
Abstract
Depression is a multifactorial disease with unknown etiology affecting globally. It’s the second most significant reason for infirmity in 2020, affecting about 50 million people worldwide, with 80% living in developing nations. Recently, a surge in depression research has been witnessed, resulting in a multitude of emerging techniques developed for prediction, evaluation, detection, classification, localization, and treatment. The main purpose of this study is to determine the volume of depression research conducted on different aspects such as genetics, proteins, hormones, oxidative stress, inflammation, mitochondrial dysfunction, and associations with other mental disorders like anxiety and stress using traditional and medical intelligence (medical with AI). In addition, it also designs a comprehensive survey on detection, treatment planning, and genetic predisposition, along with future recommendations. This work is designed through different methods, including a systematic mapping process, literature review, and network visualization. In addition, we also used VOSviewer software and some authentic databases such as Google Scholar, Scopus, PubMed, and Web of Science for data collection, analysis, and designing comprehensive picture of the study. We analyzed 60 articles related to medical intelligence, including 47 from machine learning with 513,767 subjects (mean ± SD = 10,931.212 ± 35,624.372) and 13 from deep learning with 37,917 subjects (mean ± SD = 3159.75 ± 6285.57). Additionally, we also found that stressors impact the brain's cognitive and autonomic functioning, resulting in increased production of catecholamine, decreased cholinergic and glucocorticoid activity, with increased cortisol. These factors lead to chronic inflammation and hinder the brain's normal functioning, leading to depression, anxiety, and cardiovascular disorders. In the brain, reactive oxygen species (ROS) production is increased by IL-6 stimulation and mitochondrial cytochrome c oxidase is inhibited by nitric oxide, a potent inhibitor. Proteins, lipids, oxidative phosphorylation enzymes, and mtDNA are further disposed to oxidative impairment in the mitochondria. Consequently, mitochondrial dysfunction exacerbates oxidative stress, impairs mitochondrial DNA (mtDNA) or deletions of mtDNA, increases intracellular Ca2+ levels, changes in fission/fusion and mitochondrial morphology, and lastly leads to neuronal death. This study highlights the multidisciplinary approaches to depression with different aspects using traditional and medical intelligence. It will open a new way for depression research through new emerging technologies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In recent days, human lifestyle has changed due to pandemic scenarios affected by psychological and neurological behavioral changes that has led to depression and anxiety [1, 2]. As per WHO, depression is anticipated to be the second most significant reason for infirmity in 2020 affecting about 50 million people worldwide, with 80% living in developing nations [3]. Human psychological disorders like anxiety disorder, mood disorder, and depression are associated with human behavior and are also connected with eating disorders [4]. The negative effects of depression on the human brain have been linked to the increased neuro-pathologies caused by prevalent neurodegenerative illnesses including Alzheimer’s, Parkinson’s, and Huntington’s [5, 6]. Neurological disorders like epilepsy, migraine, stroke and multiple sclerosis decrease the quality of health. Also, it has been seen that anxiety and depression impact low health and quality of life [7]. Stress leads to depression and tension, affecting the physiology of neuro-immune consequences, and it has been observed that focus is more effective in women than men [8].
Mental health has a very essential role in personal well-being and public health. According to WHO, mental health illness is categorized as a global public health problem [9, 10]. Depression is categorized as a severe medical illness for personal and general mental health, and depression can be seen regardless of age, gender, and financial status [11,12,13]. Depression could be a factor affecting negative impact on the lifestyle of an individual leading to social life disruptions [14]. In addition, clinical depression can be addressed by symptoms like feelings of sadness, loss of appetite, sleep cycle disturbances, guilt, incapable of decision making, which could result in self-harm attempts [15]. There are three categories of depression stages. Depression among various populations is associated with physical illness, severe neuropsychological impairment, and low clinical outcomes [14]. Depression is considered a neurological disorder that affects worldwide 3 million people yearly [11].
While significant effort has been made to investigate the pathophysiology and molecular causes of the disease using a variety of methods, the exact cause of Depression is still unknown. From a physiological perspective, Depression is characterized by symptom heterogeneity and alterations in numerous bodily systems. In general, a number of factors, including genetic, environmental, and psychological ones, work together to cause Depression. Depression is a complex health problem, it cannot be tailored by focusing only on one aspect [16]. There exist various diagnostic methods for depression, and they are time-consuming. Also, most of them followed self-reporting or self-diagnosis of patients [12], and are well known to be consulting a psychiatrist or psychologist [11, 13]. In other words, there have been several well-established techniques available for diagnosis, and require experienced health professionals. There is a possibility of misdiagnosis due to overlapping symptoms of the different disorders. Hence, this situation could lead to an increased risk of prolonged major depression. Diagnosis is an essential aspect of depressive disorder treatment in time and is responsible for recovery.
Previous research has mostly looked into particular medical diseases linked to depression because of the complexity and variability of medical data. It has been proved that the use of "big data" and machine-learning techniques and algorithms can uncover important patterns and connections in health data while handling heterogeneous data without rigid limits [17]. In the diagnosis of the associated factors of depression, artificial intelligence (AI) can help at greater extent. New techniques of machine learning and deep learning have made diagnosis and treatment better [18, 19]. Recent research on reaction–diffusion terms in genetic regulatory networks has produced numerous impressive findings, including stability, state estimation, and sampled-data state estimation. One of the most popular topics and ones with promising outcomes is the study of reaction–diffusion neural networks (RDNNs), such as the dynamical analysis of impulsive RDNNs (IRDNNs). The stability is hardly ever obtained when the neural networks are impacted by external input. Therefore, the Sontag-originally conceived input-to-state stability (ISS) is used to assess how external input affects the stability of neural networks [20]. Based on these newly emerging techniques it can be assumed that such techniques can help in diagnosing the underlying issue of depression too. A person's brain structure may change as a result of depression, which can also have psychological effects. Repeated stressful events can eventually harm the human brain in long-term depression. Human brain structural changes can include cortical atrophy, oxygen deprivation, and inflammation. So these complex changes in the near future can be diagnosed and treated by RDNNS, ISS and non- linear dynamics [21].
We have accumulated recent research to address depression and its associates. We have conducted this review to handle important information related to depression-like effects, detection, treatment, and psycho-neurological human behaviors such as stress and anxiety. Previously, there is not a reliable review or meta-analysis available as comprehensive as this one, to the best of our knowledge. This review aims to outline and analyze numerous issues associated with depression among humans and deliver an explanation to the following research questions (RQs):
RQ1: What is the relationship between depression, stress, and anxiety?
RQ2: What are the effects of depression on the human brain and cardiac systems in relation to oxidative stress, inflammation, and mitochondrial dysfunction in depression?
RQ3: What are the effects of depression on genes, proteins, and hormones in the human body?
RQ4: What is the major role of medical intelligence in depression?
RQ5: What is the concept for treating and diagnosing depression patients?
Additionally, the main contribution of this survey is given below:
-
To find out the association of psycho-neurological human behavior such as stress and anxiety with depression.
-
To find out the changes in genes, proteins, hormones, oxidative stress, inflammation, mitochondrial dysfunction, brain, and cardiac during depression.
-
To find the major role of medical intelligence (medical + artificial intelligence) in the detection, prediction, classification, recommendation, and treatment of depression.
-
To find the treatment and diagnosis based on the present scenario with research gap and future recommendations for upcoming researchers, doctors, scientists, and scholars.
-
To design and suggest the closest terms based on previous and current studies using VOSviewer and word clouds to help readers, students, researchers, doctors, scientists, and academicians.
The rest of this survey discusses the methodology of the review, followed by answering the research questions (relationship, effect, role, detection, and treatment), along with the discussion (importance of the present study, network visualization, world cloud, and comparisons), research gaps of the previous studies, and future directions or ideas about work on depression in different aspects like medically, biologically, psychologically, and engineering.
Methods
The following steps were performed in the methods: (a) planning as per PRISMA checklist for publication (b) accomplished a comprehensive literature exploration for information (c) data extraction (d) data analyses (e) analysis of subgroups or subsets, and (f) reporting results [22, 23].
Eligibility criteria
The article selection procedure was divided into two stages. The initial step included one of the authors to assess publications based on the title and abstract. Four scholars independently analyzed publications that were screened. After carefully reviewing the data, the four authors extracted the data independently to prevent bias, and the results were structured in a table. Table 1 listed numerous factors considered while determining exclusion and inclusion criteria.
Information source and search strategies
We compiled relevant literature linked to depression available on Google Scholar, Scopus, PubMed and Web of Science databases using an automated search. These databases are most popular in the modern and traditional research in the world. We widened our search terms and categories to gather enough research relating to our topics. Table 2 lists the keywords utilized in the literature search based on RQs.
Data selection and collections
We looked at papers' titles, keywords, and abstracts to define their aptness and relevance for inclusion in this review. Data from primary studies was effectively extracted, and the quality of the data was independently reviewed. The final decision on inclusion were made, and articles were selected from 1996 to 2023. Four researchers independently analyzed and extracted the data. For any disagreement, the data for the confirmation was reviewed by three other researchers. The PRISMA checklist was referred for the assessment [24]. This paper include detailed records regarding the major role of medical intelligence in depression details of previously published work using machine learning and deep learning in depression were evaluated through objective, the number of subjects, dataset, domains, classifier, and performance measures were documented. Any disagreements among the writers were settled by consensus. In addition, the relation between depression, stress, and anxiety, the effects and relation of depression on brain and cardiac systems with the relation between oxidative stress, inflammation, and mitochondrial dysfunction in depression, the effect of depression on gene, protein, and hormone, and treatment and diagnosis of depression patients with evidence-based studies with the mechanism of action of natural bioactive molecules in medicinal plants for depression.
Synthesis of the result
Statistical methods were performed for the strategy of data synthesis. The major role of medical intelligence in the depression details of previously published work using machine learning and deep learning in depression were evaluated through objectives, the number of subjects, dataset, domains, classifier, and performance measures. We also retrieved related to depression with machine learning and deep learning such as per (a) publication under open access and subscription, (b) year-wise publications, and (c) country-wise share, in the Web of Science database. Additionally, we designed a Network visualization based on a previously published article related to this study.
Medical intelligence in the depression
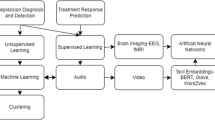
Medical Intelligence terms are made up of medical and artificial intelligence (AI). The application of artificial intelligence is summarized in Fig. 1. Machine learning is growing as a dynamic research area in many fields of science including computer vision, natural language processing, speech recognition, genes expression, image recognition, and signal processing, [25,26,27]. Whereas deep learning is a subset of the machine learning that learns the learning process. Deep neural network is a branch of deep learning and can be employed in extracting information from signals.

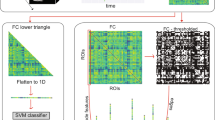
Application of AI in the depression
Filho et al. [28] assessed the effectiveness of machine learning algorithms in identifying patients with depression by analyzing clinical, laboratory, and sociodemographic data collected from the Brazilian National Network for Research on Cardiovascular Diseases between June 2016 and July 2018. Zhang et al. [29] developed a machine-learning framework to predict the risk of postpartum depression (PPD) using data extracted from electronic health records (EHRs). Poletti et al. [30] emphasized the importance of innovative tools for early diagnosis of bipolar disorder (BD), the integration of biomarker research into clinical practice, and the development of novel therapeutic strategies for depressive disorders. Pearson et al. [31] found that multiple variables can predict symptom improvement following an Internet intervention, although each variable contributes only modestly. Hochman et al. [32] created and validated a machine learning-based model for predicting PPD using electronic health record (EHR) data, and discovered new predictors for PPD. Liu et al. [33] aimed to enhance the response to reward-related stimuli in major depressive disorder (MDD) by targeting dopaminergic signaling in the entire brain. Kambeltz et al. [34] developed an algorithm that utilizes clinical patterns and machine learning to predict the response of transcranial direct current stimulation (tDCS) and escitalopram in individuals with major depression. Na et al. [35] focused on constructing a predictive model based on machine learning to anticipate the future onset of depression. Helbich et al. [36] studied 1190 people aged 60 and up in a cross-sectional study. The abbreviated Geriatric Depression Scale assessed depressive symptoms (GDS-15). A fully convolutional neural network extracted streetscape green and blue spaces from Tencent Street View data. On a neighborhood level, indicators produced from street view photos were compared to those derived from satellite-based normalized difference water index (NDWI), normalized difference vegetation index (NDVI), and GlobeLand30 land cover data. Multilevel regressions with neighborhood-level random effects were used to determine the relationships between neighborhood-levels green and blue regions. They concluded that green and blue areas in the street view are protective against depression in the elderly in China, but longitudinal confirmation is needed to infer causality. Different characteristics of natural habitats are represented by the street view and satellite-derived green and blue space metrics. Street view data and deep learning are useful tools for automated environmental exposure assessments. Oh et al. [37] reported that a deep-learning approach had got AUC of 0.91 and 0.89 for predicting depression in NHANES and K-NHANES, respectively. With an AUC of 0.92, a deep-learning algorithm trained on serial datasets predicted the prevalence of depression in the next two years of data. NHANES with machine learning classifiers could help predict depression in K-NHANES. The maximum performance (AUC: 0.77) was achieved using logistic regression, followed by the deep learning method (AUC: 0.74). Mumtaz et al. [38] could change clinical applications for EEG-based depression detection. Based on the findings, it is possible to conclude that the deep learning framework might be used to diagnose depression automatically. Gui et al. [39] have used a convolutional neural network (CNN) with local residual response to represent four different types of functional magnetic resonance imaging (fMRI) data obtained by depressed patients and healthy persons while listening to happy and negative emotions music. To match the features and obtain the correlation matrix, they utilized a large convolution kernel of the same size as the correlation matrix. At the beginning four-dimensional fMRI data was utilized to create a two-dimensional correlation matrix of one person's brain based on ROIs, which was then processed using a threshold value chosen based on complex network and small-world network properties. In this article, the deep learning model is compared for classification with other algorithms. Finally, researchers compute matching ROIs from the intermediate outputs of their deep learning model, which can aid in further research in related disciplines. Furthermore, in [40], mainly focused on visual and auditory markers of patients functioning for clinical diagnosis, therapy selection, and prognosis, detection method. Identifying these signals helped improve clinical assessment consistency, sensitivity, and scalability. They wanted to see if clinical features from free speech responses to a brief interview, one month after trauma, could be captured using machine learning-based semantic, computer vision, and acoustic analysis to classify MDD and PTSD. Concluding, audio visual markers can be helpful tools to measure post trauma status of patients with MDD and PTSD. In another study by Little et al. [14] twenty-nine patients with Late-life depression (LLD) and 29 age-matched controls wore a wrist-worn device that captured their acoustic surroundings for seven days. Deep learning models were constructed and verified on an independent speech dataset to automatically interpret acoustic input. While respecting participants' privacy, total speech activity and the proportion of speech produced by the device wearer were recognized. A neuropsychological test battery, as well as clinical and self-report scales along with general and social functioning were used to assess the degree of depression. Using graph theory, Li et al. [13] investigated aberrant structure in the functional connectivity network of moderate depression in [7]. Second, they suggested a new categorization model for mild depression recognition. Third, they used CNN to process two-dimensional reparatory from the 2D data form the functional connectivity matrices using EEG. Inspired by recent breakthroughs in the ability of deep recurrent CNNs, to classify mental load. The classification model correctly identified mild depression with an accuracy of 80.74% [11]. According to the findings, combining a CNN with a functional connectivity matrix could give a potential objective method for detecting moderate depression. Numerous studies based on machine learning and deep learning employing electroencephalogram (EEG) have been undertaken [11]. The asymmetry matrix picture achieved 98.85% accuracy in the alpha band, outperforming most of the methods given in earlier studies [11]. To detect depression, Knag et al. [11] developed a deep model based on CNN and long short-term memory (LSTM). The local features and EEG signal sequence are learned using CNN and LSTM. To build feature maps in the deep learning model, filters convolve with the input signal in the convolution layer. All the collected characteristics are fed into the LSTM, which learns various patterns in the signal before doing classification using fully connected layers. The memory cells in the LSTM allow it to recall important features for a long time. It also includes several functions for updating the weights during workouts. The model was tested using a random splitting technique, which yielded an accuracy of 99.07% and 98.84% for the right and left hemisphere EEG signals, respectively. Zhang et al. [41] concluded a clinical trial on the handling of epileptic patients with anxiety and sadness using electronic nerve stimulation from the Internet of things. They start their paper by employing literary technique to investigate the origins of epilepsy and previous treatment methods. Finally, the assessment of epileptic symptoms, sadness, and anxiety before and after therapy between the observation and the control groups were examined. They discovered that, of the 50 cases in the trial, the observation group that employed electrical nerve stimulation therapy had five people who stopped having seizures following treatment, accounting for 10%, whereas the control group using traditional medicine had none. Furthermore, the observation group's SAS and SDS ratings were minor than those of the control group. As a result, using electrical nerve stimulation, to treat epilepsy with anxiety and depression, has improved presentation and can assist patients in speedy recovery. In addition, the most common performance measures of the machine learning model are used in the depression are mentioned in Eqs. (1)-(4) [42,43,44,45,46,47,48,49,50] below:
We have designed the database related to the role of the machine and deep learning in depression based on previous studies, mentioned in Fig. 2. It is evaluated based on open access (59%) and subscription (41%) publications, year-wise and country-wise. In the country-wise publications, the United States of America (USA) has the highest (16%), China (14%), and India (12%) is in second and third numbers, respectively. We found that related to machine and deep learning in depression 59% papers are published as open access and 41% of papers published as subscription or close access. In year-wise publication highest rate is in 2019 and 2021 (31%) and the lowest rate is in 2018 and 2022 (3%). While, in country wise publication, USA (16%), China (14%), and India (12%) is in Top 3 and in lowest Argentina (2%), Australia (2%), Canada (2%), Germany (2%), Norway (2%), Spain (2%), Thailand (2%), Turkey (2%), Italy (2%), Japan (2%), Malaysia (2%), and New Zealand (2%). These details would be helpful for researchers, doctors, and scholars to work in this area. In addition, we have also evaluated the previously published research article related to depression with machine learning and deep learning shown in Tables 3 and 4.

Details for the previously published articles related to depression with machine learning and deep learning such as a publication under open access and subscription, b year-wise publications, and c country-wise share, in the Web of Science database
Association between depression, stress, and anxiety
Three important terms define psychological distress: stress, anxiety, and depression. Stress is a mental or physical sign such as irritability or digestive trouble whereas anxiety is defined as transient fear and uncertainty about the future. Its severity depends on the intensity and frequency of experiencing anxiety [93]. Stress is caused by several foreign stimuli, such as the daily stressful events, school grades of adolescents, and financial problems of adults, which can result in irritability. Prolonged irritability and helplessness to solve problems cause chronic stress, leading to depressive disorders [94]. Anxiety disorders include general and perinatal anxiety, phobia, panic syndromes, social anxiety syndrome, obsessive–compulsive disorder (OCD), post-traumatic stress disorder, and body dysmorphic syndrome [95]. Chronic stress and anxiety can result in depression [96]. There is evidence for the accumulating effect of daily stressors on cardiac health, such as unhealthy eating practices and a sedentary lifestyle [97]. Daily stressors impact human health which leads to worry, and these prolonged everlasting worries lead to a depressive state. Major depressive disorder affects the quality of life (QoL). Numerous studies have established and explored the relation between depression and QoL [98]. Psychological stress is a significant factor in major depressive disorders in animal and human models. Chronic psychological stress activates inflammatory pathways resulting in inflammation [99]. Resultant inflammation leads to Cardiac heart diseases (CHD) and neurological deformities. Stressors impact the brain's cognitive and autonomic functioning, resulting in the increased production of catecholamine, decreased cholinergic activity, decreased glucocorticoid activity, and increased cortisol. These factors lead to chronic inflammation and hinder brain's normal working, leading to depression, anxiety, and cardiovascular disorders [100]. In major depressive disorders, neurotransmitters such as catecholamine, norepinephrine, and/or dopamine have important roles [101]. However, the role of the catecholamine actions in the pathophysiology of major depression is understood partially. Norepinephrine binds to α1- and β-adrenergic receptors and results in a stimulatory influence on cell signaling; specifically, increases intracellular phospholipase C and cAMP. However, stimulation of the α2-adrenergic receptor subdues intracellular cAMP and inhibits signaling [102]. In melancholic depression, norepinephrine stimulates anxiety and hyperarousal, promotes corticotropin-releasing hormone-mediated hypercortisolism, promotes insulin resistance, and causes bone loss [103]. In an experimental investigation, the urinary catecholamine was measured in depressed and everyday individuals. Catecholamine levels were found to be significantly increased in depressed individuals [104]. Terms such as stress, anxiety and depression are frequently used where the stress is a basic short-term issue which if left untreated can lead to anxiety. Anxiety is a chronic issue that can become the cause of major depressive disorder. In this vicious cycle sometimes depression results in anxiety too. The relation between stress, depression and anxiety is illustrated in Fig. 3.

Relationship between psycho-neurological human behavior such as stress, anxiety, and depression
Depression and anxiety increase plasma catecholamine that results in the reactive oxygen species (ROS) formation. ROS formed in a depressed state can further affect the coding and non-coding regions. ROS causes transient dynamics of si-IncRNA in the nucleus. It accumulates in polysome, replacing mRNA and causing transcriptional stress [105]. The impact of stress on the molecular level can be different in both genders. An experimental study concluded that the Dusp6 gene is downregulated in stress affecting the transcriptional pathway in female mice, whereas ERK signaling and neuron excitability increased in males [106]. These transcriptional modifications play a role in major depressive disorders (MDD) and can be studied further to develop anti-depressive medications accordingly. A study conducted on Chinese university students showed that high sugar intake, gender, grades, and complaints of stress and anxiety were associated with depression [107]. The presence of injury, a high-fat diet, and depression was associated with anxiety and stress. This study concludes that stress, depression, and anxiety are correlated to causing psychological distress [108].
Effects of depression on the brain and cardiac systems
Clinical depression is an adverse form of continuous stress. Stress negatively impacts human behavior and mental health. Persistent and prolonged stress leads to hippocampus function impairment because of the increased glucocorticoid levels [109]. Constant pressure leads to the neural scar effect's gradual loss of hippocampus volume. Hippocampus impairment aggravates stress-induced memory deficit and cognitive impairment [110]. It is vulnerable and targets part of the brain in depression. It can result in neurofibrillary tangles and global ischemia. Repeated stress causes dendritic atrophy in the CA3 region [111]. A study was conducted by Samuel et al. [112] in which they concluded pre-and post-synaptic effect of depression on neurons reduces the number of NMDA receptors activating the TPA/plasmin system. TPA/plasmin system acts as a mediator in the devastating impact of chronic depression on hippocampal function at the neural level was on stressed mice. Others were normal and showed significant loss of hippocampal volume in stressed mice within a ten-day tenure. Normal mice brain was not affected by the environment provided and no significant change was noted in the total brain volume of both groups; another conclusion was that the same type of stress has an asymmetric impact on both sides of the hippocampus [113]. In depression, the left hippocampal part has more volume reduction than the right one [109].
Histopathological studies done postpartum on people who were depressed in life showed cortical and subcortical region alterations. Those areas were functionally disabled. Major depression disorder can be diagnosed by the neuroimaging of the orbitofrontal region of the brain [114], where the thickness of the cortical is reduced, and the density of neuron and glial cells are decreased [111]. The progressive histopathological loss because of depression causes traumatic brain injury, a significant cause of disability and death around the globe [115]. Depression increases the number of reactive oxygen species, causing mitoc stress in the body that lowers the antioxidants [116]. The significant effect of oxidative stress is seen in the brain, with a high need for oxygen, fat, and low antioxidant levels [117]. The increased oxidative stress because of depression causes neurodegenerative disorders. Pro-oxidants such as copper are found in the free form more and less in depressive patients, affecting neuronal excitability and functioning. The copper radical also hinders neurological signal transmission and is negatively influenced as they alter the cortical glutamatergic neurotransmission [118]. Oxidative stress caused by depression is also linked with cardiac hypertrophy, leading to heart failure because of the increased free oxygen species and decreased antioxidant defense [119]. Studies suggest that heart failure resulting from myocardial infarction is associated with antioxidant deficit and myocardial oxidative stress [120]. ROS is linked with arrhythmic conditions, leading to cerebrovascular dysfunction and myocardial infarction. Another study conducted on patients with acute myocardial infarction showed that reactive oxygen species are directly connected with the pathogenesis of atherosclerosis, causing acute coronary artery disease and causing aggravation in the ischemic condition of the heart [121].
Major depression causes multiple health problems. Two subjects were studied for four years in a cohort study, one group with cardiac disease and depression and another group with depression but not having cardiac diseases. It was concluded that cardiac mortality increases in depressed individuals in both groups. Another study states that even if the social and environmental factors are still minor and major depression is the causative agent of early death, minor depression is more associated with elderly patients [111, 122]. Physical and emotional stress sometimes causes reversible cardiomyopathy associated with acute onset of cardiac pain and abnormal cardiac wall motion. Stress cardiomyopathy is sometimes confused with coronary heart disease, but the enzymatic levels such as troponin T and troponin I increase, becoming a risk of heart attack [123]. SCM is also found to elevate other cardiac enzymes such as plasma catecholamine and neuropeptide levels, which can cause myocardial stunning and brain injury [124]. Figure 4 illustrates the impact of depression on the nervous and cardiac system. The hypothalamic-pituitary axis can be activated and necrohormones can be secreted as a result of alterations in the central nervous system (CNS), which can destabilize the sympathovagal balance. The progressive onset of coronary artery disease (CAD), plaque activation, and an acute episode can all be caused by immune system suppression and an increase in pro-inflammatory cytokine release [125].

Impact of depression on the nervous and cardiac system
Relation between oxidative stress, inflammation, and mitochondrial dysfunction in depression
Morava et al. [126] reported that chronic mild stress causes dissipation of mitochondrial membrane potential, inhibition of mitochondrial oxidative phosphorylation (OXPHOS), and ultrastructure damage of mitochondria in numerous brain areas plus the hippocampus, cortex, and hypothalamus. These findings conclude that mitochondrial dysfunction leads to brain energy impairment, and perhaps causes depression. Furthermore, studies have reported that patients who suffer from depression show reduced glucose utilization in the PFC, caudate nucleus, and anterior cingulated gyrus [127].
Activation of inflammatory, immune, oxidative, increased HPA-axis and nitrosamine stress paths have been observed in major depression as evident from many studies. Stress increases IL-1β, TNFα, IL-6, and another pro-inflammatory cytokine. Mitochondrial damages are induced by the mitochondrial complexes I and IV suppression by TNF-α, a pro-inflammatory cytokine, and pyruvate dehydrogenase activities. In the brain, reactive oxygen species (ROS) production is increased by IL-6 stimulation and mitochondrial cytochrome c oxidase is inhibited by Nitric oxide, a potent inhibitor [128].
The other factor persuading the aetiology of depression is an inequity between ROS production and the antioxidant defense mechanism. Brain oxidative stress is increased in depression which lowers brain glutathione concentration, catalase, superoxide dismutase, and total antioxidant capacity as reported in-vivo study in mice [129]. The core site of the cell’s ROS production are mitochondria and extremely prone to oxidative damage. Proteins, lipids, oxidative phosphorylation enzymes and mtDNA are further disposed to oxidative impairment in mitochondria. Consequently, mitochondrial dysfunctions exacerbate oxidative stress, impairment of mitochondrial DNA (mtDNA) or deletions of mtDNA, increase in intracellular Ca2+ levels, changes in fission/fusion and mitochondrial morphology and lastly leads to neuronal death. Additionally, mitochondrial dysfunction is conceded by energy demand upsurge for the cellular repair process and in this way damage to mitochondria leads to more damage [128].
Effects of depression on gene, protein, and hormone
Depression is a multifactorial and multi-genetic health problem. Several genetic mutations are seen that are connected to depression. The Association between genetic variants, mood-related traits, and medication of environmental factors is shown in Table 5 [130]. The hypothalamic-pituitary-adrenocortical system (HPA) plays a significant role in the cause and development of depression [131]. HPA system is hyper-activated in depression by the part of corticotropic releasing hormone (CRH) and glucocorticoid binding receptor system found in the hippocampus. HPA system dysregulation causes cognitive impairment in depressed people [132]. Depression is associated with CVD, but the mechanism is unclear. A study claimed depression increases C reactive proteins in the body, which causes systemic inflammation resulting in CVD risk [133]. Inflammation and depression have a bilateral relationship, as depression enhances the activation of CRP, IL-1, and IL-6, which is positively associated with inflammation and increased BMI and vice versa [134]. Cortisol is secreted at the hormonal level, and the hypothalamus pituitary-adrenal axis (HPA) is also hyper-activated in depression. An increase in cortisol levels makes individuals more vulnerable to mood disorders. Estrogens are a group of hormones that are associated with women reproductive health. In depression, estrogen levels are negatively correlated. Decrease in estrogen hormones in female leads to depression and anxiety, whereas increasing estrogen levels in women helps reduce depression symptoms [135, 136]. When cortisol levels are high, it works on the amygdala producing simultaneous responses, which later are shifted to the hippocampus to rationalize the situation. This transition because of depression is dependent more on an individual's cognitive processing before the onset of puberty [137].
Noradrenaline and ACTH show a more rapid increase in acute stress than cortisol levels. An increase in ACTH levels elevates cortisol secretion, and it also causes fatty tissue deposition in the body. Acute stress also promotes leptin and IL-6 these parameters can increase the weight of the depressed person [136]. In major depressive disorder patients, depression affects the peripheral inflammatory markers activation such as cytokines, interleukins, chemokines, and tumor necrosis factor-alpha further affects the blood circulation and parts of the brain such as the amygdala. Moreover, in women, elevated estrogen levels aggravate mood swings and stress conditions. Estrogen also affects the mechanism of action of antidepressants and the body's response to them [138]. In depression, it is evident that mitogen-activated protein kinase, particularly ERK, is down-regulated in depressed individuals at the hippocampus, and prefrontal cortex levels along with the reduction of BDNF and CREB activity [99]. The gut microbiome is an important component of the microbiota-gut-brain axis (MGBA), which influences the brain and behaviour. Disturbance of the gut microbiome affects tryptophan (TRP) levels. TRP is an essential amino acid and there are two major TRP metabolism pathways in the brain and peripheral systems: > 95% of TRP is converted into kynurenine (KYN) and its breakdown products, which are involved in inflammation, immune response, and excitatory neurotransmission, while a small portion of TRP is used to produce transmitters like 5-HT. An earlier investigation revealed that the enzyme IDO1 was involved in the KYN pathway and that patients with depression had higher plasma KYN/TRP ratios. TPH2 is an isoform of TPH that regulates the brain's production of 5-HT. According to studies, TPH2 aberrant expression can raise a person's risk of suicidal thoughts and severe affective disorder score [139]. Another gene that plays a significant role in depression aggravations is 5 HT1A. Due to its crucial significance in the autoregulation of the functional activity of the brain's 5-HT system, the 5-HT1A receptor draws particular attention. Overall, 5-HT1A signaling reduces protein kinase activity and neuronal firing rate. The pre- and postsynaptic 5-HT neurotransmission implicated in mechanisms of sleep, stress response, appetite, sexual motivation, aggressive behavior, depression, and anxiety is powerfully regulated by 5-HT1A receptors. It has been demonstrated that genetically defined aggression is correlated with decreased 5-HT1A receptor mRNA expression in the midbrain, decreased 5-HT1A receptor density in the hypothalamus, frontal cortex, and amygdala, and lower 5-HT1A receptor functional activity [140].
Treatment and diagnosis of depression patients
Depression is one of the major health concerns faced by human beings worldwide. It is more prevalent in low-income countries and can trigger many other disabilities [141]. The effectiveness of treatment for depression is dependent on several factors such as differences in gender, comorbidities, behaviors, and socioeconomic conditions [142]. Multiple treatments are implied to reduce depression in human surroundings. From the beginning of the twenty-first century, nine major antidepressants have been introduced to treat depression. Newly formulated drugs are structurally different from previously existing medicines such as monoamines. Depression has multiple factors, and the treatment plan should be according to them. It is essential first to rule out the underlying cause of depression. Monoamine oxidase inhibitors are effectively in depressed patients who do not respond to tricyclics [143]. Estrogen therapy could be done in women facing prenatal or postnatal depression and premenopausal stages [142]. Cognitive-behavioral therapy is also used to treat depression. An experimental study was conducted to compare behavioral activation of cognitive therapy and behavioral therapy and skills to control automatic thoughts without CT. Results showed that both treatments are equally effective, but the attributional style was predictive only in BA, not CT. Psychotherapies are found most effective even in pandemic times, as provided by the e-counselling strategy [144]. Exercise or physical activity probably has a central effect on depression via an increase in the release of β-endorphins, in the accessibility of brain neurotransmitters such as dopamine, serotonin, and noradrenaline, or in brain-derived neurotropic factors. Wu et al. [145] provided evidence for the effectiveness of Aerobic training in Parkinson’s disease with depression patients had minimal physical and mental symptoms and improvement in their QoL and decrease in depressive symptoms. Aerobic exercise with a public health dose of 17.5 kcal/kg/week energy expenditure is also effective in lowering the severity of depression [146]. Another study also claims that when physical activity is added to antidepressants in one's treatment, it shows more positive responses [147]. Multiple levels of treatments for depression can range from lifestyle modification, psychotherapy, anti-depressive medication, estrogen therapy, CBT to the use of AI. Treatments of depression based on different ways are summarized in Fig. 5.

Treatment of depression based on different techniques
The Unani medicine (USM) is a traditional complementary and alternative system of medicine for treating depression. It has holistic principles that support a practitioner in turning a diagnosis into a treatment plan and employs various techniques. It obeys a complete healing philosophy. Hence, in USM various therapies are available for curing the sickness as well as improving the patient's general health. There is rising evidence of the usefulness of herbal medicines in treating anxiety and depressive disorders. Psychotherapy, dietary treatment, or pharmacotherapy can be used alone or in combination to treat depression. Psychiatric diseases have been discussed in detail in Unani medicine, which identified numerous symptoms of mental faculties due to the participation of vitiated humour, particularly yellow bile and black bile. Still, their symptoms are discussed under several headings such as melancholia, delusion, hallucination, insomnia, disorder of love, palpitation, etc. Avicenna recognized numerous mental illnesses including the disorder of love, which was defined as an obsessive disorder approaching severe depression [148]. In Arabic and Unani literature, anxiety has been described, while the word psyche is appended to anxiety to describe its psychological state. Izterab Nafsani means "concern, fear, and excessive pondering”. It's also used to describe a stumbling block to routine tasks [149, 150].
As per the role of diet, there is another dietary element named as probiotic commonly found in yogurt that can be very helpful for depression patients. Probiotics' primary function in the treatment of depression is to modulate the gut microbiota to restore the balance of the gut's microorganisms. By encouraging the biotherapeutic activity of the advantageous microbiota and inhibiting the pathogenic action of the pathobionts, probiotics have a positive impact on human health [61]. A bacterium is the best option for a probiotic if it can penetrate the target organ, which is typically the intestines, endure numerous physiological stressors, including the shifting pH down the gastrointestinal canal, and stop the progression of the disease [62, 63]. The most popular microorganisms employed as probiotics are Lactobacillus spp. and Bifidobacterium spp. because of their wide range of health-promoting qualities. These bacterial species are well-known for their potential as antidepressants and for having good safety profiles. They have a modest pathogenic potential and hardly accelerate the horizontal spread of antibiotic resistance in pathogens [151].
Temperament is a unique condition in the USM of an individual that reflects metabolic, neuroendocrine, genetic, and some environmental balance at the optimal adjustment of function level [150]. The body's normal and healthy functioning depends on the harmony of certain temperament, and disruption in this state is the source of bad health, resulting in various medical states. Simple imbalance of temperament is defined as a change in the equilibrium of four qualities, namely warmness, coldness, moistness, and dryness. If this imbalance occurs at the level of body fluids/humour, it is defined as abnormal substantial temperament [149, 150]. Hippocrates' humoral theory is well known and his idea assumes that the body contains four humours expressed as sanguine, phlegmatic, choleric, and melancholic based on the humour present in them. Each individual is expected to have a different humoral constitution that reflects their overall health. Any change in this has an impact on his overall health. Psychic, vital, and digestive faculties are the three major faculties in Unani medicine to manage the human body and are unique to a given tissue or organ, and they are responsible for the organ's distinct tasks. Nutrition, growth, and reproduction are all addressed by digestive power/faculty. Brain is said to be the seat of psychic or mental power, which is concerned with sensory, intellect, and motor functions. These are perceptive/cognitive faculties, of which there are two types: external perceptive power and internal perceptive powers. Internal perceptive faculties are connected with the intellectual functioning of the brain. In contrast, sensory function is external perceptive power and also includes five external senses such as hearing, vision, smell, taste, and tactile sensation. Psychiatric issues are addressed in depth in the psychiatric diseases in Unani literature. Imaginative power, thinking power, and memory were described by Haly Abbas (Majusi) [150, 152].
Traditional Unani medicine describes that the brain is at the center of these abilities, which allows them to plan and execute functions of imagination, reasoning, and memory. The change in quantitative or qualitative of humours predominantly morbid black bile and loss of continuity leads to an imbalance temperament of the brain and act as a risk factor for psychiatric, mental illnesses caused by disturbance of mental faculties [153]. Psychiatric diseases produce depression, grief, hallucination, mood swings, delusion, sadness, negative thoughts, etc. These symptoms are surmised as depression. Forgetfulness and dementia (Alzheimer’s disease) arise in old age due to changes in the brain, morbid phlegm accumulation in the brain whereas excessive dryness causes insomnia [154]. Pneuma movement outward or inward is seen in various emotions for example in anger the pneumatic moves sudden and outward, gradual and outwards as in happiness, in fear, sudden and inward and gradual and inwards as in sadness [3]. Internal perceptual capacities are five in number includes faculty of composite sense, imagination, memory, and ideation powers [154].
Faculty of composite sense is the capacity to convert all sensations, react to this form, and combine their shapes. Memory power is responsible for the retention and memorizing of the shapes of things. Imagination power is defined as the perception of thinking. Ideation and memory power help to performs imagination power. Imaginative power is concerned with creating abstract concepts, imagination, and thoughts. They were only divided into three categories by Haly Abbas and other physicians: thought, thinking and memory processes are considered as a single faculty.
The brain is classified into three functional parts by Unani physicians: forebrain, midbrain, and hindbrain. The forebrain has the processes/power of the thought, the midbrain thinking and hindbrain memory. If a disease affects the entire brain, all three processes and functions become impaired. If the condition is limited to a particular brain area, the deficiency will only affect that faculty. Psychiatric disorders are classified as depression/ melancholia, insomnia, palpitation, delirium, insanity and other terms in the Unani medical system [155]. Avicenna has recommended the use of medications that increase the substance of the brain, purify the brain, sedative, brain tonics, and medications that promote memory, heart tonic, brain stimulants, and memory enhancers. Blood purifiers purify the blood to some extent. The medications that stop producing and prevent gaseous material migration towards the brain from other body organs may potentially be used in the treatment if necessary [3]. The following are the therapy principles:
-
Except for sanguine humor, concocting the affected humour, primarily through concoctions followed by purgatives for morbid matter evacuation, and secondarily venesection.
-
Using medications such as moisturizer, alternatives of temperament, therapy like massage, exercise, and exhilarants to relieve tachycardia, palpitation, thirst, and overall coldness.
-
Using psychiatric counselling and administering brain tonics.
Treatment care plan is determined by the humour that is impacted. Depression is frequently produced by the combustion of one of the four senses of humour, which then transforms into the black bile variety; as a result, the afflicted humour, i.e., the predominance of black bile throughout the body, must be removed. Depending on the patient’s condition, venesection of the saphenous or cephalic vein is performed until the running blood’s blackish hue and viscosity persist. Following venesection, black bile purgative is advised such as medicated decoction of roots of Papaver somniferum, Ziziphus sativa, Cordia latifolia, Andopogams haenarthus, Caparis spinosa root wall, Rubia cordifolia, each 25 gm, and given with sweet almond oil (Roghan Badam Shirin) in a dose of 70 ml for 7–10 days continuously [150, 152]. Evacuation is produced with semisolid preparation (Jawarishat), which consists of Cuscuta reflexa, Terminalia chebula unripe fruit, and Boswellia serrata. Following venesection, lamb flesh cooked with Cucurbita maxima, Spinacia olereacea, and dressed with almond oil, as well as half-boiled egg yolk with Sharbat-i-Banafsha, can be advocated to produce moistness in the blood. As a purgative, Habb-i-Ustukhudoos (Lavandula stoechas) can be used. If purgation is required, Cuscuta reflexa infusion and Lavandula stoechas with cow’s churned milk should be provided [156].
Mechanism of action of natural bioactive molecules in medicinal plants for depression
Medicinal plants comprise many natural bioactive compounds useful in psychiatric disorders (anxiety, depression, etc.) as they possess antidepressants, nootropic (cognitive enhancing), anxiolytic, hypnotic, sedative, antioxidant, and analgesic potential activities. The versatile cellular mechanism of action of these plants involves stimulating CNS activity or sedating and adaptable endocrine system’s healthy function. Specific plant secondary metabolites such as tannin, phenolic compounds, and alkaloids bind to neurotransmitter/neuromodulator receptors acts through general function and alteration in neurotransmitter synthesis. Other traditional properties such as “adaptogenic” and “tonic” activities are hypothesized to augment adaptation to exogenous stressors through multifaceted effects on the endocrine system and neurochemistry [157]. Monoamine oxidases (MAOs) are localized on the mitochondrial outer membrane and they are Flavin adenine dinucleotide (FAD) co-factor-dependent enzymes. These enzymes catalyze the oxidation of endogenous and xenobiotic monoamines. Thus, MAOs modulate the levels of monoamine neurotransmitters and play a potential role in the central and peripheral nervous system. MAO-A and MAO-B are two isoforms that are present in most mammalian tissues. Monoamine oxidase MAO inhibitors (MAOIs) inhibit the activity either of MAO-A or MAO-B [158]. Antidepressants are MAO inhibitors of type A (MAOI-A). Phytoconstituent flavonoids (catechin and quercetin) inhibit MAO. Quercetin inhibits MAO-A. "Flavonoids activated upstream MAPK–kinase–kinase, inhibited oxidative stress-induced apoptosis, and prevented Jun N-terminal kinase activation”. Catechin increases serum BDNF. Polyphenols, the second metabolite in the plant material acts on TrkB and TrkA expression and neurogenesis are amplified which results in neuroprotection and antidepressant potential [159]. Tannins act as antioxidants [160]. It is supported that the energy metabolism of mitochondria might have an antidepressant activity [161]. Several Unani plants extract and natural products such as P. somniferum, Z. jujube, S. nigrum, B. monnieri, C. sativa, T. terrestris, W. somnifera, V. officinalis, Chamomilla officinalis, Echium amoenum, etc. have been examined and screened for their possible neuro pharmacological actions in diverse animal models including mice and rats [162]. A study reported that black cohosh, chaste berry, passionflower, chamomile, lavender, and saffron seem to be beneficial in mitigating depression with favorable risk–benefit profiles compared to standard treatments [163]. Numerous human clinical trials provide initial positive evidence of the antidepressant properties of C. sativus, E. amoenum, and R. rosea. However, they concluded that watchfulness is suggested when interpreting the results as numerous studies have not been replicated. Furthermore, in vitro and in vivo evidence of several herbs are currently unexplored in human studies [157].
Z. jujube seeds, leaves and fruits have sedative, hypnotic, and anxiolytic actions. It contains phytoconstituents such as triterpenic acids, flavonoids, phenolic acids, nucleosides, saponins, cerebrosides, vitamins, and total sugars. Its chemical compounds are Zizybeoside I and II, Zizyphus saponin I and II Jujubasaponin IV, Swertisin, Lotoside I and II, Chryseoriol, and Quercetin [164]. In the mice model, B. monniera exhibited antidepressant activity [165]. B. monnieri plant is reported to have anxiolytic, antidepressant, antiepileptic, and anti-parkinsonism activities. It contains phytoconstituents such as alkaloids (nicotine, bacosides A & B Brahmin, and herpestine), saponins (monnierin and hersaponin), flavonoids (apigenin and luteolin), and sterols like beta-sitosterol and stigma-sterol, proven for neuro pharmacological activities. T. terrestris leaves and the whole plant are proven for anxiolytic, antidepressant and sedative activities. Its phytoconstituents are flavonoids, saponins, alkaloids glycosides, and tannins. The chemical compounds present in T. terrestris are quercetin, stigmasterols, rutin, tigogenin, neotigogenin, ruscogenin, cafeoyl, kaempferol, tribulosid, chlorogenin, terrestribisamide, Beta-sitosterol, norharmane harmane, and tribulusterine [166]. Similarly, W. somnifera has been reported to have anticonvulsant, antidepressant, anxiolytic, and anti-Parkinson actions, mostly due to the presence of sitoindosides VII–X, withanolides, and withaferin-A [167]. Müller et al. [168] use 2500 participants with depression, reported the combination of valerian (600 mg) and St John’s-wort (600 mg) showed improved effects than each of them alone. Valeriana officinalis (valerian) acts as a partial agonist on the 5-hydroxytryptamine 2A receptor and the γ-aminobutyric acid (GABA)-A receptor comparable to benodizapenes and boosts melatonin release thereby having antidepressant action. The valerenic acid and valepotriates, natural bioactive molecules of valerian root are accountable for their above mentioned application [169]. Amsterdam et al. [170] reported in an RCT on 57 patients that chamomile capsules (220 mg/dl) for 8 weeks significantly decreased the depression score in the chamomile than in the placebo group. Women during the postpartum period who consumed chamomile tea reported significant improvement in quality of sleep and depression in a controlled trial [171]. Apigenin and quercetin are bioactive molecules in chamomile with antidepressant potential because they can modulate dopamine, norepinephrine, GABA messaging, serotonin and controls hypothalamic pituitary adrenal (HPA) axis activity, and inhibits monoamine oxidase (MOA) enzyme action [170]. Sayyah et al. [172] reported E. amoenum (borage) (375 mg) showed significant antidepressant activity than placebo in a 6 weeks RCT. Rosmarinic acid and the sinine are the bioactive molecules were identified in Borage [173]. Some studies on borage recognized the role of oxidative stress in the anxiety of rodents. According to this, it has been shown that induction of oxidative stress in mice occurs at the same time as anxiety. E. amoenum has antidepressant, anxiolytic, anti-obsessive–compulsive, anti-inflammatory, antioxidant, and analgesic properties. The functional mechanism of E. amoenum perhaps depends on γ linolenic acid (GLA) [174]. Flowers of E. amoenum have GLA and anti-inflammatory and antioxidant properties. Cyanidin 3-glucoside is the most common anthocyanin present in the E. amoenum petals that has neuroprotective action and has routinely been used as an antidepressant and anxiolytic medicine in Asia [175]. Lavandula spp. is potentially useful in depression, anxiety and somatic tension. In various studies in animal models, anxiolytic activity has been proven. Lavender acts through GABA modulation (based on volatile constituents) [162]. An RCT confirmed that lavender tincture with imipramine was more effective than lavender alone in mild to moderate depression [176]. Other studies confirmed that L. angustifolia oil and Linalool had antidepressant and anxiolytic potentials in experimental animal models. viz., modulates both dopaminergic and serotonergic pathways, and improves the signaling. Another study established that lavender essential oil exhibits dose-dependent specificity for NMDA receptor [177]. Nikfarjam et al. [178] confirmed in an RCT that L. officinalis, as well as venlafaxine, were effective in major depressive disorder. Another double-blind RCT study showed that M. officinalis and L. angustifolia had similar effects to fluoxetine in mild to moderate depression [179]. Liu et al. [180] reported that Rhodiola rosea extracts in the hippocampus raise the 5-HT level, promote the proliferation of neural stem cells, and repair the damaged neurons in depressive rodent models. Rhodioloside a chemical compound present in R. rosea potentially inhibits stress-induced p-SAPK/p-JNK signaling pathways, showing its anti-depressant activity. Nymphaea lotus and N. Alba (Niloufer) flowers have anxiolytic, antidepressant, antioxidant, and sedative properties.
The seed extract of C. sativum demonstrated antidepressant-like activity by interacting with adrenoceptors, GABAergic receptor and dopamine D2 receptor thereby increasing norepinephrine, dopamine and decreasing GABA levels in mice brains [181]. The whole plant of C. sativum L. (Kishneez) exhibited antianxiety, anti-epileptic, antioxidant, and anti-inflammatory properties. In the animal models of anxiety, it improved exploratory activity and restored monoamines and GABA levels, reducing excitotoxicity levels of glutamate in the hippocampus region. It contains linalool, limonene and myrcene molecules which exhibit anxiolytic activity [182]. Flower and root of Viola odorata Linn (Banafasha/Sweet Violet) exhibited anxiolytic, antidepressant, sedative, anti-inflammatory, and antioxidant properties. The V. odorata extract (100–400 mg/kg) reduced immobility time in both force swimming test (FST) and tail suspension test (TST) in male mice animal models. The bioactive molecules in V. odorata are delphinidin, P-coumaric acid, tocopherol, anthocyanin, violanin chloride, anthocyanin, rutoside, friedelin and beta-sitosterol [183]. Curcumin treatment exerted significant antidepressant activity that is equivalent to the SSRIs (fluoxetine and imipramine), renowned antidepressant drugs. In addition, it also prevents hippocampal BDNF levels from diminution in stress animal models and comparable to imipramine. Curcumin upsurges dopamine levels in the animal model (rodents) and the brain significantly reducing the properties of agents that induce a decrease in dopamine and adrenaline concentration. Hence various researches during the past decade confirmed that curcumin can control the levels of the neurotransmitter (norepinephrine, dopamine, serotonin and BDNF) that are accountable for behavior and mood regulation [184]. Furthermore, curcumin reduces pro-inflammatory cytokines gene expression, downregulates ICAM-1 and MCP-1, suppresses NFκB induction, procollagen type I, and HMGB1, cyclooxygenase-2, and tissue inhibitor of MP-1 and induces PPAR-γ and have an effect on inflammation [185]. Curcumin's bioactive molecule also possesses antioxidant activity that is interconnected which triggers many antioxidant enzyme actions including catalase, glutathione transferase, and heme-oxygenase-1 [186]. Khayat et al. [187] stated that neurotransmitters levels were increased by curcumin, as a result, improved premenstrual mood and behavioral symptoms and COX-2 enzyme were inhibited as a result reducing physical symptoms of menstruation. Crocin present in C. sativus inhibits dopamine and norepinephrine reuptake, whereas safranal inhibits the reuptake of serotonin through the NMDA receptor. Allium sativum is useful in neurodegenerative disorders instigated by oxidant-mediated brain cell mutilation, mainly Alzheimer’s [188]. In the human brain, garlic intake perhaps inhibits β-amyloid protein (Aβ) aggregation. A preclinical study in ovariectomized rats exhibited significant antidepressant properties of garlic and black sesame present in the dietary supplement [189]. Garlic, possibly reduces brain oxidative stress, hence effective in anxiety and depression behaviors in diabetic rats [190]. In addition, antidepressant-like activity was proven in a preclinical study conducted in mice, which exhibited that garlic extract inhibited MAO-A and MAO-B [191]. Fruit of Terminalia chebula Retz exhibited antidepressant and anxiolytic properties in an animal model (rodent). A study confirmed that in premenstrual mood and behavioral symptoms in women in the luteal phase, serum BDNF levels are lesser. In PMS women, treatment with Zinc supplement causes a noteworthy surge in BDNF than placebo. It has antidepressant antioxidant, and anti-inflammatory activities. It also perhaps affects inflammatory markers i.e., hs-CRP and, consequently, improves psycho-behavioral premenstrual symptoms [188]. Moreover, Zn2+ has an inhibitory role at GABA-A receptors [192]. A study confirmed that zinc increases the mRNA and BDNF protein in the hippocampus. It induces the MMP that triggers TrKP, then leads cells to release pro-BDNF and convert to BDNF. BDNF helps in the differentiation and endurance of serotonin in the neuron. In the body, Zinc also has antioxidant action and is hypothetical to counter the excess ROS and inhibits NADPH oxidase [193]. IL-10 effects on the brain and behavior and possess anti-inflammatory immune function and takes part in depression anxiety, and modulation of mood symptoms [193]. Vitamin D decreases inflammation and has antidepressant activity, as the action of 1,α, 25-dihydroxy vitamin D3 (1α, 25(OH) 2D3) is mediated through Interleukins. Vit D3 impedes IL-12 production in activated macrophages. The preliminary action of 1α, 25(OH) 2D3 is a cyclical downhearted regulation of IL-12B appearance at the beginning of inflammation, till it supports the immune rejoinder with a likely level. Moreover, a secondary action of IL-10 happens that switches off the IL-12B gene [193]. In addition, the rhizome extract also has a tranquillizing effect. Iron, zinc, magnesium, etc. micronutrients deficiency leads to depression. Polypody rhizome and wheat germ contains iron, zinc magnesium hence useful to reduce depression and other pscyho-behavioral symptoms [194].
Evidence based studies of composite formulation
Sharbat-e-Ahmed Shahi is an antidepressant Unani compound formula used for depression and insomnia. One of the ingredients is P. vulgare, the investigators testified that this compound potentially increases the availability of tryptophan, a 5HT precursor in blood and brain. Hence this compound increases 5-HT in the brain and has anxiolytic and antidepressant actions in experimental rats [195]. P. vulgare, a bioactive molecule, phytoecdysteroids possibly influence the activity of the central nervous system because of GABA-A receptor neuromodulatory action and neurotransmitter metabolism effect partially (increases the synthesis of GABA and decrease the breakdown of acetylcholine), and antioxidant properties [196]. Yasir et al. [197] investigated the effect of Sharbat Ahmad Shahi on serum BNDF levels in mild to moderate cases of depression and concluded that the formulation improved the serum BDNF level in 20 diagnosed cases of depression. Urooj et al. [198] studied animal models (rodents) and confirmed the antidepressant activity of both Majoon Najah extracts and the traditional compound Unani formulation. They concluded that antidepressant activity of Majoon Najah was exhibited because of multiple constituents present in its ingredients that possibly interact with dopaminergic adrenergic, and serotonergic receptors to result in increased levels of dopamine, norepinephrine, and serotonin with reduced GABA levels in animal brains [199]. The ingredients of the compound formulation are T. chebula Retz, T. bellerica Roxb, E. officinalis Gaertn, O. turpethum Linn, P. vulgare Linn, C. reflexa Roxb and L. stoechas Mill. A preclinical study in mice showed E. officinalis Gaertn extract (Amla) had anti-depressant activity similar to imipramine and fluoxetine [199]. Its anti-depressant potential was credited to inhibit MAO-A and GABA [199]. In an animal model (mice) T. bellirica aqueous and ethanolic extracts showed significant antidepressant-like activity by interacting with dopaminergic, adrenergic and serotonergic systems [200]. Koneru et al. [201] reported anti-depressant activity of Itrifal Kishneezi, a Unani compound formulation in Swiss albino mice, comparable with fluoxetine and imipramine. Itrifal Kishneezi contains T. chebula, T. belerica, E. officinalis, C. sativum clarified butter and honey. Zakerin’s group in an experimental study on rats investigated the antidepressant action of a polyherbal syrup containing E. amoenum, M. officinalis, L. angustifolia, Z. jujuba, A. capillus-veneris, G. glabra, F. vulgare, C. myxa, F. parviflora, and Alhagi spp. Manna [202]. They confirmed that polyherbal syrup exhibited significant antidepressant activity and caused an increased in 5 HT and NA levels in the rat without any effect on BDNF [202]. Antidepressant-like activity of G. glabra L. was investigated in mouse models and researchers concluded that G. glabra antidepressant activity appears to be facilitated by the increase of brain dopamine and norepinephrine and the inhibition of MOA [202]. Singh et al. [203] investigated the antidepressant activity of Foeniculum vulgare (fennel) fruits methanolic extract in experimental animal models. And it is concluded that F. vulgare exhibited antidepressant effects through MOA inhibitory actions. In chronic stress, in adult male mice A. capillus veneris exhibited antidepressant action [204]. Aqueous extract of M. officinalis showed antidepressant properties similar to imipramine [205]. Khamira Gawzaban Ambari Jadwar Ood Saleeb Wala is reported to possess antidepressant activity in mice. This compound formulation contains Paeonia emodi Wall. ex Royle, Althaea officinalis L., Borago officinalis L. (Flower), Melissa officinalis L. Cocoon of Bombyx mori L., Santalum álbum L., Delphinium denudatum Wall. ex Hook & T, Salvia haematodes W., Lallemantia royleana Benth., Borago officinalis L. (Leaf), Cheiranthus cheiri L., Coriandrum sativum L., Ambra grasea, silver leaves, and gold leaves. In addition, in animal model mice Khamira Gawzaban Ambari Jadwar Ood Saleeb Wala also showed improvement in learning and memory function. Sufoof Jawahar Mohra exhibited significant antidepressant activity at 12 and 24 mg/kg in FST model [206]. Lee et al. [207] summarized the therapeutic benefits of phytochemicals such as curcumin, quercetin ferulic acid, carvacrol, proanthocyanidin, L-Theanine, and resveratrol in depression.
The phytochemicals and herbs' antidepressive properties have been related to various mechanisms including monoamine neurotransmitters, HPA axis, and neurogenesis/neurotrophic factors mechanisms. Completely seems to include the promotion of neuronal cell survival and differentiation and neuronal cell apoptosis inhibition. Phytomedicine application is a possible choice for depression treatment where conventional drugs are not appropriate due to their low effectiveness and side effects. However, the investigator recommended that the safety and efficacy of above-mentioned phytochemicals for depression must be reinforced by clinical studies. Figure 6 summarizes the role of oxidative stress, mitochondrial dysfunction and inflammatory process in depression and actions of bioactive molecules of herbal medicines as antidepressant, antioxidant, and anti-inflammatory.

Depiction of the role of oxidative stress, mitochondrial dysfunction and inflammatory process in depression and actions of bioactive molecules (rosmarinic acid, luteolin, apigenin, quercetin, beta-sitosterol, anthocyanin, withanolides, withaferin-A, and valerenic acid are beneficial in depression) of herbal medicines as antidepressant, antioxidant and anti-inflammatory
Depressive moods and episodes can be a barrier to exercise, so further studies suggest making exercise plans specifically for depressed patients [208]. Psychodynamic psychotherapy treatment is required for depressed individuals as they feel losing their self-esteem. Psychotherapy helps patients stay calm and at peace with their lives [208]. Age-specific treatments still need to be conducted. Probiotics are also good in improving the symptoms of depression [209]; probiotics from the food sources such as pickles, yoghurt, and fermented products can be added to the diet of depressing patients to reduce the episode frequency and improve the severity. The anxiety symptoms can also be reduced by Omega 3 fatty acid supplementation, as in depression, the omega-six is increased, ad omega-three fatty acids are reduced [210]. It increases the severity of the disease. So, omega-three food sources such as olive oil and coconut oils can also be added to the patient's diet and supplements. The treatment for depression patients is inadequate in 50% of the cases, so a multistage treatment is proposed for depression [211]. The affected area will be studied first. Secondly, the target areas will be treated with novel antidepressants [211]. Based on the biomarkers involved, further treatment plans and diagnosis plans for depression should be made. Particular attention is required for the treatment plan of depression based on epigenetic and biochemical markers, as these markers can help target specific sites affected by depression. It is believed that such a treatment will be more effective and quick [212].
Digital help in depression is a new technique and an effective one in lowering the cases of depression. It does not require a person to visit a consultant's office, and it is both time and money-saving [213]. A suite of indelicate apps, easy to download on one's phone, offers interactive learning and psycho-educational tools. A pilot study showed positive impacts on lowering the frequency of depressive episodes [58]. The various type of treatment related to depression are mentioned in Fig. 6.
Discussion
In this review, we have integrated and reviewed the effects of depression on the human brain and cardiac systems in the relation between oxidative stress, inflammation, and mitochondrial dysfunction in depression. Further, the effects of depression on genes, proteins, and hormones in the human body were also reviewed with the major role of machine learning and deep learning in depression. In addition, we also retrieved data regarding preclinical and clinical studies conducted on various Unani single medicinal plants and composite formula plus concept for treating and diagnosing depression patients using Unani and the modern system of medicine. Further, the relationship between depression, stress, and anxiety was also comprehended.
Clinical Depression impacts the general well-being of an individual. Prolonged depression results in hippocampus atrophy, neural scars, and memory deficit. Depression affects CNS and other human body systems such as the cardiovascular, GI and reproductive systems. Oxidative stress caused by depression affects the heart, leading to cardiac hypertrophy, and decreased antioxidant defense can result in cardiac failure. As per the etiology of depression, several factors are highlighted in current reviews, such as genetic factors, hormones, HPA axis, and environmental factors [113]. Currently, depression is considered as the disease of the century as its incidence is increasing in society. Multiple treatments are available for depressive disorders, but the effectivity varies by mean of gender, socioeconomic status and co-morbidities. The use of medicinal plants are considered as a therapeutic substitute for treatment with the no or minimal side effects and treatment of depression through the action of different chemical compounds present in the structure of plants [180]. In USM, the authentic classical texts surmised single as well as composite Unani formulations effective for the treatment of psychiatric disorders including depression. Single herbs bioactive molecules such as linalool, limonene, delphinidin, P-coumaric acid, tocopherol, anthocyanin, violanin chloride, anthocyanin, rutoside, friedelin, curcumin, beta-sitosterol, bacosides A & B Brahmin, herpestine, monnierin, hersaponin, apigenin, luteolin, and myrcene are useful to treat depression, and anxiety. In addition, composite Unani formulae showed the potent action in depression such as (Sharbat-e-Ahmed Shahi, Majoon Najah, Itrefal Kishneez, Khamira Gawzaban Ambari Jadwar Ood Saleeb Wala, and Sufoof Jawahar Mohra) are proven of their efficacy and safety in preclinical and clinical studies in depression and anxiety [195, 197, 198, 201, 206]. Affirmative effects of various Unani herbs and their active compounds such as chamomile, M. officinalis, Z. jujube, S. nigrum, B. monnieri, T. terrestris, W. somnifera, sweet violet, terminalia, lavender, borage, saffron, turmeric, valerian, and Rhodiola rosea L. in mild, moderate or major depression amelioration have been reported in preclinical and clinical trials [214]. The aforementioned Unani medicinal plants show antidepressant properties and have lesser side effects than synthetic drugs. Further, many of these herbs also have anti-inflammatory, antioxidant, sedative, anxiolytic and other properties. Hence, they have the potential to treat patients with depression. Furthermore, in clinical practice, the empirical Unani formulas have been proven to have superior efficacy than single drugs, perhaps due to their reciprocated detoxification and synergistic interactions. In a composite formula, the synergy of multiple herbs triggers the interactions between herbal molecules from versatile herbs. Other anti-depressant therapies include monoamine therapy [121], Estrogen therapy in females, and congenital behavioral therapies, which can help to increase the impact of medications and help to cure the depressive disorder. Lifestyle modification has been studied and proved to prevent many health problems. In the case of depressive patients, physical activity and a healthy diet are also proven as significant factors to reduce anxiety and depressive behaviors [215]. In the pathophysiology of depression, a major challenge is lack of an assimilated database together with all interactions among the pathological aspects across biological systems, though efforts have been made to recognize the specific interactions within the CNS [216]. The mechanisms of action as per data collected, it is established that the aforementioned medicinal plants referred can modulate the brain signaling pathways responsibly for the symptoms of depression. This is accomplished with inhibition of the serotonin transporter protein or sensitization of serotonin receptors or inhibits MA, alterations in the transmission of GABAergic and/or glutamatergic transmitters, increase BDNF, effect on concentrations of serotonin in the synaptic cleft and act on dopamine. However, although these actions have been scientifically proven, considerable research is still required to confirm the safe usage of these mediators as herbal medicines in the substitute or adjunctive handling of depressive disorders [180, 217].
We designed a novel network visualization diagram based on the previously published data using VOSviewer [218] shown in Fig. 7. While, we compared the closest terms based on the network visualization techniques, published keywords, and our present study, mentioned in Fig. 8. This study will open a way to find relevant and significant work related to the depression. It would be helpful for researchers, academicians, scholars, scientists, and doctors to find out the exact work related to depression. Previously, many researchers have implemented network visualization techniques in different areas like premenstrual syndrome [49], insomnia disorder [219], bruxism disorder [220], motor imagery [27], augmented reality [221], stress [26], blockchain technology [222], and smartphone addiction [223]. In addition, some researchers used word cloud in the area of anxiety, premenstrual syndrome with oxidative stress and inflammation [49], motor imagery with deep learning [27], education with augmented reality [221], human stress with machine learning [26], cryptocurrency with blockchain technology [222], yoga with intelligence [47].

Network visualization based on a previously published article related to this study

Word cloud based on previously published keywords and this study
We compared our study with previously published reviews [224,225,226,227,228] mentioned in Table 6. We found that our study is a comprehensive effort for researchers, scientists, doctors, academicians, and scholars related to depression. It provides necessary details in multidisciplinary areas such as zoology, botany, chemistry, pharmacy, medical, psychology, food, medicine, computer, electronics, electrical, and engineering. It also covers the present, past, and future aspects to depression.
The feasibility of the results obtained from the implementation and computational point of view in the review article on depression, focusing on AI, genetics, hormones, and oxidative stress, along with detection, treatment, and effects, relies on several important considerations. First and foremost, the availability of high-quality and relevant data is crucial. The presence of comprehensive datasets comprising genetic information, hormone levels, oxidative stress markers, and depression-related data is essential for conducting robust analyses. The quality, size, and diversity of these datasets play a significant role in the reliability and generalizability of the results. From a computational perspective, the study must have access to sufficient computational power. Analyzing genetic data, applying machine learning algorithms, performing network visualizations using tools like VOSviewer, and generating word clouds can be computationally intensive tasks. Adequate processing power, memory, and storage resources are required to handle the data and implement the necessary algorithms effectively. Additionally, the development and optimization of appropriate algorithms are crucial for the feasibility of the results. Designing machine learning models, creating genetic analysis pipelines, and developing statistical methods tailored to the specific research objectives are essential. The accuracy, performance, and interpretability of these algorithms significantly impact the validity and usefulness of the obtained results. The integration and interpretation of findings from different domains, such as AI, genetics, hormones, and oxidative stress, require careful consideration. Bridging multiple disciplines and combining various sources of data necessitate expertise and collaboration between researchers. Ensuring that experts from diverse fields are involved in the analysis and interpretation processes enhances the accuracy and meaningfulness of the conclusions drawn. Moreover, feasibility of the results also relies on the ability to reproduce study's findings. Providing well-documented code, data, and methodologies allows for independent validation and replication by other researchers. Reproducibility promotes transparency and strengthens the reliability of the study's outcomes.
Research gap and future directions
There have been several proposed methods for the diagnosis of depression and treatment. Most of the studies discussed diagnosis techniques, including questionnaires conducted during self-reporting. Many multimodal approaches are in practice in extensions to this, but the outcome is poor. In contrast to time constraints and the effectiveness of diagnosis, we need to consider more robust techniques and multimodal approaches to help patients, doctors and society. In authors address [28] the lack of information on patient history and socioeconomic conditions of individual patients with different geographical locations, there is a possibility that false information is being provided by patients. Diversification of seriocomically and geographical regions are necessary inputs. Multimodal studies where biomarkers of patients with EHR data alongside various other parameters could show accurate and robust outcomes in the prediction of stages of depression, the effect of treatment, and expected outcomes. Most of the studies has discussed the techniques of diagnosis which includes questionnaires that are conducted at the time of self-reporting and in extension to this there have been many multimodal approaches in practice, but the outcome is poor. In contrast to time constraints and effectiveness of diagnosis, we need to consider more robust techniques and multimodal approaches that will help patients, doctors and society.
Our survey discussed various studies conducted to understand depression on patients’ overall quality of life. There are many challenges and gaps that can be addressed for future work starting by proposing a multimodal diagnostic approach to handle depression diagnosis. At the same time, we can think of designing new models for early diagnoses that help to increase the efficacy of treatment. The future prospects of depression research are filled with promise and potential. Researchers are actively exploring various avenues to deepen our understanding of depression and improve treatment outcomes. One key area of focus is the development of personalized medicine, where advancements in genetics and molecular biology allow for tailored treatments based on an individual's unique genetic and biological markers. This approach holds the potential to enhance treatment efficacy and minimize adverse effects. Additionally, the integration of AI and machine learning is revolutionizing the field of mental health research. AI algorithms can analyze large-scale data sets, including electronic health records, genetic profiles, and patient-reported outcomes, to identify patterns and predictors of depression. This enables the development of more accurate diagnostic tools and predictive models, which can assist healthcare professionals in making informed treatment decisions. Another emerging frontier is the exploration of novel therapeutic approaches beyond traditional medications and psychotherapy. Researchers are investigating alternative treatments such as transcranial magnetic stimulation (TMS), deep brain stimulation (DBS), and psychedelic-assisted therapies, which have shown promising results in treating depression. These innovative approaches offer new avenues for patients who have not responded well to conventional treatments. Moreover, the growing recognition of the mind–body connection has led to increased research on lifestyle interventions and holistic approaches. Techniques like mindfulness meditation, exercise, yoga, and nutritional interventions are being studied for their potential benefits in managing depression symptoms and improving overall well-being. Collaborative efforts between different scientific disciplines, including neuroscience, psychology, genetics, pharmacology, and technology, are further fueling advancements in depression research. This interdisciplinary approach fosters a comprehensive understanding of the complex mechanisms underlying depression and opens doors to innovative treatment strategies. Overall, the future of depression research is bright. As scientific knowledge expands and technology continues to advance, we can expect to see breakthroughs in personalized medicine, AI-driven diagnostics, novel therapeutics, and holistic approaches. These advancements hold the potential to transform the field, improve patient outcomes, and bring new hope to individuals living with depression.
Conclusion
This study highlights the relationship, classification, identification, recognition, effect, detection, and treatment aspects such as traditional to emerging technologies related to depression. It has also provided the research gaps and future directions for the readers to work on depression in any of the research interests like using AI in medical. Further investigation can be done to provide necessary details in a single study related to other psycho-neurological human behaviors such as anxiety and stress. Consequently, vigorous methodology, pharmacological good manufacturing practice and the use of bioengineering to certify bioequivalence of product, smart health, and bigger application of genetic knowledge, is still required to endorse assurance in this area. This manuscript has unrevealed the limitations of existing treatments and approaches. It has also provided the detailing of challenges faced in rehabilitation and treatment of Depression. Enlightening the aspects of AI that can be used in better diagnosis and treatment of depression this write-up has summarized all major tools and machine learning methods. Using the present techniques and suggested future advancements of AI can further be improved and studied in the healthcare sector especially in case of depression.
Data availability statement
Not applicable.
References
Gorlova A, Svirin E, Pavlov D, Cespuglio R, Proshin A, Schroeter CA, Lesch K-P, Strekalova T (2023) Understanding the role of oxidative stress, neuroinflammation and abnormal myelination in excessive aggression associated with depression: recent input from mechanistic studies. Int J Mol Sci 24:915. https://doi.org/10.3390/ijms24020915
Xiao X, Zhu X, Fu S, Hu Y, Li X, Xiao J (2020) Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: a multi-center cross-sectional survey investigation. J Affect Disord 274:405–410. https://doi.org/10.1016/j.jad.2020.05.081
Waseem A, Akram U, Ahmad W, Fazil M (2020) Medicinal plants used for treatment of psychiatric disorders in Unani medicine. Acta Sci Neurol 3:11–17. https://doi.org/10.31080/asne.2020.03.0189
Hasan MR, Paul BK, Ahmed K, Mahmud S, Dutta M, Hosen MS, Hassan MM, Bhuyian T (2020) Computational analysis of network model based relationship of mental disorder with depression. Biointerface Res Appl Chem 10:6293–6305. https://doi.org/10.33263/BRIAC105.62936305
Várkonyi D, Török B, Sipos E, Fazekas CL, Bánrévi K, Correia P, Chaves T, Farkas S, Szabó A, Martínez-Bellver S, Hangya B, Zelena D (2022) Investigation of anxiety- and depressive-like symptoms in 4- and 8-month-old male triple transgenic mouse models of Alzheimer’s disease. Int J Mol Sci 23:10816. https://doi.org/10.3390/ijms231810816
Galts CPC, Bettio LEB, Jewett DC, Yang CC, Brocardo PS, Rodrigues ALS, Thacker JS, Gil-Mohapel J (2019) Depression in neurodegenerative diseases: common mechanisms and current treatment options. Neurosci Biobehav Rev 102:56–84. https://doi.org/10.1016/j.neubiorev.2019.04.002
Prisnie JC, Sajobi TT, Wang M, Patten SB, Fiest KM, Bulloch AGM, Pringsheim T, Wiebe S, Jette N (2018) Effects of depression and anxiety on quality of life in five common neurological disorders. Gen Hosp Psychiatry 52:58–63. https://doi.org/10.1016/j.genhosppsych.2018.03.009
Bekhbat M, Neigh GN (2018) Sex differences in the neuro-immune consequences of stress: focus on depression and anxiety. Brain Behav Immun 67:1–12. https://doi.org/10.1016/j.bbi.2017.02.006
Evans-Lacko S, Aguilar-Gaxiola S, Al-Hamzawi A, Alonso J, Benjet C, Bruffaerts R, Chiu WT, Florescu S, De Girolamo G, Gureje O, Haro JM, He Y, Hu C, Karam EG, Kawakami N, Lee S, Lund C, Kovess-Masfety V, Levinson D, Navarro-Mateu F, Pennell BE, Sampson NA, Scott KM, Tachimori H, Ten Have M, Viana MC, Williams DR, Wojtyniak BJ, Zarkov Z, Kessler RC, Chatterji S, Thornicroft G, Al-Kaisy MS, Andrade LH, Borges G, Bromet EJ, Bunting B, Caldas De Almeida JM, Cardoso G, Cia AH, Degenhardt L, Demyttenaere K, Fayyad J, Hinkov H, Hu CY, Huang Y, De Jonge P, Karam AN, Kiejna A, Lepine JP, McGrath J, Medina-Mora ME, Moskalewicz J, Piazza M, Posada-Villa J, Slade T, Stagnaro JC, Stein DJ, Torres Y, Whiteford H, Wojtyniak B (2018) Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: Results from the WHO World Mental Health (WMH) surveys. Psychol Med 48:1560–1571. https://doi.org/10.1017/S0033291717003336
IHME (2020) Global Health Data Exchange (GHDx), Inst. Heal. Metrics Eval. http://ghdx.healthdata.org/
Kang M, Kwon H, Park JH, Kang S, Lee Y (2020) Deep-asymmetry: asymmetry matrix image for deep learning method in pre-screening depression. Sensors (Switzerland) 20:1–12. https://doi.org/10.3390/s20226526
Wang X, Chen S, Li T, Li W, Zhou Y, Zheng J, Chen Q, Yan J, Tang B (2020) Depression risk prediction for Chinese microblogs via deep-learning methods: content analysis. JMIR Med Inform 8:e17958. https://doi.org/10.2196/17958
Li X, La R, Wang Y, Hu B, Zhang X (2020) A deep learning approach for mild depression recognition based on functional connectivity using electroencephalography. Front Neurosci. https://doi.org/10.3389/fnins.2020.00192
Little B, Alshabrawy O, Stow D, Ferrier IN, McNaney R, Jackson DG, Ladha K, Ladha C, Ploetz T, Bacardit J, Olivier P, Gallagher P, O’Brien JT (2021) Deep learning-based automated speech detection as a marker of social functioning in late-life depression. Psychol Med 51:1441–1450. https://doi.org/10.1017/S0033291719003994
Thoduparambil PP, Dominic A, Varghese SM (2020) EEG-based deep learning model for the automatic detection of clinical depression. Phys Eng Sci Med 43:1349–1360. https://doi.org/10.1007/s13246-020-00938-4
Fan T, Hu Y, Xin J, Zhao M, Wang J (2020) Analyzing the genes and pathways related to major depressive disorder via a systems biology approach. Brain Behav. https://doi.org/10.1002/brb3.1502
Dipnall JF, Pasco JA, Berk M, Williams LJ, Dodd S, Jacka FN, Meyer D (2016) Into the bowels of depression: unravelling medical symptoms associated with depression by applying machine-learning techniques to a community based population sample. PLoS ONE 11:e0167055. https://doi.org/10.1371/journal.pone.0167055
Chen P, Liu Q, Wei L, Zhao B, Jia Y, Lv H, Fei X (2019) Automatically structuring on Chinese ultrasound report of cerebrovascular diseases via natural language processing. IEEE Access 7:89043–89050. https://doi.org/10.1109/ACCESS.2019.2923221
Liu Q, Xia F, Yin Q, Jiang R (2018) Chromatin accessibility prediction via a hybrid deep convolutional neural network. Bioinformatics 34:732–738. https://doi.org/10.1093/bioinformatics/btx679
Wei T, Li X, Stojanovic V (2021) Input-to-state stability of impulsive reaction–diffusion neural networks with infinite distributed delays. Nonlinear Dyn 103:1733–1755. https://doi.org/10.1007/s11071-021-06208-6
Dev A, Roy N, Islam MK, Biswas C, Ahmed HU, Amin MA, Sarker F, Vaidyanathan R, Mamun KA (2022) Exploration of EEG-based depression biomarkers identification techniques and their applications: a systematic review. IEEE Access 10:16756–16781. https://doi.org/10.1109/ACCESS.2022.3146711
Abelha M, Fernandes S, Mesquita D, Seabra F, Ferreira-Oliveira AT (2020) Graduate employability and competence development in higher education—a systematic literature review using PRISMA. Sustain 12:5900. https://doi.org/10.3390/SU12155900
Singh S, Kumar K (2020) Review of literature of lean construction and lean tools using systematic literature review technique (2008–2018). Ain Shams Eng J 11:465–471. https://doi.org/10.1016/j.asej.2019.08.012
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Teelhawod N, Akhtar F, Bin Heyat MB, Tripathi P, Mehrotra R, Asfaw AB, Al Shorman O, Masadeh M (2021) Machine learning in E-health: a comprehensive survey of anxiety. In: 2021 Int. Conf. Data Anal. Bus. Ind. ICDABI 2021. IEEE, pp 167–172.https://doi.org/10.1109/ICDABI53623.2021.9655966
Akhtar F, Bin Heyat MB, Li JP, Patel PK, Rishipal, Guragai B (2020) Role of machine learning in human stress: a review. In: 2020 17th int. comput. conf. wavelet act. media technol. inf. process. ICCWAMTIP 2020, IEEE, pp 170–174.https://doi.org/10.1109/ICCWAMTIP51612.2020.9317396
Guragai B, Alshorman O, Masadeh M, Bin Heyat MB (2020) A survey on deep learning classification algorithms for motor imagery. In: Proc. Int. Conf. Microelectron. ICM, IEEE, pp 1–4. https://doi.org/10.1109/ICM50269.2020.9331503.
de Souza Filho EM, Veiga Rey HC, Frajtag RM, Arrowsmith Cook DM, de Carvalho LND, Pinho Ribeiro AL, Amaral J (2021) Can machine learning be useful as a screening tool for depression in primary care? J Psychiatr Res 132:1–6. https://doi.org/10.1016/j.jpsychires.2020.09.025
Zhang Y, Wang S, Hermann A, Joly R, Pathak J (2021) Development and validation of a machine learning algorithm for predicting the risk of postpartum depression among pregnant women. J Affect Disord 279:1–8. https://doi.org/10.1016/j.jad.2020.09.113
Poletti S, Vai B, Mazza MG, Zanardi R, Lorenzi C, Calesella F, Cazzetta S, Branchi I, Colombo C, Furlan R, Benedetti F (2021) A peripheral inflammatory signature discriminates bipolar from unipolar depression: a machine learning approach. Prog Neuro-Psychopharmacol Biol Psychiatry. https://doi.org/10.1016/j.pnpbp.2020.110136
Pearson R, Pisner D, Meyer B, Shumake J, Beevers CG (2019) A machine learning ensemble to predict treatment outcomes following an internet intervention for depression. Psychol Med 49:2330–2341. https://doi.org/10.1017/S003329171800315X
Hochman E, Feldman B, Weizman A, Krivoy A, Gur S, Barzilay E, Gabay H, Levy J, Levinkron O, Lawrence G (2021) Development and validation of a machine learning-based postpartum depression prediction model: a nationwide cohort study. Depress Anxiety 38:400–411. https://doi.org/10.1002/da.23123
Liu Y, Admon R, Mellem MS, Belleau EL, Kaiser RH, Clegg R, Beltzer M, Goer F, Vitaliano G, Ahammad P, Pizzagalli DA (2020) Machine learning identifies large-scale reward-related activity modulated by dopaminergic enhancement in major depression. Biol Psychiatry Cogn Neurosci Neuroimaging 5:163–172. https://doi.org/10.1016/j.bpsc.2019.10.002
Kambeitz J, Goerigk S, Gattaz W, Falkai P, Benseñor IM, Lotufo PA, Bühner M, Koutsouleris N, Padberg F, Brunoni AR (2020) Clinical patterns differentially predict response to transcranial direct current stimulation (tDCS) and escitalopram in major depression: a machine learning analysis of the ELECT-TDCS study. J Affect Disord 265:460–467. https://doi.org/10.1016/j.jad.2020.01.118
Na KS, Cho SE, Geem ZW, Kim YK (2020) Predicting future onset of depression among community dwelling adults in the Republic of Korea using a machine learning algorithm. Neurosci Lett. https://doi.org/10.1016/j.neulet.2020.134804
Helbich M, Yao Y, Liu Y, Zhang J, Liu P, Wang R (2019) Using deep learning to examine street view green and blue spaces and their associations with geriatric depression in Beijing, China. Environ Int 126:107–117. https://doi.org/10.1016/j.envint.2019.02.013
Oh J, Yun K, Maoz U, Kim TS, Chae JH (2019) Identifying depression in the National Health and Nutrition Examination Survey data using a deep learning algorithm. J Affect Disord 257:623–631. https://doi.org/10.1016/j.jad.2019.06.034
Mumtaz W, Qayyum A (2019) A deep learning framework for automatic diagnosis of unipolar depression. Int J Med Inform. https://doi.org/10.1016/j.ijmedinf.2019.103983
Gui R, Chen T, Nie H (2019) The impact of emotional music on active ROI in patients with depression based on deep learning: a task-state fMRI study. Comput Intell Neurosci. https://doi.org/10.1155/2019/5850830
Schultebraucks K, Yadav V, Shalev AY, Bonanno GA, Galatzer-Levy IR (2022) Deep learning-based classification of posttraumatic stress disorder and depression following trauma utilizing visual and auditory markers of arousal and mood. Psychol Med 52:957–967. https://doi.org/10.1017/S0033291720002718
Zhang B, Wang W, Wang S, Li S, Liu M, Wang L, Yang C (2021) Clinical study on electronic medical neuroelectric stimulation based on the internet of things to treat epilepsy patients with anxiety and depression. J Healthc Eng. https://doi.org/10.1155/2021/6667309
Qayyum S, Sultana A, Bin Heyat MB, Rahman K, Akhtar F, Ul Haq A, Alkhamis BA, Alqahtani MA, Gahtani RM (2023) Therapeutic efficacy of a formulation prepared with Linum usitatissimum L., Plantago ovata Forssk., and honey on uncomplicated pelvic inflammatory disease analyzed with machine learning techniques. Pharmaceutics 15:643. https://doi.org/10.3390/pharmaceutics15020643
Ali L, He Z, Cao W, Rauf HT, Imrana Y, Bin Heyat MB (2021) MMDD-ensemble: a multimodal data-driven ensemble approach for Parkinson’s disease detection. Front Neurosci 15:1–11. https://doi.org/10.3389/fnins.2021.754058
Iqbal MS, Abbasi R, Bin Heyat MB, Akhtar F, Abdelgeliel AS, Albogami S, Fayad E, Iqbal MA (2022) Recognition of mRNA N4 acetylcytidine (ac4C) by using non-deep vs. deep learning. Appl Sci 12:1–16. https://doi.org/10.3390/app12031344
Bin Heyat MB, Akhtar F, Khan A, Noor A, Benjdira B, Qamar Y, Abbas SJ, Lai D (2020) A novel hybrid machine learning classification for the detection of bruxism patients using physiological signals. Appl Sci 10:1–16. https://doi.org/10.3390/app10217410
Bin Heyat MB, Akhtar F, Abbas SJ, Al-Sarem M, Alqarafi A, Stalin A, Abbasi R, Muaad AY, Lai D, Wu K (2022) Wearable flexible electronics based cardiac electrode for researcher mental stress detection system using machine learning models on single lead electrocardiogram signal. Biosensors 12:427. https://doi.org/10.3390/bios12060427
Pal R, Adhikari D, Bin Heyat MB, Ullah I, You Z (2023) Yoga meets intelligent internet of things: recent challenges and future directions. Bioengineering 10:459. https://doi.org/10.3390/bioengineering10040459
Bin Heyat MB, Akhtar F, Sultana A, Tumrani S, Teelhawod BN, Abbasi R, Amjad Kamal M, Muaad AY, Lai D, Wu K (2022) Role of oxidative stress and inflammation in insomnia sleep disorder and cardiovascular diseases: herbal antioxidants and anti-inflammatory coupled with insomnia detection using machine learning. Curr Pharm Des 28:3618–3636. https://doi.org/10.2174/1381612829666221201161636
Sultana A, Rahman K, Bin Heyat MB, Akhtar F, Muaad AY (2022) Role of inflammation, oxidative stress, and mitochondrial changes in premenstrual psychosomatic behavioral symptoms with anti-inflammatory, antioxidant herbs, and nutritional supplements. Oxid Med Cell Longev 2022:3599246. https://doi.org/10.1155/2022/3599246
Sultana A, Begum W, Saeedi R, Rahman K, Bin Heyat MB, Akhtar F, Son NT, Ullah H (2022) Experimental and computational approaches for the classification and correlation of temperament (Mizaj) and uterine dystemperament (Su’-I-Mizaj Al-Rahim) in abnormal vaginal discharge (Sayalan Al-Rahim) based on clinical analysis using support vector mach. Complexity 2022:1–16. https://doi.org/10.1155/2022/5718501
Koutsouleris N, Dwyer DB, Degenhardt F, Maj C, Urquijo-Castro MF, Sanfelici R, Popovic D, Oeztuerk O, Haas SS, Weiske J, Ruef A, Kambeitz-Ilankovic L, Antonucci LA, Neufang S, Schmidt-Kraepelin C, Ruhrmann S, Penzel N, Kambeitz J, Haidl TK, Rosen M, Chisholm K, Riecher-Rössler A, Egloff L, Schmidt A, Andreou C, Hietala J, Schirmer T, Romer G, Walger P, Franscini M, Traber-Walker N, Schimmelmann BG, Flückiger R, Michel C, Rössler W, Borisov O, Krawitz PM, Heekeren K, Buechler R, Pantelis C, Falkai P, Salokangas RKR, Lencer R, Bertolino A, Borgwardt S, Noethen M, Brambilla P, Wood SJ, Upthegrove R, Schultze-Lutter F, Theodoridou A, Meisenzahl E (2021) Multimodal machine learning workflows for prediction of psychosis in patients with clinical high-risk syndromes and recent-onset depression. JAMA Psychiat 78:195–209. https://doi.org/10.1001/jamapsychiatry.2020.3604
Byeon H (2020) Development of a depression in Parkinson’s disease prediction model using machine learning. World J Psychiatry 10:234–244. https://doi.org/10.5498/wjp.v10.i10.234
Richter T, Fishbain B, Markus A, Richter-Levin G, Okon-Singer H (2020) Using machine learning-based analysis for behavioral differentiation between anxiety and depression. Sci Rep. https://doi.org/10.1038/s41598-020-72289-9
van Bronswijk SC, Bruijniks SJE, Lorenzo-Luaces L, Derubeis RJ, Lemmens LHJM, Peeters FPML, Huibers MJH (2021) Cross-trial prediction in psychotherapy: external validation of the personalized advantage index using machine learning in two Dutch randomized trials comparing CBT versus IPT for depression. Psychother Res 31:78–91. https://doi.org/10.1080/10503307.2020.1823029
Shin D, Lee KJ, Adeluwa T, Hur J (2020) Machine learning-based predictive modeling of postpartum depression. J Clin Med 9:1–14. https://doi.org/10.3390/jcm9092899
Németh R, Sik D, Máté F (2020) Machine learning of concepts hard even for humans: the case of online depression forums. Int J Qual Methods. https://doi.org/10.1177/1609406920949338
Benfares C, Akhrif O, El Idrissi YEB, Hamid K (2021) A clinical support system for classification and prediction of depression using machine learning methods. Comput Intell 37:1619–1632. https://doi.org/10.1111/coin.12377
Qi B, Fiori LM, Turecki G, Trakadis YJ (2020) Machine learning analysis of blood microRNA data in major depression: a case-control study for biomarker discovery. Int J Neuropsychopharmacol 23:505–510. https://doi.org/10.1093/ijnp/pyaa029
Alsagri HS, Ykhlef M (2020) Machine learning-based approach for depression detection in twitter using content and activity features. IEICE Trans Inf Syst E 103D:1825–1832. https://doi.org/10.1587/transinf.2020EDP7023
Solomonov N, Lee J, Banerjee S, Flückiger C, Kanellopoulos D, Gunning FM, Sirey JA, Liston C, Raue PJ, Hull TD, Areán PA, Alexopoulos GS (2021) Modifiable predictors of nonresponse to psychotherapies for late-life depression with executive dysfunction: a machine learning approach. Mol Psychiatry 26:5190–5198. https://doi.org/10.1038/s41380-020-0836-z
Tennenhouse LG, Marrie RA, Bernstein CN, Lix LM (2020) Machine-learning models for depression and anxiety in individuals with immune-mediated inflammatory disease. J Psychosom Res. https://doi.org/10.1016/j.jpsychores.2020.110126
Rajpurkar P, Yang J, Dass N, Vale V, Keller AS, Irvin J, Taylor Z, Basu S, Ng A, Williams LM (2020) Evaluation of a machine learning model based on pretreatment symptoms and electroencephalographic features to predict outcomes of antidepressant treatment in adults with depression: a prespecified secondary analysis of a randomized clinical trial. JAMA Netw Open. https://doi.org/10.1001/jamanetworkopen.2020.6653
Shatte ABR, Hutchinson DM, Fuller-Tyszkiewicz M, Teague SJ (2020) Social media markers to identify fathers at risk of postpartum depression: a machine learning approach. Cyberpsychol Behav Soc Netw 23:611–618. https://doi.org/10.1089/cyber.2019.0746
Helbich M, Hagenauer J, Roberts H (2020) Relative importance of perceived physical and social neighborhood characteristics for depression: a machine learning approach. Soc Psychiatry Psychiatr Epidemiol 55:599–610. https://doi.org/10.1007/s00127-019-01808-5
Razavi R, Gharipour A, Gharipour M (2020) Depression screening using mobile phone usage metadata: a machine learning approach. J Am Med Inform Assoc 27:522–530. https://doi.org/10.1093/jamia/ocz221
Zhang W, Liu H, Silenzio VMB, Qiu P, Gong W (2020) Machine learning models for the prediction of postpartum depression: application and comparison based on a cohort study. JMIR Med Inform. https://doi.org/10.2196/15516
Yang Z, Chen C, Li H, Yao L, Zhao X (2020) Unsupervised classifications of depression levels based on machine learning algorithms perform well as compared to traditional norm-based classifications. Front Psychiatry. https://doi.org/10.3389/fpsyt.2020.00045
Zhdanov A, Atluri S, Wong W, Vaghei Y, Daskalakis ZJ, Blumberger DM, Frey BN, Giacobbe P, Lam RW, Milev R, Mueller DJ, Turecki G, Parikh SV, Rotzinger S, Soares CN, Brenner CA, Vila-Rodriguez F, McAndrews MP, Kleffner K, Alonso-Prieto E, Arnott SR, Foster JA, Strother SC, Uher R, Kennedy SH, Farzan F (2020) Use of machine learning for predicting escitalopram treatment outcome from electroencephalography recordings in adult patients with depression. JAMA Netw Open 3:e1918377. https://doi.org/10.1001/jamanetworkopen.2019.18377
Zhao M, Feng Z (2020) Machine learning methods to evaluate the depression status of Chinese recruits: a diagnostic study. Neuropsychiatr Dis Treat 16:2743–2752. https://doi.org/10.2147/NDT.S275620
Aguilera A, Figueroa CA, Hernandez-Ramos R, Sarkar U, Cemballi A, Gomez-Pathak L, Miramontes J, Yom-Tov E, Chakraborty B, Yan X, Xu J, Modiri A, Aggarwal J, Jay Williams J, Lyles CR (2020) MHealth app using machine learning to increase physical activity in diabetes and depression: clinical trial protocol for the DIAMANTE Study. BMJ Open. https://doi.org/10.1136/bmjopen-2019-034723
Delgadillo J, Salas Duhne PG (2020) Targeted prescription of cognitive-behavioral therapy versus person-centered counseling for depression using a machine learning approach. J Consult Clin Psychol 88:14–24. https://doi.org/10.1037/ccp0000476
Cui L, Wang C, Wu Z, Peng D, Huang J, Zhang C, Huang J, Hong W, Wang Y, Chen J, Liu T, Rong H, Yang H, Fang Y (2020) Symptomatology differences of major depression in psychiatric versus general hospitals: a machine learning approach. J Affect Disord 260:349–360. https://doi.org/10.1016/j.jad.2019.09.030
Wollenhaupt-Aguiar B, Librenza-Garcia D, Bristot G, Przybylski L, Stertz L, Kubiachi Burque R, Ceresér KM, Spanemberg L, Caldieraro MA, Frey BN, Fleck MP, Kauer-Sant’Anna M, Cavalcante Passos I, Kapczinski F (2020) Differential biomarker signatures in unipolar and bipolar depression: a machine learning approach. Aust N Z J Psychiatry 54:393–401. https://doi.org/10.1177/0004867419888027
McGinnis EW, Anderau SP, Hruschak J, Gurchiek RD, Lopez-Duran NL, Fitzgerald K, Rosenblum KL, Muzik M, McGinnis RS (2019) Giving voice to vulnerable children: machine learning analysis of speech detects anxiety and depression in early childhood. IEEE J Biomed Heal Inform 23:2294–2301. https://doi.org/10.1109/JBHI.2019.2913590
Kim H, Lee SH, Lee SE, Hong S, Kang HJ, Kim N (2019) Depression prediction by using ecological momentary assessment, actiwatch data, and machine learning: observational study on older adults living alone. JMIR MHealth UHealth. https://doi.org/10.2196/14149
Gong J, Simon GE, Liu S (2019) Machine learning discovery of longitudinal patterns of depression and suicidal ideation. PLoS ONE. https://doi.org/10.1371/journal.pone.0222665
Besteher B, Gaser C, Nenadić I (2019) Machine-learning based brain age estimation in major depression showing no evidence of accelerated aging. Psychiatry Res Neuroimaging 290:1–4. https://doi.org/10.1016/j.pscychresns.2019.06.001
Li X, Zhang X, Zhu J, Mao W, Sun S, Wang Z, Xia C, Hu B (2019) Depression recognition using machine learning methods with different feature generation strategies. Artif Intell Med. https://doi.org/10.1016/j.artmed.2019.07.004
Fatima I, Abbasi BUD, Khan S, Al-Saeed M, Ahmad HF, Mumtaz R (2019) Prediction of postpartum depression using machine learning techniques from social media text. Expert Syst. https://doi.org/10.1111/exsy.12409
Kasthurirathne SN, Biondich PG, Grannis SJ, Purkayastha S, Vest JR, Jones JF (2019) Identification of patients in need of advanced care for depression using data extracted from a statewide health information exchange: a machine learning approach. J Med Internet Res. https://doi.org/10.2196/13809
Zandvakili A, Philip NS, Jones SR, Tyrka AR, Greenberg BD, Carpenter LL (2019) Use of machine learning in predicting clinical response to transcranial magnetic stimulation in comorbid posttraumatic stress disorder and major depression: a resting state electroencephalography study. J Affect Disord 252:47–54. https://doi.org/10.1016/j.jad.2019.03.077
Zhao K, So HC (2019) Drug repositioning for schizophrenia and depression/anxiety disorders: a machine learning approach leveraging expression data. IEEE J Biomed Health Inform 23:1304–1315. https://doi.org/10.1109/JBHI.2018.2856535
Dinga R, Marquand AF, Veltman DJ, Beekman ATF, Schoevers RA, van Hemert AM, Penninx BWJH, Schmaal L (2018) Predicting the naturalistic course of depression from a wide range of clinical, psychological, and biological data: a machine learning approach. Transl Psychiatry. https://doi.org/10.1038/s41398-018-0289-1
Wallert J, Gustafson E, Held C, Madison G, Norlund F, Von Essen L, Olsson EMG (2018) Predicting adherence to internet-Delivered psychotherapy for symptoms of depression and anxiety after myocardial infarction: machine learning insights from the U-CARE heart randomized controlled trial. J Med Internet Res. https://doi.org/10.2196/10754
Zilcha-Mano S, Roose SP, Brown PJ, Rutherford BR (2018) A machine learning approach to identifying placebo responders in late-life depression trials. Am J Geriatr Psychiatry 26:669–677. https://doi.org/10.1016/j.jagp.2018.01.001
Kautzky A, Dold M, Bartova L, Spies M, Vanicek T, Souery D, Montgomery S, Mendlewicz J, Zohar J, Fabbri C, Serretti A, Lanzenberger R, Kasper S (2018) Refining prediction in treatment-resistant depression: results of machine learning analyses in the TRD III sample. J Clin Psychiatry. https://doi.org/10.4088/JCP.16m11385
Hilbert K, Lueken U, Muehlhan M, Beesdo-Baum K (2017) Separating generalized anxiety disorder from major depression using clinical, hormonal, and structural MRI data: a multimodal machine learning study. Brain Behav. https://doi.org/10.1002/brb3.633
Dipnall JF, Pasco JA, Berk M, Williams LJ, Dodd S, Jacka FN, Meyer D (2017) Why so GLUMM? Detecting depression clusters through graphing lifestyle-environs using machine-learning methods (GLUMM). Eur Psychiatry 39:40–50. https://doi.org/10.1016/j.eurpsy.2016.06.003
Cvetković J (2017) Breast cancer patients’ depression prediction by machine learning approach. Cancer Invest 35:569–572. https://doi.org/10.1080/07357907.2017.1363892
Mehltretter J, Rollins C, Benrimoh D, Fratila R, Perlman K, Israel S, Miresco M, Wakid M, Turecki G (2020) Analysis of features selected by a deep learning model for differential treatment selection in depression. Front Artif Intell. https://doi.org/10.3389/frai.2019.00031
Lin E, Kuo PH, Liu YL, Yu YWY, Yang AC, Tsai SJ (2018) A deep learning approach for predicting antidepressant response in major depression using clinical and genetic biomarkers. Front Psychiatry. https://doi.org/10.3389/fpsyt.2018.00290
Jawad K, Mahto R, Das A, Ahmed SU, Aziz RM, Kumar P (2023) Novel cuckoo search-based metaheuristic approach for deep learning prediction of depression. Appl Sci 13:5322. https://doi.org/10.3390/app13095322
Black CN, Bot M, Scheffer PG, Cuijpers P, Penninx BWJH (2015) Is depression associated with increased oxidative stress? A systematic review and meta-analysis. Psychoneuroendocrinology 51:164–175. https://doi.org/10.1016/j.psyneuen.2014.09.025
Uliaszek AA, Zinbarg RE, Mineka S, Craske MG, Sutton JM, Griffith JW, Rose R, Waters A, Hammen C (2010) The role of neuroticism and extraversion in the stress-anxiety and stress-depression relationships. Anxiety Stress Coping 23:363–381. https://doi.org/10.1080/10615800903377264
Basavanthappa B (2011) Essentials of mental health nursing. https://doi.org/10.5005/jp/books/11321
Jacobson NS, Dobson KS, Truax PA, Addis ME, Koerner K, Gollan JK, Gortner E, Prince SE (1996) A component analysis of cognitive—behavioral treatment for depression. J Consult Clin Psychol 64:295–304. https://doi.org/10.1037/0022-006X.64.2.295
Salustri C, Squitti R, Zappasodi F, Ventriglia M, Bevacqua MG, Fontana M, Tecchio F (2010) Oxidative stress and brain glutamate-mediated excitability in depressed patients. J Affect Disord 127:321–325. https://doi.org/10.1016/j.jad.2010.05.012
Cho Y, Lee JK, Kim DH, Park JH, Choi M, Kim HJ, Nam MJ, Lee KU, Han K, Park YG (2019) Factors associated with quality of life in patients with depression: a nationwide population-based study. PLoS ONE 14:e0219455. https://doi.org/10.1371/journal.pone.0219455
Yang L, Zhao Y, Wang Y, Liu L, Zhang X, Li B, Cui R (2015) The effects of psychological stress on depression. Curr Neuropharmacol 13:494–504. https://doi.org/10.2174/1570159x1304150831150507
Wirtz PH, von Känel R (2017) Psychological stress, inflammation, and coronary heart disease. Curr Cardiol Rep 19:111. https://doi.org/10.1007/s11886-017-0919-x
Hamon M, Blier P (2013) Monoamine neurocircuitry in depression and strategies for new treatments. Prog Neuro-Psychopharmacol Biol Psychiatry 45:54–63. https://doi.org/10.1016/j.pnpbp.2013.04.009
Maletic V, Eramo A, Gwin K, Offord SJ, Duffy RA (2017) The role of norepinephrine and its α-adrenergic receptors in the pathophysiology and treatment of major depressive disorder and schizophrenia: a systematic review. Front Psychiatry. https://doi.org/10.3389/fpsyt.2017.00042
Gold PW, Wong ML (2021) Re-assessing the catecholamine hypothesis of depression: the case of melancholic depression. Mol Psychiatry 26:6121–6124. https://doi.org/10.1038/s41380-021-01133-x
Peacock BN, Scheiderer DJ, Kellermann GH (2017) Biomolecular aspects of depression: a retrospective analysis. Compr Psychiatry 73:168–180. https://doi.org/10.1016/j.comppsych.2016.11.002
Hernández-Hernández OT, Martínez-Mota L, Herrera-Pérez JJ, Jiménez-Rubio G (2018) Role of estradiol in the expression of genes involved in serotonin neurotransmission: implications for female depression. Curr Neuropharmacol 17:459–471. https://doi.org/10.2174/1570159x16666180628165107
Labonté B, Engmann O, Purushothaman I, Menard C, Wang J, Tan C, Scarpa JR, Moy G, Loh YHE, Cahill M, Lorsch ZS, Hamilton PJ, Calipari ES, Hodes GE, Issler O, Kronman H, Pfau M, Obradovic ALJ, Dong Y, Neve RL, Russo S, Kazarskis A, Tamminga C, Mechawar N, Turecki G, Zhang B, Shen L, Nestler EJ (2017) Sex-specific transcriptional signatures in human depression. Nat Med 23:1102–1111. https://doi.org/10.1038/nm.4386
Weng TT, Hao JH, Qian QW, Cao H, Fu JL, Sun Y, Huang L, Tao FB (2012) Is there any relationship between dietary patterns and depression and anxiety in Chinese adolescents? Public Health Nutr 15:673–682. https://doi.org/10.1017/S1368980011003077
Finger BC, Dinan TG, Cryan JF (2011) High-fat diet selectively protects against the effects of chronic social stress in the mouse. Neuroscience 192:351–360. https://doi.org/10.1016/j.neuroscience.2011.06.072
Werner A (2004) Psychodynamic treatment of depression. Am J Psychiatry 161:2146–2146. https://doi.org/10.1176/appi.ajp.161.11.2146
Kim KH (2021) Level of troponin release can aid in early exclusion of stress-induced (Takotsubo) cardiomyopathy. J Cardiovasc Imaging 29:234–235. https://doi.org/10.4250/jcvi.2021.0076
Mohr DC, Tomasino KN, Lattie EG, Palac HL, Kwasny MJ, Weingardt K, Karr CJ, Kaiser SM, Rossom RC, Bardsley LR, Caccamo L, Stiles-Shields C, Schueller SM (2017) Intellicare: an eclectic, skills-based app suite for the treatment of depression and anxiety. J Med Internet Res. https://doi.org/10.2196/jmir.6645
Robinson SD, Lee TW, Christie DL, Birch NP (2015) Tissue plasminogen activator inhibits NMDA-receptor-mediated increases in calcium levels in cultured hippocampal neurons. Front Cell Neurosci. https://doi.org/10.3389/fncel.2015.00404
Cowen PJ (2010) Not fade away: the HPA axis and depression. Psychol Med 40:1–4. https://doi.org/10.1017/S0033291709005558
Wallace CJK, Foster JA, Soares CN, Milev RV (2020) The effects of probiotics on symptoms of depression: protocol for a double-blind randomized placebo-controlled trial. Neuropsychobiology 79:108–116. https://doi.org/10.1159/000496406
McEwen BS (1999) Stress and hippocampal plasticity. Annu Rev Neurosci 22:105–122. https://doi.org/10.1146/annurev.neuro.22.1.105
Bremner JD, Narayan M, Anderson ER, Staib LH, Miller HL, Charney DS (2000) Hippocampal volume reduction in major depression. Am J Psychiatry 157:115–117. https://doi.org/10.1176/ajp.157.1.115
Bitsko RH, Holbrook JR, Ghandour RM, Blumberg SJ, Visser SN, Perou R, Walkup JT (2018) Epidemiology and impact of health care provider-diagnosed anxiety and depression among US children. J Dev Behav Pediatr 39:395–403. https://doi.org/10.1097/DBP.0000000000000571
Schmidt PJ (2005) Depression, the perimenopause, and estrogen therap. Ann N Y Acad Sci. https://doi.org/10.1196/annals.1347.003
Sramek JJ, Cutler NR (2011) The impact of gender on antidepressants. Curr Top Behav Neurosci 8:231–249. https://doi.org/10.1007/7854_2010_118
Emeny RT, Bidlingmaier M, Lacruz ME, Linkohr B, Peters A, Reincke M, Ladwig KH (2014) Mind over hormones: sex differences in associations of well-being with IGF-I, IGFBP-3 and physical activity in the KORA-Age study. Exp Gerontol 59:58–64. https://doi.org/10.1016/j.exger.2014.08.001
Thase ME, Trivedi MH, Rush AJ (1995) MAOIs in the contemporary treatment of depression. Neuropsychopharmacology 12:185–219. https://doi.org/10.1016/0893-133X(94)00058-8
Penninx BWJH, Geerlings SW, Deeg DJH, Van Eijk JTM, Van Tilburg W, Beekman ATF (1999) Minor and major depression and the risk of death in older persons. Arch Gen Psychiatry 56:889–895. https://doi.org/10.1001/archpsyc.56.10.889
Ramaker RC, Bowling KM, Lasseigne BN, Hagenauer MH, Hardigan AA, Davis NS, Gertz J, Cartagena PM, Walsh DM, Vawter MP, Schatzberg AF, Barchas JD, Watson SJ, Bunney BG, Akil H, Bunney WE, Li JZ, Cooper SJ, Myers RM (2017) Post-mortem molecular profiling of three psychiatric disorders. Genome Med 9:72. https://doi.org/10.1186/s13073-017-0458-5
Abraham J, Mudd JO, Kapur N, Klein K, Champion HC, Wittstein IS (2009) Stress cardiomyopathy after intravenous administration of catecholamines and beta-receptor agonists. J Am Coll Cardiol 53:1320–1325. https://doi.org/10.1016/j.jacc.2009.02.020
Stefanatou A, Kouris N, Lekakis J (2010) Treatment of depression in elderly patients with cardiovascular disease: research data and future prospects. Hellenic J Cardiol 51:142–152
Morava E, Gardeitchik T, Kozicz T, de Boer L, Koene S, de Vries MC, McFarland R, Roobol T, Rodenburg RJT, Verhaak CM (2010) Depressive behaviour in children diagnosed with a mitochondrial disorder. Mitochondrion 10:528–533. https://doi.org/10.1016/j.mito.2010.05.011
Gardner A, Johansson A, Wibom R, Nennesmo I, Von Döbeln U, Hagenfeldt L, Hällström T (2003) Alterations of mitochondrial function and correlations with personality traits in selected major depressive disorder patients. J Affect Disord 76:55–68. https://doi.org/10.1016/S0165-0327(02)00067-8
Bansal Y, Kuhad A (2016) Mitochondrial Dysfunction in Depression. Curr Neuropharmacol 14:610–618. https://doi.org/10.2174/1570159x14666160229114755
Zhang D, Wen X, Wang X, Shi M, Zhao Y (2009) Antidepressant effect of Shudihuang on mice exposed to unpredictable chronic mild stress. J Ethnopharmacol 123:55–60. https://doi.org/10.1016/j.jep.2009.02.029
Bagdy G, Juhasz G, Gonda X (2012) A depresszió új, bizonyítékokon alapuló gén-környezet interakciós modellje. Neuropsychopharmacol Hungarica 14:213–220. https://doi.org/10.5706/nph201212001
Pawlak R, Rao BSS, Melchor JP, Chattarji S, McEwen B, Strickland S (2005) Tissue plasminogen activator and plasminogen mediate stress-induced decline of neuronal and cognitive functions in the mouse hippocampus. Proc Natl Acad Sci USA 102:18201–18206. https://doi.org/10.1073/pnas.0509232102
Ryder AL, Cohen BE (2021) Evidence for depression and anxiety as risk factors for heart disease and stroke: implications for primary care. Fam Pract 38:365–367. https://doi.org/10.1093/fampra/cmab031
Dunn AL, Trivedi MH, Kampert JB, Clark CG, Chambliss HO (2005) Exercise treatment for depression: efficacy and dose response. Am J Prev Med 28:1–8. https://doi.org/10.1016/j.amepre.2004.09.003
Maes M (2001) Psychological stress and the inflammatory response system. Clin Sci 101:193–194. https://doi.org/10.1042/CS20010157
Cuijpers P, Quero S, Dowrick C, Arroll B (2019) Psychological treatment of depression in primary care: recent developments. Curr Psychiatry Rep 21:129. https://doi.org/10.1007/s11920-019-1117-x
Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B (2016) Exercise as a treatment for depression: a meta-analysis adjusting for publication bias. J Psychiatr Res 77:42–51. https://doi.org/10.1016/j.jpsychires.2016.02.023
Kiecolt-Glaser JK, Belury MA, Andridge R, Malarkey WB, Glaser R (2011) Omega-3 supplementation lowers inflammation and anxiety in medical students: a randomized controlled trial. Brain Behav Immun 25:1725–1734. https://doi.org/10.1016/j.bbi.2011.07.229
Hill MF, Singal PK (1996) Antioxidant and oxidative stress changes during heart failure subsequent to myocardial infarction in rats. Am J Pathol 148:291–300
Cheng S, Zhu Z, Li H, Wang W, Jiang Z, Pan F, Liu D, Ho RCM, Ho CSH (2023) Rifaximin ameliorates depression-like behaviour in chronic unpredictable mild stress rats by regulating intestinal microbiota and hippocampal tryptophan metabolism. J Affect Disord. https://doi.org/10.1016/j.jad.2023.02.086
O’Neill M (2001) Role of 5-HT1A and 5-HT1B receptors in the mediation of behavior in the forced swim test in mice. Neuropsychopharmacology 24:391–398. https://doi.org/10.1016/S0893-133X(00)00196-2
Giannakakis A, Zhang J, Jenjaroenpun P, Nama S, Zainolabidin N, Aau MY, Yarmishyn AA, Vaz C, Ivshina AV, Grinchuk OV, Voorhoeve M, Vardy LA, Sampath P, Kuznetsov VA, Kurochkin IV, Guccione E (2015) Contrasting expression patterns of coding and noncoding parts of the human genome upon oxidative stress. Sci Rep. https://doi.org/10.1038/srep09737
John S (2020) Hormones and depression in women. Insights Depress Anxiety 4:064–065. https://doi.org/10.29328/journal.ida.1001022
Kvam S, Kleppe CL, Nordhus IH, Hovland A (2016) Exercise as a treatment for depression: a meta-analysis. J Affect Disord 202:67–86. https://doi.org/10.1016/j.jad.2016.03.063
Danner M, Kasl SV, Abramson JL, Vaccarino V (2003) Association between depression and elevated C-reactive protein. Psychosom Med 65:347–356. https://doi.org/10.1097/01.PSY.0000041542.29808.01
Wu PL, Lee M, Huang TT (2017) Effectiveness of physical activity on patients with depression and Parkinson’s disease: a systematic review. PLoS ONE 12:1–14. https://doi.org/10.1371/journal.pone.0181515
Imboden C, Gerber M, Beck J, Eckert A, Pühse U, Holsboer-Trachsler E, Hatzinger M (2019) Effects of aerobic exercise as add-on treatment for inpatients with moderate to severe depression on depression severity, sleep, cognition, psychological well-being, and biomarkers: study protocol, description of study population, and manipulation check. Front Psychiatry. https://doi.org/10.3389/fpsyt.2019.00262
Mao X, Terpolilli NA, Wehn A, Cheng S, Hellal F, Liu B, Seker B, Plesnila N (2020) Progressive histopathological damage occurring up to one year after experimental traumatic brain injury is associated with cognitive decline and depression-like behavior. J Neurotrauma 37:1331–1341. https://doi.org/10.1089/neu.2019.6510
Amr SS, Tbakhi A (2007) Ibn Sina (Avicenna): the prince of physicians. Ann Saudi Med 27:134–135. https://doi.org/10.5144/0256-4947.2007.134
Suomalainen K (2018) Sinä, konteksti ja monitulkintaisuus. Virittäjä. https://doi.org/10.23982/vir.63686
Kökcü A (2019) İbn Sina ve İhvan-ı Safa Bağlamında Matematikten Metafiziğe Sayı ve Nicelik Algısı. Beytulhikme Int J Philos 9:59–74. https://doi.org/10.18491/beytulhikme.1438
Johnson D, Letchumanan V, Thum CC, Thurairajasingam S, Lee L-H (2023) A microbial-based approach to mental health: the potential of probiotics in the treatment of depression. Nutrients. https://doi.org/10.3390/nu15061382
Derakhshan AR (2017) Natural treatments for fissure in Ano used by traditional persian scholars, Razi (Rhazes) and Ibn Sina (Avicenna). J Evid Based Complement Altern Med 22:324–333. https://doi.org/10.1177/2156587216650302
I. translation by K.G. Sina (2010) Al Qanoon fit Tibb, Idarae Kitabus Shifa, New Dilhi
Anwar N, Ahmed NZ, Shahida T, Kabiruddin K, Aslam H (2017) The role of Mufarrehat (Exhilarants) in the management of depression: an evidence based approach. J Psychiatry. https://doi.org/10.4172/2378-5756.1000420
Khambaty M, Parikh RM (2017) Cultural aspects of anxiety disorders in India. Dialogues Clin Neurosci 19:117–126. https://doi.org/10.31887/dcns.2017.19.2/rparikh
Ahmed NZ, Alam A, Khalid M, Sheeraz M, Qamri MA (2015) An insight on Malankholia (Melancholia): Unani perspective. Med J Islam World Acad Sci 23:140–146. https://doi.org/10.5505/ias.2015.58076
Sarris J, Panossian A, Schweitzer I, Stough C, Scholey A (2011) Herbal medicine for depression, anxiety and insomnia: a review of psychopharmacology and clinical evidence. Eur Neuropsychopharmacol 21:841–860. https://doi.org/10.1016/j.euroneuro.2011.04.002
Yeung AWK, Georgieva MG, Atanasov AG, Tzvetkov NT (2019) Monoamine oxidases (MAOs) as privileged molecular targets in neuroscience: research literature analysis. Front Mol Neurosci. https://doi.org/10.3389/fnmol.2019.00143
Naoi M, Shamoto-Nagai M, Maruyama W (2019) Neuroprotection of multifunctional phytochemicals as novel therapeutic strategy for neurodegenerative disorders: antiapoptotic and antiamyloidogenic activities by modulation of cellular signal pathways. Future Neurol 14:FNL9. https://doi.org/10.2217/fnl-2018-0028
Sofiane G, Wafa N, Ouarda D (2015) Antioxidant, antimicrobial and anti-inflammatory activities of flavonoids and tannins extracted from Polypodium vulgare L. Asian J Biochem Pharm Res 5:114–122
Allen J, Romay-Tallon R, Brymer KJ, Caruncho HJ, Kalynchuk LE (2018) Mitochondria and mood: mitochondrial dysfunction as a key player in the manifestation of depression. Front Neurosci 12:1–13. https://doi.org/10.3389/fnins.2018.00386
Khan AW, Khan AU, Shah SMM, Ullah A, Faheem M, Saleem M (2019) An updated list of neuromedicinal plants of Pakistan, their uses, and phytochemistry. Evid Based Complement Altern Med 2019:1–27. https://doi.org/10.1155/2019/6191505
Yeung KS, Hernandez M, Mao JJ, Haviland I, Gubili J (2018) Herbal medicine for depression and anxiety: a systematic review with assessment of potential psycho-oncologic relevance. Phyther Res 32:865–891. https://doi.org/10.1002/ptr.6033
Wang S, Zhang J, Zhang Z, Gao W, Yan Y, Li X, Liu C (2014) Identification of chemical constituents in the extract and rat serum from Ziziphus jujuba mill. by HPLC-PDA-ESI-MSn. Iran J Pharm Res 13:1055–1064
Mannan MA, Abir AB, Rahman MR (2015) Antidepressant-like effects of methanolic extract of Bacopa monniera in mice. BMC Complement Altern Med 15:337. https://doi.org/10.1186/s12906-015-0866-2
Wang Z, Zhang D, Hui S, Zhang Y, Hu S (2013) Effect of Tribulus terrestris saponins on behavior and neuroendocrine in chronic mild stress depression rats. J Tradit Chin Med 33:228–232. https://doi.org/10.1016/s0254-6272(13)60130-2
Bhattacharya SK, Bhattacharya A, Sairam K, Ghosal S (2000) Anxiolytic-antidepressant activity of Withania somnifera glycowithanolides: an experimental study. Phytomedicine 7:463–469. https://doi.org/10.1016/S0944-7113(00)80030-6
Müller D, Pfeil T, Von den Driesch V (2003) Treating depression comorbid with anxiety—results of an open, practice-oriented study with St John’s wort WS® 5572 and valerian extract in high doses. Phytomedicine 10:25–30. https://doi.org/10.1078/1433-187X-00305
Ahmadi M, Khalili H, Abbasian L, Ghaeli P (2017) Effect of valerian in preventing neuropsychiatric adverse effects of efavirenz in HIV-positive patients: a pilot randomized, placebo-controlled clinical trial. Ann Pharmacother 51:457–464. https://doi.org/10.1177/1060028017696105
Amsterdam JD, Shults J, Soeller I, Mao JJ, Rockwell K, Newberg AB (2012) Chamomile (Matricaria recutita) may provide antidepressant activity in anxious, depressed humans: an exploratory study. Altern Ther Health Med 18:44–49
Chang SM, Chen CH (2016) Effects of an intervention with drinking chamomile tea on sleep quality and depression in sleep disturbed postnatal women: a randomized controlled trial. J Adv Nurs 72:306–315. https://doi.org/10.1111/jan.12836
Komaki A, Rasouli B, Shahidi S (2015) Anxiolytic effect of Borago officinalis (Boraginaceae) extract in male rats. Avicenna J Neuro Psych Physiol. https://doi.org/10.17795/ajnpp-27189
Sayyah M, Sayyah M, Kamalinejad M (2006) A preliminary randomized double blind clinical trial on the efficacy of aqueous extract of Echium amoenum in the treatment of mild to moderate major depression. Prog Neuro-Psychopharmacol Biol Psychiatry 30:166–169. https://doi.org/10.1016/j.pnpbp.2005.10.005
Farahmand M, Khalili D, Ramezani Tehrani F, Amin G, Negarandeh R (2020) Effectiveness of Echium amoenum on premenstrual syndrome: a randomized, double-blind, controlled trial. BMC Complement Med Ther 20:295. https://doi.org/10.1186/s12906-020-03084-2
Farahmand M, Khalili D, Ramezani Tehrani F, Amin G, Negarandeh R (2021) Could anise decrease the intensity of premenstrual syndrome symptoms in comparison to placebo? A double-blind randomized clinical trial. J Complement Integr Med 17:1–10. https://doi.org/10.1515/jcim-2019-0077
Akhondzadeh S, Kashani L, Fotouhi A, Jarvandi S, Mobaseri M, Moin M, Khani M, Jamshidi AH, Baghalian K, Taghizadeh M (2003) Comparison of Lavandula angustifolia Mill. tincture and imipramine in the treatment of mild to moderate depression: a double-blind, randomized trial. Prog Neuro-Psychopharmacol Biol Psychiatry 27:123–127. https://doi.org/10.1016/S0278-5846(02)00342-1
Caputo L, Reguilon MD, Mińarro J, De Feo V, Rodriguez-Arias M (2018) Lavandula angustifolia essential oil and linalool counteract social aversion induced by social defeat. Molecules 23:2694. https://doi.org/10.3390/molecules23102694
Nikfarjam M, Rakhshan R, Ghaderi H (2017) Comparison of effect of Lavandula officinalis and venlafaxine in treating depression: a double blind clinical trial. J Clin Diagn Res 11:KC01–KC04. https://doi.org/10.7860/JCDR/2017/20657.10233
Araj-Khodaei M, Noorbala AA, Yarani R, Emadi F, Emaratkar E, Faghihzadeh S, Parsian Z, Alijaniha F, Kamalinejad M, Naseri M (2020) A double-blind, randomized pilot study for comparison of Melissa officinalis L. and Lavandula angustifolia Mill. and fluoxetine for the treatment of depression. BMC Complement Med Ther 20:207. https://doi.org/10.1186/s12906-020-03003-5
Liu L, Liu C, Wang Y, Wang P, Li Y, Li B (2015) Herbal medicine for anxiety, depression and insomnia. Curr Neuropharmacol 13:481–493. https://doi.org/10.2174/1570159x1304150831122734
Sudha K, Deepak G, Sushant K, Vipul P, Nilofer N, Kharade M, Madhukar S (2011) Study of antidepressant like effect of Coriandrum sativum and involvement of monoaminonergic and gabanergic system. Int J Res Ayurveda Pharm 2:267–270. www.ijrap.net
Sahoo S, Brijesh S (2020) Anxiolytic activity of Coriandrum sativum seeds aqueous extract on chronic restraint stressed mice and effect on brain neurotransmitters. J Funct Foods 68:103884. https://doi.org/10.1016/j.jff.2020.103884
(2021) Evaluation of the antidepressant-like effect of the aqueous extract of Prunus mahaleb L. seed kernels in mice. Univ Thi-Qar J Sci. https://doi.org/10.32792/utq/utjsci/vol8/1/6
Fanaei H, Khayat S, Kasaeian A, Javadimehr M (2016) Effect of curcumin on serum brain-derived neurotrophic factor levels in women with premenstrual syndrome: a randomized, double-blind, placebo-controlled trial. Neuropeptides 56:25–31. https://doi.org/10.1016/j.npep.2015.11.003
Wang Y, Li J, Zhuge L, Su D, Yang M, Tao S, Li J (2014) Comparison between the efficacies of curcumin and puerarin in C57BL/6 mice with steatohepatitis induced by a methionine- and choline-deficient diet. Exp Ther Med 7:663–668. https://doi.org/10.3892/etm.2013.1461
Iqbal M, Sharma SD, Okazaki Y, Fujisawa M, Okada S (2003) Dietary supplementation of curcumin enhances antioxidant and phase II metabolizing enzymes in ddY male mice: possible role in protection against chemical carcinogenesis and toxicity. Pharmacol Toxicol 92:33–38. https://doi.org/10.1034/j.1600-0773.2003.920106.x
Khayat S, Fanaei H, Kheirkhah M, Moghadam ZB, Kasaeian A, Javadimehr M (2015) Curcumin attenuates severity of premenstrual syndrome symptoms: a randomized, double-blind, placebo-controlled trial. Complement Ther Med 23:318–324. https://doi.org/10.1016/j.ctim.2015.04.001
Jafari F, Tabarrai M, Abbassian A, Jafari F, Ayati MH (2021) Effect of garlic (Allium sativum) supplementation on premenstrual disorders: a randomized, double-blind, placebo-controlled trial. Evid Based Complement Altern Med 2021:1–9. https://doi.org/10.1155/2021/9965064
Bhandare SS, Tembhurne SV (2014) Antidepressant effects of dietary supplements Garlic and Black sesame extracts in ovariectomized rats: involving possible estrogenic and antioxidant mechanism. Int J PharmTech Res 6:168–173
Rahmani G, Farajdokht F, Mohaddes G, Babri S, Ebrahimi V, Ebrahimi H (2020) Garlic (Allium sativum) improves anxiety- and depressive-related behaviors and brain oxidative stress in diabetic rats. Arch Physiol Biochem 126:95–100. https://doi.org/10.1080/13813455.2018.1494746
Dhingra D, Goyal PK (2008) Evidences for the involvement of monoaminergic and GABAergic systems in antidepressant-like activity of Tinospora cordifolia in mice. Indian J Pharm Sci 70:761–767. https://doi.org/10.4103/0250-474X.49118
Carver CM, Chuang SH, Reddy DS (2016) Zinc selectively blocks neurosteroid-sensitive extrasynaptic δGABAA receptors in the hippocampus. J Neurosci 36:8070–8077. https://doi.org/10.1523/JNEUROSCI.3393-15.2016
Heidari H, Amani R, Feizi A, Askari G, Kohan S, Tavasoli P (2019) Vitamin D supplementation for premenstrual syndrome-related inflammation and antioxidant markers in students with vitamin D deficient: a randomized clinical trial. Sci Rep 9:1–8. https://doi.org/10.1038/s41598-019-51498-x
Ataollahi M, Ali Akbari SA, Mojab F, Majd HA (2015) The effect of wheat germ extract on premenstrual syndrome symptoms. Iran J Pharm Res 14:159–166
Ahmed M, Azmat A (2017) Decreased brain serotonin turnover rate following administration of Sharbat-e-Ahmed Shah produces antidepressant and anxiolytic effect in rats. Metab Brain Dis 32:1785–1790. https://doi.org/10.1007/s11011-017-0065-6
Thiem B, Kikowska M, Maliński MP, Kruszka D, Napierała M, Florek E (2017) Ecdysteroids: production in plant in vitro cultures. Phytochem Rev 16:603–622. https://doi.org/10.1007/s11101-016-9483-z
Yasir M, Ali A, Ahmad I, Khan N, Ashraf M (2021) Effect of herbal formulation Sharbat Ahmad Shahi on serum BDNF level in mild to moderate cases of depressive disorder. J Complement Med Res 12:265. https://doi.org/10.5455/jcmr.2021.12.04.39
Urooj M, Husain GM, Nadeem M, Naikodi MAR, Alam M, Kazmi MH (2020) Antiepileptic and antidepressant activity of Majoon Najah (a traditional Unani Formulation) in experimental animals. Int J Pharm Investig 10:396–401. https://doi.org/10.5530/ijpi.2020.3.70
Dhingra D, Joshi P, Gupta A, Chhillar R (2012) Possible involvement of monoaminergic neurotransmission in antidepressant-like activity of Emblica officinalis fruits in mice. CNS Neurosci Ther 18:419–425. https://doi.org/10.1111/j.1755-5949.2011.00256.x
Dhingra D, Valecha R (2007) Evaluation of antidepressant-like activity of aqueous and ethanolic extracts of Terminalia bellirica Roxb. fruits in mice. Indian J Exp Biol 45:610–616
Zakerin S, Hajimehdipoor H, Mortazavi SA, Sabetkasaei M, Choopani R, Fahimi S (2021) A herbal syrup: formulation and antidepressant effect in male rat. J Rep Pharm Sci 10:101–109. https://doi.org/10.4103/jrptps.JRPTPS_136_19
Dhingra D, Sharma A (2006) Antidepressant-like activity of Glycyrrhiza glabra L. in mouse models of immobility tests. Prog Neuro-Psychopharmacol Biol Psychiatry 30:449–454. https://doi.org/10.1016/j.pnpbp.2005.11.019
Singh JN, Sunil K, Rana AC (2013) Antidepressant activity of methanolic extract of foeniculum vulgare (fennel) fruits in experimental animal models. J Appl Pharm Sci 3:65–70. https://doi.org/10.7324/JAPS.2013.3912
Ahmadpoor J, Valipour Chahardahcheric S, Setorki M (2019) The Protective effect of hydroalcoholic extract of the Southern Maidenhair Fern (Adiantum capillus-veneris) on the depression and anxiety caused by chronic stress in adult male mice: an experimental randomized study. Iran Red Crescent Med J. https://doi.org/10.5812/ircmj.86750
Lin SH, Chou ML, Chen WC, Lai YS, Lu KH, Hao CW, Sheen LY (2015) A medicinal herb, Melissa officinalis L. ameliorates depressive-like behavior of rats in the forced swimming test via regulating the serotonergic neurotransmitter. J Ethnopharmacol 175:266–272. https://doi.org/10.1016/j.jep.2015.09.018
Qureshi MA, Husain GM, Urooj M, Khan MA, Husain M, Kazmi MH (2021) Preclinical safety, anxiolytic and antidepressant activity of Sufoof Jawahar Mohra: a Unani formulation. Adv Integr Med 8:114–121. https://doi.org/10.1016/j.aimed.2020.06.003
Lee G, Bae H (2017) Therapeutic effects of phytochemicals and medicinal herbs on depression. Biomed Res Int 2017:1–11. https://doi.org/10.1155/2017/6596241
Chan SWY, Harmer CJ, Norbury R, O’Sullivan U, Goodwin GM, Portella MJ (2016) Hippocampal volume in vulnerability and resilience to depression. J Affect Disord 189:199–202. https://doi.org/10.1016/j.jad.2015.09.021
Wang JQ, Mao L (2019) The ERK pathway: molecular mechanisms and treatment of depression. Mol Neurobiol 56:6197–6205. https://doi.org/10.1007/s12035-019-1524-3
Koelsch S, Boehlig A, Hohenadel M, Nitsche I, Bauer K, Sack U (2016) The impact of acute stress on hormones and cytokines, and how their recovery is affected by music-evoked positive mood. Sci Rep 6:23008. https://doi.org/10.1038/srep23008
Reppermund S, Zihl J, Lucae S, Horstmann S, Kloiber S, Holsboer F, Ising M (2007) Persistent cognitive impairment in depression: the role of psychopathology and altered hypothalamic-pituitary-adrenocortical (HPA) system regulation. Biol Psychiatry 62:400–406. https://doi.org/10.1016/j.biopsych.2006.09.027
Müller MB, Holsboer F (2006) Mice with mutations in the HPA-system as models for symptoms of depression. Biol Psychiatry 59:1104–1115. https://doi.org/10.1016/j.biopsych.2006.02.008
Tse G, Yan BP, Chan YWF, Tian XY, Huang Y (2016) Reactive oxygen species, endoplasmic reticulum stress and mitochondrial dysfunction: the link with cardiac arrhythmogenesis. Front Physiol. https://doi.org/10.3389/fphys.2016.00313
Setorki M (2020) Medicinal herbs with anti-depressant effects. J HerbMed Pharmacol 9:309–317. https://doi.org/10.34172/jhp.2020.39
Fava GA (2002) Long-term treatment with antidepressant drugs: The spectacular achievements of propaganda. Psychother Psychosom 71:127–132. https://doi.org/10.1159/000056279
Li C, Huang J, Cheng YC, Zhang YW (2020) Traditional Chinese medicine in depression treatment: from molecules to systems. Front Pharmacol. https://doi.org/10.3389/fphar.2020.00586
Sharma P, Manchanda R, Goswami R, Chawla S (2019) Biodiversity and therapeutic potential of medicinal plants. In: Environ. Concerns Sustain. Dev. Vol. 2 Biodiversity, Soil Waste Manag., pp 27–44. https://doi.org/10.1007/978-981-13-6358-0_2
van Eck NJ, Waltman L (2014) Visualizing bibliometric networks. In: Meas. Sch. Impact, pp 285–320. https://doi.org/10.1007/978-3-319-10377-8_13
Bin Heyat MB, Akhtar F, Ansari MA, Khan A, Alkahtani F, Khan H, Lai D (2020) Progress in detection of insomnia sleep disorder: a comprehensive review. Curr Drug Targets 22:672–684. https://doi.org/10.2174/1389450121666201027125828
Bin-Heyat MB, Akhtar F, Khan MH, Ullah N, Gul I, Khan H, Lai D (2020) Detection, treatment planning, and genetic predisposition of bruxism: a systematic mapping process and network visualization technique. CNS Neurol Disord Drug Targets 20:755–775. https://doi.org/10.2174/1871527319666201110124954
Sheikh S, Bin Heyat MB, AlShorman O, Masadeh M, Alkahatni F (2021) A review of usability evaluation techniques for augmented reality systems in education. In: 2021 Innov. New Trends Eng. Technol. Sci. Educ. Conf. IETSEC 2021, IEEE, pp 1–6. https://doi.org/10.1109/IETSEC51476.2021.9440506
Akhtar F, Li JP, Bin Heyat MB, Quadri SL, Ahmed SS, Yun X, Haq AU (2019) Potential of blockchain technology in digital currency: a review. In: 2019 16th Int. Comput. Conf. Wavelet Act. Media Technol. Inf. Process. ICCWAMTIP 2019, IEEE, Chengdu, pp 85–91.https://doi.org/10.1109/ICCWAMTIP47768.2019.9067546
Akhtar F, Patel PK, Bin Heyat MB, Yousaf S, Baig AA, Mohona RA, Mutoffar MM, Bhattacharya T, Teelhawod BN, Li JP, Kamal MA, Wu K (2022) Smartphone addiction among students and its harmful effects on mental health, oxidative stress, and neurodegeneration towards future modulation of anti-addiction therapies: a comprehensive survey based on SLR, research questions, and network visualization. CNS Neurol Disord Drug Targets. https://doi.org/10.2174/1871527321666220614121439
Ortega MA, Alvarez-Mon MA, García-Montero C, Fraile-Martinez O, Guijarro LG, Lahera G, Monserrat J, Valls P, Mora F, Rodríguez-Jiménez R, Quintero J, Álvarez-Mon M (2022) Gut microbiota metabolites in major depressive disorder—deep insights into their pathophysiological role and potential translational applications. Metabolites 12:50. https://doi.org/10.3390/metabo12010050
Claeys EHI, Mantingh T, Morrens M, Yalin N, Stokes PRA (2022) Resting-state fMRI in depressive and (hypo)manic mood states in bipolar disorders: a systematic review. Prog Neuro-Psychopharmacol Biol Psychiatry 113:110465. https://doi.org/10.1016/j.pnpbp.2021.110465
Lv QY, Chen MM, Li Y, Yu Y, Liao H (2022) Brain circuit dysfunction in specific symptoms of depression. Eur J Neurosci 55:2393–2403. https://doi.org/10.1111/ejn.15221
Gunning FM, Oberlin LE, Schier M, Victoria LW (2021) Brain-based mechanisms of late-life depression: implications for novel interventions. Semin Cell Dev Biol 116:169–179. https://doi.org/10.1016/j.semcdb.2021.05.002
Rajkumar RP (2021) Gut hormones as potential therapeutic targets or biomarkers of response in depression: the case of motilin. Life 11:892. https://doi.org/10.3390/life11090892
Acknowledgements
We would like to thank Prof. Naseem, Prof. Singh, Prof. Lai, Prof. Chandel, Prof. Ansari, Prof. Siddiqui, Dr. Saba, Ms. Parveen, Ms. Jianning, Ms. Pillai, Ms. Yitian (Claire) Zhang, Fangyuan (Tiffany), and Shuyun (Jane) Zhang for their support, help, and appreciation. We also acknowledge the IoT Research Center of Shenzhen University for providing the facilities for this study.
Author information
Authors and Affiliations
Contributions
MBBH, FA, FM, and AS: conceptualization, methodology, writing-original draft, investigation, project administration; software, validation, and resources; AYM, IG, MS, and WA: data curation, validation, methodology, formal analysis, and writing-review and editing; SMAI, AAB, and ITD: supervision, conceptualization, visualization, investigation, resources, and writing-review and editing; KW: data curation, formal analysis, software, and writing-original draft. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Heyat, M.B.B., Akhtar, F., Munir, F. et al. Unravelling the complexities of depression with medical intelligence: exploring the interplay of genetics, hormones, and brain function. Complex Intell. Syst. 10, 5883–5915 (2024). https://doi.org/10.1007/s40747-024-01346-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40747-024-01346-x