
Abstract
Intentional and unintentional medication non-adherence is a particular challenge for patients with inflammatory bowel disease (IBD). Non-adherence can affect patients’ quality of life, which can result in unfavorable treatment outcomes, more hospitalizations, and higher healthcare-related costs. The purpose of this study was to assess whether a tailored text message intervention designed to modify illness and medication adherence beliefs in patients with IBD would increase treatment compliance and change patients’ illness perceptions and medication concerns. This pilot study utilized a pre-test-post-test non-randomized design. A sample of 32 IBD patients was recruited within the UK. Participants’ medication beliefs and illness perception scores determined the set of tailored daily text messages, which were sent to patients over duration of 12 weeks. Medication adherence increased post-intervention, as “forgetting to take medication” decreased while “never” forgetting to take medication increased over time. A significant increase in treatment control and coherence and a decreased level of concern surrounding their condition was evident. Participants’ level of concern towards their medications changed during the 12 weeks, with a baseline mean concern score of 3.08 (.57) in comparison to the 12 weeks mean concern score of 2.89 (.59), which is statistically different, t (31) = 2.16, p < .038, r = .36 (medium effect). Sixty-six percent of participants from the baseline were aware of the necessity of their medication: “without my medication I would become ill.” The results have direct implications for improving medication adherence and changing illness and medication beliefs. This study validated the benefits of text messages and highlighted the importance of addressing these beliefs in order to understand the reasons for non-adherence fully.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Inflammatory bowel disease (IBD) is used to describe two conditions which are characterized as chronic and lifelong: Crohn’s disease and ulcerative colitis (NHS Choices 2017). These idiopathic conditions affect around one in 250 people living within the UK, and are not gender-specific (Crohn’s and Colitis UK 2012). Although these conditions are not curable, treatment to manage the symptoms is frequently offered to patients. However, adherence is not always optimal, and patients with IBD go through stages of maintenance (when the inflammation reduces and the pain subsides) where they begin to feel better, and this is usually when noncompliance to their medication may begin (Broide et al. 2017). Despite the long-term benefits of these medications, a commitment to adhering to the medication regimen is challenging for most IBD suffers, and may not always take priority. The consequences of missing a dose can be detrimental, and is attributed to build-up over time, increasing disease progression.
The fundamental issues related to non-adherence are compounded by the complex nature of human behavior. Although the term “adherence” commonly refers to the physical act of taking medicine, its definition encompasses more than just the patient’s response towards medication, but instead takes into account the whole treatment experience. Horne et al. (2005) found that patients need to be supported throughout the experience, covering prescription, collection, and administration. Furthermore, they highlight that “stipulating unconditional and unquestionable adherence to prescribers’ instructions as our goal, in most cases, is not justified if the patient has not made an informed choice about taking their medication” (Horne et al. 2005, p. 37).
In a study by Ediger et al. (2007) explained that non-adherence to treatment can also be a result of the patient’s experience with medication, irrespective of gender. Ardizzone et al. (1999) found a link between drug palatability and drug formulation, which resulted in difficulties in swallowing the tablet, the dislike of loose powder, and unmanageable general or specific side effects of the medication, such as pain or abdominal discomfort. Similarly, D’inca et al. (2008) found that a significant reason for low treatment compliance to IBD medication was the high-dose expectation and complex regimen which required patients to take medication three times a day at specific time points. Other indicators of non-adherence were due to a lack of understanding of how and when to take the medication, skepticism about drug efficacy and safety, and forgetfulness (Engel et al. 2017).
Patients may not always be able to assess consciously the beneficial factors of taking their treatment as prescribed. Despite the fact that the benefits of adhering is associated with better overall health outcomes (Horne et al. 2005). Compliance to medication and the complicated relationship people develop regarding their diagnosis will differ for every individual: some may be very adherent, while others may be less. In the event that some are not compliant, there is a need to understand their reasons, which may not always be clear.
Illness Perception and Medication Beliefs
Leventhal et al. (1992) introduced the common-sense model (CSM) of illness representation, which suggests that patients’ beliefs surrounding their illness are integrated within existing schemas, which enable them to understand their condition and adopt coping strategies. The model consists of five components: (1) identity (the name/label given to the symptoms and conditions, which will differ for each patient’s perceptions), (2) cause (the personal adopted ideas as to the etiology of the condition, based on information gathered from personal experiences and health professionals), (3) timeline (the beliefs surrounding the duration of the condition, which are interchanging over the duration of the condition), (4) consequence (the beliefs surrounding how their condition will impact on their life, particularly the physical and social aspects), and (5) curability/controllability (the beliefs about whether this condition can be controlled or cured).
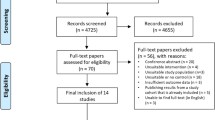
Leventhal et al. (1992) state that each patient develops an individualistic view that serves as the foundation of the illness beliefs, which change over time. The perceptions will evolve from the start of a diagnosis, while the individual is learning more about the condition and ways to cope. During this process, new representations are formed along the way, and these transition into the patient’s schemas. This, in turn, contributes to our understanding of how and why patients develop personal beliefs surrounding their medication and the ways in which they view their treatment pathway. For this reason, patients with the same condition can hold disparate views surrounding their illness, which may explain why some patients are adherent to their medication regimen and others are not (Fig. 1).

Consort diagram for the IBD TMI pilot study—illustrates the pathway of recruitment which led to the end of the research study
Illness Perception/Medication Beliefs and IBD
The multifactorial nature of medication adherence depends very much on how the patients perceive the benefits of their treatment, and on their understanding of the diagnosis. Kane and Shaya (2008) found that around 60% of patients fail to adhere to their prescribed medication dose, and around 70% fail to take their prescribed medication. Often, adherence research specific to IBD has found that patients become non-adherent when they begin to question the need for medication, particularly during periods of remission (Kane and Shaya 2008). Similarly, the fear of developing an addiction to the medication limits willingness to comply with planned treatment (Lesnovska et al. 2010). Horne et al. (2009) found that non-adherence to maintenance therapy was due to beliefs associated with the “need” for therapy and the potential adverse effects of long-term treatment. Therefore, understanding what these pre-conceived beliefs are—and then offering an interventional initiative which seeks to address these beliefs—should elicit change. Better understanding and knowledge about the treatment journey can increase patients’ self-efficacy in managing their illness and can highlight any pre-existing illness beliefs and medication concerns, which, in turn, supports increased compliance (Lenti and Selinger 2016).
The new generation of health interventions is moving towards digitized innovative methods that seek to support people in managing their health conditions more effectively. Interventions delivered through mobile platforms are increasing rapidly. We do not understand the long-term benefits of these mobile interventions and how they can change health behaviors, however. Research measuring the success of text messaging interventions (TMIs) has been published since 2002, with the first study of this kind focusing on mobile messaging and asthma (Neville et al. 2002). Since 2002, there have been a number of papers testing the impact of text messages as part of a health intervention, or as a standalone tool (Gerber et al. 2009; Franklin et al. 2006; Fjeldsoe et al. 2009). These studies have found promising results and have shown that TMIs are targeting a variety of health conditions such as weight loss (Gerber et al. 2009) and chronic health conditions such as asthma and diabetes (Franklin et al. 2006; Petrie et al. 2012).
TMIs are noticeably low-cost and adaptable, and the content of the messaging is quite flexible. This simple but sophisticated method has the capacity to reach a multitude of people across the globe. In addition, TMIs have a number of qualities such as offering personalized, time-specific messages, and the ability support reinforcement through repetition. Furthermore, this method can be significantly effective for those who use their mobile device frequently and enjoy communicating via this process (Hall et al. 2015). Mobile statistics have shown that 99% of sent text messages are opened, while 90% of all mobile text messages are read within 3 min of being received (Hall et al. 2015). Therefore, we can assume that sending health messages via this mode of communication will be accessible, effective, and measurable.
TMIs can be relatively successful, but developers should be mindful of how they deliver the messages. A recent review found that interventions that used personalized messages and messages of unpredictable frequency over the course of the interventions were more successful than interventions that offered a fixed messaging frequency (Head et al. 2013). This finding was similar to Vervloet et al. (2012) systematic review. This review specifically focused on the effectiveness of electronic reminders such as SMS, audio/visual reminders, pagers, and beeper systems. Within this critical review, non-adherent patients became adherent over time in all but two of the 13 studies. The two that were not successful were due to the frequency of the messages, as weekly reminders were deemed more appropriate than daily. The significance of reminder messages was ignored when reminders were sent daily, regardless of whether the patient had already taken their medication or not. Vervloet et al. (2012) argue that sending daily reminders develops a habituated attitude, which has a negative influence on the patient.
Studies evaluating IBD adherence to medication using behavioral interventions focusing on self-management techniques via SMS have found that TMIs, when offered to pediatric IBD patients, resulted in a significant increase in medication adherence over a period of 6–12 months. The modified text messages sent to patients were simple, short messages that only targeted adherence to medication and not illness beliefs or medication concerns (Keefer et al. 2011). This translates into other chronic conditions, as established in DeKoekkoek et al. (2015) review. They found 13 published TMI studies that have all validated the benefits of text messaging as an intervention to improve medication adherence across different chronic conditions, besides IBD.
The aim of this study was to evaluate the feasibility and acceptability of a mobile text messaging intervention aimed to increase adherence in people living with IBD. The objective was to evaluate the suitability of the intervention and to provide a preliminary evaluation of responses to the intervention. It was hypothesized that participants will show changes in their illness and medication beliefs, as well as improved adherence to their medication.
Methods
Study Design
The research design for this pilot study was a pre-test-post-test non-randomized design. Specifically, the research design was a within-subject design, which consisted of two time points (baseline and 12 weeks). All of the study participants took part in the same interventional offering in terms of frequency of messages. The independent variable was the use of tailored text messages specific to the participants’ beliefs, which were pre-defined from the questionnaire measurements. The study measured the difference in adherence to medication, changes in illness perception, and medication beliefs (dependent variables).
Participants
The target population for this pilot study consisted of participants from across the UK. The sample for this study was made up of adults who have a diagnosis of inflammatory bowel disease (IBD), aged 18 years and older, and who volunteered to participate in the 3-month study. Participants were required to have access to a mobile phone.
Participant Recruitment
Study participants were recruited via study adverts that were distributed around a university campus and local GP surgeries. Participants were also recruited via paid advertisement on popular social media sites. Facebook was chosen as the main recruiting site, as it has open access to the public and billions of daily users. A website domain was purchased and developed to assist potential participants in enquiring about or enrolling onto the study (www.crohnsdiseasestudy.org.uk). The designated website included relevant information for the study and directed participants to self-enroll by prompting them to complete an “I’m interested” form. Once completed, an email notification was sent to the researcher, who then emailed the consent form and participant information sheet to interested participants. The preloaded consent form, information sheet, and information related to the study were also found on the website. Using the CONSORT process, the recruitment lasted for approximately 2 months (January 2014 until March 2014).
There was a high number of interested participants at the beginning of the recruitment phase of this project (n = 122). Of the 122 who completed the “I’m interested” form, 32 signed and returned the consent form and completed the pre-questionnaire. Ninety potential participants did not respond to the invitation, accounting for an overall 26% recruitment rate. On completion of the study, all 32 participants completed the post-questionnaires. There were no incentives offered to participants.
Data Collection
The data collection process was accomplished in two phases, once at the beginning of the study, and once again at the end of the study. Validated questionnaires which have been tested for reliability were administrated at both time points (pre and post). Below is the outline of each questionnaire and scoring mechanism.
The Demographic Data Questionnaire was created by the researcher and collected basic medical history, age, gender, year of diagnosis, ethnicity, and medication usage.
The Brief Illness Perception Questionnaire (BIPQ; Broadbent et al. 2006) measured how a patient perceives their illness. The sub-constructs of illness perception cluster around five significant themes: identity, cause, timeline, consequences, and cure control. The following are some examples related to the sub-constructs: “Identity”—“how much does your illness effect your life?” (0 = “no effect at all” and 10 =
“severely effects my life”) and “Timeline—“how long do you think your illness will continue?” (0 = “a very short time” and 10 = ‘forever’). Each item is scored on an 11-point Likert scale. Total scores for this questionnaire were calculated by summing the item scores together and reverse scoring items 3, 4, and 7. A higher total score reflects a more threatening view of the illness, whereas a lower score indicates benign illness representation. The BIPQ has shown good test-re-test validity in six illness group psychometric properties, and has been shown to measure patients’ cognitive and emotional representation of their illness, including consequences, timeline, personal control, treatment control, identity, coherence, concern, emotional response, and causes (Broadbent et al. 2006).
Beliefs About Medication Questionnaire (BMQ; Weinman et al. 1996). BMQ assesses both the general and specific medication beliefs of a participant. The objective of this questionnaire is to help the researcher understand why some people fail to adhere to their medication by learning about their medication perception. The BMQ is divided into two sections: BMQ-General (sub-scales: Overuse and Harm, 4 items per sub-scale) and BMQ-Specific (sub-scales: Necessity and Concerns, 5 items per sub-scale). The specific section assesses patients’ beliefs about medications prescribed for an illness and comprises two scales assessing personal beliefs about the necessity of medication prescribed for controlling their illness. Sections included “my health at present depends on my IBD medicine” (5 statements) and concerns about the potential adverse consequences of taking it, i.e., “I sometimes worry about becoming too dependent on my IBD medication” (5 statements). Each statement has 5-point Likert scale answers (strongly disagree, disagree, uncertain, agree, and strongly agree). The answers are scored from 1 = “strongly disagree” to 5 = “strongly agree,” and the points of each scale are summed to give a scale score. Higher scores indicate stronger beliefs in the concepts of the scale (high/low necessity and high/low concern).
The Adherence Measure (Morisky et al. 1986) measured levels of medication adherence. Using one item question from the 4-item questionnaire, the adherence measure was presented to participants through the following question: “How often do you forget to take your medication?” Participants were asked to rate their level of adherence on a scale of 1 (“never”) to 6 (“very often”). The question was adapted from the validated Morisky Medication Adherence Scale (MARS). For the purposes of this study, the interest lay in understanding how often patients would forget to take their medication, as opposed to learning about the other variables within this measure (Morisky et al. 1986).
Procedure
Once the initial questionnaires were completed and received by the researcher, the information was logged and an email, and “test” text message were sent to the participants to confirm that their number was working and that they could receive text messages from the program number. Participants were prompted to reply to the email and to confirm their receipt of the message. Over the course of the12 weeks, participants were sent tailored text messages based on their baseline BIPQ and BMQ scores. Messages were selected randomly—but specific to each BIPQ scores—and participants who scored high or low on each of the targeted beliefs were sent messages from that category. If participants did not score high or low in the target beliefs, they were not sent text messages relating to that belief. The frequency of these messages differed over the 12 weeks (illustrated in Table 1). A completed template of messages which included allocated times for each message was preloaded onto a text messaging program every week in order to ensure accuracy of messages, and this was checked by the researcher on a weekly basis prior to the messages going out to participants. At the end of the 12 weeks, participants were prompted to repeat the pre-screener questionnaires, including the BMQ, BIPQ, and the adherence scale. Pre-and post-scores were used to measure the efficacy of the program.
Text Messages—Process Plan
Table 1 outlines the frequency of text messages sent to participants. There was a decrease in messages sent from weeks 4–8, with an increase to three messages per day from weeks 8–12. The frequency differed to allow participants to manage the informational load and engage with the study, instead of feeling overwhelmed with a continuous set of messages. Participants received targeted, tailored text messages related to their illness and medication beliefs. Each belief consisted of seven messages, giving a total of 112 messages. The aim of the messages was to address participants’ prior illness and medication beliefs relating to their condition (Tables 2 and 3).
Analytic Strategy
The data were analyzed using the statistical package SPSS version 22 (SPSS Inc.). Based on the aims of the research, changes in illness perception scores pre- and post-process were compared using a parametric paired sample t test. This was to test for any significant differences in participants’ illness perceptions within the sample group over the period of 3 months. In order to use the t test, the assumptions were met, ensuring that the data was normally distributed, the variance between the groups were equal, and the sample size was adequate (at least 30 cases).
The research aimed to measure a change in participants’ medications beliefs (necessity and concern) over 3 months, and a paired sample t test using the scores (pre/post) was conducted to examine the mean differences within the group. In addition, participants did not drop out of the study over the 3 months. The final complete data set did not include any missing data.
Although this is a pilot study, the post-screener offered space for participants to include qualitative feedback of their experience if they had any additional insight or recommendations regarding the acceptability and suitability of the intervention.
Sample Size
Lancaster et al. (2004) recommend that the sample size for a pilot study should be 30 participants. Other evidence has suggested that a sample size between 24 and 50 participants is justifiable for such a study.
Results
The study sample consisted of 32 participants with a mean age of 42 years all of whom completed pre- and post-questionnaires. Out of the 32 participants, 39% were white British, and 68% females. Demographic characteristics of study participants are shown in Table 4.
Medication Adherence
Self-reported adherence was measured at baseline and at the end of the 12 weeks. Participants were asked “how often do you forget to take your medication?” Figure 2 below illustrates the pre- and post-process self-reported medication adherence scores per participant over the 3 months. A total of 32 participants rated how often they forgot to take their medication on a scale of 1–6 (1 = never and 6 = very often).

Self-reported medication adherence rating
Medication adherence increased post-intervention, as “forgetting to take medication” decreased while “never” forgetting to take medication increased over time. The rate of self-reported adherence at pre-intervention was 1 (3.1%) and there was an increased level of change over 3 months, with the rate of adherence at 11 (34.4%) at the 3-month interval. This suggests that the tailored text messages increase medication adherence.
Illness Perception
There was no overall significant difference in illness perception, but significant changes occurred in three categories of the IPQ: concern, coherence, and treatment control. A paired sample t test reported an increase in treatment control and coherence, and a decreased level of concern surrounding their condition. This analysis shows that text messages did change the beliefs in a direction consistent with an increase in adherence.
The paired sample t test indicated a significant change in the data set when comparing pre- and post-intervention mean IPQ scores. In particular, there was a change in concern at baseline (M = 7.53, SD = 2.1), and at 12 weeks, (M = 6.66, SD = 1.8) which was significantly lower post-intervention, with t = (31), 2.35, p < .025. This was the same for coherence, at baseline (M = 3.09, SD = 1.9) and at 12 weeks (M = 6.53, SD = 3.0), and was significantly higher post-intervention, with t = (31), − 5.63, p < .001. Finally, treatment control at baseline (M = 3.91, SD = 1.9) and at 12 weeks, (M = 6.72, SD = 1.9) was significantly higher at 12 weeks, with t = (31), − 6.04, p < .001. There was no significant change in consequences, identity, timeline, and emotional representation.
Medication Adherence
Descriptive Statistics
The baseline means concern score of 3.08 (.57) in comparison to the 12-week mean concern score of 2.89 (.59) is statistically different; t (31) = 2.16, p < .038, r = .36 (medium effect). This suggests that participants’ level of concern towards their medications changed during the 12 weeks. When comparing the baseline necessity mean scores of 2.37 (.55) with post-intervention necessity mean scores of 2.39 (.74), no statistical significance was evident from the t test; t (31) = .171, p > .865. This change is consistent with an increase in adherence to medication, suggesting that when participants’ level of concern is decreased, they are more likely to adhere to their treatment.
Percentage Rating of Each Question Within the BMQ
Table 5 presents baseline and post-intervention self-reported participant measures for the Beliefs About Medication Questionnaire. Interestingly, the results indicate that 66% of participants at the baseline were aware of the necessity of their medication: “without my medication I would become ill.” This suggests that they agree that their health is dependent on their medication. Understanding the links between their health and medication increased post-intervention, with 71% of participants reporting that their health was reliant on their medication intake.
Concerns relating to the long-term effects of the medication were significantly high: at baseline, 91% of participants agreed “I sometimes worry…” This concern was also evident when 62% of participants agreed that “having to take medicine worries me.’ These worries decreased post-intervention, however, with only 37% agreeing that they were still worried about their medication.
Table 5 shows that a change in each domain has occurred from baseline to-post-intervention; this suggests that sending tailored text messages can change an individual’s beliefs surrounding their medication.
Discussion
This research evaluated the efficacy of personalized tailored text messages. Personalization was based on participants’ illness perceptions and medication beliefs. These results were analyzed over a 12-week period, and baseline, and post-test results were compared for each questionnaire administered. A statistical analysis was carried out in order to measure the significance of the data. The results found that a significant change occurred over the period of interest.
Self-reported medication adherence was shown to improve over the 12 weeks, with participants stating that they had started to “never or rarely” miss their medication dose. There was no specific set of text messages for the adherence category; instead, messages were tailored to each participant’s specific illness and medication beliefs, and this was the approach taken throughout the study.
Results from the illness perception questionnaire were compared pre- and post-intervention; evidently, a significant change occurred for three domains within the IPQ, namely concern, coherence, and treatment control. Participants’ levels of concern surrounding their condition reduced post-intervention. Coherence and treatment control increased post-intervention, which suggests that participants felt more in control of their condition, possibly as a result of the daily positive IBD messages which enabled participants to become more aware of the demands of their condition. The results support prior research which posits that personal beliefs about IBD play a significant part in the adjustment to the diagnosis (Leventhal et al. 1992; Horne et al. 2009; Tsianou et al. 2017; Lenti and Selinger 2017). So far, the hypothesis can be accepted, as the results have indicated a change in adherence, illness perception, and medication beliefs. In order to offer a detailed explanation of these findings, however, discussion will outline how and why these changes may have occurred and will investigate whether this was a true experimental effect and whether these findings are consistent with the common-sense model of illness representation.
Medication Adherence
Measuring adherence was instrumental in understanding whether text messages were eliciting any type of behavioral shift, particularly in terms of a change in medication. Similarly to the Petrie et al. (2012) study, this research has identified a positive medication adherence trend over the period of 3 months. Participants were more likely to “never” forget to take their medication post-intervention. Although this is a positive finding, understanding the occurrence of this shift will help in evaluating the methodology. Earlier discussions and the reviewed literature on adherence suggested that sending targeted messages specific to the individual, instead of generic messages, is generally more acceptable (Dekoekkoek et al. 2015; Head et al. 2013). Similarly, there is a consensus that patients may not always be willing to admit that they are not adhering to their medication. Given this, offering an alternative strategy for identifying patients and informing them about the benefits of medication via messaging has been shown to be effective in addressing some of the underlying concerns relating to non-adherence. Therefore, this type of intervention can be applied to those who may not always be in touch with their healthcare providers, and can offer a means of challenging any pre-conceived, unconscious assumptions regarding their medication.
Illness Perception Scale
Level of Concern
Participants’ levels of concern were measured via the illness perception scale, and the analysis reported a significant difference over the period of 3 months. This finding was consistent with previous research (Petrie et al. 2001). Indeed, this change is positive, but in order to help understand why there was a behavioral shift, we need to recognize why patients may hold these concerns. As discussed earlier, Kelly et al. (2014) systematic review stated that the most common themes for non-adherence was patients’ knowledge and attitude surrounding their medication, and the negative beliefs they associated with their treatment, including about side effects of the medication. They found that these perceived concerns influenced patients’ decisions to become non-adherent. Similarly, Moser et al. (1995) outlined some of the significant concerns held by IBD patients, including beliefs surrounding the possibility of having an ostomy bag, the general effects of medication, surgery, the uncertain nature of the disease, and lack of energy.
With this acknowledgment, both studies recommended that our understanding of the level of information patients have about their condition and any disease-related concerns should be queried and considered within clinical practice, thereby equipping patients to feel more empowered to self-manage their condition. These findings are consistent with Gadkari and McHorney (2012), who also believe that removing or altering patients preconceived negative beliefs surrounding their medication would increase medication adherence.
This study has been able to illustrate the links between the benefits of educating patients about their condition by reducing the number of preconceived concerns held by the individuals via text message. The process of sending personalized text messages—addressing topics such as “the effects of medication” and “the importance of managing your diagnosis”—has been shown to improve and reduce significant levels of concern.
Coherence
Participants’ coherence positively increased post-intervention; this change suggests that respondents felt more in control of their condition, and that receiving daily positive IBD messages enabled participants to become more aware of what their condition entails. Previous research has outlined the importance of coherence, and the benefits of addressing this. The concept of coherence is used to describe a person’s capacity to respond to stressful situations; given the complexity of living with IBD, personal resources and capabilities are often drawn upon in response to managing the condition. Given the significant increase in coherence post-intervention, we can assume that this method of addressing motivation and tackling challenges has been successful by providing clear and coherent information about IBD, which is an important protective factor against psychological stress. Findings such as this further support the imperative nature of tailored text messages, as this method opens many different communication pathways and permits the researcher to tackle other underlying factors such as coherence, which other methods may neglect.
Treatment Control
A lack of understanding about treatment can significantly influence how a patient may accept their diagnosis, or adhere to their treatment regimen. Patients fear a loss of control over their treatment decisions, as these are mostly left to the clinician. Therefore, taking responsibility for their treatment can represent delicate territory for some. Nevertheless, offering strategies to cope with and understand the importance and purpose of treatment for IBD can help to empower patients to feel a part of the process, instead of merely receiving and following orders. Effective management to change beliefs from “I am not in control of my treatment” to “I know I can make the right treatment decisions” can be empowering and motivating. The results from this study found a significant increase in treatment control after the 12 weeks. Participants felt more involved with their treatment, through understanding how their treatment was helpful in the short- and long-term, together with outlining the consequences of non-adherence. This was yet another positive finding, which supports the idea of sending targeted text messages.
Beliefs About Medication Scale
As discussed earlier, Tsianou et al. (2017) suggested that the most important factor affecting compliance with medication regimens is how one feels about the drugs they are prescribed, which then contributes to how successful they are in following the doctor’s advice. This is of interest, as this study has supported this assumption and confirmed that patients’ levels of concern around medication can be addressed through some types of interventional or conversation process. In practice, this should alter the concern threshold and increase patients’ awareness of necessity for their treatment. Although there was a significant change in levels of concern around medication, this was not transferred to heightened awareness of the necessity for treatment. Over the period of 12 weeks, the results found no significant change in participants’ beliefs about the necessity of treatment. This is not to say that the text messages did not address this; however, another explanation could be that at baseline, participants’ understanding that their treatment was necessary for their condition was already high, which is why a change did not occur.
This research aimed to uncover, challenge, and change the cognitive representation of IBD using text messages. An increase in treatment control and coherence represents the emergence of positive beliefs about controllability and personal understanding of IBD. Addressing these variables in isolation without the other measures has already shown a positive change with this technique. When comparing the outcomes of this study in combination, however, we can agree that this methodology has been positive and can confirm that offering non-conventional alternative strategies via technological interventions can be effective in targeting hard-to-reach patients across different regions. Therefore, this study has added to the IBD literature and has re-confirmed the findings of Petrie et al. (2001) in their asthma intervention. This transferable method can be applied to different therapy areas and offers the possibility of a significant change in attitudes and beliefs surrounding medication and diagnosis. Mobile interventions are scalable and cost-effective, and do not require face-to-face interactions for participants or researchers. This form of a narrative approach permits the researcher to devise effective and meaningful messages and encourages the delivery of informative health messages.
One participant observed: “I enjoyed taking part in this study, and I honestly felt the last text was a really positive boost (“you are doing your best to manage Crohn’s). At the time of receiving this, I was flaring more than I had been and it really made me feel positive.” This suggests that the text messages were not only supportive in encouraging medication intake, but that participants also utilized the messages as a source of positive encouragement and reinforcement. A recommendation to test this method in other chronic conditions can be considered; an extension of this study can also be suggested. There are, of course, other variables that could be introduced within this study design, such as quality of life measurements and or motivational measures of self-efficacy, in order to test whether the messages have increased intrinsic motivation and if this change can improve participants’ quality of life.
Mobile health is steadily increasing within the healthcare domain; studies such as this can help educate and enforce change. These findings can contribute considerably to the development and evaluation of other TMI interventions and verify the importance of developing subtle, innovative techniques that are based in health psychology theories.
Conclusions
This is the first study evaluating the effects of tailored text messages with IBD patients. Previous research has focused on asthma patients, as previously discussed, and has demonstrated a positive behavioral shift in beliefs and perceptions (Petrie et al. 2001). Studies that have adopted text messaging within their design have consistently shown improved health behavior outcomes, such as quality of life improvements, increases in health literacy, decreases in concerns about medication, and improvements in self-management.
The outcome demonstrates the efficacy of mobile text messages and shows positive results in eliciting change in prior beliefs and perceptions about individuals’ diagnoses and conditions. However, this process also acknowledges the weaknesses in this study, for instance medication compliance was based on patients’ self-report; adaption of this study should find alternative ways to collect data and not be reliant on self-report. The pilot study acquired a small sample size, and extending this for future studies can verify the results and be more representative to the general population.
Nevertheless, this inexpensive and useful tool, if used correctly, can make a positive impact in areas such as illness perceptions, medication beliefs, and levels of medication adherence for IBD patients. This evaluation has shown that tailoring text messages, although time-consuming, does in fact elicit positive change in areas where other techniques or methods may not be as effective.
References
Ardizzone, S., Bollani, S., Manzionna, G., & Porro, G. B. (1999). Inflammatory bowel disease approaching the 3rd millennium pathogenesis and therapeutic implications? European Journal of Gastroenterology & Hepatology, 11(1), 27–32.
BPS, (2014) Code of human research ethics. Retrieved from: http://www.bps.org.uk/sites/default/files/documents/code_of_human_research_ethics.pdf.
Broadbent, E., Petrie, K. J., Main, J., & Weinman, J. (2006). The brief illness perception questionnaire. Journal of Psychosomatic Research, 60(6), 631–637.
Broide, E., Dor, A. E., Ruhimovitch, N., Shitrit, A. B., Sklerovsky, F., Benjaminov, S. M., et al. (2017). Can we predict adherence to treatment in IBD patients? Gastroenterology, 152(5), S852.
Crohn’s and Ulcerative Colitis UK (2012) Retrieved from: http://www.nacc.org.uk/content/home.asp#top.
DeKoekkoek, T., Given, B., Given, C. W., Ridenour, K., Schueller, M., & Spoelstra, S. L. (2015). mHealth SMS text messaging interventions and to promote medication adherence: an integrative review. Journal of Clinical Nursing, 24(19–20), 2722–2735. https://doi.org/10.1111/jocn.12918.
D’inca, R., Bertomoro, P., Mazzocco, K., Vettorato, M. G., Rumiati, R., & Sturniolo, G. C. (2008). Risk factors for non-adherence to medication in inflammatory bowel disease patients. Alimentary pharmacology & therapeutics, 27(2), 166–172.
Ediger, J. P., Walker, J. R., Graff, L., Lix, L., Clara, I., Rawsthorne, P., & Bernstein, C. N. (2007). Predictors of medication adherence in inflammatory bowel disease. The American Journal of Gastroenterology, 102(7), 1417–1426.
Engel, T., Ungar, B., Ben-Haim, G., Levhar, N., Eliakim, R., & Ben-Horin, S. (2017). Re-phrasing the question: a simple tool for evaluation of adherence to therapy in patients with inflammatory bowel disease. United European Gastroenterology Journal, 5(6), 880–886.
Fjeldsoe, B. S., Marshall, A. L., & Miller, Y. D. (2009). Behavior change interventions delivered by mobile telephone short-message service. American Journal of Preventive Medicine, 36(2), 165–173.
Franklin, V. L., Waller, A., Pagliari, C., & Greene, S. A. (2006). A randomized controlled trial of sweet talk, a text-messaging system to support young people with diabetes. Diabetic Medicine, 23(12), 1332–1338.
Gadkari, A. S., & McHorney, C. A. (2012). Unintentional non-adherence to chronic prescription medications: How unintentional is it really? BMC Health Services Research Published online June 2012. https://doi.org/10.1186/1472-6963-12-98.
Gerber, B. S., Stolley, M. R., Thompson, A. L., Sharp, L. K., & Fitzgibbon, M. L. (2009). Mobile phone text messaging to promote healthy behaviors and weight loss maintenance: a pilot study. Health Informatics Journal, 15(1), 17–25.
Hall, A. K., Cole-Lewis, H., & Bernhardt, J. M. (2015). Mobile text messaging for health: a systematic review of reviews. Annual Review of Public Health, 36, 393–415. https://doi.org/10.1146/annurev-publhealth-031914-122855.
Head, K. J., Noar, S. M., Iannarino, N. T., & Harrington, N. G. (2013). Efficacy of text messaging-based interventions for health promotion: a meta-analysis. Social Science & Medicine, 97, 41–48.
Horne, R., Weinman, J., Barber, N., Elliott, R., Morgan, M. (2005). Concordance, adherence and compliance in medicine taking. In Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO).
Horne, R., Parham, R., Driscoll, R., & Robinson, A. (2009). Patients’ attitudes to medicines and adherence to maintenance treatment in inflammatory bowel disease. Inflammatory Bowel Diseases, 15(6), 837–844.
Kane, S., & Shaya, F. (2008). Medication non-adherence is associated with increased medical health care costs. Digestive. Diseases and Sciences, Published online April 2008, 53, 1020–1024. https://doi.org/10.1007/s10620-007-9968-0.
Keefer, L., Kiebles, J. L., Martinovich, Z., Cohen, E., van Denburg, A., & Barrett, T. A. (2011). Behavioral interventions may prolong remission in patients with inflammatory bowel disease. Behaviour Research and Therapy, 49, 145–150.
Kelly, M., McCarthy, S., & Sahm, L. J. (2014). Knowledge, attitudes and beliefs of patients and carers regarding medication adherence: a review of qualitative literature. European Journal of Clinical Pharmacology, 70(12), 1423–1431.
Lancaster, G. A., Dodd, S., & Williamson, P. R. (2004). Design and analysis of pilot studies: recommendations for good practice. Journal of Evaluation in Clinical Practice, 10(2), 307–312.
Lenti, M. V., & Selinger, C. P. (2016). Patients’ beliefs and concerns about the necessity of long-term therapies are crucial for medication adherence for inflammatory bowel disease. Journal of Crohn’s and Colitis.
Lenti, M. V., & Selinger, C. P. (2017). Medication non-adherence in adult patients affected by inflammatory bowel disease: a critical review and update of the determining factors, consequences and possible interventions. Expert review of gastroenterology & hepatology, 11(3), 215–226.
Lesnovska, K. P., Hjortswang, H., & Börjeson, S. (2010). What do patients need to know? Living with inflammatory bowel disease. Journal of Clinical Nursing, Published online September 2014, 23, 1718–1725. https://doi.org/10.1111/jocn.12321.
Leventhal, H., Diefenbach, M., & Leventhal, E. A. (1992). Illness cognition: using common sense to understand treatment adherence and affect cognition interactions. Cognitive Therapy and Research, 16(2), 143–163.
Morisky, D. E., Green, L. W., & Levine, D. M. (1986). Concurrent and predictive validity of a self-reported measure of medication adherence. Medical Care, 24, 67–74.
Moser, G., Tillinger, W., Sachs, G., Genser, D., Maier-Dobersberger, T., Spies, K., & Gangl, A. (1995). Disease-related worries and concerns: a study on out-patients with inflammatory bowel disease. European Journal of Gastroenterology & Hepatology, 7(9), 853–858.
Neville, R., Greene, A., McLeod, J., Tracy, A., & Surie, J. (2002). Mobile phone text messaging can help young people manage asthma. BMJ, 325, 600.
NHS Choices (2017). Retrieved from: https://www.nhs.uk/conditions/inflammatory-bowel-disease/.
Petrie, J. K., Perry, K., Broadbent, E., & Weinman, J. (2001). A text messaging programme designed to modify patient illness and treatment beliefs improves self-reported adherence to asthma preventer medication. British Journal of Health Psychology, BPS, published online February. https://doi.org/10.1111/j.2044-8287.2011.02033.
Petrie, K. J., Perry, K., Broadbent, E., & Weinman, J. (2012). A text message programme designed to modify patients’ illness and treatment beliefs improves self-reported adherence to asthma preventer medication. British journal of health psychology, 17(1), 74–84.
Tsianou, K., Giannakeas, N., Tsipouras, M. G., Tzallas, A. T., Skamnelos, A., et al. (2017). Accessing patient views about medication in chronic conditions using the beliefs about medicine questionnaire (BMQ): A review study. The Journal of Drug Research and Development, 3(1). https://doi.org/10.16966/2470-1009.130.
Vervloet, M., Linn, A. J., van Weert, J. C. M., de Bakker, D. H., Bouvy, M. L., & Dijk, L. v. (2012, published online April 2012). The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: a systematic review of the literature. Journal of the American Medical Informatics Association, 696–704. https://doi.org/10.1136/amiajnl-2011-000748.
Weinman, J., Petrie, K. J., Moss-Morris, R., & Horne, R. (1996). The illness perception questionnaire: a new method for assessing the cognitive representation of illness. Psychology and Health, 11(3), 431–445.
Acknowledgments
Thank you to all the participants who kindly dedicated their time to take part in this study and the reviewers who offered advice and guidance throughout the duration of the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical standard
All aspects of the research methodology reported have been reviewed and approved by the XX ethics committee. The research proposal was submitted to the ethics committee in accordance with the British Psychological Society Code of Human Research Ethics Framework (BPS 2014).
Ethical Considerations (e.g., IRB information, consent process, if applicable)
There were low risks associated with this study and the measures administrated to the participants. Participants were given a full description of the study outlined within the information sheet and a consent form which was explained and signed prior to the commencement of the study. Participants had the choice to opt out at any time during the 12 weeks or up to the point of write-up, without declaring a reason for withdrawal. Participants were anonymized, and their confidentiality was respected by replacing their names with ID numbers. Any information collated from the research was stored in a secure location, and documents stored on a PC were password-protected. At the end of the 12 weeks, participants were debriefed and offered a chance to read the completed research paper if published. If participants were interested in the outcome of the study, there was an option to have a summary of the results sent out to them via an email request
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Riaz, S., Jones Nielsen, J.D. A Pilot Study of a Text Messaging Intervention to Modify Illness and Medication Beliefs Among Patients Diagnosed with Inflammatory Bowel Disease. J. technol. behav. sci. 4, 42–52 (2019). https://doi.org/10.1007/s41347-018-0083-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41347-018-0083-1