
Abstract
The goal of this research was to assess the role of professional isolation on mental health symptoms via stress among employees working remotely due to COVID-19. Additionally, this research explored the interactive effect of management communication on the relationship between professional isolation and stress, and stress and mental health symptoms. In Study 1, behavior analysts who were working remotely as a result of the pandemic completed assessments of professional isolation, stress, and mental health symptoms at two points in time, separated by two weeks. Study 2 replicated and extended the findings from Study 1 in a sample of remote employees recruited from Amazon’s Mechanical Turk using a three-wave design. Findings of both Study 1 and Study 2 suggested that stress mediated the relationship between professional isolation and mental health symptoms. Additionally, management communication buffered the association between stress and mental health symptoms in Study 2. Lastly, the indirect effect of professional isolation on mental health symptoms was stronger for those who received less communication from their management. The findings of these two studies expand our understanding of the mechanism and boundary condition through which professional isolation is related to mental health symptoms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The U.S. Bureau of Labor Statistics reported that 25% of American employees worked from home at least part of the time in 2017–2018 (BLS, 2019). Due to the COVID-19 pandemic this number has increased substantially. As of mid-May, 2020, 68% of American employees reported performing some or all of their work-related tasks from home (Hickman & Saad, 2020). Hence, a large proportion of the population that was not accustomed to working remotely now found themselves working from home (Wang et al., 2021). Therefore, in addition to the stressors presented in the pandemic, individuals may experience increased professional isolation. In fact, recent research identified professional isolation as a transitional challenge during the pandemic (Wang et al., 2021), which may occur due to the reduction in interactions with one’s colleagues (Cooper & Kurland, 2002).
In light of the recent changes in the modality of work from on-site to remote, research on professional isolation is more urgent than ever. Although numerous studies have examined the effects of remote work on both individual and organizational outcomes (e.g., Golden et al., 2006; Vega et al., 2015), the construct of professional isolation has received considerably less research attention. This oversight is concerning because the constructs of telework and professional isolation are not synonymous. Telework refers to “the substitution of communication technology for work‐related travel, and can include paid work from home, a satellite office, a telework centre or any other work station outside of the main office for at least one day per work week” (Martin & MacDonnell, 2012, p. 603). In contrast, professional isolation has been broadly defined as the “perception of a lack of availability of support and recognition, missed opportunities for informal interactions with co-workers, and not being part of the group” (Marshall et al., 2007, p. 160) as a result of working remotely. In fact, findings of a qualitative study showed that only 57% of their telework sample experienced professional isolation, suggesting that not all teleworkers necessarily experience professional isolation (Mann et al., 2000). Considering those who teleworked previously may have chosen to work remotely and had the option to work from the premises of their employer for at least part of the week, they may not have necessarily felt disconnected from their work, or experienced stress as a result of working remotely. Measuring professional isolation directly avoids the assumption of conflation of these constructs.
This study makes two contributions to the literature on professional isolation. First, we use two separate samples of employees who were required to work remotely due to the pandemic and assess the prospective effects of professional isolation on mental health symptoms via stress. Since the policies during the pandemic ceased all face-to-face interactions outside of one’s family (Matias et al., 2020), individuals mandated to work remotely may have felt isolated or disconnected from their coworkers. Therefore, for the purposes of this study, we conceptualize professional isolation as missed opportunities for interactions with ones’ coworkers.
Considering that the option to perform one’s duties from their workplace may be largely unavailable to many, employees are having to learn to work remotely, which may be stressful. Prior to the COVID-19 pandemic, working from home was a luxury that was only afforded to the relatively affluent (Desilver, 2020) and, often pursued based on employee preferences (Kniffin et al., 2021). However, the pandemic has forced most of the workforce to engage in mandatory remote work. Most of the existing research on professional isolation has been conducted with employees who choose to work remotely (e.g., Golden et al., 2008), and may not generalize to employees who are now being required to work remotely as a result of the pandemic.
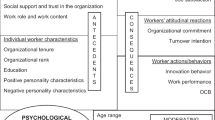
Second, we examine the moderating effect of management communication in mitigating the association between professional isolation and stress, and stress and mental health symptoms. Management communication is defined as the degree to which employees receive adequate information regarding the functioning of the organization (Vander Elst et al., 2010). Through an open communication channel, management can notify employees of relevant policy changes with regards to working remotely, thereby alleviating stress and reducing mental health symptoms. The hypothesized model is presented in Fig. 1.

Hypothesized model for Study 1 and Study 2
Theoretical Framework
We utilize the Conservation of Resources (COR; Hobfoll, 1989) framework to examine professional isolation as a precursor to stress and mental health symptoms among those working remotely during the COVID-19 pandemic, as well as the moderating effect of management communication. Stress is characterized by “a situation wherein job-related factors interact with a worker to change (i.e., disrupt or enhance) his or her psychological and/or physiological condition such that the person (i.e., mind–body) is forced to deviate from normal functioning (Beehr & Newman, 1978, p. 670). The COR theory postulates that individuals strive to acquire resources they value. Stress ensues due to 1) loss of resources, 2) threat to current resources, and 3) inadequate return on investment made to increase resources. Over time, one’s inability to cope with stress can result in mental health symptoms, such as feelings of anxiety, sadness, and hopelessness, among others (Hart & Cooper, 2001; Kahn & Byosiere, 1992).
The COR is well situated to provide insights regarding the role of professional isolation on stress and mental health symptoms. During the current global pandemic, several organizations have asked their employees to work from home (Chang et al., 2021), which may limit their interactions with their coworkers. As a result of fewer face-to-face interactions, remote employees are likely to feel detached from their organization (Bartel et al., 2012) and experience loneliness (Wang et al., 2021). Therefore, we argue that lack of interactions with ones’ coworkers (i.e., professional isolation) may be viewed as a threat to and/or loss of social resources.
Consistent with COR, the appraisal of professional isolation (i.e., threat to and/or loss of interactions with ones’ coworkers) can lead to employee stress. Consequently, the experience of stress is likely to result in strain if employees are unable to make up for those lost resources, thereby heightening their mental health symptoms. Prior research has shown that professional isolation is positively related to stress (Dussault et al., 1999), and stress is related to mental health symptoms (Sawhney et al., 2018). Taking into account this theoretical and empirical evidence, we pose the following hypothesis:
-
Hypothesis 1: Professional isolation will exhibit an indirect positive effect on mental health symptoms through employee stress.
Moderating Role of Management Communication
Organizations switched their operations to a virtual modality due to the COVID-19 pandemic (Sanders et al., 2020), which may have resulted in ambiguity regarding role expectations. During crisis situations, employees often turn to their management for information, and it becomes the responsibility of the organization to effectively communicate crucial information with its employees on a timely basis so that they are able to carry out their tasks (Allen, 1992; van der Meer et al., 2017). We note that while management communication may provide information about the organization’s strategy for managing work arrangements during the pandemic, it may not fully fill the void created by the lack of interactions with ones’ coworkers. Research conducted during the pandemic has demonstrated that ineffective communication from their management is a challenge experienced by remote workers (Wang et al., 2021).
Consistent with COR theory, we argue that management communication can serve as an energy resource that alleviates the effects of professional isolation on stress, and stress on mental health symptoms (Hobfoll et al., 2018). For the purposes of the current study, we define management communication as relaying timely, adequate and accurate information about working remotely (Kernan & Hanges, 2002). Management communication may facilitate a better understanding of changes in working arrangements during the pandemic. For instance, through communication, management can inform employees regarding the duration of time they will spend working remotely, as well as articulate any changes in policies and procedures, subsequently enhancing predictability of their working situation and alleviating stress. Such information may elevate employees’ perception of control by reducing ambiguity (DiFonzo & Bordia, 1998) and giving them relevant knowledge regarding when they may be able to return to work, thereby equipping them to better cope with professional isolation (Stephens & Long, 2000). Accordingly, we hypothesize the following:
-
Hypothesis 2: Management communication will moderate the positive relationship between professional isolation and stress, such that the association between professional isolation and stress will be weaker when participants experience higher versus lower management communication.
At the same time, we expect that the risk of employees’ stress during the pandemic escalating into mental health symptoms may be lower for those who receive adequate communication from their management. The COR theory’s gain paradox principle posits that the salience of resource gain increases in the face of resource loss. Stated differently, when threatened with resource loss, securing additional resources becomes critical (Hobfoll et al., 2018). In the context of the current study, when faced with stress, management communication may serve as a resource to counter the negative effects of stress on employees’ mental health. As an example, employees who receive information from their management pertaining to remote work arrangements may perceive greater control and be able to bounce back from the stress they were experiencing, thus inhibiting their mental health symptoms. Conversely, the loss spirals of those who do not receive information from their management while experiencing stress may gain both momentum and magnitude (Hobfoll et al., 2018). Consequently, we pose the following hypothesis:
-
Hypothesis 3: Management communication will moderate the positive relationship between stress and mental health symptoms, such that the association between stress and mental health symptoms will be weaker when participants experience higher versus lower management communication.
Taken together, this research presents a moderated mediation model, whereby management communication serves as a resource of the indirect association between professional isolation and mental health symptoms through stress. Employees experiencing professional isolation while working remotely may experience less stress if they receive management communication. Such communication may provide the much-needed information to employees regarding changes in work policies during the pandemic, thus enhancing their perception of control (DiFonzo & Bordia, 1998), thereby reducing the deleterious effects of stress on mental health symptoms. On the other hand, perception of professional isolation may initiate a resource loss spiral for those who do not receive communication from their management, resulting in stress and mental health symptoms (Hobfoll et al., 2018). Given the above, we propose the following hypothesis:
-
Hypothesis 4: The indirect relationship between professional isolation and mental health symptoms through stress is moderated by management communication, such that this indirect relationship is stronger at lower levels of management communication.
Overview of Study 1 and Study 2
The goal of Study 1 was to explore whether professional isolation predicted both stress and mental health symptoms in behavior analysts who were required to work remotely during the COVID-19 pandemic. Behavior analysts are professionals who provide behavioral intervention services, based on the science of behavior and learning, to address problems of social significance with the purpose of improving the quality of life of the individuals they serve (Fisher et al., 2021). The majority of their work typically is conducted face-to-face in highly interactive sessions, during which behavior analysts interact with their clients, colleagues, paraprofessionals, and other stakeholders. Over 80% of board certified registered behavioral technicians (RBT®), assistant behavior analysts (BCaBA®), and behavior analysts (BCBA®) provide clinical services to children, individuals with disabilities, and/or other vulnerable populations (Behavior Analysis Certification Board, 2021).
Given the nature of the work performed by behavior analysts, they experience high rates of job burnout and work-related stress (Plantiveau et al., 2018). During the COVID-19 pandemic, behavior analysts also experienced additional sources of stress resulting from distractions, challenges posed by having to identify ways to deliver behavioral services safely, having to quickly pivot to delivering services remotely, and a work environment with greatly diminished social interaction (e.g., Behavioral Health Center of Excellence, 2020; Jimenez-Gomez et al., 2021). This drastic and sudden change may result in increased stress and expression of mental health symptoms. Hence, we considered this sample appropriate for the current study.
Study 2 attempted to replicate and extend the findings from Study 1 in a more diverse working sample to delineate whether the effects of professional isolation on stress and mental health exist in employees across industries that are required to work remotely as a result of the pandemic. In particular, this study explored whether management communication serves as a resource that mitigates the effects of professional isolation on stress, and stress on mental health symptoms.
Both Study 1 and Study 2 utilized a prospective design with assessments separated by two weeks. The rationale for testing these variables at different time points was twofold. First, in order to reduce attrition, we wanted to keep the length of the survey to a minimum. Second, we did not expect the measures of professional isolation, management communication, stress, or mental health symptoms to fluctuate much over the timeframe of the study. In light of these considerations, we opted to examine the relationships between our study variables using a prospective design rather than a longitudinal design.
Study 1 Method
Participants and Procedure
The data presented in this study are from a larger study on stress and well-being of behavior analysts. None of the variables presented in this study have been published in other studies. The sample for this study comprised of 130 behavior analysts residing within the United States. On average, participants were 33.98 years of age (SD = 8.59), predominantly female (85.70%), and White (87.70%). In this sample, 75.40% participants indicated that their primary place of work was center- or clinic-based, in-school, community-based, or other prior to the pandemic.
An invitation to participate in the study was sent to all members of the Behavior Analyst Certification Board in April, 2020. Prior to completing the survey, members were asked to indicate whether their employers were requiring them to work remotely, as well as the number of hours they were working at the time of the survey. Those who were employed 20 h or more per week and working remotely were retained for this study. A total of 266 members completed the survey in its entirety at Time 1. These participants were invited to complete another survey at Time 2, two weeks later. Of these, 130 participants provided complete responses. Participants who completed both surveys were entered in a raffle to win one of 25 Amazon gift cards worth $25.00.
Measures
Professional Isolation
Five items adopted from Hawthorne (2006) were used to measure professional isolation at Time 1. Participants were instructed to indicate the extent to which they felt isolated from their coworkers during the COVID-19 pandemic. Items developed for professional isolation are presented in the Appendix. All items were measured on a 5-point Likert scale, from 1 = “Not at all” to 5 = “Extremely.” Cronbach’s alpha reliability for this scale was 0.80.
Stress
We used Cohen et al.’s (1983) 10-item measure to assess stress at Time 2. Participants indicated the frequency with which they experienced stress since the COVID-19 pandemic. A sample item included “Felt that you were unable to control the important things in your life.” This scale utilized a 5-point Likert scale, from 1 = “Never” to 5 = “Very frequently.” Cronbach’s alpha reliability for this scale was 0.90.
Mental Health Symptoms
Eleven items from the American College Health Assessment II (ACHA, 2016) were used to assess mental health symptoms at Time 2. Participants indicated the frequency with which they experienced mental health symptoms since the COVID-19 pandemic. A sample item in this measure was “Felt overwhelming anxiety.” All items were measured on a 5-point Likert scale, ranging from 1 = “Never” to 5 = “Very frequently.” Cronbach’s alpha reliability for this scale in the current study was 0.76.
Study 1 Results
In order to ascertain that the study variables could be distinguished from one another, we conducted confirmatory factor analysis (CFA) with robust maximum likelihood estimation (MLR) using Mplus 7.4. In line with the recommendations by Little et al. (2002), we created five parcels for stress by averaging two items per parcel. Considering the odd number of items for mental health symptoms, we created three parcels by averaging three items per parcel, and two items for the fourth parcel. We tested a three-factor model where items for professional isolation, and parcels for stress and mental health symptoms were allowed to load on their respective factors. Results suggested inadequate fit for this model, χ2 (74) = 286.23, p < 0.01, CFI = 0.77, RMSEA = 0.11, 90% C.I. of RMSEA [0.10, 0.12]. Because the initial three-factor model failed to adequately fit the data, we used the Lagrange Multiplier test (Byrne, 2006) to determine the cause of misfit. Consistent with recommendations in the literature (MacCallum et al., 1992), we allowed one error covariance between two items in the professional isolation measure to be freely estimated to enhance model fit. This respecified model demonstrated significantly better fit, χ2 (73) = 117.36, p < 0.01, CFI = 0.95, RMSEA = 0.05, 90% C.I. of RMSEA [0.03, 0.07].
Means, standard deviations, and correlations for all study variables are provided in Table 1. Correlation coefficients indicated that professional isolation was positively related to stress (r = 0.29, p < 0.01), but not mental health symptoms. Stress exhibited a positive association with mental health symptoms (r = 0.49, p < 0.01).
Hypothesis 1 was tested using the PROCESS macro (Hayes, 2017), which allows simultaneous examination of mediation and moderation effects. Hypothesis 1 predicted that stress would mediate the relationship between professional isolation and mental health symptoms. For the purposes of testing this hypothesis, we used model 4 in the PROCESS macro, and employed a bias-corrected bootstrapping procedure with 10,000 samples to test the mediation effect. As shown in Table 2, professional isolation at Time 1 was positively related to stress at Time 2 (B = 0.23, SE = 0.07, p < 0.01). Meanwhile, stress at Time 2 predicted mental health symptoms at Time 2 (B = 0.41, SE = 0.07, p < 0.01). The indirect effect of professional isolation on Time 2 mental health symptoms was significant (effect = 0.09, SE = 0.03, 95% CI [0.03, 0.16]. These findings provide support for Hypothesis 1.
Study 2 Method
Participants and Procedure
Data for Study 2 were gathered between March, 2020 through May, 2020 from 269 Amazon’s Mechanical Turk (MTurk) workers who resided in the United States. The mean age of participants was 39.34 (SD = 10.86) years, and they worked 41.43 (SD = 4.34) hours per week. Approximately 56% of participants were male. The majority of the participants were married (50%) or single (39%). With respect to ethnicity, 80% of the participants were White, followed by Asian (12%), and Black (5%). Participants were employed in various industries, including educational services, information technology, finance, and healthcare, among others, and 57.2% of our participants indicated that they had worked remotely for 15 h or fewer prior to the pandemic.
Consistent with recommendations in the literature (Buhrmester et al., 2018), a qualification survey was posted on MTurk where participants indicated whether they were employed, the number of hours they were employed, and whether they were required to work remotely due to COVID-19. A total of 2,448 participants completed the qualification survey. Participants were retained if they 1) were employed, 2) worked 30 h or more per week, and 3) were required to work remotely due to COVID-19. Based on the responses to the qualification survey, 745 participants were eligible to participate in the study and were invited to complete the Time 1 survey. Of these, 369 participants that were working remotely completed the survey. Two weeks later, at Time 2, participants from Time 1 were invited to complete another survey, of which 324 remote employees responded. At Time 3, all remote participants from Time 2 were invited to complete a survey two weeks post the Time 2 survey. A total of 269 participants working remotely responded to the Time 3 survey. In order to ensure that only employees that were working remotely were retained, participants were asked to indicate whether they were working remotely at all three time points. Two attention check items were embedded in each of the three surveys. A sample attention check item was “Please select strongly disagree for this item.” Responses were only retained if participants passed all attention checks across the three surveys.
Measures
We assessed professional isolation and management communication at Time 1, stress at Time 2, and mental health symptoms at Time 3. We used the same measures of professional isolation and stress as in Study 1. In Study 2, the Cronbach’s alpha reliability was 0.80 for professional isolation and 0.91 for stress. Below, we provide details for measures of management communication and mental health symptoms that were administered in Study 2.
Management Communication
Four items were developed for this study to measure management communication (see Appendix for items). In line with the conceptualization of communication in the workplace (Kernan & Hanges, 2002), items on this scale assessed timeliness, accuracy, and adequacy of the communication received. Additionally, we added a fourth item that captured employees’ overall perceptions about being kept in the loop regarding remote working arrangements. All items were measured on a 5-point Likert scale, from 1 = “Never” to 5 = “Very frequently.” Cronbach’s alpha reliability for this scale was 0.90.
Mental Health Symptoms
We used the 23-item DSM-5 Self-Rated Level 1 Cross-Cutting Symptom Measure (American Psychiatric Association, 2015) to assess mental health symptoms. All items were measured on a 5-point Likert scale, from 1 = “Not at all” to 5 = “Nearly every day.” A sample item for this scale was “Feeling nervous, anxious, frightened, worried, or on edge.” Cronbach’s alpha reliability for this scale in this study was 93.
Control Variable
In Study 2, we controlled for household income before taxes. Response categories were: 1 = “Less than $15,000,” 2 = “$15,000—$24,999,” 3 = “$25,000—$34,999,” 4 = “$35,000—$49,999,” 5 = “$50,000—$74,999,” 6 = “$75,000—$99,999,” 7 = “$100,000—$149,999,” 8 = “$150,000—$199,999,” and 9 = “$200,000 and above.” Prior research has indicated that socioeconomic factors are correlated with employee well-being (Probst et al., 2018).
Study 2 Results
We used the same procedures outlined in Study 1 to conduct a CFA in Study 2. We tested a four-factor model where items for professional isolation and management communication, and parcels for stress (i.e., same five parcels that were used in Study 1) and mental health symptoms (i.e., five parcels created by averaging four items, and sixth parcel created by averaging three items) were allowed to load on their respective factors. The initial model demonstrated inadequate fit, χ2 (168) = 737.84, p < 0.01, CFI = 0.84, RMSEA = 0.09, 90% C.I. of RMSEA [0.09, 0.10]. Similar to Study 1, the Lagrange Multiplier test suggested the inclusion of an error covariance between two items in the professional isolation measure to enhance model fit. Upon including the error covariance, the model demonstrated significantly better fit, χ2 (167) = 471.65, p < 0.01, CFI = 0.91, RMSEA = 0.07, 90% C.I. of RMSEA [0.06, 0.08].
Although the assessment of the predictors (professional isolation and management communication), mediator (stress), and criterion (mental health symptoms) was temporally separated to alleviate concerns of common method variance (CMV; Podsakoff et al., 2003), we proceeded to empirically examine the degree to which CMV was present in our data. Therefore, the measurement model tested previously was re-estimated after including an uncorrelated method factor. Results suggested that not only did the measurement model with the method factor provided adequate fit, but the fit improved significantly compared to the measurement model without the method factor, Δχ2 = 49.82, p < 0.01, Δdf = 19). However, the method factor only accounted for 12.30% of the total variance, which is substantially lower than the 25% reported in the literature (Williams et al., 1989). Therefore, it is safe to conclude that while CMV was present in the data, it is unlikely to bias the results of the current study.
Means, standard deviations, reliabilities, and correlations for all Study 2 variables are presented in Table 3. Bivariate correlations indicated that professional isolation was positively (r = 0.35, p < 0.01) and management communication was negatively (r = -0.24, p < 0.01) related to stress at Time 2. Stress at Time 2 was also positively associated with mental health symptoms at Time 3 (r = 0.62, p < 0.01).
Similar to Study 1, we tested Hypothesis 1 in Study 2 using Model 4 in the PROCESS macro. As indicated in Table 4, controlling for income, professional isolation at Time 1 predicted stress at Time 2 (B = 0.32, SE = 0.05, p < 0.01), and stress predicted mental health symptoms at Time 3 (B = 0.42, SE = 0.04, p < 0.01). No relationship was found between professional isolation and mental health symptoms. Hypothesis 1 was supported in Study 2 as the indirect effect of professional isolation on mental health symptoms via stress was significant (effect = 0.14, SE = 0.03, 95% CI [0.08, 0.19]).
Hypothesis 2 predicted that management communication would buffer the positive relationship between professional isolation and stress, and Hypothesis 3 asserted that the interactive effect between management communication and stress would predict mental health symptoms. In order to test the mediated effects, and stage 1 and stage 2 moderated effects, we used model 58 in the PROCESS macro (see Table 5). While the interaction between management communication and stress predicted mental health symptoms (effect = -0.10, SE = 0.04, p < 0.05), management communication did not moderate the professional isolation – stress relationship. Therefore, Hypothesis 2 was not supported.
Considering that we did not find support for stage 1 moderation, we tested Hypotheses 3 and 4 using model 14 in the PROCESS macro that focused only on the second stage moderation (see Table 6). Our findings indicated that controlling for income, management communication interacted with stress to predict mental health symptoms (B = -0.10, SE = 0.04, p < 0.05). To delineate the form of interaction, we plotted the regression lines for high and low levels of management communication (i.e., 1 SD above and below the mean), consistent with recommendations by Aiken et al. (1991). The two-way interaction plotted in Fig. 2 revealed that the positive relationship between stress and mental health symptoms was significant at both high (t = 7.45, p < 0.01) and low (t = 9.66, p < 0.01) levels of management communication. However, the slope was steeper under low levels of management communication. Hence, Hypothesis 3 was supported.

Interaction between management communication at Time 1 and stress at Time 2 in predicting mental health symptoms at Time 3 in Study 2
Lastly, Hypothesis 4 predicted that the indirect relationship between professional isolation and mental health symptoms would be stronger for those who received less communication from their management. Results indicated that the conditional indirect effect of professional isolation on mental health symptoms was significant under both high (effect = 0.11, SE = 0.03, 95% CI = 0.06 to 0.16) and low (effect = 0.16, SE = 0.03, 95% CI = 0.10 to 0.23) levels of management communication. However, the effect was stronger for those who received less communication. An examination of the index of moderated mediation which provides an interval estimate that “is a direct quantification of the linear association between the indirect effect and the putative moderator of that effect” (Hayes, 2015, p. 3), indicated that the two conditional effects characterized by different values of management communication were statistically different, thereby partially supporting Hypothesis 4.
Discussion
With the emergence of COVID-19, working remotely may become a new reality for many. Considering that prior research suggests that at least 57% the employees who work remotely experience professional isolation (Mann et al., 2000), studies on the effects of professional isolation on employee outcomes are more urgent than ever. Although studies have demonstrated the effects of professional isolation on work-related outcomes (Bartel et al., 2012; Bentein et al., 2017; Golden et al., 2008; Mulki & Jaramillo, 2011), research on the effects of professional isolation on employee health are deficient (Bentein et al., 2017). Thus, an examination of the effects of professional isolation on stress and mental health symptoms is pertinent for those working remotely.
Our findings across two samples indicate that professional isolation, which can be viewed as a threat to and/or loss of social resources, is positively associated with stress, and further predicts mental health symptoms. These results are consistent with the assertions made by the Conservation of Resources (COR; Hobfoll, 1989) framework which posits that professional isolation may threaten interpersonal resources at work, which could result in stress. Although we did not draw from uncertainty management theory (Lind & Van den Bos, 2002) in the current study, our findings lend support to this theory in the context of professional isolation. The core premise of this theory is that individuals seek predictability in their environment, and lack thereof can lead to stress. Mandating remote work during the COVID-19 pandemic may have produced feelings of relational uncertainty with respect to their standing with one’s coworkers and superiors, resulting in stress and poor mental health.
Inconsistent with our hypotheses, management communication did not moderate the association between professional isolation and stress. We provide two main reasons for this lack of significance. One explanation for this finding is that other resources, such as support from one’s leader and peers may be more meaningful to those working remotely when compared to management communication relating to remote working policies. For instance, a recent study indicated that coworker support was especially important for those working remotely to be productive during the COVID-19 pandemic (Keller et al., 2020). It is also plausible that other forms of communication, such as job-related communication, may be more pertinent in reducing stress. Future research may consider exploring the interactive effects of professional isolation with various forms of support and communication in predicting stress of remote employees.
Our findings also suggested that the relationship between stress and mental health symptoms can be contained with adequate management communication. In line with COR, high quality management communication may serve as an energy resource which provides knowledge regarding working arrangements, as well as when employees will likely return to work. By doing so, effective communication may remove any ambiguity surrounding work arrangements while giving employees hope to return to work. In the present research, mental health symptoms increased for those who received less versus greater management communication. Not only do these findings bolster the support for effective management communication as a resource during COVID-19, it paves a path for future intervention research to alleviate negative consequences of stress by increasing timely communication and information flow in their organization. Overall, the results of our study align with the theoretical propositions of the COR, thus bolstering its importance in the occupational stress literature.
Practical Implications
Our research also has practical implications that need to be highlighted. The findings of our study indicate that professional isolation is prevalent among employees who are required to work remotely during the pandemic, and is indirectly related to their mental health. Considering that much of the professional isolation is associated with employee development activities, such as interpersonal networking, informal learning, and mentoring (Cooper & Kurland, 2002), organizations can ensure that these opportunities are adequately available to employees who are being required to work remotely.
The current study also substantiates the importance of management communication during a time of uncertainty. Our results indicated that the indirect effect of professional isolation on mental health symptoms was stronger for those who experienced lower management communication. These findings suggest that while organizations may not be able to fully eliminate professional isolation, they can play a pivotal role in reducing ambiguity, and consequently enhancing the mental health of remote workers by effectively communicating with its employees in a timely manner.
Limitations and Directions for Future Research
The findings of our study should be considered in light of its limitations. First, although we utilized a prospective design in both Study 1 and Study 2, we cannot infer causality due to the correlational nature of both studies. While the pattern of results in both studies were in line with most of our hypotheses, we cannot conclude with certainty that professional isolation results in stress or vice versa. Similarly, we cannot rule out any potential confounds or alternative explanations in our findings. Researchers may consider testing our model using longitudinal design to establish causality (Zapf et al., 1996).
Our second limitation concerns the measurement of professional isolation. Although we asked participants to report the extent to which they experienced professional isolation during the pandemic, we did not capture the experience of professional isolation due to the pandemic. Furthermore, we did not capture the sources of professional isolation across the two samples. While some participants may experience professional isolation as a result of the lack of interactions with their coworkers, others may experience it because they are being ostracized. Considering that the outcomes of professional isolation may vary depending on the source of isolation, future research may consider the source as a moderator of the professional isolation – employee health relationship.
Third, the conceptualization of management communication in the current study may be simplistic. Existing research has used alternative conceptualizations of communication (i.e., job-related vs. non job-related, positive vs. negative, etc.; Beehr et al., 1990) that may be relevant, but were not considered in the present research. As an example, Stephens and Long (2000) demonstrated that positive communication about work reduced the intensity of the relationship between experiencing traumatic stressors and strain. Furthermore, research suggests that frequency of communication may be equally important to consider when studying organizational communication (Bakker & Xanthopoulou, 2009). Therefore, we urge researchers to not only examine different types of communication, but also the frequency of communication as a way of mitigating stress.
Fourth, we relied on a sample recruited from Amazon’s Mechanical Turk, which may be considered a limitation. However, researchers have argued that MTurk offers access to an ethnically and socioeconomically diverse sample (Casler et al., 2013) which is representative of the labor market (Michel et al., 2018). We believe that our use of the MTurk platform to recruit participants was justified since the goal of Study 2 was to replicate and extend our findings from Study 1 with a diverse working sample.
Fifth, while this research utilized a validated measure of stress that has been frequently cited in the literature (Kotsou et al., 2011), we realize that this scale is contaminated as it captures perceived control, as well as one’s response to stress (Cavaiola & Stout, 2017). Future research may consider using a clean measure of stress that assesses one’s affective response to professional isolation to determine whether the findings from the current study can be replicated.
Conclusion
Using two independent samples, this study explored the indirect effect of professional isolation on mental health symptoms through stress in employees who were required to work remotely due to the COVID-19 pandemic. Additionally, this research assessed the moderating role of management communication on the indirect effect of professional isolation on mental health symptoms. Results suggested that stress mediated the positive relationship between professional isolation and mental health symptoms. Additionally, management communication buffered the positive association between stress and mental health symptoms and the indirect effect of professional isolation on mental health symptoms. These findings expand our understanding of the effects of professional isolation and management communication on employee well-being during a pandemic.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
References
Aiken, L. S., West, S. G., & Reno, R. R. (1991). Multiple regression: Testing and interpreting interactions. Sage.
Allen, M. W. (1992). Communication and organizational commitment: Perceived organizational support as a mediating factor. Communication Quarterly, 40(4), 357–367. https://doi.org/10.1080/01463379209369852
American College Health Association (ACHA). (2016). National College Health Assessment II: Canadian Reference Group Report Fall 2016. Linthicum: Author.
American Psychiatric Association. (2015). Diagnostic and Statistical Manual-5 Self-Rated Level 1 Cross Cutting Symptom Measure-Adult. Retrieved from https://www.psychiatry.org/psychiatrists/practice/dsm/dsm-5/online-assessment-measures
Ashforth, B. E., & Mael, F. (1989). Social identity theory and the organization. Academy of Management Review, 14(1), 20–39.
Bakker, A. B., & Xanthopoulou, D. (2009). The crossover of daily work engagement: Test of an actor–partner interdependence model. Journal of Applied Psychology, 94(6), 1562.
Bartel, C. A., Wrzesniewski, A., & Wiesenfeld, B. M. (2012). Knowing where you stand: Physical isolation, perceived respect, and organizational identification among virtual employees. Organization Science, 23(3), 743–757. https://doi.org/10.1287/orsc.1110.0661
Beehr, T. A., & Newman, J. E. (1978). Job stress, employee health, and organizational effectiveness: A facet analysis, model, and literature review 1. Personnel Psychology, 31(4), 665–699.
Beehr, T. A., King, L. A., & King, D. W. (1990). Social support and occupational stress: Talking to supervisors. Journal of Vocational Behavior, 36(1), 61–81.
Behavioral Health Center for Excellence. (2020). COVID-19 FAQs for ABA Organizations. https://bhcoe.org/resources/covid-19-faqs-for-aba-providers/
Behavior Analyst Certification Board. (2021). BACB certificant data. https://www.bacb.com/bacb-certificant-data/
Bentein, K., Garcia, A., Guerrero, S., & Herrbach, O. (2017). How does social isolation in a context of dirty work increase emotional exhaustion and inhibit work engagement? A process model. Personnel Review, 46, 1620–1634. https://doi.org/10.1108/PR-09-2016-0227
Bentley, T. A., Teo, S. T., McLeod, L., Tan, F., Bosua, R., & Gloet, M. (2016). The role of organisational support in teleworker wellbeing: A socio-technical systems approach. Applied Ergonomics, 52, 207–215. https://doi.org/10.1016/j.apergo.2015.07.019
Brown, L. A., & Roloff, M. E. (2015). Organizational citizenship behavior, organizational communication, and burnout: The buffering role of perceived organizational support and psychological contracts. Communication Quarterly, 63(4), 384–404. https://doi.org/10.1080/01463373.2015.1058287
Buhrmester, M. D., Talaifar, S., & Gosling, S. D. (2018). An evaluation of Amazon’s Mechanical Turk, its rapid rise, and its effective use. Perspectives on Psychological Science, 13, 149–154. https://doi.org/10.1177/1745691617706516
Byrne, B. M. (2006). Structural equation modeling with EQS: Basic concepts, applications, and programming (2nd ed.). Erlbaum.
Casler, K., Bickel, L., & Hackett, E. (2013). Separate but equal? A comparison of participants and data gathered via Amazon’s MTurk, social media, and face-to-face behavioral testing. Computers in Human Behavior, 29, 2156–2160. https://doi.org/10.1016/j.chb.2013.05.009
Cavaiola, A. A., & Stout, D. (2017). Other facets of workplace abuse: An exploratory study. The Psychologist-Manager Journal, 20(4), 246–266.
Chang, Y., Chien, C., & Shen, L. F. (2021). Telecommuting during the coronavirus pandemic: Future time orientation as a mediator between proactive coping and perceived work productivity in two cultural samples. Personality and Individual Differences, 171, 1–6. https://doi.org/10.1016/j.paid.2020.110508
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396.
Cooper, C. D., & Kurland, N. B. (2002). Telecommuting, professional isolation, and employee development in public and private organizations. Journal of Organizational Behavior, 23(4), 511–532.
Desilver, D. (2020). Working from home was a luxury for the relatively affluent be- fore coronavirus—Not any more. World Economic Forum. Retrieved from https://www.weforum.org/agenda/2020/03/working-from-home-coronavirus-workers-future-of-work/
DiFonzo, N., & Bordia, P. (1998). A tale of two corporations: Managing uncertainty during organizational change. Human Resource Management, 37(3–4), 295–303. https://doi.org/10.1002/(SICI)1099-050X(199823/24)37:3/4%3c295::AID-HRM10%3e3.0.CO;2-3
Dussault, M., Deaudelin, C., Royer, N., & Loiselle, J. (1999). Professional isolation and occupational stress in teachers. Psychological Reports, 84, 943–946. https://doi.org/10.2466/PR0.84.3.943-946
Fisher, W. W., Groff, R. A., & Roane, H. A. (2021). In W. W. Fisher, C. C., Piazza, & H. S. Roane (Eds.). Handbook of Applied Behavior Analysis. The Guilford Press.
Golden, T. D., Veiga, J. F., & Simsek, Z. (2006). Telecommuting’s differential impact on work-family conflict: Is there no place like home? Journal of Applied Psychology, 91, 1340–1350. https://doi.org/10.1037/0021-9010.91.6.1340
Golden, T. D., Veiga, J. F., & Dino, R. N. (2008). The impact of professional isolation on teleworker job performance and turnover intentions: Does time spent teleworking, interacting face-to-face, or having access to communication-enhancing technology matter? Journal of Applied Psychology, 93(6), 1412–1421. https://doi.org/10.1037/a0012722
Hart, P. M., & Cooper, C. L. (2001). Occupational stress: Toward a more integrated framework. In N. Anderson, D. S. Ones, H. K. Sinangil, & C. Viswesvaran (Eds.), Handbook of industrial, work, and organizational psychology (Vol. 2, pp. 93–114). Sage.
Harvey, P., & Harris, K. J. (2010). Frustration-based outcomes of entitlement and the influence of supervisor communication. Human Relations, 63(11), 1639–1660.
Hawthorne, G. (2006). Measuring social isolation in older adults: Development and initial validation of the friendship scale. Social Indicators Research, 77, 521–548. https://doi.org/10.1007/s11205-005-7746-y
Hayes, A. F. (2015). An index and test of linear moderated mediation. Multivariate Behavioral Research, 50(1), 1–22.
Hayes, A. F. (2017). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (2nd ed.). Guilford Publications.
Hickman, A., & Saad, L. (2020). Reviewing remote work in the U.S. under COVID-19. Gallup. https://news.gallup.com/poll/311375/reviewing-remote-work-covid.aspx
Hobfoll, S. E. (1989). Conservation of resources. A new attempt at conceptualizing stress. American Psychologist, 44, 513–524. https://doi.org/10.1037/0003-066X.44.3.513
Hobfoll, S. E., Halbesleben, J., Neveu, J. P., & Westman, M. (2018). Conservation of resources in the organizational context: The reality of resources and their consequences. Annual Review of Organizational Psychology and Organizational Behavior, 5, 103–128. https://doi.org/10.1146/annurev-orgpsych-032117-104640
Jimenez-Gomez, C., Sawhney, G., & Albert, K. M. (2021). Impact of COVID-19 on the applied behavior analysis workforce: Comparison across remote and nonremote workers. Behavior Analysis in Practice. https://doi.org/10.1007/s40617-021-00625-0
Kahn, R. L., & Byosiere, P. (1992). Stress in organizations. In M. D. Dunnette & L. M. Hough (Eds.), Handbook of industrial and organiza- tional psychology (Vol. 3, pp. 571–650). Consulting Psychologists Press.
Keller, A., Knight, C., & Parker, S. (2020). Boosting job performance when working from home: Four key strategies. Society for Industrial and Organizational Psychology. https://www.siop.org/Research-Publications/Items-of-Interest/ArtMID/19366/ArticleID/4623/Boosting-Job-Performance-When-Working-from-Home-Four-Key-Strategies
Kernan, M. C., & Hanges, P. J. (2002). Survivor reactions to reorganization: Antecedents and consequences of procedural, interpersonal, and informational justice. Journal of Applied Psychology, 87(5), 916–928.
Kniffin, K. M., Narayanan, J., Anseel, F., Antonakis, J., Ashford, S. P., Bakker, A. B., ... & Vugt, M. V. (2021). COVID-19 and the workplace: Implications, issues, and insights for future research and action. American Psychologist, 76(1), 63.
Kotsou, I., Nelis, D., Grégoire, J., & Mikolajczak, M. (2011). Emotional plasticity: Conditions and effects of improving emotional competence in adulthood. Journal of Applied Psychology, 96(4), 827.
Lind, E. A., & Van den Bos, K. (2002). When fairness works: Toward a general theory of uncertainty management. Research in Organizational Behavior, 24, 181–223.
Little, T. D., Cunningham, W. A., Shahar, G., & Widaman, K. F. (2002). To parcel or not to parcel: Exploring the question, weighing the merits. Structural Equation Modeling, 9(2), 151–173.
Mann, S., Varey, R., & Button, W. (2000). An exploration of the emotional impact of tele‐working via computer‐mediated communication. Journal of Managerial Psychology, 668–690.https://doi.org/10.1108/02683940010378054
Marshall, G. W., Michaels, C. E., & Mulki, J. P. (2007). Workplace isolation: Exploring the construct and its measurement. Psychology & Marketing, 24, 195–223. https://doi.org/10.1002/mar.20158
Matias, T., Dominski, F. H., & Marks, D. F. (2020). Human needs in COVID-19 isolation. Journal of Health Psychology, 25(7), 871–882.
Martin, B. H., & MacDonnell, R. (2012). Is telework effective for organizations? A meta‐analysis of empirical research on perceptions of telework and organizational outcomes. Management Research Review.
MacCallum, R. C., Roznowski, M., & Necowitz, L. B. (1992). Model modifications in covariance structure analysis: the problem of capitalization on chance. Psychological Bulletin, 111(3), 490.
McCloskey, D. W., & Igbaria, M. (2003). Does" out of sight" mean" out of mind"? An empirical investigation of the career advancement prospects of telecommuters. Information Resources Management Journal, 16, 19–34. https://doi.org/10.4018/irmj.2003040102
Michel, J. S., O’Neill, S. K., Hartman, P., & Lorys, A. (2018). Amazon’s Mechanical Turk as a viable source for organizational and occupational health research. Occupational Health Science, 2, 83–98.
Mulki, J. P., & Jaramillo, F. (2011). Workplace isolation: Salespeople and supervisors in USA. The International Journal of Human Resource Management, 22, 902–923. https://doi.org/10.1080/09585192.2011.555133
Orhan, M. A., Rijsman, J. B., & Van Dijk, G. M. (2016). Invisible, therefore isolated: Comparative effects of team virtuality with task virtuality on workplace isolation and work outcomes. Revista De Psicología Del Trabajo y De Las Organizaciones, 32(2), 109–122. https://doi.org/10.1016/j.rpto.2016.02.002
Parker, S. K., & Sprigg, C. A. (1999). Minimizing strain and maximizing learning: The role of job demands, job control, and proactive personality. Journal of Applied Psychology, 84(6), 925–939.
Plantiveau, C., Dounavi, K., & Virués-Ortega, J. (2018). High levels of burnout among early-career board-certified behavior analysts with low collegial support in the work environment. European Journal of Behavior Analysis, 19, 195–207. https://doi.org/10.1080/15021149.2018.1438339
Podsakoff, P. M., MacKenzie, S. B., Lee, J. Y., & Podsakoff, N. P. (2003). Common method biases in behavioral research: a critical review of the literature and recommended remedies. Journal of Applied Psychology, 88(5), 879.
Probst, T. M., Sinclair, R. R., Sears, L. E., Gailey, N. J., Black, K. J., & Cheung, J. H. (2018). Economic stress and well-being: Does population health context matter? Journal of Applied Psychology, 103(9), 959.
Sanders, K., Nguyen, P. T., Bouckenooghe, D., Rafferty, A., & Schwarz, G. (2020). Unraveling the what and how of organizational communication to employees during COVID-19 pandemic: Adopting an attributional lens. The Journal of Applied Behavioral Science, 56, 289–293. https://doi.org/10.1177/0021886320937026
Sawhney, G., Jennings, K. S., Britt, T. W., & Sliter, M. T. (2018). Occupational stress and mental health symptoms: Examining the moderating effect of work recovery strategies in firefighters. Journal of Occupational Health Psychology, 23(3), 443.
Stephens, C., & Long, N. (2000). Communication with police supervisors and peers as a buffer of work-related traumatic stress. Journal of Organizational Behavior, 21, 407–424.
Tajfel, H., & Turner, J. C. (1985). The social identity theory of intergroup behavior. In S. Worchel & W. G. Austin (Eds.), Psychology of intergroup relations (2nd ed., pp. 7–24). Nelson-Hall.
Thoits, P. A. (1983). Multiple identities and psychological well-being: A reformulation and test of the social isolation hypothesis. American Sociological Review, 174–187.
U.S. Bureau of Labor Statistics. (2019). Economic new release: Table 1. Workers who could work at home, did work at home, and were paid for work at home, by selected characteristics, averages for the period 2017–2018. https://www.bls.gov/news.release/flex2.t01.htm
van der Meer, T. G., Verhoeven, P., Beentjes, H. W., & Vliegenthart, R. (2017). Communication in times of crisis: The stakeholder relationship under pressure. Public Relations Review, 43, 426–440. https://doi.org/10.1016/j.pubrev.2017.02.005
Vander Elst, T., Baillien, E., De Cuyper, N., & De Witte, H. (2010). The role of organizational communication and participation in reducing job insecurity and its negative association with work-related well-being. Economic and Industrial Democracy, 31, 249–264. http://journals.sagepub.com/loi/eida
Vega, R. P., Anderson, A. J., & Kaplan, S. A. (2015). A within-person examination of the effects of telework. Journal of Business and Psychology, 30(2), 313–323. https://doi.org/10.1007/s10869-014-9359-4
Wang, B., Liu, Y., Qian, J., & Parker, S. K. (2021). Achieving effective remote working during the COVID-19 pandemic: A work design perspective. Applied Psychology, 70(1), 16–59. https://doi.org/10.1111/apps.12290
Williams, L. J., Cote, J. A., & Buckley, M. R. (1989). Lack of method variance in self-reported affect and perceptions at work: Reality or artifact? Journal of Applied Psychology, 74, 462–468.
Zapf, D., Dormann, C., & Frese, M. (1996). Longitudinal studies in organizational stress research: A review of the literature with reference to methodological issues. Journal of Occupational Health Psychology, 1, 145–169.
Author information
Authors and Affiliations
Contributions
The first and second authors contributed to the study conception and design. Material preparation and data analyses were performed by the third and fourth author. The first draft of the manuscript was written by Dr. Gargi Sawhney, and all authors commented on the initial versions of the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
The study was approved by the IRB prior to data collection.
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Professional Isolation
-
1.
It is easy to relate to your coworkers
-
2.
You are isolated from your coworkers
-
3.
It is easy to get in touch with your coworkers
-
4.
You are separated from your coworkers
-
5.
You have coworkers to share your feeling with
Management Communication
-
1.
The management kept me in the loop while making decisions about employees working remotely
-
2.
The amount of information I received about working remotely from the management was adequate
-
3.
The information I received from the management about working remotely was timely
-
4.
The information I received from the management about working remotely was accurate
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sawhney, G., Jimenez-Gomez, C., Cook, P. et al. Isolated and Stressed? Examining the Effects of Management Communication in Alleviating Mental Health Symptoms during COVID-19. Occup Health Sci 7, 89–110 (2023). https://doi.org/10.1007/s41542-022-00133-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41542-022-00133-9