, sex, and age as a continuous variable, was computed with logistic regression. From the multivariate model, mutual adjusted ORs as a measure of relative risks were estimated. These adjusted OR can be interpreted as the direct effect of an individual comorbid disease, adjusted for confounding and/or mediation through age, sex, and the other 26 comorbid diseases included in the model [33].
To evaluate possible effect modification by associated factors and allow for stratified evaluation of infection risk, we performed stratified analyses estimating the cumulative incidence and adjusted ORs by age and sex for the primary outcome.
Estimates were presented with 95% confidence intervals (CIs). Analysis was performed using R software (version 2022.02.1).
This article follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) and the Reporting of studies Conducted with Observational Routinely collected Data (RECORD) guidelines for cohort studies.
Results
Among the total cohort (n = 92,239), the median age was 83 years, 71% of patients were women, and 36% had no record of comorbidity within the past 5 years. The most prevalent comorbid diseases were hypertension (23%), heart arrhythmia (15%), and cerebrovascular disease (14%), followed by chronic pulmonary disease, any solid tumors, and fluid/electrolyte disorders, with a prevalence of 10–11% (Table 1).
Any infection
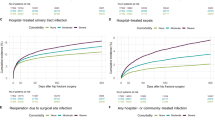
A total of 14,199 patients were treated in hospital for any infection within the first 30 days after surgery, corresponding to a cumulative incidence of 15%. For patients with no record of any of the 27 comorbid diseases, the cumulative incidence of infection was 12%.
The cumulative incidence of infection was highest among patients with renal disease (24%), depression/anxiety (23%), and chronic pulmonary disease (23%). The lowest cumulative incidences were found among patients with metastatic solid tumors (15%), any solid tumors (16%), and rheumatic disease (17%) (Fig. 1).

Bar chart plotting 30-day cumulative incidence of any infection for the total cohort, and with stratification by no comorbid disease or selected comorbidities
The crude OR for infection varied between 0.94 (95% CI 0.80–1.10) for solid metastatic tumors and 1.77 (95% CI 1.63–1.92) for renal disease. The second, third, and fourth highest crude ORs were 1.71 (95% CI 1.62–1.80) for chronic pulmonary disease, 1.65 (95% CI 1.53–1.77) for depression/anxiety, and 1.58 (95% CI 1.39–1.79) for hypotension (Fig. 2).

Forest plot of crude odds ratios for any infection, comparing patients with vs. without each selected comorbidity, at 30-day follow-up. OR odds ratio, CI confidence interval
The adjusted OR varied between 0.93 (95% CI 0.88–0.99) for any solid tumors and 1.61 (95% CI 1.52–1.70) for chronic pulmonary disease. The second, third, and fourth highest adjusted ORs were 1.39 (95% CI 1.29–1.51) for depression/anxiety, 1.32 (95% CI 1.21–1.45) for renal disease, and 1.28 (95% CI 1.17–1.39) for complicated diabetes (Fig. 3).

Forest plot of adjusted odds ratios for any infection at 30-day follow-up, mutually adjusted for age, sex, and comorbid diseases. OR odds ratio, CI confidence interval
Pneumonia
Within 30 days after surgery, 5784 patients had an incident hospital record of pneumonia. The cumulative incidence of pneumonia was 6% for the total cohort and 4% for patients with no comorbid disease. The highest cumulative incidence of pneumonia was observed among patients with chronic pulmonary disease (12%), renal disease (11%), and hypotension (10%).
The adjusted ORs varied between 0.83 (95% CI 0.62–1.09) for liver disease and 2.22 (95% CI 2.07–2.39) for chronic pulmonary disease (Online Resource 2).
Urinary tract infection
In the first month postoperatively, 6614 patients had an incident hospital-treated urinary tract infection. The cumulative incidence of urinary tract infection was 7% for the overall cohort and 6% among patients with no comorbid disease. The cumulative incidence was highest among patients with depression/anxiety (11%) and hypotension (10%). The adjusted ORs varied between 0.81 (95% CI 0.62–1.04) for metastatic solid tumors and 1.41 (95% CI 1.26–1.56) for depression/anxiety (Online Resource 2).
Stratified analysis
The cumulative incidence of infection for the total cohort and for patients with no comorbid disease increased with age, whereas cumulative incidence by selected comorbid disease increased or varied slightly across age groups, except for dementia, for which the cumulative incidence decreased with increasing age. In a comparison of the oldest patients (≥ 85 years) to the youngest patients (65–74 years), most adjusted ORs decreased with increasing age (Online Resource 2).
The cumulative incidence overall, among patients with no comorbid disease, and by selected comorbid diseases, was higher among male than female patients. In female patients, most adjusted ORs were similar to or higher than those in male patients (Online Resource 2).
Discussion
Most of the selected chronic comorbid diseases were predictors of infection in the first postoperative 30 days among patients with hip fracture. The highest absolute risks of any infection were observed among patients with chronic pulmonary disease, renal disease, and depression/anxiety.
Comparison to existing research
The prevalence of some of the investigated diseases was comparable to those previously reported (e.g., peripheral vascular disease of 5.9% vs. 4.6–8.9% [34,35,36]), while others differed noticeably (e.g., diabetes 8.2% vs. 12.5–24% or chronic pulmonary disease 10.5% vs. 12–23% [34,35,36]). These differences in prevalence are likely explained by differences between our study population and the populations of previous studies, including differences in age (aged ≥ 65 years vs. aged < 90 years [34] or aged ≥ 55 years [35]), gender (men and women vs. women only [35]), and nationality (Denmark vs. United States [34, 36] or Norway [35]). Additional explanations for the differences in prevalence include the applied methods and definitions used for the detection of comorbid diseases, e.g., data source (registry data vs. viewing medical records [34]), diagnosis codes (ICD-10 vs. ICD-9 [34, 36]), and lookback periods (5 years vs. 1–7 years [35] or undisclosed [34, 36]).
Few studies have evaluated the associations of one to five selected comorbid diseases and specific infections (e.g., pneumonia or urinary tract infection) among patients with hip fractures [15,16,17,18,19]. Our findings on pneumonia and urinary tract infection after hip fracture are in agreement with findings from some [15, 16, 19] but not all [15, 17, 18] previous studies. For example, the presence of diabetes as a predictor of pneumonia is supported by some previous studies [16] but not others [17, 18]. Discrepancies in the results between our study and previous studies are likely to be explained by differences in methodology, including differences in study type (e.g., non-intervention vs. intervention studies [18]), follow-up time (e.g., 30-day follow-up vs. in-hospital follow-up [17]), and measurement of outcomes (e.g., recorded diagnosis codes vs. requirement for antibiotic treatment [17, 18] or positive paraclinical tests suggesting infection [18]). In addition, differences in the sample size (92,239 vs. 86–806 patients [15,16,17,18,19]), selection of the study population (e.g., nationwide vs. single center [17, 18] or use of more exclusion criteria [18]), data collection, data availability, case mix (patients ≥ 65 vs. ≥ 70 [17] years of age), and healthcare setting might have introduced selection and information biases, or weakened the generalizability among study populations.
Interpretation and perspectives
The associations we found may be explained through both causative mechanisms and factors such as age, sex, and lifestyle factors, and through association with other comorbidities [37]. For example, chronic pulmonary disease is a well-known risk factor for pneumonia and therefore, as expected, was a strong predictor of pneumonia in our study [38, 39]. We also found depression/anxiety to be an important predictor. Depression has been reported as a risk factor for infection; however, depression, particularly later in life, might be strongly associated with age-associated comorbid diseases [40, 41]. However, depression/anxiety remained an important predictor after adjustment for comorbid disease, age, and sex. Other factors, including smoking status, reduced immune status, and frailty might explain an increased vulnerability to infection among those with depression/anxiety [42,43,44].
The individual comorbid diseases could be considered markers of frailty or an underlying burden of disease [45, 46]. This could partially explain the associations observed for comorbid diseases that are not well-established risk factors for infection, such as hypotension, or comorbid diseases that are more transitory and potentially not present at time of surgery, e.g., fluid or electrolyte disorder or anemia. Frailty, which is prevalent in the older population, is generally described as a state of diminished reserve and physical stamina, as well as increased vulnerability to adverse health related outcomes [45]. Frailty is not synonymous with comorbidity or disability, although all three conditions are closely related [45]. We were not able to accurately measure frailty for several reasons. First, although tools for evaluating frailty exist and are increasingly implemented, particularly in geriatric medicine, consensus is lacking on one single well-defined and well-recognized measure of frailty [47, 48]. Second, in the available registries, frailty tests have not been documented. Third, the available tools for calculating frailty scores that would be applicable to our data rely largely on comorbidity status and other proxies [47]. Fourth, patients may present with serious comorbidity without being frail [45].
Unexpectedly, patients with comorbid diseases, such as metastatic solid tumors or dementia, had the lowest cumulative incidence of any infection. Metastatic solid tumors were associated to reduced infection risk in male patients, and dementia was associated to reduced risk in patients ≥ 85 years of age. However, these estimates appear to have been biased by the competing risk of death [49]. Factors such as delay in clinical recognition of infection or missed diagnoses, perhaps especially among those with dementia, metastatic tumors, or advanced age, could have contributed to an increased risk of mortality. Moreover, patients presenting with infections can be admitted to a hospital, treated in the community setting, or even given end of life care—a choice likely to depend on the patient’ comorbidities. Thus, our results are likely to have been influenced by the decisions regarding level of care.
In this study, we investigated comorbid diseases diagnosed or treated in the hospital setting. However, some milder comorbid diseases may be exclusively diagnosed and treated in general practice, and certain comorbid diseases are known to be underreported, e.g., dementia [50]. This could have contributed to the high cumulative incidence of infections among those we identified as having no comorbid disease.
Our results on the incidence and ORs for a wide range of chronic comorbid diseases may be relevant in clinical decision-making, considering patient-specific information, for decreasing infection rates in patients with hip fractures. Thus, clinicians might consider quality of care in patients with comorbidities, as previous studies reported an inverse association between increasing comorbidity level and fulfillment of quality-of-care indicators relevant for infection prevention, such as post-surgical mobilization [51, 52]. Interventions consisting of patient tailored programs including education and involvement of family caregivers or implementation of early transitional care programs to continue the multidisciplinary effort in the home-setting potentially could benefit patients at high infection risk [53, 54]. As such, the results of this study may help clinicians plan infection-preventive preoperative and postoperative care, initiate surveillance for early detection of infections, or inform patients of their expected infection risk.
Methodological considerations
This study has limitations. First, our study cohort was based on data from the DMHFR [22]. Although the completeness and coverage of the DMHFR is unknown, reporting to the register is mandatory and partly automated, and orthopedic departments had economic incentives to report the surgeries performed in the entirety of the study period. Thus, the capture rate is believed to be high, and the selection bias is likely to be minimal.
Second, bias from misclassification of any variables cannot be excluded. The event of hip fracture surgery, as recorded in the DMHFR, has a positive predictive values (PPV) of 100% [22].
Although there is an economic incentive for the hospitals to report diagnoses to the DNPR, the validity of most comorbid diseases included in our study was evaluated previously using various population samples. The reported PPVs ranged between 80 and 100%, indicating a low level of over-reporting [24, 55,56,57]. It is unknown whether the PPVs of the remaining comorbid diseases in the DNPR are at the same level.
A study in patients with cancer has reported PPVs of 98% for any infection and 93% for pneumonia in the Danish National Patient Registry [58]. Infection diagnoses from emergency department contacts have been reported to have a PPV of 78% [30].
We did not have access to information from general practice consultation visits, because data on diagnoses given in general practice are not recorded in any registry. Therefore, this study was restricted to comorbid diseases and infections serious enough to require hospital contact. Consequently, our estimated prevalences of hospital-diagnosed comorbid diseases are lower than the prevalence would have been if we had been able to include the milder cases from general practice and undiagnosed cases. Under the assumption that hospital-diagnosed comorbid diseases are more severe than those solely diagnosed in general practice, these hospital-diagnosed comorbid diseases might be stronger predictors of severe infection and thus infection treated in hospital. However, the opposite may apply for certain comorbid diseases, e.g., severe dementia, where the clinician might opt for infection treatment in the community setting.
Third, the results of our study are best generalized to populations with similar case mix and from countries with similar healthcare setting and hip fracture treatment as that of our study population.
Conclusion
Incident infection was present in 15% of patients in the first 30 days after hip fracture surgery. Moreover, 71% of patients with hip fractures with infection had one or more comorbid diseases. Our results indicated that most comorbid diseases are important predictors of a wide range of infections in patients within the first 30 days after surgery for hip fracture.
Data availability
To protect the privacy of patients, it is by Danish law prohibited to make individual level data publicly available.
References
Wu AM et al (2021) Global, regional, and national burden of bone fractures in 204 countries and territories, 1990–2019: a systematic analysis from the global burden of disease study 2019. Lancet Healthy Longev 2(9):e580–e592. https://doi.org/10.1016/s2666-7568(21)00172-0
Veronese N, Maggi S (2018) Epidemiology and social costs of hip fracture. Injury 49(8):1458–1460. https://doi.org/10.1016/j.injury.2018.04.015
Williamson S, Landeiro F, McConnell T, Fulford-Smith L, Javaid MK, Judge A et al (2017) Costs of fragility hip fractures globally: a systematic review and meta-regression analysis. Osteoporos Int 28(10):2791–2800. https://doi.org/10.1007/s00198-017-4153-6
Roche JJ, Wenn RT, Sahota O, Moran CG (2005) Effect of comorbidities and postoperative complications on mortality after hip fracture in elderly people: prospective observational cohort study. BMJ 331(7529):1374. https://doi.org/10.1136/bmj.38643.663843.55
Pedersen AB, Ehrenstein V, Szépligeti SK, Lunde A, Lagerros YT, Westerlund A et al (2017) Thirty-five-year trends in first-time hospitalization for hip fracture, 1-year mortality, and the prognostic impact of comorbidity: a Danish Nationwide Cohort Study, 1980–2014. Epidemiology 28(6):898–905. https://doi.org/10.1097/ede.0000000000000729
Peeters CM, Visser E, Van de Ree CL, Gosens T, Den Oudsten BL, De Vries J (2016) Quality of life after hip fracture in the elderly: a systematic literature review. Injury 47(7):1369–1382. https://doi.org/10.1016/j.injury.2016.04.018
Folbert EC, Hegeman JH, Gierveld R, van Netten JJ, Velde DV, Ten Duis HJ et al (2017) Complications during hospitalization and risk factors in elderly patients with hip fracture following integrated orthogeriatric treatment. Arch Orthop Trauma Surg 137(4):507–515. https://doi.org/10.1007/s00402-017-2646-6
Rohold CK, Lauritzen JB, Jørgensen HL (2021) Causes of death among 93,637 hip fracture patients—data based on the Danish National Registry of causes of death. Eur J Trauma Emerg Surg. https://doi.org/10.1007/s00068-021-01791-0
Kjørholt KE, Johnsen SP, Kristensen NR, Prieto-Alhambra D, Pedersen AB (2019) Increasing risk of hospital-treated infections and community-based antibiotic use after hip fracture surgery: a nationwide study 2005–2016. J Bone Miner Res 34(3):437–446. https://doi.org/10.1002/jbmr.3620
Kjørholt KE, Kristensen NR, Prieto-Alhambra D, Johnsen SP, Pedersen AB (2019) Increased risk of mortality after postoperative infection in hip fracture patients. Bone 127:563–570. https://doi.org/10.1016/j.bone.2019.07.023
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40(5):373–383. https://doi.org/10.1016/0021-9681(87)90171-8
Gadgaard NR, Varnum C, Nelissen R, Vandenbroucke-Grauls C, Sørensen HT, Pedersen AB (2023) Comorbidity and risk of infection among patients with hip fracture: a Danish population-based cohort study. Osteoporos Int. https://doi.org/10.1007/s00198-023-06823-6
Hu T, Zhao X, Wu M, Li Z, Luo L, Yang C et al (2022) Prevalence of depression in older adults: a systematic review and meta-analysis. Psychiatry Res 311:114511. https://doi.org/10.1016/j.psychres.2022.114511
Kocełak P, Mossakowska M, Puzianowska-Kuźnicka M, Sworczak K, Wyszomirski A, Handzlik G et al (2022) Prevalence and risk factors of untreated thyroid dysfunctions in the older Caucasian adults: results of PolSenior 2 survey. PLoS ONE 17(8):e0272045. https://doi.org/10.1371/journal.pone.0272045
Hälleberg Nyman M, Johansson JE, Persson K, Gustafsson M (2011) A prospective study of nosocomial urinary tract infection in hip fracture patients. J Clin Nurs 20(17–18):2531–2539. https://doi.org/10.1111/j.1365-2702.2011.03769.x
Yu Y, Zheng P (2022) Determination of risk factors of postoperative pneumonia in elderly patients with hip fracture: what can we do? PLoS ONE 17(8):e0273350. https://doi.org/10.1371/journal.pone.0273350
Salarbaks AM, Lindeboom R, Nijmeijer W (2020) Pneumonia in hospitalized elderly hip fracture patients: the effects on length of hospital-stay, in-hospital and thirty-day mortality and a search for potential predictors. Injury 51(8):1846–1850. https://doi.org/10.1016/j.injury.2020.05.017
Chang SC, Lai JI, Lu MC, Lin KH, Wang WS, Lo SS et al (2018) Reduction in the incidence of pneumonia in elderly patients after hip fracture surgery: an inpatient pulmonary rehabilitation program. Medicine (Baltimore) 97(33):e11845. https://doi.org/10.1097/md.0000000000011845
Delgado A, Cordero GGE, Marcos S, Cordero-Ampuero J (2020) Influence of cognitive impairment on mortality, complications and functional outcome after hip fracture: dementia as a risk factor for sepsis and urinary infection. Injury 51(Suppl 1):S19-s24. https://doi.org/10.1016/j.injury.2020.02.009
Statistics Denmark: Population figures 2023. https://www.dst.dk/en/Statistik/emner/borgere/befolkning/befolkningstal. Accessed 2023
Kristensen PK, Röck ND, Christensen HC, Pedersen AB (2020) The Danish multidisciplinary hip fracture registry 13-year results from a population-based cohort of hip fracture patients. Clin Epidemiol 12:9–21. https://doi.org/10.2147/clep.S231578
Hjelholt TJ, Edwards NM, Vesterager JD, Kristensen PK, Pedersen AB (2020) The positive predictive value of hip fracture diagnoses and surgical procedure codes in the Danish multidisciplinary hip fracture registry and the Danish national patient registry. Clin Epidemiol 12:123–131. https://doi.org/10.2147/clep.S238722
Schmidt M, Pedersen L, Sørensen HT (2014) The Danish civil registration system as a tool in epidemiology. Eur J Epidemiol 29(8):541–549. https://doi.org/10.1007/s10654-014-9930-3
Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT (2015) The Danish national patient registry: a review of content, data quality, and research potential. Clin Epidemiol 7:449–490. https://doi.org/10.2147/clep.S91125
Elixhauser A, Steiner C, Harris DR, Coffey RM (1998) Comorbidity measures for use with administrative data. Med Care 36(1):8–27. https://doi.org/10.1097/00005650-199801000-00004
Pratt NL, Kerr M, Barratt JD, Kemp-Casey A, Kalisch Ellett LM, Ramsay E et al (2018) The validity of the Rx-Risk comorbidity index using medicines mapped to the anatomical therapeutic chemical (ATC) classification system. BMJ Open 8(4):e021122. https://doi.org/10.1136/bmjopen-2017-021122
Kristensen KB, Lund LC, Jensen PB, Broe A, Rotbain E, Damkier P et al (2022) Development and validation of a nordic multimorbidity index based on hospital diagnoses and filled prescriptions. Clin Epidemiol 14:567–579. https://doi.org/10.2147/clep.S353398
Al-Mashat H, Lindskou TA, Møller JM, Ludwig M, Christensen EF, Søvsø MB (2022) Assessed and discharged—diagnosis, mortality and revisits in short-term emergency department contacts. BMC Health Serv Res 22(1):816. https://doi.org/10.1186/s12913-022-08203-y
Storbjerg DK, Gadgaard NR, Pedersen AB (2024) Any infection among patients with hip fracture: predictive ability of Charlson, Elixhauser, Rx-Risk, and nordic comorbidity indices. Surgeon 22(1):e61–e68. https://doi.org/10.1016/j.surge.2023.11.004
Henriksen DP, Nielsen SL, Laursen CB, Hallas J, Pedersen C, Lassen AT (2014) How well do discharge diagnoses identify hospitalised patients with community-acquired infections? A validation study. PLoS ONE 9(3):e92891. https://doi.org/10.1371/journal.pone.0092891
Buzkova P, Barzilay JI, Mukamal KJ (2019) Assessing risk factors of non-fatal outcomes amid a competing risk of mortality: the example of hip fracture. Osteoporos Int 30(10):2073–2078. https://doi.org/10.1007/s00198-019-05048-w
George A, Stead TS, Ganti L (2020) What’s the risk: differentiating risk ratios, odds ratios, and hazard ratios? Cureus 12(8):e10047. https://doi.org/10.7759/cureus.10047
Green MJ, Popham F (2019) Interpreting mutual adjustment for multiple indicators of socioeconomic position without committing mutual adjustment fallacies. BMC Public Health 19(1):10. https://doi.org/10.1186/s12889-018-6364-y
Bohl DD, Basques BA, Golinvaux NS, Baumgaertner MR, Grauer JN (2014) Nationwide inpatient sample and national surgical quality improvement program give different results in hip fracture studies. Clin Orthop Relat Res 472(6):1672–1680. https://doi.org/10.1007/s11999-014-3559-0
Lunde A, Tell GS, Pedersen AB, Scheike TH, Apalset EM, Ehrenstein V et al (2018) the role of comorbidity in mortality after hip fracture: a nationwide Norwegian study of 38,126 women with hip fracture matched to a general-population comparison cohort. Am J Epidemiol 188(2):398–407. https://doi.org/10.1093/aje/kwy251
Bekeris J, Wilson LA, Bekere D, Liu J, Poeran J, Zubizarreta N et al (2021) Trends in comorbidities and complications among patients undergoing hip fracture repair. Anesth Analg 132(2):475–484. https://doi.org/10.1213/ane.0000000000004519
Moons KG, Royston P, Vergouwe Y, Grobbee DE, Altman DG (2009) Prognosis and prognostic research: what, why, and how? BMJ 338:b375. https://doi.org/10.1136/bmj.b375
Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW et al (2007) Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 356(8):775–789. https://doi.org/10.1056/NEJMoa063070
Restrepo MI, Sibila O, Anzueto A (2018) Pneumonia in patients with chronic obstructive pulmonary disease. Tuberc Respir Dis (Seoul) 81(3):187–197. https://doi.org/10.4046/trd.2018.0030
Andersson NW, Goodwin RD, Okkels N, Gustafsson LN, Taha F, Cole SW et al (2016) Depression and the risk of severe infections: prospective analyses on a nationwide representative sample. Int J Epidemiol 45(1):131–139. https://doi.org/10.1093/ije/dyv333
Blazer DG (2003) Depression in late life: review and commentary. J Gerontol: Series A 58(3):M249–M265. https://doi.org/10.1093/gerona/58.3.M249
Fluharty M, Taylor AE, Grabski M, Munafò MR (2017) The association of cigarette smoking with depression and anxiety: a systematic review. Nicotine Tob Res 19(1):3–13. https://doi.org/10.1093/ntr/ntw140
Kiecolt-Glaser JK, Glaser R (2002) Depression and immune function: central pathways to morbidity and mortality. J Psychosom Res 53(4):873–876. https://doi.org/10.1016/s0022-3999(02)00309-4
Buigues C, Padilla-Sánchez C, Garrido JF, Navarro-Martínez R, Ruiz-Ros V, Cauli O (2015) The relationship between depression and frailty syndrome: a systematic review. Aging Ment Health 19(9):762–772. https://doi.org/10.1080/13607863.2014.967174
Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G (2004) Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci 59(3):255–263. https://doi.org/10.1093/gerona/59.3.m255
Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M (2009) Defining comorbidity: implications for understanding health and health services. Ann Fam Med 7(4):357–363. https://doi.org/10.1370/afm.983
Gilbert T, Neuburger J, Kraindler J, Keeble E, Smith P, Ariti C et al (2018) Development and validation of a hospital frailty risk score focusing on older people in acute care settings using electronic hospital records: an observational study. Lancet 391(10132):1775–1782. https://doi.org/10.1016/s0140-6736(18)30668-8
Sukkriang N, Punsawad C (2020) Comparison of geriatric assessment tools for frailty among community elderly. Heliyon 6(9):e04797. https://doi.org/10.1016/j.heliyon.2020.e04797
Vesterager JD, Madsen M, Hjelholt TJ, Kristensen PK, Pedersen AB (2022) Prediction Ability of Charlson, Elixhauser, and Rx-Risk comorbidity indices for mortality in patients with hip fracture. a Danish population-based cohort study from 2014–2018. Clin Epidemiol 14:275–287. https://doi.org/10.2147/clep.S346745
Holm E, Jacobsen KK, de Lony TB, Lembeck M, Pedersen H, Andersson C et al (2022) Frequency of missed or delayed diagnosis in dementia is associated with neighborhood socioeconomic status. Alzheimers Dement (N Y) 8(1):e12271. https://doi.org/10.1002/trc2.12271
Schrøder CK, Hjelholt TJ, Møller H, Madsen M, Pedersen AB, Kristensen PK (2022) Comorbidity and quality of in-hospital care for hip fracture patients. J Am Med Dir Assoc 23(4):671–7.e4. https://doi.org/10.1016/j.jamda.2022.01.078
Vesterager JD, Kristensen MT, Pedersen AB (2021) Loss of pre-fracture basic mobility status at hospital discharge for hip fracture is associated with 30-day post-discharge risk of infections - a four-year nationwide cohort study of 23,309 Danish patients. Injury 52(7):1833–1840. https://doi.org/10.1016/j.injury.2021.04.037
Morkisch N, Upegui-Arango LD, Cardona MI, van den Heuvel D, Rimmele M, Sieber CC et al (2020) Components of the transitional care model (TCM) to reduce readmission in geriatric patients: a systematic review. BMC Geriatr 20(1):345. https://doi.org/10.1186/s12877-020-01747-w
Pedersen LH, Gregersen M, Barat I, Damsgaard EM (2018) Early geriatric follow-up visits to nursing home residents reduce the number of readmissions: a quasi-randomised controlled trial. Eur Geriatr Med 9(3):329–337. https://doi.org/10.1007/s41999-018-0045-3
Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sørensen HT (2011) The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish national registry of patients. BMC Med Res Methodol 11:83. https://doi.org/10.1186/1471-2288-11-83
Schmidt M, Johannesdottir SA, Lemeshow S, Lash TL, Ulrichsen SP, Bøtker HE et al (2013) Obesity in young men, and individual and combined risks of type 2 diabetes, cardiovascular morbidity and death before 55 years of age: a Danish 33-year follow-up study. BMJ Open 3(4):e002698. https://doi.org/10.1136/bmjopen-2013-002698
Sundbøll J, Adelborg K, Munch T, Frøslev T, Sørensen HT, Bøtker HE et al (2016) Positive predictive value of cardiovascular diagnoses in the Danish national patient registry: a validation study. BMJ Open 6(11):e012832. https://doi.org/10.1136/bmjopen-2016-012832
Holland-Bill L, Xu H, Sørensen HT, Acquavella J, Sværke C, Gammelager H et al (2014) Positive predictive value of primary inpatient discharge diagnoses of infection among cancer patients in the Danish national registry of patients. Ann Epidemiol 24(8):593–7. https://doi.org/10.1016/j.annepidem.2014.05.011
Funding
Open access funding provided by Aarhus Universitet. This study was supported by grants from Helsefonden (grant number 20-B-0140), Helga og Peter Kornings Fond, Frimodt-Heineke Fonden, and Department of Clinical Medicine at Aarhus University, Denmark. The sponsors had no role in the design, data collection, analysis, interpretation, or submission of the study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conceptualization and methodology of the study. NRG performed the literature search and formal analysis and wrote the original draft. All authors contributed to the interpretation, provided comments on multiple iterations of the manuscript, and approved final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
NRG, RN, HTS, and ABP report no personal conflicts of interest. CV received travel expenses with no relevance to the present study from Stryker. Department of Clinical Epidemiology, Aarhus University Hospital, receives funding for other studies from companies in the form of research grants to (and administered by) Aarhus University. None of those studies have any relation to the present study.
Ethical approval
The study was reported to the Danish Data Protection Agency through registration at Aarhus University (record number: AU-2016-051-000001, sequential number 880).
Patient consent
Patient consent is not required by Danish law for registry-based studies.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gadgaard, N.R., Varnum, C., Nelissen, R. et al. Major comorbid diseases as predictors of infection in the first month after hip fracture surgery: a population-based cohort study in 92,239 patients. Eur Geriatr Med (2024). https://doi.org/10.1007/s41999-024-00989-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41999-024-00989-w