
Abstract
Introduction
This study aimed to contribute to the existing literature by testing whether the same classes of antisocial behavior typically uncovered in the literature would be revealed with the additional information about heterotypic antisocial behavior. We investigated the development of men’s antisocial behavior in its homotypic and heterotypic forms from age 12 to 30 years in a large representative sample.
Material and methods
Data were drawn from the National Longitudinal Study of Adolescent to Adult Health. This study included 3639 male participants from 6 birth cohorts (1977–1982), first assessed in 1995 and followed up to 2008–2009. Homotypic antisocial behavior comprised items that were assessed at every wave, and heterotypic antisocial behavior comprised adolescent- and adult-specific items. Group-based modeling was used to identify classes of antisocial behavior.
Results
Five trajectories were identified: low, life-course-persistent, adolescent-limited, moderate declining, and adult-peak.
Conclusion
By including heterotypic items, we showed that a group whose antisocial behavior is typically identified as emerging in adulthood was already engaging in moderate levels of antisocial behavior in adolescence. The implications of sample characteristics and forms of antisocial behavior for accurate classification are discussed.
Similar content being viewed by others

Introduction
Developmental Trajectories of Antisocial Behavior and Theory
Moffitt’s [28] taxonomic theory of antisocial behavior has inspired a large body of research on heterogeneity among offenders in the etiology and development of their antisocial behavior. Moffitt proposed that life-course-persistent offenders engage in high levels of antisocial behavior starting in childhood and persisting through adulthood. Antisocial behavior in this group is hypothesized to arise from neuropsychological impairments that are exacerbated by exposure to criminogenic environments. In contrast, adolescent-limited offenders display antisocial behavior primarily during adolescence. Their behavior is motivated by the perception that stealing, cheating, rule-breaking, and violence will enable them to acquire desired goods and privileges typically reserved for adults. Although empirical tests of the taxonomy are more consistent with the existence of an adolescent-onset than an adolescent-limited group [6, 39] and challenge etiological distinctions between life-course-persistent and adolescent-onset offenders [16], there is robust empirical support for distinct trajectories of antisocial behavior across the life course [21, 41].
With advances in group-based modeling [31, 32] which can model trajectories of antisocial behavior using longitudinal data, a large number of studies have tested Moffitt’s taxonomic theory [21]. These studies have typically identified between 4 and 7 classes of antisocial behavior trajectories, including the life-course-persistent group, adolescent-limited group, and a low antisocial group. Additional classes have been revealed, including a childhood-limited group who exhibit severe conduct problems in childhood but desist from antisocial behavior by adolescence [1, 19, 37, 38]. Studies using official records have identified a group with an adult-onset offending pattern [13, 48], but evidence is mixed using self-report data. Several studies using population-based samples have identified a late-onset trajectory of offenders whose antisocial behavior starts to accelerate from very low to higher levels in their late teens [7, 9], but others have failed to reveal such a pattern [4, 45]. There are two explanations of adult-onset criminality. One is that individuals who appear to become involved in antisocial behavior as adults were already involved in antisocial behavior in childhood or adolescence, but not at levels that would necessarily be detectable to the juvenile justice system [15, 29]. In contrast, the “late blooming” hypothesis proposes that the adult-onset group is protected by a supportive school and family environment in childhood and adolescence, but that they begin to engage in antisocial behavior as adults when these supports fall away and they face difficulties coping with the social demands and strains of adult roles [44].
Because group-based trajectory modeling typically relies on homotypic forms of antisocial behavior (i.e., behaviors that can be measured in the same way across time), we aim to contribute to the literature by testing whether simultaneously modeling heterotypic forms of antisocial behavior (i.e., behaviors that change in form over time, like truanting from school in adolescence and job absenteeism in adulthood) would influence the trajectories we identified. An accurate picture of developmental heterogeneity in antisocial behavior should take into account both homotypic and heterotypic antisocial behavior. It remains largely unknown whether the inclusion of heterotypic antisocial behavior would alter either the number or the shape of observed trajectories.
Homotypic and Heterotypic Forms of Antisocial Behavior
The distinction between homotypic and heterotypic forms of antisocial behavior captures the fact that some forms of antisocial behavior can be measured in the same way over time (e.g., fighting) whereas other forms of antisocial behavior are substantially more common at some points in development than others. The distinction does not refer to homogeneity or heterogeneity in the kinds of antisocial behavior described in each category. For example, fighting and stealing are considered homotypic antisocial behaviors because they can both be observed from early in childhood into adulthood, but they represent heterogeneous forms of antisocial behavior (i.e., violent versus property-related antisocial behaviors). Homotypic continuity in antisocial behavior reflects the fact that, for example, children who get into physical fights with other children tend to become adults who get into physical fights with other adults [20]. In contrast, heterotypic forms of antisocial behavior describe behaviors that manifest themselves in different ways at different ages. For example, skipping school as an adolescent may reflect the same underlying construct as skipping work as an adult, but these behaviors are measured with different items at different ages. Other behaviors may lack counterparts at earlier or later points in development or may become so uncommon that they are no longer measured. For example, adolescents are unlikely to engage in high rates of check fraud whereas adults are unlikely to engage in acts of graffiti. Typically, adolescent-specific antisocial behaviors are not measured in adulthood, and adult-specific antisocial behaviors are not measured in adolescence in large-scale studies such as the National Longitudinal Survey of Youth and the National Longitudinal Study of Adolescent Health.
Although there is ample evidence for both homotypic and heterotypic continuity in antisocial behavior, trajectory studies are typically conducted with measures of antisocial behavior that can be measured the same way over time (i.e., homotypic antisocial behavior). Including only those items that do not vary with age makes it unclear whether observed trajectories are a true function of age versus measurement bias stemming from omitted items. For example, a model may show that homotypic antisocial behavior has declined from adolescence into adulthood, but the model will fail to capture whether a person is engaging in forms of crime that are typically observed only in adulthood (e.g., committing fraud). Such a model would give a misleading impression of desistance.
Attempts have been made to take into account the heterotypic continuity of antisocial behavior when investigating the heterogeneity in the development of antisocial behavior. Odgers et al. [39] handled this problem by creating age-appropriate items to identify different behaviors as manifestations of the same underlying construct (e.g., truanting from school in adolescence and skipping work in adulthood). The problem inherent in this approach is that some adolescent behaviors do not have adult counterparts and vice versa, and these behaviors are left out the model. Nagin and Tremblay [34] proposed modeling heterotypic continuity with a joint trajectory approach. In order to test the developmental pathway of the covert behavior problems [24, 25], they modeled trajectories of oppositional behavior from age 6 to 15, trajectories of property delinquency from age 11 to 17, and the probability of transitioning from one to the other. Nagin and Tremblay’s approach is ideal for testing the development of specific forms of antisocial behavior that may have different manifestations in childhood versus adolescence, but it is less ideal for identifying developmental patterns of antisocial behavior defined more broadly (e.g., covert and overt forms of antisocial behavior measured simultaneously).
Current Study
We aimed to contribute to the existing literature by testing whether the same classes typically uncovered in the antisocial behavior literature would be revealed with the additional information about heterotypic antisocial behavior. To this end, we used a multiple domain latent class growth analysis to simultaneously model both heterotypic and the development of homotypic antisocial behavior over time. A sequential cohort study design with a large representative sample was employed to investigate how antisocial behaviors change from age 12 to 30 years, which includes the peak period for desistance and persistence.
The National Longitudinal Study of Adolescent to Adult Health (Add Health) offers two methodological advantages. First, the group-based trajectory model is premised on the assumption that the mixing distribution can be well approximated by a few discrete distributions with a limited number of points of support; so, the estimated parameters should stabilize with increasing sample size [12, 22]. Thus, large samples like Add Health are required to generate reliable class numbers and class memberships.
Second, the cohort sequential design of Add Health means that the observation frame extends from early adolescence into adulthood which has implications for the number and the shape of identified trajectories [32]. For example, a quadratic term will best capture the rate of change in antisocial behavior over time, where it is anticipated that antisocial behavior will increase rapidly in adolescence and decline gradually from late adolescence into adulthood (i.e., the age-crime curve). Nevertheless, it is expected that there will be some persistence in antisocial behavior into adulthood. Without any observations in adulthood to capture such persistence, the decline in antisocial behavior may appear to be steeper than it really is. As revealed in Eggleston et al. [14], when a shorter follow-up period was used to estimate trajectories of antisocial behavior, there was indeed a steeper increase and decline, and the peak ages of antisocial behavior were slightly younger as compared to when observations were available later in adulthood. In addition, without observations into adulthood, it is impossible to detect the existence of an adult-onset group as suggested by Eggleston and Laub [13]. Thus, in its large size and lengthy follow-up period, Add Health differs from most studies in the literature that either follow large samples over a relatively narrow span of the life course [8, 11] or that follow small samples over a relatively long span [3, 41].
The current study only included male participants for three reasons. First, men, on average, engage in more antisocial behavior than women, and there has been a long tradition of studying men’s antisocial behavior because of its significant cost to society [21, 26, 35, 43]. Second, although Odgers et al. [39] found support for measurement invariance of antisocial behavior across ages 6 to 26 years for males, they did not find such support for females. Thus, for females, antisocial behaviors measured in adolescence carried a different meaning from the same items measured in adulthood. Last, despite the increasing number of studies examining trajectories of females’ antisocial behavior [5, 10, 39], there is a much larger body of research on trajectories of men’s antisocial behavior. Because we hypothesized that the inclusion of heterotypic forms of antisocial behavior would alter our understanding of the development of antisocial behavior, we restricted our investigation to male participants to enable a clear comparison with previous findings about male’s trajectories of antisocial behavior.
Method
Sample
Participants were drawn from the in-home interview sample of the Add Health. The Add Health project was approved by the Non-Biomedical IRB division of the Office of Human Research Ethics at the University of North Carolina at Chapel Hill. Add Health is a longitudinal study of a nationally representative sample of adolescents from the USA who were in grades 7 through 12 in 1994–1995 when the study began. The Add Health study originally comprised 90,118 adolescents who were selected via a stratified, random school selection procedure. Adolescents were selected for the longitudinal in-home interview subsample via a multistage, stratified, school-based, cluster sampling design and have been interviewed at four waves, most recently in 2008–2009. The wave 1 in-home interview sample comprised 20,745 12- to 18-year olds (78.9 % response rate of all eligible participants). Wave 2 in-home interviewing was conducted in 1996 (88.2 % response rate with a resulting sample size of 15,197; with 12th graders from wave 1 excluded from wave 2, but included at subsequent waves). Wave 3 was conducted in 2001–2002 (77.4 % response rate with a resulting sample size of 15,197), and wave 4 was conducted in 2008–2009 (80.3 % response rate with a resulting sample size of 15,701), at which point participants were 24 to 32 years old.
Add Health has a sequential cohort (or accelerated) study design, with up to four waves of data for 10 birth cohorts (born between 1974 and 1983). For example, participants born in the 1982 cohort were 13 years old at wave 1 of the study and 26 years old at wave 4. Note that participants were asked whether they engaged in various antisocial behaviors in the past 12 months. Thus, participants who were 13 years old when data were collected were reporting on their antisocial behavior when they were 12 years old (see Fig. 1 upper panel). Assuming that cohort effects on the developmental trajectories are minimal, the design can model developmental trajectories over a relatively wide age range instead of modeling trajectories with only four time points reflecting the four waves of the study (see Analytic plan for tests of cohort effects). We included six birth cohorts (born between 1977 and 1982; cohort size ranged from 898 to 2056) and excluded four that were so small as to be nonrepresentative (e.g., cohort sizes ranged from 6 to 277). Only male participants from the six birth cohorts who had complete data were retained in the final analysis (N = 3639) (Fig. 2).

Modeling heterogeneity of antisocial behavior development from age 12 to age 30 with sequential cohort study design, extending semiparametric Poisson mixture models (SPMM) by simultaneously modeling the influence of adolescent- and adult-specific heterotypic antisocial behavior on class membership. The shape of the trajectory of homotypic antisocial behavior from age 12 to age 30 is determined by the latent factors of the intercept at age 12, linear and quadratic change in antisocial behavior as a function of age. Heterotypic antisocial behavior is represented by adolescent- and adult-specific scores. Homotypic and heterotypic antisocial behavior are conditional on class membership. Note. ASB = antisocial behavior. Participants were asked whether they engaged in various antisocial behaviors in the past 12 months; therefore, for participants that were 13 years at the time of data collection, they were reporting their antisocial behavior for when they were 12 years

Flow chart of retaining participants for final analysis
The final sample included participants who self-identified as White (N = 2,044), African American (N = 606), Hispanic (N = 521), Native American (N = 17), Asian American (N = 236), multiracial (N = 185), and other ethnicities (N = 30). The median income reported by parents at wave 1 was 40.00 thousand dollars (mean = 47.97; SD = 47.98). Individuals excluded from the final analysis (N = 628; either from the small cohorts or with missing data on antisocial behavior) had a lower household income (M = 42.25; SD = 45.77) than the retained sample (t = −2.46, p = .014). The two groups did not differ in their self-control, social support, self-esteem level, or the percentage of parents that were married. The excluded differed from the retained in their ethnicity makeup (χ2 = 16.75, df = 6, p = .01), and White participants were disproportionately represented among those who were excluded from the sample.
Measures
Homotypic Antisocial Behavior
At every wave of the study, participants were asked whether they engaged in various antisocial behaviors in the past 12 months. Nine of these antisocial behavior items were measured at all four waves. We define these as “homotypic” antisocial behavior items. These items assessed property-related and violent antisocial behaviors, including deliberately damaging another person’s property, stealing items worth more than (or less than) $50, selling marijuana or other drugs, going into a house or building to steal things, using or threatening to use a weapon to get things from others, pulling a knife or gun on someone, taking part in a group (e.g., gang) fight, and shooting or stabbing someone. The items were dichotomously scored to indicate whether the respondent had ever engaged in that behavior and then summed to reflect how many types of antisocial behaviors the respondent had committed. Every participant had one homotypic antisocial behavior count score at each wave, for a total of four scores across all waves of the study. Descriptive statistics for homotypic antisocial behavior at each age are reported in Table 1.
Heterotypic Antisocial Behavior
Beyond the 9 items assessed at each wave, additional antisocial behavior items were assessed at some waves, but not others. We define these as “heterotypic” antisocial behavior items. For example, at waves 1 and 2, adolescents were asked about truancy from school, but by waves 3 and 4, these items were not included, presumably because respondents were no longer in school. In contrast, questions about white collar crime were assessed at waves 3 and 4, but not at earlier waves. We constructed an adolescent-specific heterotypic antisocial behavior score comprising 6 items measured at waves 1 and 2 (painting graffiti or signs on other’s property or in a public place; lying to parents or guardians about where they had been or whom they were with; taking something from a store without paying for it; running away from home; driving a car without the owner’s permission; being loud, rowdy, or unruly in a public place). We also constructed an adult-specific measure comprising 3 items measured at waves 3 and 4 (buying, selling, or holding stolen property; using another’s credit card, bank card, or automatic teller card without permission or knowledge; deliberately writing a bad check). Adolescent- and adult-specific items were dichotomously scored to indicate whether the respondent had ever engaged in those behaviors in the past 12 months and summed to form adolescent- and adult-specific total scores. Descriptive statistics for heterotypic antisocial behavior are reported in Table 1.
Covariates
Covariates were included to determine whether they varied as a function of class. Covariates included demographics measures at wave 1 such as participants’ ethnicity (coded as White, African American, Hispanic, Asian, multiracial, and others), whether their parents were married, and the household income. At wave 1, participants also reported on their feelings of caring, support, and understanding from parents, teachers, and friends or other adults (1 = not at all; 5 = very much) with 7 items which were then summed to form a total score indicating level of social support (α = .77). Self-esteem was assessed with 4 items at wave 1 about how much they were satisfied with themselves as a person (1 = strongly disagree; 5 = strongly agree) and then summed to form total scores (α = .78). Last, a self-control measure was included as a covariate. Consistent with the concept proposed by Gottfredson and Hirshi [17], (low) self-control was defined as being impulsive (e.g., tending to act before thinking through the consequences of one’s actions). Although a self-control questionnaire was not administered in Add Health, seven items were assessed that capture aspects of self-control at wave 1[27]. Participants were asked how much they agreed (1 = strongly agree; 5 = strongly disagree) with 4 statements: (a) when you have a problem to solve one of the first things you do is to get as many facts about the problem as possible; (b) when you are attempting to find a solution to a problem you usually try to think of as many different way to approach the problem as possible; (c) when making decisions you generally use a systematic method for judging and comparing alternatives; and (d) after carrying out a solution to a problem you usually try to analyze what went right and what went wrong. In addition, participants were asked how often in the past year they had trouble paying attention in school, getting homework done, and keeping your mind on what you were doing. All seven items were reversed coded, z-transformed, and then summed to form a composite score, with higher scores reflecting higher levels of self-control (α = .70). This self-control measure was previously found to have a good convergent validity in the Add Health study (see [27]).
Procedure
All participants received the same interview, which was 1 to 2 h long depending on the participant’s age and experiences. The majority of interviews were conducted in participants’ homes. To protect confidentiality, no paper questionnaires were used. Instead, all data were recorded on laptop computers. For less sensitive topics, the interviewer read the questions aloud and entered the participant’s answers. For more sensitive topics, the participants listened through earphones to prerecorded questions and entered the answers directly. In addition to maintaining data security, this minimized the potential for interviewer or parental influence.
Analysis Plan
We modeled simultaneously heterogeneity in developmental trajectories of homotypic antisocial behavior and in heterotypic antisocial behavior from age 12 to age 30. Analyses were conducted in Mplus 6 (Muthén and Muthén 1998–2012) using maximum likelihood estimation with robust standard errors and incorporated sampling weights which adjusted for the stratified and clustered sampling design of Add Health and also adjusted for differential response and attrition rates over time.
To estimate heterogeneity in antisocial behavior development, we estimated a series of latent class growth analyses (LCGA). LCGA is a person-centered analysis premised on the assumption that there are unobserved but distinct groups of individuals who follow similar developmental trajectories [31]. LCG models estimate a different mean growth curve for each class. Within-class variation in growth factors is not allowed. The homotypic and heterotypic antisocial behavior scores are count variables that are assumed to have a Poisson distribution. The current model extends semiparametric Poisson mixture models (SPMM) [23, 33] by simultaneously modeling the influence of adolescent- and adult-specific heterotypic antisocial behavior on class membership. Thus, classes were derived from five elements: three latent factors representing development in homotypic antisocial behavior (initial level, linear, and quadratic change in antisocial behavior as a function of age) and two indicators of heterotypic antisocial behavior (adolescent-specific and adult-specific) (Fig. 1). We first tested unconditional models with Eq. (1):
where \( {\lambda}_{i{t}_{homotypic}}^j \) is the individual i’s rate of homotypic antisocial behavior at time t conditional on membership in class j, and Age it is the individual i’s age at time t. The coefficients β j0 , β j1 , and β j2 determine the shape of the trajectory and the superscript j denotes that the coefficients differ across classes, which allows each class to have a distinct trajectory. We centered age at 13 years, so that the rate of homotypic antisocial behavior at age 12 is \( {e}^{{\boldsymbol{\beta}}_0^{\boldsymbol{j}}} \). The heterotypic antisocial behaviors are modeled by Eqs. 1.2 and 1.3, where λ j i_teen and λ j i_adult are the individual i’s rates of adolescent- and adult-specific antisocial behavior conditional on membership in class j, both β j3 and β j4 are superscripted by j to denote that the estimates are different across classes.
We tested a series of unconditional models to determine the optimal class number. Bayesian information criterion (BIC), Lo-Mendell-Rubin likelihood ratio test (LMR-LRT), parsimony, and the meaningfulness of class were all taken into account [31, 32, 36]. Note that although a simulation study revealed that the Bootstrap likelihood ratio test performed the best, it cannot currently accommodate complex survey data [36], and Add Health data has a multistage, stratified, school-based, cluster sampling design. A significant LMR-LRT and a smaller BIC indicate a good fit of the model. After classes were identified, we examined basic characteristics of each class in terms of their demographics and levels of related constructs (see “Covariates” section).
The current study assumed that the cohort effects on the developmental trajectories are minimal, so that the design can model developmental trajectories over a relatively wide age range (i.e., age 12 to 30) instead of modeling trajectories with only four time points reflecting the four waves of the study. To test for cohort effects, we conducted a conditional growth curve analysis with cohort status (represented as 5 dummy variables with the oldest cohort as the reference category) as a predictor of the intercept, linear, and quadratic change in the antisocial behavior development from age 12 to age 30. Because chi-square test is sensitive to large sample size, we inspected coefficient parameters rather than relying on the chi-square statistic. Given the number of coefficients (i.e., 5 cohorts generated 15 parameters in total for intercept, linear, and quadratic slopes) and the increasing chance of type I error, we used a corrected α level of .003 for coefficient inspection. Results revealed no significant cohort effects for intercept (p = .37, .85, .27, .08, .03 for cohort 1978, 1979, 1980, 1981, and 1982), linear slope (p = .37, .88, .40, .03, .006 for cohort 1978, 1979, 1980, 1981, and 1982), or quadratic slope (p = .38, .92, .63, .03, and .004 for cohort 1978, 1979, 1980, 1981, and 1982). All p values were above the corrected α level, although these stringent corrections may have overlooked real differences between the oldest (1977) and youngest (1982) cohorts. Generally, however, cohort effects on growth trajectory parameters appear to be minimal. Although it would be optimal to test for cohort effects in a growth model with more than one class, such a model would not converge due to the large number of parameters being estimated.
Results
Our aim was to identify the optimal number of classes to capture developmental heterogeneity in antisocial behavior. In the Add Health data, the BIC continued to decrease as the number of classes increased. The LMR-LRT remained significant until we increased the class number to six, suggesting that the six-class solution did not improve the model fit in a significant way as compared to the five-class solution (see Table 2). In addition, for the six-class solution, the smallest class comprised only 2.00 %, or 73 out of 3639 participants. This small group might not constitute a meaningful class in a practical sense. The optimal class number appears to be five. We labeled the five classes as “low,” “moderate declining,” “life-course-persistent,” and “adolescent-limited,” and “adult-peak.” Developments in the homotypic antisocial behavior and in the heterotypic antisocial behavior for each class are presented in Table 3 and plotted in Fig. 3. These five classes differed in their self-control level, self-esteem, and social support during adolescence. Although they did not differ with respect to household income at the first wave of the study, they did differ with respect to parents’ marital status and race/ethnicity. Mean and standard deviation of covariates by class membership are reported in Table 4.

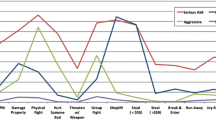
Five-class solution for multiple domain latent class growth analysis. a Estimated rates for homotypic antisocial behavior from age 12 to 30 years. b Estimated rates for adolescent- and adult-specific heterotypic antisocial behavior
The low class comprised individuals who displayed little or no antisocial behavior, as revealed by a virtually zero count of homotypic antisocial behavior and adult-specific antisocial behavior. This class engaged in some adolescent-specific antisocial behavior, but they had the lowest count among all five groups. The low class scored among the highest on self-esteem, social support, and self-control.
Individuals in the life-course-persistent class had a very high rate of homotypic antisocial behavior at age 12 and remained relatively high across time. They also exhibited very high levels of adolescent-specific antisocial behavior and the highest levels of adult-specific antisocial behavior compared with the other classes. Overall, they scored among the lowest on self-esteem, social support, and self-control.
Individuals in the moderate declining class engaged in moderate levels of homotypic and heterotypic antisocial behavior in early adolescence, but their antisocial behavior declined over time. Individuals in the moderate declining class scored among the average on their self-esteem, social support, and self-control as compared to the other four classes.
We identified a class characterized as adolescent-limited that displayed very high levels of homotypic and heterotypic antisocial behavior during adolescence. By the time they were in their early twenties, they engaged in as little homotypic and heterotypic antisocial behavior as the low class. The adolescent-limited class had similarly low scores on the self-control and social support measures as the life-course-persistent class and they had the lowest scores on the self-esteem measures.
Individuals in the adult-peak class engaged in very low levels of homotypic antisocial behavior at age 12. However, their homotypic antisocial behavior gradually increased, peaked by their mid-twenties, and then gradually declined, reaching the same rate as the life-course-persistent class. Furthermore, they engaged in nearly as much adult-specific antisocial behavior as the life-course-persistent class. Although this class engaged in relatively low levels of homotypic antisocial behavior in adolescence, they engaged in almost twice as much adolescent-specific antisocial behavior as the low class. They had much higher scores on self-esteem, social support, and self-control than the moderate-declining, the adolescent-limited, and the life-course-persistent class. Their self-control and social support scores were the second-highest, and their self-esteem score was as high as the low class.
In sum, by modeling both heterotypic and homotypic antisocial behavior, we identified many of the same classes as other studies have, with the exception of the adult-peak class. Although homotypic antisocial behaviors emerged in adulthood in this group, they were already engaging in heterotypic antisocial behavior at a relatively high rate during adolescence. Thus, without modeling both heterotypic and homotypic antisocial behaviors, this group would look like it had an adult onset of antisocial behavior.
Discussion
The current study examined the development of antisocial behavior in its homotypic and heterotypic forms from age 12 to 30 years in a large representative sample. With one exception, the inclusion of heterotypic as well homotypic forms of antisocial behavior made relatively little difference to the number, shape, or interpretation of identified trajectories. That is, like many other groups, we identified low, life-course-persistent, and adolescent-limited groups [21, 41]. We also identified a moderate declining group which is similar to the childhood-limited group identified in other studies [39, 42], though the Add Health study did not have data extending back to early or middle childhood.
Where it mattered to have simultaneously modeled homotypic and heterotypic forms of antisocial behavior was in the identification of the adult-peak group. Focusing solely on homotypic forms of antisocial behavior, this group appeared to have an adult onset of antisocial behavior. In reality, however, this group was already engaging in moderate levels of adolescent-specific antisocial behaviors prior to adulthood, including painting graffiti in a public place and running away from home. For example, although males in this group engaged in just over .5 homotypic antisocial behaviors per year when they were 15 years old, they engaged in adolescent-specific antisocial behaviors at approximately 3 times that rate (i.e., 1.5). Thus, previous studies that have identified an adult-onset group may be unintentionally misrepresenting the actual onset of antisocial behavior if they have not modeled behaviors that are prevalent in adolescence, but not in adulthood. For example, some studies that have identified an adult-onset group only used official records, and sometimes only with records from age 18 onward [13, 18]. It is possible that individuals in this group lack a juvenile record, but were in fact committing minor forms of antisocial behavior such as running away from home or truanting from school at a relatively high rate.
Although our data provided some support for the hypothesis that individuals who appear to have an adult-onset of antisocial behavior are already engaging in some forms of antisocial behavior in adolescence, our data were potentially consistent with the late-blooming hypothesis as well. As seen from Table 4, the adult-peak class had self-esteem and social support scores that were close to those of the low class, suggesting that a supportive environment during childhood and adolescence might have been preventing them from engaging in even higher rates of antisocial behavior in adolescence [44, 46]. Additional data would be needed to test the hypothesis that this group was having a difficult time making a successful transition to adulthood.
The large size of the Add Health sample enabled us to differentiate groups that might otherwise have been combined in smaller samples. Moffitt’s [28] theory of developmental heterogeneity in antisocial behavior predicted the existence of an adolescence-limited group that would engage in high levels of delinquency starting in adolescence and would desist by young adulthood. Given little empirical evidence of desistance by young adulthood, this group was later redefined as an adolescent-onset group in revisions to the theory [39]. We argue that the large sample size of Add Health allowed us to (a) identify an adolescent-limited group consistent with the original theory and (b) potentially explain why this group is more often identified as adolescent-onset in smaller samples. That is, the large sample size of Add Health allowed us to differentiate two groups: one with a rapid rising speed and a very high peak at age 17 years (i.e., adolescent-limited) and another with a slow rising speed and a peak at mid-20s (i.e., adult-peak). In a smaller sample with less power to differentiate trajectories of antisocial behavior, these two groups would likely be combined into an adolescent-onset class. Consistent with this possibility, the adolescent-limited and adult-peak groups together in our study comprised 19 % of the males, similar to the 19 % of the population which was classified into the adolescent-onset group [39].
The relatively large number of trajectories identified in our study might have resulted from the use of self-reported measures of antisocial behavior as well as the large sample size. In contrast to criminal records which tend to capture the most severe forms of antisocial behavior, self-reported antisocial behavior measures capture relatively minor as well as more severe offenses. As a result, measures of self-reported antisocial behavior usually have greater variability than measures of antisocial behavior based on official records. Because of this increased variability, more trajectories are typically detected in studies of self-reported antisocial behavior versus studies of antisocial behavior based on official records [21].
The current study is descriptive in nature, but it is informative to risk assessment and prevention. The accurate identification of trajectories contributes to precise classification, which in turn would lead to better practice in risk assessment and focused intervention. Future research should focus more on identification of group-specific risk factors. The distinct developmental trajectories in antisocial behavior suggest that different preventative interventions may be necessary at different points in the life course. There are two potential time windows for effective intervention. The first one is early childhood. Early childhood intervention would be particularly important for the life-course-persistent group. Studies have shown that the life-course-persistent group is characterized by neurodevelopmental risk factors (e.g., reading difficulty, low IQ) that differentiate them from the adolescent-onset group and that might serve as effective targets of intervention [30, 29, 39]. More research is needed, however, to uncover factors that differentiate the life-course-persistent from the childhood-limited group because limited resources may not be well spent on intervening with the latter group if they will desist from antisocial behavior by the time they reach adolescence anyway. Few studies have attempted to differentiate these groups. Such studies have shown that parent and family characteristics like maternal anxiety during pregnancy, partner cruelty to the mother in the early childhood period, harsh parenting [2], and family history of psychiatric disorder [38] are more characteristic of early-onset persistent conduct problems versus childhood-limited conduct problems. In addition, life-course-persistent youth have been shown to have lower scores on measures of social competence, including socioemotional competence and pragmatic language ability [40]. Thus, although the findings require replication, childhood interventions may be most effectively targeted at youth who are engaging in high levels of conduct problems and whose families are characterized by high rates of harsh verbal and physical discipline as well as adult domestic violence and may involve efforts to improve social and emotional competencies.
The other time window for effective intervention is late adolescence with a focus on the adult-peak group. Because the adult-peak group is responsible for half of the antisocial behavior observed in the population in adulthood, it is important to identify factors that cause them to escalate from relatively minor, adolescent-specific antisocial behaviors to more serious adult antisocial behaviors and to devise prevention efforts that target these factors [48]. Much less is known about factors that differentiate the adult-peak group from other trajectories. One possibility is that the adult-peak group is characterized by higher rates of internalizing problems relative to the those who are on an early-onset persistent trajectory [46, 47]. If the findings on internalizing problems are consistently associated with adult-peak group, we may be particularly concerned with adolescents who are engaging in relatively high rates of adolescent-specific antisocial behavior and who also have high levels of anxiety and depressive symptoms.
Limitations
The findings of the current study should be considered in light of three limitations. First, the youngest age at which antisocial behavior was first measured in the Add Health respondents included in our analyses was 12 years. Thus, the observed trajectories did not capture childhood-onset antisocial behavior although we surmise that the moderate declining class is equivalent to the childhood-limited class identified in previous research [1, 39]. Second, because of a lack of prospective or retrospective data on respondents’ childhood environments or individual characteristics in childhood, we could not test whether the five trajectories were etiologically distinct.
Third, because we only included individuals who had nonmissing data on our antisocial behavior measures, we did not account for those who were incarcerated or who were not assessed across all four waves in the study. Thus, our life-course-persistent group may not have included individuals who were involved in frequent, severe, and chronic antisocial behavior (although presumably it would have included those who had managed to evade detection or sentencing in the criminal justice system). This could explain why the group we identified as “life-course-persistent” was engaging in fairly modest levels of antisocial behavior by the time they were in their late twenties and early thirties, although rates of antisocial behavior in this group were still high relative to other groups. It is worth noting that population-based samples like Add Health and samples of criminal offenders or other high-risk groups provide different kinds of information. On the one hand, high-risk samples can elucidate patterns of severe antisocial behavior over time, and may therefore be informative about the types of antisocial behavior that carry the greatest costs to society. On the other hand, population-based samples are necessary to understand heterogeneity in the development of antisocial behavior and the population composition. For instance, although a sample of high-risk offenders could be assumed to include many individuals who follow a life-course-persistent trajectory of antisocial behavior, such a sample would not be informative about the prevalence of life-course-persistent antisocial behavior in the population. Moreover, individuals who engage in moderate levels of antisocial behavior, such as the adolescent-limited or childhood-limited group, may not be identified in the high-risk samples; yet, they contribute to our understanding of the development of antisocial behavior. Accurate identification of these groups is needed before researchers can further investigate precursors and outcomes of different trajectories.
Conclusion
Despite these limitations, our data shed light on patterns of antisocial behavior that have not previously been revealed. Although the inclusion of heterotypic as well as homotypic forms of antisocial behavior made little difference to the trajectories that have typically been identified in longitudinal research, accounting for adolescent- and adult-specific antisocial behaviors did clarify behavior in a group that has sometimes (and controversially) been identified as initiating antisocial behavior in adulthood. Our findings underscore the importance of modeling heterogeneity in large, population-based samples observed over suitably long periods of time for purposes of accurate classification. Accurate identification of groups will improve chances that researchers will successfully identify etiological differences across groups as well as factors that promote desistance.
References
Aguilar, B., Sroufe, L. A., Egeland, B., & Carlson, E. (2000). Distinguishing the early-onset/persistent and adolescence-onset antisocial behavior types: From birth to 16 years. Development and Psychopathology, null(02):109–132.
Barker, E. D., & Maughan, B. (2009). Differentiating early-onset persistent versus childhood-limited conduct problem youth. The American Journal of Psychiatry, 166(8), 900–908. doi:10.1176/appi.ajp.2009.08121770.
Bersani, B. E., Nieuwbeerta, P., & Laub, J. H. (2009). Predicting trajectories of offending over the life course: findings from a Dutch Conviction Cohort. Journal of Research in Crime and Delinquency, 46(4), 468–494. doi:10.1177/0022427809341939.
Blokland, A. A. J., & Nieuwbeerta, P. (2005). The effects of life circumstances on longitudinal trajectories of offending*. Criminology, 43(4), 1203–1240. doi:10.1111/j.1745-9125.2005.00037.x.
Brennan, L., & Shaw, D. (2013). Revisiting data related to the age of onset and developmental course of female conduct problems. Clinical Child & Family Psychology Review, 16(1), 35–58. doi:10.1007/s10567-012-0125-8.
Brennan, P. A., Hall, J., Bor, W., Najman, J. M., & Williams, G. (2003). Integrating biological and social processes in relation to early-onset persistent aggression in boys and girls. Developmental Psychology, 39(2), 309–323. doi:10.1037/0012-1649.39.2.309.
Bushway, S. D., Thornberry, T. P., & Krohn, M. D. (2003). Desistance as a developmental process: a comparison of static and dynamic approaches. Journal of Quantitative Criminology, 19(2), 129–153.
Campbell, S. B., Spieker, S., Vandergrift, N., Belsky, J., & Burchinal, M. (2010). Predictors and sequelae of trajectories of physical aggression in school-age boys and girls. Development and Psychopathology, 22(01), 133–150. doi:10.1017/S0954579409990319.
Chung, I.-J., Hill, K. G., Hawkins, J. D., Gilchrist, L. D., & Nagin, D. S. (2002). Childhood predictors of offense trajectories. Journal of Research in Crime and Delinquency, 39(1), 60–90. doi:10.1177/002242780203900103.
Cohen, M. A., Piquero, A. R., & Jennings, W. G. (2010). Monetary costs of gender and ethnicity disaggregated group-based offending. American Journal of Criminal Justice, 35(3), 159–172. doi:10.1007/s12103-010-9071-5.
Côté, S., Vaillancourt, T., LeBlanc, J. C., Nagin, D. S., & Tremblay, R. E. (2006). The development of physical aggression from toddlerhood to pre-adolescence: a nation wide longitudinal study of Canadian children. Journal of Abnormal Child Psychology, 34(1), 68–82. doi:10.1007/s10802-005-9001-z.
D’Unger, A., Land, K. C., McCall, P. L., & Nagin, D. S. (1998). How many latent classes of delinquent/criminal careers? results from mixed poisson regression analyses. American Journal of Sociology, 103(6), 1593–1630. doi:10.1086/231402.
Eggleston, E. P., & Laub, J. H. (2002). The onset of adult offending: A neglected dimension of the criminal career. Journal of Criminal Justice, 30(6), 603–622. doi:10.1016/S0047-2352(02)00193-9.
Eggleston, E. P., Laub, J. H., & Sampson, R. J. (2004). Methodological sensitivities to latent class analysis of long-term criminal trajectories. Journal of Quantitative Criminology, 20(1), 1–26.
Elander, J., Rutter, M., Simonoff, E., & Pickles, A. (2000). Explanations for apparent late onset criminality in a high-risk sample of children followed up in adult life. British Journal of Criminology, 40(3), 497–509. doi:10.1093/bjc/40.3.497.
Fairchild, G., van Goozen, S. H. M., Calder, A. J., & Goodyer, I. M. (2013). Research review: evaluating and reformulating the developmental taxonomic theory of antisocial behaviour. Journal of Child Psychology and Psychiatry, 54(9), 924–940. doi:10.1111/jcpp.12102.
Gottfredson, M., & Hirshi, T. (1990). A general theory of crime. Stanford: Stanford University Press.
Gomez-Smith, Z., & Piquero, A. R. (2005). An examination of adult onset offending. Journal of Criminal Justice, 33(6), 515–525. doi:10.1016/j.jcrimjus.2005.08.001.
Huesmann, L. R., Dubow, E. F., & Boxer, P. (2009). Continuity of aggression from childhood to early adulthood as a predictor of life outcomes: implications for the adolescent-limited and life-course-persistent models. Aggressive Behavior, 35(2), 136–149. doi:10.1002/ab.20300.
Huesmann, L. R., Eron, L. D., Lefkowitz, M. M., & Walder, L. O. (1984). The stability of aggression over time and generations. Retrieved from http://deepblue.lib.umich.edu/handle/2027.42/83380
Jennings, W. G., & Reingle, J. M. (2012). On the number and shape of developmental/life-course violence, aggression, and delinquency trajectories: A state-of-the-art review. Journal of Criminal Justice, 40(6), 472–489. doi:10.1016/j.jcrimjus.2012.07.001.
Kiefer, J., & Wolfowitz, J. (1956). Consistency of the maximum likelihood estimator in the presence of infinitely many incidental parameters. The Annals of Mathematical Statistics, 27(4), 887–906. doi:10.1214/aoms/1177728066.
Land, K. C., McCall, P. L., & Nagin, D. S. (1996). A comparison of poisson, negative binomial, and semiparametric mixed poisson regression models with empirical applications to criminal careers data. Sociological Methods & Research, 24(4), 387–442. doi:10.1177/0049124196024004001.
Loeber, R. (1991). Antisocial behavior: more enduring than changeable? Journal of the American Academy of Child & Adolescent Psychiatry, 30(3), 393–397. doi:10.1097/00004583-199105000-00007.
Loeber, R., Wung, P., Keenan, K., Giroux, B., Stouthamerloeber, M., Vankammen, W., & Maughan, B. (1993). Developmental pathways in disruptive child-behavior. Development and Psychopathology, 5(1–2), 103–133. doi:10.1017/S0954579400004296.
Maldonado-Molina, M. M., Jennings, W. G., & Komro, K. A. (2009). Effects of alcohol on trajectories of physical aggression among urban youth: an application of latent trajectory modeling. Journal of Youth and Adolescence, 39(9), 1012–1026. doi:10.1007/s10964-009-9484-y.
McGloin, J. M., & Shermer, L. O. (2009). Self-control and deviant peer network structure. Journal of Research in Crime and Delinquency, 46(1), 35–72. doi:10.1177/0022427808326585.
Moffitt, T. E. (1993). Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychological Review, 100(4), 674–701. doi:10.1037/0033-295X.100.4.674.
Moffitt, T. E. (2006). A review of research on the taxonomy of life course persistent versus adolescent-limited antisocial behavior. In F. T. Cullen, J. P. Wright, & K. R. Blevins (Eds.), Taking stock: the status of criminological theory (advances in criminological theory) (Vol. 15, pp. 277–311). New Brunswick: Transaction.
Moffitt, T. E., Caspi, A., Rutter, M., & Silva, P. A. (2001). Sex differences in antisocial behaviour: conduct disorder, delinquency, and violence in the dunedin longitudinal study. Cambridge: Cambridge University Press.
Muthén, B., & Muthén, L. K. (2000). Integrating person-centered and variable-centered analyses: growth mixture modeling with latent trajectory classes. Alcoholism, Clinical and Experimental Research, 24(6), 882–891. doi:10.1111/j.1530-0277.2000.tb02070.x.
Nagin, D. S. (2005). Group-based modeling of development. Cambridge: Harvard University Press.
Nagin, D. S., & Land, K. C. (1993). Age, criminal careers, and population heterogeneity: specification and estimation of a nonparametric, mixed poisson model. Criminology, 31, 327.
Nagin, D. S., & Tremblay, R. E. (2001). Analyzing developmental trajectories of distinct but related behaviors: a group-based method. Psychological Methods, 6(1), 18–34. doi:10.1037/1082-989X.6.1.18.
Nagin, D., & Tremblay, R. E. (1999). Trajectories of boys’ physical aggression, opposition, and hyperactivity on the path to… Child Development 70(5):1181
Nylund, K. L., Asparouhov, T., & Muthen, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: a monte carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569.
Odgers, C. L., Caspi, A., Broadbent, J. M., Dickson, N., Hancox, R. J., Harrington, H., & Moffitt, T. E. (2007). Prediction of differential adult health burden by conduct problem subtypes in males. Archives of General Psychiatry, 64(4), 476–484. doi:10.1001/archpsyc.64.4.476.
Odgers, C. L., Milne, B. J., Caspi, A., Crump, R., Poulton, R., & Moffitt, T. E. (2007). Predicting prognosis for the conduct-problem boy: can family history help? Journal of the American Academy of Child & Adolescent Psychiatry, 46(10), 1240–1249. doi:10.1097/chi.0b013e31813c6c8d.
Odgers, C. L., Moffitt, T. E., Broadbent, J. M., Dickson, N., Hancox, R. J., Harrington, H., & Caspi, A. (2008). Female and male antisocial trajectories: From childhood origins to adult outcomes. Development and Psychopathology, 20(02), 673–716. doi:10.1017/S0954579408000333.
Oliver, B. R., Barker, E. D., Mandy, W. P. L., Skuse, D. H., & Maughan, B. (2011). Social cognition and conduct problems: a developmental approach. Journal of the American Academy of Child & Adolescent Psychiatry, 50(4), 385–394. doi:10.1016/j.jaac.2011.01.006.
Piquero, A. R., Farrington, D. P., Nagin, D. S., & Moffitt, T. E. (2010). Trajectories of offending and their relation to life failure in late middle age: findings from the cambridge study in delinquent development. Journal of Research in Crime and Delinquency, 47(2), 151–173. doi:10.1177/0022427809357713.
Russell, M. A., Robins, S. J., & Odgers, C. L. (2014). Developmental perspectives: sex differences in antisocial behavior from childhood to adulthood. In R. Gartner & B. McCarthy (Eds.), The Oxford handbook of gender, sex, and crime (pp. 286–315). New York: Oxford University Press.
Sampson, R. J., & Laub, J. H. (2003). Life-course desisters? Trajectories of crime among delinquent boys followed to age 70*. Criminology, 41(3), 555–592. doi:10.1111/j.1745-9125.2003.tb00997.x.
Thornberry, T. P., & Krohn, M. D. (2005). Applying interactional theory to the explanation of continuity and change in antisocial behavior. In D. P. Farrington (Ed.), Integrated developmental and life-course theories of offending (advances in criminological theory) (Vol. 14, pp. 183–209). New Brunswick: Transaction.
Wiesner, M., & Capaldi, D. M. (2003). Relations of childhood and adolescent factors to offending trajectories of young men. Journal of Research in Crime and Delinquency, 40(3), 231–262. doi:10.1177/0022427803253802.
Zara, G., & Farrington, D. P. (2009). Childhood and adolescent predictors of late onset criminal careers. Journal of Youth and Adolescence, 38(3), 287–300. doi:10.1007/s10964-008-9350-3.
Zara, G., & Farrington, D. P. (2010). A longitudinal analysis of early risk factors for adult-onset offending: What predicts a delayed criminal career? Criminal Behaviour and Mental Health: CBMH, 20(4), 257–273. doi:10.1002/cbm.763.
Zara, G., & Farrington, D. P. (2013). Assessment of risk for juvenile compared with adult criminal onset implications for policy, prevention, and intervention. Psychology, Public Policy, and Law, 19(2), 235–249. doi:10.1037/a0029050.
Acknowledgments
We thank John MacDonald for his valuable comments on an earlier draft of this paper. This research was supported by a grant from the William T. Grant Foundation (grant 10909) to SRJ. This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chen, F.R., Jaffee, S.R. The Heterogeneity in the Development of Homotypic and Heterotypic Antisocial Behavior. J Dev Life Course Criminology 1, 269–288 (2015). https://doi.org/10.1007/s40865-015-0012-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40865-015-0012-3