
Abstract
To assess New Zealand mental health clinicians and trainees’ knowledge, usage patterns, and attitudes towards digital mental health tools and their potential role in clinical practice. Participants recruited through professional organisations and training programs completed an online survey (August 2021 to February 2022). Eligible participants included Registered Health Professionals working in mental health or those enrolled in relevant training programs. The survey explored their knowledge, use of digital interventions, and perspectives on incorporating digital tools into clinical practice. Quantitative responses were summarised for the entire sample, and free-text responses regarding perceived benefits and concerns were coded to establish their relative importance. One hundred forty-four people started the survey and a total of 118 participants (77% female, 68% NZ European) completed it. Key findings indicated that 81% of the respondents had used digital tools, 65% rated their knowledge as moderate or higher, and 86% expressed interest in utilising digital tools. The primary advantages included ease of access and empowerment for clients, while concerns centred around the digital divide and the threat that digital tools may be used to replace traditional services. Clinicians demand more support and training including access to locally accredited tools. Blended (digital interwoven with in-person) support was highly favoured too. New Zealand mental health clinicians generally hold favourable views towards digital tools, with a significant proportion already trying them in their clinical practice. Clinicians are wary of digital approaches exacerbating existing inequities and want free of charge, secure, user-friendly, and evidence-based tools.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The popularity of commercially available smartphone apps to support mental health and wellbeing has grown significantly, increasing from 10,000 in 2017 to 20,000 in 2021 (Gooding, 2019). These apps have primarily targeted self-management of mild to moderate mental health issues such as depression, anxiety, and stress. Consequently, meaningful integration of digital tools into clinical practice has progressed slowly (Wozney et al., 2017). However, with the onset of the global pandemic in 2020, mental health services were compelled to embrace digital technology (Farrer et al., 2022). For many health practitioners and their clients, this marked their first experience with digital health tools (Wind et al., 2020). The pandemic is believed to have significantly heightened awareness, enthusiasm, and the likely future acceptance of digital tools in healthcare (Torous et al., 2020).
The increasing demand for mental healthcare, driven by escalating rates of mental distress and illness, underscores the pressing need for innovation, with digital tools poised to play a pivotal role (Rucklidge et al., 2018; Whiteford et al., 2016). If widely adopted, these tools hold the potential to transform healthcare, bridging treatment gaps and providing effective care to many individuals who otherwise might not access mental health services (Gooding, 2019; Gratzer et al., 2021). A substantial body of clinical trials has demonstrated the effectiveness of digital interventions across diverse modalities, diagnoses, and levels of problem severity (Batra et al., 2017; Deady et al., 2017).
An increasing array of devices, websites, apps, and wearable technologies have demonstrated the ability to enhance healthcare quality while containing costs. However, the integration of digital mental health tools into clinical care has been slow (Wind et al., 2020). Research underscores the pivotal role of clinicians in promoting the adoption and engagement of digital health tools among clients. However, this is significantly contingent on their knowledge and perceptions of the ‘eHealth space’ (Jacob et al., 2020; Topooco et al., 2017). Keeping pace with technology and its applications and translating research findings into meaningful day-to-day clinical practice can pose challenges for clinicians (Fairburn & Patel, 2017).
Internationally, research on clinician knowledge, attitudes, and training in digital mental tools forms a relatively small body of work (Kerst et al., 2020). Overall, existing findings indicate that clinicians exhibit an interest in digital mental health and acknowledge its potential benefits; however, they harbour various concerns and face limitations regarding knowledge and training. These factors collectively hinder the widespread adoption and utilisation of this technology in clinical settings (Kerst et al., 2020; Surmann et al., 2017; Topooco et al., 2017).
Within New Zealand (NZ), only three studies pertaining to mental health clinicians and digital technology have been identified. Van Kessel (2021) explored the use of technology within therapy among clinical psychologists, revealing reasonable levels of technology adoption, including the use of emails and smart devices. Wilson and Donkin (2021) surveyed New Zealanders’ attitudes towards digital health interventions and noted that health practitioners exhibited greater knowledge and held more positive attitudes than the general population. Variava et al. (2021) found modest levels of digital competency among a sample of NZ clinical psychologists, with high competence in managing ethical obligations in the digital space but lower proficiency in conducting psychological assessments online.
In New Zealand, the public enjoys access to a number of evidence-based tools developed both domestically and internationally. Many of these tools receive support or funding from the Ministry of Health/Te Whatu Ora (Health NZ) (DaRocha et al., 2021). The government is actively shaping a Digital Strategic Framework to steer the utilisation of digital technologies within the public health system. Furthermore, it endorses innovation in digital health and has allocated funding for digital wellbeing tools (McBeth, 2021; Ministry of Health, 2020).
Our study aimed to enhance our understanding of how mental health clinicians in New Zealand use and perceive digital health interventions. We placed particular emphasis on identifying the strengths clinicians associate with these interventions and the concerns they harbour regarding integrating digital mental health tools into clinical settings. Our study employed the umbrella term ‘digital mental health tools,’ encompassing online structured eTherapy, informational websites, smartphone apps, chatbots, and virtual reality.
Method
Participants and Procedure
The inclusion criteria required participants to be Registered Health Practitioners (RHPs) working in New Zealand mental health services or be enrolled in a specialist clinical training program (such as clinical psychology, counselling psychology, psychiatry). In New Zealand, legislation mandates that individuals who practise certain health professions (e.g. nursing, occupational therapy or psychology) must be registered with their respective regulatory bodies (Ministry of Health, 2023).
Recruitment ran from August 2021 to February 2022. Professional associations, organisations for mental health RHPs and coordinators from training programs were contacted to distribute an electronic recruitment poster to their members/staff. The study flyer was posted in relevant social media groups. Social media advertisements ran on Instagram and Facebook from October to November 2021.
Participants were invited to complete a brief questionnaire hosted on Qualtrics. They were presented with an on-screen participant information sheet and subsequently granted electronic consent to participate in the study, with the option to discontinue the survey at any point. They could opt-in to enter a prize draw for one of three $50 vouchers. This project was approved by the University of Auckland Human Participants Ethics Committee (UAHPEC), reference number: UAHPEC22599.
Measures
The survey comprised 28 questions, four conditional, and these were organised into two sections: (1) knowledge and use and (2) attitudes towards digital tools. Demographic questions were placed at the end. The questions encompassed a variety of formats, including five-point Likert scales, yes/no responses, multiple-choice selections, and free-text input.
Knowledge and Use of Digital Tools
Participants were asked how much they knew about digital mental health tools, if they had used them before and if clients had asked about them. If digital tools had been used, follow-up (conditional) questions were asked (e.g. the type of tools used, which particular tools and frequency of use). We also asked where participants go to find digital tools and to rate their digital literacy from ‘no knowledge’ to ‘expert knowledge’.
We asked a range of questions about participants’ confidence and interest in using digital tools, the potential role they might play in supporting clients, what elements made tools useable, how important it was to have digital tools designed for specific populations, and what could increase the uptake of digital mental health tools. Finally, we asked participants to identify what they saw as digital tools’ advantages and their concerns about using digital tools in clinical practice.
Demographic and Professional Characteristics
We collected demographic information, including gender, age, ethnicity, and location within New Zealand. Additionally, we inquired about participants’ type of work or training, years of clinical experience, professional degree (if currently working) or type of training program (if a trainee), speciality, and the institution where they received their training. It is worth noting that not all questions were mandatory, and some allowed for the selection of multiple answers.
Analyses
All quantitative data from the survey were analysed using SPSS Version 28.0.1.0. Descriptive statistics were used to describe frequencies. As the study was explorative, no statistical testing of differences was deemed appropriate. The qualitative data from the free-text responses underwent a coding analysis process using NVivo software Release 1.61 to identify recurring and common categories within the dataset. We followed the Braun and Clarke (2006) approach and started by reading through all the free-text responses to gain a general understanding of the content. Next, we assigned codes to portions of the text that represented specific ideas. If a response included more than one idea, several codes were assigned. Both authors reviewed the coded data and, over time, through consensus, arrived at a final list of codes for each question.
Results
Sample Characteristics
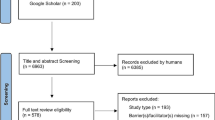
144 people answered at least a part of the survey, and 118 completed it fully. We present the results for each question based on the available data and note the sample size in each case. Participants were primarily (77%) female. Most (68%) identified as NZ European and 79% were between 31 and 60 years old. Full demographics are in Table 1 below (note: the demographics section concluded the survey and garnered the lowest number of responses).
Most participants (59%) were employed full-time, and most (82%) worked with adult clients. The majority (58%) were employed in the public health system, and two-thirds (66%) worked in secondary services (community/outpatient). 13% of the sample were trainees/students, and most were enrolled full-time. A full description of professional characteristics is in Table 2 below.
Use and Knowledge of Digital Mental Health Tools
Overall, from 144 responses collected in this section, 81% (n = 117) had previously used digital mental health tools with a client. Almost half (n = 67, 47%) reported knowing a moderate amount about digital mental health tools, 34% (n = 49) had ‘a little’ knowledge, and 15% (N = 22) reported knowing’a lot’. 11% (n = 13) rated their level of digital literacy as beginner, 64% (n = 75) as intermediate and 25% (n = 30) as expert.
For those who had used digital tools, smartphone apps (n = 95, 84%) were most commonly used, followed by informational websites (n = 76, 67%) and online structured eTherapy (n = 54, 48%). When asked how often they used digital tools, of 113 responses, most (n = 86, 60%) used them with either “few” or “some” clients, 14% (n = 20) used it with most clients, 1% (2 people) used it with all clients and 4% (n = 5) have never used them at all.
When asked to list the most commonly used digital tool (participants could list more than one), eight tools were named by more than ten respondents each. These included: Headspace (n = 56), Calm (n = 33), Just a Thought (n = 24), Smiling Mind (n = 20), The Lowdown (n = 18), SPARX (n = 17), GROOV (n = 14) and Centre for Clinical Interventions/CCI (n = 14)Footnote 1.
Half of the clinicians surveyed (n = 69, 50%) reported instances where their clients or clients’ family members initiated discussions about digital mental health tools. These conversations often revolved around specific tools clients had encountered, with inquiries about the clinician’s recommendation. Additionally, some clients were curious about whether particular tools were suitable for their needs. Some clients took the initiative by bringing digital mental health tools to their sessions, asking for clinical opinions or wanting to share feedback.
When asked if participants knew where to find evidence-based digital mental health tools, out of 135 responses, just over half (57%) either ‘somewhat agreed’ or ‘strongly agreed’ with the statement. The predominant methods (of which participants could list more than one) reported for discovering digital tools included internet searches (n = 67), consultation with colleagues and professional resources (n = 55), and reliance on reputable New Zealand health websites (n = 31).
Attitudes
Based on 130 responses, a significant majority (86%) of clinicians expressed a keen interest in using digital mental health tools, with 65% indicating a high level of confidence in their usage. However, respondents held mixed opinions regarding the availability of evidence-based tools, as nearly half (47%) neither concurred nor disagreed with this statement.
Participants were asked to provide their level of agreement with several statements concerning the potential roles of digital tools. These statements are presented in Table 3, ordered from the highest to lowest level of endorsement.
We asked participants to rate the importance of different features/elements when considering mental health tools. Data security, being free, and ease of use were the three most highly rated features. Responses are presented in Table 4.
When asked about the importance of having digital mental health tools tailored for specific populations, there was a nearly unanimous consensus, with over three-quarters expressing that it was either “essential” or “very important.” This sentiment extended to digital tools designed for various marginalised groups, including Māori, Pasifika, LGBTQ + , individuals with disabilities, immigrants, and refugees (refer to Table 5).
Clinicians surveyed in our study favoured ‘blending’ digital tools with face-to-face therapy (76% rated this approach as ‘extremely’ or ‘very useful’). Self-help and tools utilised with clinician oversight received nearly equal ratings (49% and 51%, respectively, rated as ‘extremely or very useful’). Refer to Table 6 for details.
Clinicians believed that a library of digital tools would be one of the most effective strategies to assist them in using or recommending digital mental health tools (82% considered it ‘extremely’ or ‘very useful’). There was also strong support for having access to digital tools specifically designed for use in therapy, and the majority thought it would be beneficial to have some tools officially endorsed (see Table 7 for details).
Clinicians were invited to provide free-text descriptions of the primary benefits and concerns associated with digital mental health tools. The responses were coded into six main themes, and the advantage most frequently highlighted was “Ease of access.” In comparison, the predominant concern (out of ten themes) revolved around the “Digital divide” issue. For details and exemplar responses, refer to Tables 8 and 9.
We asked clinicians to describe features of a hypothetical digital mental health tool they would find most helpful. Their responses were coded into six themes, and the most common suggestion involved having tools that clinicians could use directly with their clients. For details, refer to Table 10.
Finally, clinicians had the opportunity to provide additional suggestions to facilitate their future use of digital mental health tools. Four primary recommendations surfaced, and the top one included endorsement from health authorities (see Table 11 for details).
Discussion
Principal Findings
A significant majority (81%) of New Zealand mental health clinicians have used digital mental health tools with their clients in the past. Their perception of digital technology is predominantly positive, and they express a desire for further knowledge in this field. A significant proportion (65%) felt confident using digital mental health tools, but only 3% rated their knowledge highly. The tools most frequently utilised include smartphone apps and informational websites, with some clinicians reporting the use of online structured eTherapy programs, including those endorsed or funded by NZ’s Ministry of Health. Interestingly, half of the surveyed clinicians noted that their clients or their clients’ whānau have inquired about digital tools, reflecting a noteworthy level of interest about the potential benefits of digital mental health tools within the community.
The primary advantages of these tools, as noted by clinicians, include ease of access, the promotion of independence and empowerment among clients, and their role as valuable adjuncts to therapy or homework assignments. A predominant concern revolves around the existing digital divide, with worries centering on the limited access to digital mental health tools within marginalised communities potentially deepening existing inequities in mental healthcare. While clinicians largely concur (84% agreement) on the instrumental role of digital mental in supporting treatment, they emphasised that these tools should not be regarded as substitutes for traditional services. Respondents also expressed uncertainty about whether digital mental health tools can improve or diminish the relationship between clinician and client (44% neither agreeing or disagreeing).
In response to what would be most useful, blended approaches (integrated with in-person sessions) were regarded most favourably. Most clinicians also would like to see the introduction of tools that their clients could utilise under clinical supervision. The key to fostering greater adoption and clinical integration of these tools appears to hinge on several factors. These include increased training, the availability of resources, and clear guidance from health authorities on the suitability and efficacy of specific tools.
Comparison to Other Literature
Only two prior studies in New Zealand have explored this area, and our survey offers a timely update, considering the substantial changes in the digital landscape in recent years. In 2016, Van Kessel (2021) surveyed New Zealand psychologists’ use and attitudes toward digital technology, revealing that 71% used smart devices and 23% employed websites –— figures that were lower than those in our findings. Both our study and Van Kessel’s research uncovered a notable interest in blended approaches (a combination of online and face-to-face therapy). This finding is particularly intriguing, as such an approach has gained traction overseas but remains relatively uncommon in New Zealand (Wentzel et al., 2016).
More recently, Wilson and Donkin (2021) surveyed NZ adults’ attitudes to digital interventions, out of whom 104 were health professionals. Their findings suggest that they were more knowledgeable and held more positive attitudes toward digital interventions than the general population. Furthermore, mental health professionals held more positive views than other physical/general health practitioners. Wilson and Donkin (2021) suggested that the uptake of uptake of digital interventions in NZ could be achieved through training for health professionals, increase use in blended approaches and co-design with Māori.
Clinicians in our survey seem to hold slightly more favourable views toward digital mental health tools than earlier overseas studies, such as Surmann et al. (2017) or Topooco et al. (2017). This shift in perspective could be attributed to evolving societal changes and the increased adoption of technology, potentially accelerated by the events of the pandemic. On the other hand, our findings resonate fairly well with the positive attitudes of Australian clinicians found by Kerst et al. (2020) and even an earlier study by Sinclair et al. (2013). This may suggest certain similarities between the New Zealand and Australian contexts compared to other health or social contexts in more distant countries. It is noteworthy that clinicians worldwide share comparable concerns regarding the risks associated with adverse outcomes and data security/privacy, as highlighted in the systematic review by Jacob et al. (2020).
Previous research, e.g. Kerst et al. (2020) and Topooco et al. (2017) found clinicians to be worried about the perceived impact on the clinician-client relationship while our respondents were ‘on the fence’ in relation to this issue. However, unlike the studies by Kerst et al. (2020) and Topooco et al. (2017), we found that clinicians were optimistic about digital tools for clients suffering from severe mental illness.
The clinicians in our study exhibited a predominant concern for the digital divide, data security/privacy, and the potential risks of adverse outcomes. While these concerns do surface in international literature (Jacob et al., 2020; Kerst et al., 2020; Surmann et al., 2017; Topooco et al., 2017), they appear to hold a higher level of significance for New Zealand clinicians compared to their counterparts abroad. The heightened emphasis on data security/privacy may stem from prior cybersecurity incidents targeting the New Zealand health system (Pullar-Strecker, 2021). Moreover, data is esteemed as “taonga” or treasure within the Māori worldview. As such, it is guaranteed protection under Te Tiriti o Waitangi, a treaty recognised and affirmed by New Zealand courts (Taiuru, 2018).
Strengths and Limitations
The survey commenced in August 2021, a fortnight before the COVID-19 Delta wave surged, prompting various regions in New Zealand to implement a range of restrictions that remained in effect until early December. During this period, the healthcare system faced heightened stress, with a redirection of time, energy, and resources to manage the crisis. While we received a satisfactory response rate from a diverse group of clinicians, we collected fewer than expected number of responses. Therefore, we refrained from conducting subgroup analyses to assess potential variations among participant groups based on factors such as speciality. We also observed attrition as the survey progressed and, in particular, our sample size for the demographics section was the smallest. We left a number of items optional to give participants flexibility but this means our data is not always complete. It is important to emphasise that our study solely delved into the New Zealand context, and while it holds significance within this context, the findings may not be applicable to other countries and healthcare jurisdictions.
Despite our dedicated recruitment efforts, including collaboration with ethnic-specific organisations, our survey yielded relatively low response rates from Māori (8%), Pasifika (2%), and Asian (9%) ethnic groups. Addressing this disparity should be considered a priority for future research, given that 16% of the clinical mental health workforce identify as Māori, and 4% identify as Pasifika (Te Pou o te Whakaaro Nui, 2018). Additionally, we had a limited response from trainees (n = 16), and it is plausible that their perspectives on digital tools may differ and due to generational differences, may potentially influence future trends in this field.
Lastly, it is important to acknowledge the potential presence of self-selection bias in our findings. It is conceivable that our survey attracted clinicians who have a greater-than-average interest in digital health and higher digital literacy. In the process, we may not have reached those individuals with less favourable attitudes toward digital tools, lower utilisation of digital technology, or those who were disinterested or unaware of this evolving field.
Notwithstanding the aforementioned limitations, our survey is timely and contributes insights into the current landscape of New Zealand mental health clinicians’ utilisation, perceptions, and apprehensions related to digital mental health tools. These findings offer guidance to researchers, policymakers, and software developers to facilitate the adoption of digital innovations in clinical practice.
Implications and Future Directions
Based on the most relevant findings, the following future directions can be considered:
-
1.
Local leadership and support for clinicians to enhance their skills in this field are essential. Relying on clinicians to individually evaluate each digital tool is impractical. Instead, they would prefer an accessible and searchable library of endorsed resources tailored for use in the New Zealand context. Such a resource would boost clinician confidence in recommending digital mental health tools to clients and alleviate the workload of busy professionals
-
2.
Exploring blended or clinician-supported digital approaches for potential implementation in New Zealand is imperative. This approach garners substantial support and has seen success in other countries, though its adoption in New Zealand remains limited. Options include adapting existing programs or developing new tools tailored to New Zealand’s unique healthcare needs.
-
3.
Data and IT security need to be at the forefront of the development and implementation of digital tools. Confidentiality and privacy are essential to clinical practice, and this must be guaranteed before clinicians can be comfortable recommending digital mental health tools to clients.
-
4.
Care is needed to ensure that the introduction of digital tools does not exacerbate existing inequities. Cost and access to digital devices/data are a concern and may marginalise some groups further. Free-to-use tools, loan devices, and offline or zero-data-rated resources are some ways in which this could be addressed.
-
5.
Continue assessing clinicians’ (and other stakeholders) needs. Digital mental health is a fast-developing area. Therefore, ongoing monitoring is needed to ensure the information on the needs, concerns and adoption of digital mental health tools is up to date.
These future directions are geared towards promoting the seamless integration of digital mental health tools into the New Zealand healthcare system, with a focus on improving accessibility while upholding stringent standards of security, equity, and user-friendliness.
Conclusion
Technology has the potential to transform how people support their mental health and engage with health services, including mental health and wellbeing support. Clinicians and the public are interested in the digital space, but time will tell how this impacts the delivery of health services in practice. The Ministry of Health in New Zealand has commenced some of this work by developing the Digital Health Strategic Framework, the assessment framework for e-mental health (the Digital Mental Health and Addiction Tool) and funding the development of tools (Ministry of Health, 2020, 2021a, b). This work needs to continue to grow, and with the current momentum of digital health, now may be the optimal time to integrate digital technology into New Zealand healthcare.
Clinicians should be at the forefront of transforming how digital health integrates with traditional clinical face-to-face practice. Developers of digital mental health tools need to work closely with clinicians to create tools that meaningfully integrate into clinical practice.
Data Availability
The collection and analysis of the data were conducted under strict ethical guidelines that do not permit individual data sharing, as it was not covered by the existing ethics approval for this research. Interested researchers may contact the corresponding author for further inquiries regarding the study's methodology or high-level findings.
Notes
The Lowdown, Just a Thought, SPARX and GROOV are New Zealand based and nationally rolled out digital wellbeing tools.
References
Batra, S., Baker, R. A., Wang, T., Forma, F., DiBiasi, F., & Peters-Strickland, T. (2017). Digital health technology for use in patients with serious mental illness: A systematic review of the literature. Medical Devices (auckland, NZ), 10, 237.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101.
DaRocha, M., Chinn, V., Ormerod, F., & Fleming, T. (2021). Aotearoa New Zealand Digital Tools for Mental Health and Wellbeing: Stocktake. Wellington: Te Hiringa Hauora | Health Promotion Agency.
Deady, M., Choi, I., Calvo, R. A., Glozier, N., Christensen, H., & Harvey, S. B. (2017). eHealth interventions for the prevention of depression and anxiety in the general population: A systematic review and meta-analysis. BMC Psychiatry, 17(1), 310. https://doi.org/10.1186/s12888-017-1473-1
Fairburn, C. G., & Patel, V. (2017). The impact of digital technology on psychological treatments and their dissemination. Behaviour Research and Therapy, 88, 19–25. https://doi.org/10.1016/j.brat.2016.08.012
Farrer, L., Clough, B., Bekker, M., Calear, A., Werner-Seidler, A., Newby, J., Knott, V., Gooding, P., Reynolds, J., Brennan, L., & Batterham, P. (2022). Telehealth use by mental health professionals during COVID-19. Australian & New Zealand Journal of Psychiatry. https://doi.org/10.1177/00048674221089229
Gooding, P. (2019). Mapping the rise of digital mental health technologies: Emerging issues for law and society. International Journal of Law and Psychiatry. https://doi.org/10.1016/j.ijlp.2019.101498
Gratzer, D., Torous, J., Lam, R. W., Patten, S. B., Kutcher, S., Chan, S., Vigo, D., Pajer, K., & Yatham, L. N. (2021). Our digital moment: Innovations and opportunities in digital mental health care. The Canadian Journal of Psychiatry, 66(1), 5–8. https://doi.org/10.1177/0706743720937833
Jacob, C., Sanchez-Vazquez, A., & Ivory, C. (2020). Social, organizational, and technological factors impacting clinicians’ adoption of mobile health tools: Systematic literature review. JMIR mHealth and uHealth. https://doi.org/10.2196/15935
Kerst, A., Zielasek, J., & Gaebel, W. (2020). Smartphone applications for depression: A systematic literature review and a survey of health care professionals’ attitudes towards their use in clinical practice. European Archives of Psychiatry and Clinical Neuroscience, 270(2), 139–152. https://doi.org/10.1007/s00406-018-0974-3
McBeth, R. (2021). Digital wellbeing tools funded by MoH. Health Informatics New Zealand (HiNZ). Retrieved September 2023, from https://www.hinz.org.nz/news/560713/Digital-wellbeing-tools-funded-by-MoH.htm
Ministry of Health. (2017). HISO 10001:2017 ethnicity data protocols. Retrieved September 2023, from https://www.health.govt.nz/system/files/documents/publications/hiso_10001-2017_ethnicity_data_protocols_may-21.pdf
Ministry of Health. (2020). Digital health strategic framework. Retrieved September 2023, from https://www.health.govt.nz/our-work/digital-health/digital-health-strategic-framework
Ministry of Health. (2021a). Assessment framework for safe e-mental health tools. Retrieved September 2023, from https://www.health.govt.nz/our-work/digital-health/other-digital-health-initiatives/assessment-framework-safe-e-mental-health-tools
Ministry of Health. (2021b). Digital enablement. Retrieved September 2023, from https://www.health.govt.nz/our-work/digital-health/digital-enablement
Ministry of Health. (2023). Health Practitioners Competence Assurance Act: Responsible authorities under the Act. Retrieved September 2023, from https://www.health.govt.nz/our-work/regulation-health-and-disability-system/health-practitioners-competence-assurance-act/responsible-authorities-under-act
Te Pou o te Whakaaro Nui. (2018). Workforce stocktake- Final report to the government inquiry into mental health & addiction, June 2018. New Zealand mental health and addiction workforce: challenges and solutions. Retrieved September 2023, from https://mentalhealth.inquiry.govt.nz/assets/Summary-reports/Te-Pou-Stocktake.pdf
Pullar-Strecker, T. (2021). Ransomware attack: Waikato DHB supporting patients after documents dumped online. Stuff. Retrieved September 2023, from https://www.stuff.co.nz/business/125592089/ransomware-attack-waikato-dhb-supporting-patients-after-documents-dumped-online
Rucklidge, J. J., Darling, K. A., & Mulder, R. T. (2018). Addressing the treatment gap in New Zealand with more therapists – Is it practical and will it work? New Zealand Medical Journal, 131(1487). Retrieved September 2023, from https://www.nzma.org.nz/journal-articles/addressing-the-treatment-gap-in-new-zealand-with-more-therapists-is-it-practical-and-will-it-work
Sinclair, C., Holloway, K., Riley, G., & Auret, K. (2013). Online mental health resources in rural Australia: Clinician perceptions of acceptability. Journal of Medical Internet Research. https://doi.org/10.2196/jmir.2772
Surmann, M., Bock, E. M., Krey, E., Burmeister, K., Arolt, V., & Lencer, R. (2017). Einstellungen gegenüber eHealth-Angeboten in Psychiatrie und Psychotherapie. Der Nervenarzt, 88(9), 1036–1043. https://doi.org/10.1007/s00115-016-0208-8
Taiuru, K. (2018). Why data is a Taonga: A customary Māori perspective. Retrieved September 2023, from https://www.taiuru.maori.nz/wp-content/uploads/Data-is-a-taonga.pdf
Topooco, N., Riper, H., Araya, R., Berking, M., Brunn, M., Chevreul, K., Cieslak, R., Ebert, D. D., Etchmendy, E., Herrero, R., Kleiboer, A., Krieger, T., Garcia-Palacios, A., Cerga-Pashoja, A., Smoktunowicz, E., Urech, A., Vis, C., Andersson, G., & consortium, E. C. (2017). Attitudes towards digital treatment for depression: A European stakeholder survey. Internet Interventions, 8, 1–9. https://doi.org/10.1016/j.invent.2017.01.001
Torous, J., Jän Myrick, K., Rauseo-Ricupero, N., & Firth, J. (2020). Digital mental health and COVID-19: Using technology today to accelerate the curve on access and quality tomorrow. JMIR Mental Health. https://doi.org/10.2196/18848
Van Kessel, K. (2021). Clinical psychologists’ attitudes towards using technology in therapy: A survey. Journal of the New Zealand College of Clinical Psychologists, 31(1), 3–9. Retrieved September 2023, from https://www.nzccp.co.nz/assets/Journal-NZCCP-Vol-311-2021.pdf
Variava, R., Douglas, M., Dobson, R., & Reynolds, L. (2021). Exploring the digital health literacy of psychologists in Aotearoa New Zealand. Journal of the New Zealand College of Clinical Psychologists, 31(1), 32–34. Retrieved September 2023, from https://www.nzccp.co.nz/assets/Journal-NZCCP-Vol-311-2021.pdf
Wentzel, J., van der Vaart, R., Bohlmeijer, E., & van Gemert-Pijnen, J. (2016). Mixing online and face-to-face therapy: How to benefit from blended care in mental health care. JMIR Mental Health, 3(1), e4534.
Whiteford, H., Ferrari, A., & Degenhardt, L. (2016). Global burden of disease studies: Implications for mental and substance use disorders. Health Affairs, 35(6), 1114–1120. https://doi.org/10.1377/hlthaff.2016.0082
Wilson, H., & Donkin, L. (2021). Understanding New Zealand adults’ attitudes towards digital interventions for health. Psychological Applications and Trends. https://doi.org/10.36315/2021inpact011
Wind, T., Rijkeboer, M., Andersson, G., & Riper, H. (2020). The COVID-19 pandemic: The “black swan” for mental health care and a turning point for e-health. Internet Interventions. https://doi.org/10.1016/j.invent.2020.100317
Wozney, L., Newton, A., Gehring, N., Bennett, K., Huguet, A., Hartling, L., Dyson, M., & McGrath, P. (2017). Implementation of eMental Health care: Viewpoints from key informants from organizations and agencies with eHealth mandates. BMC Medical Informatics and Decision Making, 17(1), 78. https://doi.org/10.1186/s12911-017-0474-9
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
This project was approved by the University of Auckland Human Participants Ethics Committee (UAHPEC), reference number: UAHPEC22599.
Consent to Participate
Informed consent was obtained from all individual participants included in this study.
Consent for Publication
All individual participants consented for the results from this study to be disemminated publically.
Competing Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rawnsley, C., Stasiak, K. Unlocking the Digital Toolbox — A Mixed Methods Survey of New Zealand Mental Health Clinicians’ Knowledge, Use and Attitudes Towards Digital Mental Health Interventions. J. technol. behav. sci. (2024). https://doi.org/10.1007/s41347-024-00403-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41347-024-00403-z