
Abstract
Purpose
Subclinical hypercortisolism (SCH) leads to metabolic derangements and increased cardiovascular risk. Cortisol autonomy is defined by the overnight 1 mg dexamethasone suppression test (DST). Saliva cortisol is an easier, stress-free, and cost-effective alternative to serum cortisol. We compared 23 h and post-1 mg DST saliva with serum cortisol to identify SCH in adrenal incidentalomas (AI).
Methods
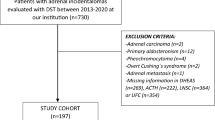
We analyzed 359 DST obtained retrospectively from 226 AI subjects (173F/53 M; 19–83 years) for saliva and serum cortisol. We used three post-DST serum cortisol cutoffs to uncover SCH: 1.8, 2.5, and 5.0 μg/dL. We determined post-DST and 23 h saliva cortisol cutoffs by ROC curve analysis and calculated their sensitivities (S) and specificities (E).
Results
The sensitive 1.8 μg/dL cutoff defined 137 SCH and 180 non-functioning adenomas (NFA): post-DST and 23 h saliva cortisol S/E were: 75.2%/74.4% and 59.5%/65.9%, respectively. Using the specific 5.0 μg/dL cortisol cutoff (22 SCH/295 NFA), post-DST and 23 h saliva cortisol S/E were 86.4%/83.4% and 66.7%/80.4%, respectively. Using the intermediate 2.5 μg/dL cutoff (89 SCH/228 NFA), post-DST and 23 h saliva cortisol S/E were 80.9%/68.9% and 65.5%/62.8%, respectively.
Conclusion
Saliva cortisol showed acceptable performance only with the 5.0 μg/dL cortisol cutoff, as in overt Cushing’s syndrome. Lower cutoffs (1.8 and 2.5 μg/dL) that identify larger samples of patients with poor metabolic outcomes are less accurate for screening. These results may be attributed to pre-analytical factors and inherent patient conditions. Thus, saliva cortisol cannot replace serum cortisol to identify SCH among patients with AI for screening DST.


Similar content being viewed by others

References
Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A, Tabarin A, Terzolo M, Tsagarakis S, Dekkers OM (2016) Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol 175:G1–G34
Chiodini I, Morelli V (2016) Subclinical hypercortisolism: how to deal with it? Front Horm Res 46:28–38
Mazzuco TL, Bourdeau I, Lacroix A (2009) Adrenal incidentalomas and subclinical Cushing’s syndrome: diagnosis and treatment. Curr Opin Endocrinol Diabetes Obes 16:203–210
Debono M, Newell-Price J (2015) Subclinical hypercortisolism in adrenal incidentaloma. Curr Opin Endocrinol Diabetes Obes 22:185–192
Rossi R, Tauchmanova L, Luciano A, Di Martino M, Battista C, Del Viscovo L, Nuzzo V, Lombardi G (2000) Subclinical Cushing’s syndrome in patients with adrenal incidentaloma: clinical and biochemical features. J Clin Endocrinol Metab 85:1440–1448
Midorikawa S, Sanada H, Hashimoto S, Suzuki T, Watanabe T, Sasano H (2001) Analysis of cortisol secretion in hormonally inactive adrenocortical incidentalomas: study of in vitro steroid secretion and immunohistochemical localization of steroidogenic enzymes. Endocr J 48:167–174
Bernini G, Moretti A, Argenio G, Salvetti A (2002) Primary aldosteronism in normokalemic patients with adrenal incidentalomas. Eur J Endocrinol 146:523–529
Erbil Y, Ademog˘lu E, Ozbey N, Barbaros U, Ozbey N, Yanik BT, Salmasliog˘lu A, Bozbora A, Ozarmag˘an S (2006) Evaluation of the cardiovascular risk in patients with subclinical Cushing syndrome before and after surgery. World J Surg 30:1665–1671
Tsuiki M, Tanabe A, Takagi S, Naruse M, Takano K (2008) Cardiovascular risks and their long-term clinical outcome in patients with subclinical Cushing’s syndrome. Endocr J 55:737–745
Toniato A, Merante-Boschin I, Opocher G, Pelizzo MR, Schiavi F, Ballotta E (2009) Surgical versus conservative management for subclinical Cushing syndrome in adrenal incidentalomas: a prospective randomized study. Ann Surg 249:388–391
Chiodini I, Morelli V, Salcuni AS, Eller-Vainicher C, Torlontano M, Coletti F, Iorio L, Cuttitta A, Ambrosio A, Vicentini L, Pellegrini F, Copetti M, Beck-Peccoz P, Arosio M, Ambrosi B, Trischitta V, Scillitani A (2010) Beneficial metabolic effects of prompt surgical treatment in patients with an adrenal incidentaloma causing biochemical hypercortisolism. J Clin Endocrinol Metab 95:2736–2745
Giorgi RB, Correa MV, Costa-Barbosa FA, Kater CE (2019) Cyclic subclinical hypercortisolism: a previously unidentified hypersecretory form of adrenal incidentalomas. J Endocr Soc 3:678–686
Terzolo M, Stigliano A, Chiodini I, Loli P, Furlani L, Arnaldi G, Reimondo G, Pia A, Toscano V, Zini M, Borretta G, Papini E, Garofalo P, Allolio B, Dupas B, Mantero F, Tabarin A (2011) AME position statement on adrenal incidentaloma. Eur J Endocrinol 164:851–870
Tateishi Y, Kouyama R, Mihara M, Doi M, Yoshimoto T, Hirata Y (2012) Evaluation of salivary cortisol measurements for the diagnosis of subclinical Cushing’s syndrome. Endocr J 59:283–289
Chiodini I, Albani A, Ambrogio AG, Campo M, De Martino MC, Marcelli G, Morelli V, Zampetti B, Colao A, Pivonello R (2017) Six controversial issues on subclinical Cushing’s syndrome. Endocrine 56:262–266
Ceccato F, Barbot M, Albiger N, Antonelli G, Zilio M, Todeschini M, Regazzo D, Plebani M, Lacognata C, Iacobone M, Mantero F, Boscaro M, Scaroni C (2018) Daily salivary cortisol and cortisone rhythm in patients with adrenal incidentaloma. Endocr 59:510–519
Liddle GW (1960) Tests of pituitary-adrenal suppressibility in the diagnosis of Cushing’s syndrome. J Clin Endocrinol Metab 20:1539–1560
Nugent CA, Nichols T, Tyler FH (1965) Diagnosis of Cushing’s syndrome—single dose dexamethasone suppression test. Arch Intern Med 116:172–176
Pavlatos FC, Smilo RP, Forsham PH (1965) A rapid screening test for Cushing’s syndrome. JAMA 193:720–723
Mattingly D (1962) A simple fluorimetric method for the estimation of free 11-hydroxycorticosteroids in human plasma. J Clin Pathol 15:374–379
Shannon IL, Prigmore JR, Brooks RA, Feller RP (1959) The 17-hydroxycorticosteroids of parotid fluid, serum and urine following intramuscular administration of repository corticotropin. J Clin Endocrinol Metab 19:1477–1480
Katz FH, Shannon IL (1969) Adrenal corticosteroids in submaxillary fluids. J Dental Res 48:448–451
Walker RF, Riad-Fahrny D, Read GF (1978) Adrenal status assessed by direct radioimmunoassay of cortisol in whole saliva or parotid saliva. Clin Chem 24:1460–1463
Vining RF, McGinley RA, Maksvytis JJ, Ho KY (1983) Salivary cortisol: a better measure of adrenal cortical function than serum cortisol. Ann Clin Biochem 20:329–335
Tabarin A, Bardet S, Bertherat J, Dupas B, Chabre O, Hamoir E, Laurent F, Tenenbaum F, Cazalda M, Lefebvre H, Valli N, Rohmer V (2008) Exploration and management of adrenal incidentalomas. French Society of Endocrinology Consensus. Ann Endocrinol 69:487–500
Zeiger MA, Thompson GB, Duh QY, Hamrahian AH, Angelos P, Elaraj D, Fishman E, Kharlip J (2009) The American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons medical guidelines for the management of adrenal incidentalomas. Endocr Pract 15:1–20
Masserini B, Morelli V, Bergamaschi S, Ermetici F, Eller-Vainicher C, Barbieri AM, Maffini MA, Scillitani A, Ambrosi B, Beck-Peccoz P, Chiodini I (2009) The limited role of midnight salivary cortisol levels in the diagnosis of subclinical hypercortisolism in patients with adrenal incidentaloma. Eur J Endocrinol 160:87–92
Nunes ML, Vattaut S, Corcuff JB, Rault A, Loiseau H, Gatta B, Valli N, Letenneur L, Tabarin A (2009) Late-night salivary cortisol for diagnosis of overt and subclinical Cushing’s syndrome in hospitalized and ambulatory patients. J Clin Endocrinol Metab 94:456–462
Huayllas MKP, Netzel BC, Singh RJ, Kater CE (2018) Serum cortisol levels via radioimmunoassay vs liquid chromatography mass spectrophotometry in healthy control subjects and patients with adrenal incidentalomas. Lab Med 49(3):259–267
Tonetto-Fernandes V, Lemos-Marini SH, Kuperman H, Ribeiro-Neto LM, Verreschi IT, Kater CE (2006) Serum 21-deoxycortisol, 17-Hydroxyprogesterone, and 11-deoxycortisol in classic congenital adrenal hyperplasia: clinical and hormonal correlations and identification of patients with 11beta-hydroxylase deficiency among a large group with alleged 21-hydroxylase deficiency. J Clin Endocrinol Metab 91:2179–2184
Ceccato F, Antonelli G, Frigo AC, Regazzo D, Plebani M, Boscaro M, Scaroni C (2017) First-line screening tests for Cushing’s syndrome in patients with adrenal incidentaloma: the role of urinary free cortisol measured by LC–MS/MS. J Endocrinol Invest 40:753–760
Eller-Vainicher C, Morelli V, Salcuni AS, Battista C, Torlontano M, Coletti F, Iorio L, Cairoli E, Beck-Peccoz P, Arosio M, Ambrosi B, Scillitani A, Chiodini I (2010) Accuracy of several parameters of hypothalamic-pituitary-adrenal axis activity in predicting before surgery the metabolic effects of the removal of an adrenal incidentaloma. Eur J Endocrinol 163:925–935
Eller-Vainicher C, Morelli V, Salcuni AS, Torlontano M, Coletti F, Iorio L, Cuttitta A, Ambrosio A, Vicentini L, Carnevale V, Beck-Peccoz P, Arosio M, Ambrosi B, Scillitani A, Chiodini I (2010) Postsurgical hypocortisolism after removal of an adrenal incidentaloma: is it predictable by an accurate endocrinological work-up before surgery? Eur J Endocrinol 162:91–99
Morelli V, Masserini B, Salcuni AS, Eller-Vainicher C, Savoca C, Viti R, Coletti F, Guglielmi G, Battista C, Iorio L, Beck-Peccoz P, Ambrosi B, Arosio M, Scillitani A, Chiodini I (2010) Subclinical hypercortisolism: correlation between biochemical diagnostic criteria and clinical aspects. Clin Endocrinol (Oxf) 73:161–166
Morelli V, Scillitani A, Arosio M, Chiodini I (2017) Follow–up of patients with adrenal incidentaloma, in accordance with the European society of endocrinology guidelines: could we be safe? J Endocrinol Invest 40:331–333
Ueland GA, Methlie P, Kellmann R, Bjorgaas M, Asvold BO, Thorstensen K, Kelp O, Thordarson HB, Mellgren G, Løvås K, Husebye ES (2017) Simultaneous assay of cortisol and dexamethasone improved diagnostic accuracy of the dexamethasone suppression test. Eur J Endocrinol 176:705–713
Nickelsen T, Lissner W, Schoffling K (1989) The dexamethasone suppression test and long-term contraceptive treatment: measurement of ACTH or salivary cortisol does not improve the reliability of the test. Exp Clin Endocrinol 94:275–280
Qureshi AC, Bahri A, Breen LA, Barnes SC, Powrie JK, Thomas SM, Carroll PV (2007) The influence of the route of oestrogen administration on serum levels of cortisol-binding globulin and total cortisol. Clin Endocrinol (Oxf) 66:632–635
Palmieri S, Morelli V, Polledri E, Fustinoni S, Mercadante R, Olgiati L, Eller Vainicher C, Cairoli E, Zhukouskaya VV, Beck-Peccoz P, Chiodini I (2013) The role of salivary cortisol measured by liquid chromatography-tandem mass spectrometry in the diagnosis of subclinical hypercortisolism. Eur J Endocrinol 168:289–296
Klose M, Lange M, Rasmussen AK, Skakkebaek NE, Hilsted L, Haug E, Andersen M, Feldt-Rasmussen U (2007) Factors influencing the adrenocorticotropin test: role of contemporary cortisol assays, body composition, and oral contraceptive agents. J Clin Endocrinol Metab 92:1326–1333
Hamrahian AH, Oseni TS, Arafah BM (2004) Measurements of serum free cortisol in critically ill patients. N Engl J Med 350:1629–1638
Tan T, Chang L, Woodward A, McWhinney B, Galligan J, Macdonald GA, Cohen J, Venkatesh B (2010) Characterizing adrenal function using directly measured plasma free cortisol in stable severe liver disease. J Hepatol 53:841–848
Ho JT, Al-Musalhi H, Chapman MJ, Quach T, Thomas PD, Bagley CJ, Lewis JG, Torpy DJ (2006) Septic shock and sepsis: a comparison of total and free plasma cortisol levels. J Clin Endocrinol Metab 91:105–114
Arafah B, Nishiyama F, Tlaygeh H, Hejal R (2007) Measurement of salivary cortisol concentration in the assessment of adrenal function in critically ill subjects: a surrogate marker of the circulating free cortisol. J Clin Endocrinol Metab 92:2965–2971
Nieman LK, Biller BM, Findling JW, Newell-Price J, Savage MO, Stewart PM, Montori VM (2008) The diagnosis of Cushing’s syndrome: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 93:1526–1540
Doi SA, Clark J, Russell AW (2013) Concordance of the late night salivary cortisol in patients with Cushing’s syndrome and elevated urine-free cortisol. Endocrine 43:327–333
Acknowledgements
Marcelo Vieira-Correa received a fellowship grant from CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior), Brazil.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the ethical committee of the Federal University of Sao Paulo.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vieira-Correa, M., Giorgi, R.B., Oliveira, K.C. et al. Saliva versus serum cortisol to identify subclinical hypercortisolism in adrenal incidentalomas: simplicity versus accuracy. J Endocrinol Invest 42, 1435–1442 (2019). https://doi.org/10.1007/s40618-019-01104-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-019-01104-8