
Abstract
Background
Older adults living in long-term care facilities (LTCF) have been severely affected by COVID-19. Hospice care (HC) facilities and palliative care are essential in treating patients dying from COVID-19. In Italy, little is known about the impact of COVID-19 on deaths in LTCF and the care provided in HC to COVID-19 patients.
Aim
To assess overall and case-specific mortality in 2020 in LTC and HC facilities in comparison to the previous five years (2015–2019).
Methods
We performed a descriptive study using data derived from the Italian national “Cause of Death” registry—managed by the Italian National Institute of Statistics—on deaths occurred in LTC and HC facilities during 2020 and the period 2015–2019.
Results
Number of deaths significantly increased in 2020 compared with 2015–2019 in LTCF (83,062 deaths vs. 59,200) and slightly decreased in hospices (38,788 vs. 39,652). COVID-19 caused 12.5% of deaths in LTCF and only 2% in hospices. Other than COVID-19, in 2020, cancer accounted for 77% of all deaths that occurred in HC, while cardiovascular diseases (35.6%) and psychotic and behavioral disorders (10%) were the most common causes of death in LTCF. Overall, 22% of the excess mortality registered in Italy during 2020 is represented by the deaths that occurred in LTCF.
Discussion and conclusion
LTCF were disproportionally affected by COVID-19, while the response to the pandemic in HC was limited. These data can help plan strategies to limit the impact of future epidemics and to better understand residential care response to COVID-19 epidemic.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
Introduction
COVID-19 poses a direct threat to older adults, who are intrinsically more at risk of adverse outcomes [1,2,3], are usually affected by multiple chronic conditions, and experience geriatric syndromes, such as frailty and cognitive impairment [4, 5]. Italy, one of the countries with the oldest population worldwide [6], has registered an excess mortality of more than 100,000 deaths in 2020, the first year of the epidemic, and the highest case-fatality rate has been observed among older multi-morbid patients [7].
Older adults in long-term care facilities represent a population that has been particularly affected by COVID-19 due to the intrinsic vulnerability of the residents, who are often institutionalized because of the higher prevalence of multiple health conditions and disability [2, 8, 9]. Also, the restrictions set in place by health authorities to reduce the spread of the virus, such as social distancing and limited visiting hours with family members, have contributed to increasing social isolation, frailty, and incident adverse events [10]. In England, during the first weeks of the pandemic, an excess mortality rate was registered among care homes residents compared to community dwellers [11, 12]. An Italian national survey of 1,356 nursing homes, hosting a total of 100,806 residents, recorded 9,154 overall deaths during the first trimester of the pandemic, with a cumulative incidence of 0.7 per 100 residents among COVID-19 confirmed cases and 3.1 per 100 residents among flu‐like symptoms cases [13, 14]. The lack of personal protective equipment (PPE) and limited availability of COVID-19 testing have also contributed to the increased mortality [11,12,13]. To this date, in Italy, the exact impact of COVID-19 on overall deaths in long-term care facilities is unknown.
Hospice care facilities are designed to provide multidimensional care, aiming to reduce physical, psychological, social, and spiritual suffering [15, 16]. The relief of suffering, but also the support of complex decision-making, the management of clinical uncertainty, the provision of psychosocial and bereavement care, and the advocacy for patients and their families are critical features of palliative care and essential components of the response during global emergencies such as epidemics [17,18,19]. Two systematic reviews have highlighted how palliative care services in hospitals and primary healthcare are essential in response to COVID-19 [18, 19], and could play a crucial role in treating patients dying from COVID-19 [17]. A study conducted in Lombardy, Italy, underlined how palliative care in an emergency context could contribute to patient selection and triage through a multidisciplinary approach to discuss the best therapeutic strategy on a case-by-case basis [20]. Older frail multi-morbid adults with complex clinical and social needs could greatly benefit from a care plan that includes palliative management, thus avoiding unnecessary hospitalization or a disproportionate intensive clinical approach [21]. In October 2020, the Palliative Care Federation (FCP) published a joint document with the Italian Palliative Care Society (SICP) suggesting recommendations and guidelines to integrate palliative care into the national pandemic plan [22]. However, little is known about the care provided in hospice to patients suffering from COVID-19 at a country level.
With this work, we aimed to assess case-specific mortality in 2020 in long-term care and hospice care facilities compared to the previous five years (2015–2019), with a specific focus on COVID-19. We also aimed to evaluate excess mortality by cause in these settings.
Methods
Deaths of the Italian resident population that occurred in 2015–2020 were analyzed. We compared different causes of death observed in 2020 in the Italian resident population to the ones observed in the previous five years (2015–2019), in terms of the mean number of casualties. Causes of death were derived from the national Cause of Death registry, managed by the Italian National Institute of Statistics, which collects copies of death certificates completed by the medical certifiers for all deaths occurring in Italy. All causes reported on the death certificate are classified according to the International Classification of Diseases, 10th Revision (ICD10) [23], using the semi-automated coding system Iris (www.iris-institute.org, accessed on 23 November 2022), which attributes ICD codes for approximately 80% of cases; the remaining 20% are reviewed by expert personnel. For each case, the underlying cause of death defined by the World Health Organization (WHO) as “the condition that initiated the train of morbid events leading to death” was selected. COVID-19 coding was performed by the latest recommendations by the WHO [24].
Study settings
The present study considered only deaths in patients who received care in a hospice or long-term care facilities (including care homes and nursing homes). The number of beds available and patients admitted to HC facilities and the number of beds available in long-term care facilities during the study's period are presented in Supplementary Materials (Supplementary Table S1).
In Italy, hospice care is provided by the National Healthcare System (“Sistema Sanitario Nazionale” or SSN). The “Sistema Sanitario Nazionale” fully covers the costs of care. The number of palliative care units has continuously expanded since the mid-2000s and provides advanced home care, hospice, and consulting services. For this study, only hospice care is considered.
Long-term care facilities in Italy cover care homes and nursing homes. Care homes (“Case di Riposo”) are assisted living facilities for older adults who are partially self-sufficient and present primarily social needs. Nursing homes provide residential healthcare and social support to individuals with different clinical conditions including chronic patients who are not autonomous (i.e., those with dementia or disabilities).
COVID-19 waves in Italy in 2020
Italy was the first nation with widespread population involvement in COVID-19, with high mortality in the spring of 2020, followed by a summer with relatively low infection incidence after easing the tight lockdown that was in effect from March 8 through May 2, 2020 [7]. The second wave arrived in late August and peaked in autumn 2020 [14]. Given the epidemiology of the COVID-19 pandemic in the country and the occurrence of two epidemic waves in 2020, for the present study, we present the distribution of death and causes of death that occurred in the country in the whole of 2020 and separately in the periods January–June and July–December.
Results
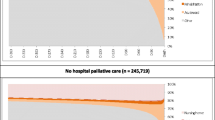
The mean number of deaths from all causes for 2015–2019 compared to 2020 is shown in Fig. 1 for hospice care facilities and in Fig. 2 for long-term care facilities. COVID-19 deaths are highlighted in black in the 2020 columns.

Mean number of deaths occurred in 2015–2019 and 2020 in Long-term care facilities. The black part of the columns represents deaths due to COVID-19

Mean number of deaths occurred in 2015–2019 and 2020 in Hospice care facilities. The black part of the columns represents deaths due to COVID-19
The figures show an increment in the total number of deaths in 2020 compared to the previous five years for long-term care facilities (83,062 vs. 59,200 deaths), consistent in both semesters analyzed. Conversely, a slight reduction was documented in the number of fatalities occurred in hospice care facilities (38,788 vs. 39,652), especially during the second semester of 2020. The number of deaths that occurred in long-term care facilities due to COVID-19 was 10,395 (12.5% of all deaths occurred in this setting in 2020). Deaths due to causes other than COVID-19 also increased in 2020 as compared with the 2015–2019 period (+ 16% deaths). COVID-19 seemed to have a minimal impact on deaths in hospice care facilities, with only 790 deaths due to COVID-19 (2% of all deaths occurred in this setting in 2020).
Table 1 shows sex distribution and mean age of deaths that occurred in hospice and long-term care facilities during the study periods. Patients who died in long-term care facilities were more likely females and older than those in hospice care facilities. Compared with the deaths registered during 2015–2019, patients who died in 2020 were more likely females and had an older age in both setting analyzed.
Finally, a comparison between the mean number of cause-specific deaths that occurred in the period 2015–2019 and the year 2020 is presented in Table 2. Data for hospice and long-term care facilities are shown according to the first and second semester periods and all-year data. In hospice care facilities, cancer was the most prevalent cause, accounting for 83% of all deaths in 2015–2019 and 77% in 2020. As already shown in Fig. 1, COVID-19 deaths were limited in this setting. In long-term care facilities, distribution of causes of death was more heterogeneous than in HC facilities. Cardiovascular diseases (25,565 deaths, 43% of all deaths), cancer (7,348 deaths, 12.4%), and psychotic and behavioral disorders (6,491 deaths, 11%) represented the most common causes of death during the period 2015–2019. Cardiovascular diseases were still the most common cause of death in this setting in 2020 (29,641 deaths, 35% of all deaths), followed by COVID-19 (10,395 deaths, 12.5%), and psychotic and behavioral disorders (8412 deaths, 10% of all deaths). With the only exception of cancer (-6.7%), the number of deaths for all other causes increased in 2020 as compared to 2015–2019. This association was consistent in both analyzed semesters, except for deaths due to respiratory diseases, which increased by 85% in the first semester and declined by 4.4% during the second semester in long-term care facilities.
Discussion
We conducted a descriptive study to assess case-specific mortality in long-term care and hospice care facilities during the year 2020 in comparison to the previous five-year time (2015–2019), with a specific focus on COVID-19. We have underlined that COVID-19 had a relevant impact on deaths that occurred in LTCF, while hospice care facilities were less significantly affected by this condition. Residents who died during 2020 in long-term care facilities were on average older than those in hospice facilities and, more often, females. In Italy, independently of the study settings, an excess mortality of 108,178 deaths during the whole of 2020 compared to the previous five-year time was registered [25]. Based on the data we presented, we can estimate that 22% of this excess mortality can be explained by deaths that have occurred in long-term care facilities. This excess mortality can be attributed to COVID-19-related deaths as a primary cause, but also to under-treatment of other diseases as well as social isolation that might have increased depressive symptoms and delirium, both conditions associated with adverse outcomes, often leading to malnutrition, being bed-bound, and eventually death [26].
Especially during the first wave of the pandemic, long-term care facilities have been disproportionally affected by COVID-19, accounting for almost 50% of COVID-19-related deaths [27], and frail and vulnerable residents were not provided appropriate physical and psychosocial support, as underlined by Heckman and colleagues [28]. Residents of long-term care facilities with COVID-19 or other acute conditions, could often not be transferred to acute care hospitals, overwhelmed by COVID-19 patients. The increased number of deaths in 2020 cannot entirely be attributed to COVID-19 but also to several other underdiagnosed and undertreated conditions. Furthermore, during the initial phase of the epidemic, healthcare resources were often relocated to acute facilities to assist patients with COVID-19, and appointments or visits for chronic conditions were repeatedly postponed. Even the management of acute conditions different from COVID-19 was often delayed. The lack of PPE and low rate of SARS-CoV-2 testing made infection control challenging and diagnosis of COVID-19 uncertain or based on clinical symptoms, favoring the spreading of the virus within long-term care facilities. During the second semester of 2020, thanks to extra-governmental funds and increased availability of PPE, many long-term care facilities were transformed into COVID-19 facilities with the purpose of caring for older COVID-19 patients discharged from acute hospitals or promptly managing residents of the facilities whom SARS-CoV-2 infected. This factor can further explain the high number of deaths occurring in long-term care facilities.
Noticeably a substantial increment of deaths that occurred in long-term care facilities due to respiratory diseases was observed in the first semester of 2020. This finding can be due to the lack of SARS-CoV-2 diagnostic tests in the first period of the pandemic. Therefore, many patients may have been classified as dying by respiratory diseases (i.e., pneumonia) rather than by COVID-19.
The response to the pandemic in hospice care facilities was very limited, even if efforts to standardize palliative care for COVID-19 patients were made on a national scale. Hospice care facilities rarely activated an admission path for patients positive for SARS-CoV-2 infection. Italian hospices continued to register mainly cancer-related deaths while COVID-19-related deaths were extremely low. A survey conducted in the U.S. on hospice agencies underlined how healthcare professionals found that inadequate supplies of PPE had an essential impact on the delivery of care during the first year of the pandemic especially, as well as the reduced number of personnel in hospices insufficient to respond to the increase in family bereavement needs efficiently. More importantly, almost one-third of respondents reported adverse effects on patient outcomes, such as inadequate symptom management and negative psychosocial effects which can be explained by shorter visitations of healthcare providers and family members to reduce probabilities of contact [29]. The number of deaths due to cancer was substantially reduced in hospice facilities in 2020. This could relate the fact that cancer patients with terminal disease often remained hospitalized if affected by COVID-19 and were not transferred to hospice care facilities. In addition, community-dwelling patients with cancer may have experienced difficulties in accessing healthcare services, including palliative care, or may have avoided contact with healthcare services due to increased risk and fear of contracting COVID-19.
Conclusions and implications
In conclusion, the data we have presented describe the scenario experienced in two different types of residential care facilities in Italy, during the first year of COVID-19 Pandemic. These data can help understand the strategies adopted in the first epidemic phase, when the National Healthcare System was unprepared to face the challenges posed by COVID-19 and to plan strategies to limit the impact of future epidemics.
Data availability
The data used for this work are public and available from the website of the Italian National Institute of Statistics (ISTAT).
References
Williamson EJ, Walker AJ, Bhaskaran K et al (2020) Factors associated with COVID-19-related death using OpenSAFELY. Nature 584:430–436
Di Bari M, Tonarelli F, Balzi D et al (2022) COVID-19, vulnerability, and long-term mortality in hospitalized and nonhospitalized older persons. J Am Med Dir Assoc 23:414-420.e1
Wilson D, Jackson T, Sapey E et al (2017) Frailty and sarcopenia: The potential role of an aged immune system. Ageing Res Rev 36:1–10
Zazzara MB, Vetrano DL, Carfì A et al (2019) Frailty and chronic disease. Panminerva Med 61:486–492
Onder G, Vetrano DL, Marengoni A et al (2018) Accounting for frailty when treating chronic diseases. Eur J Intern Med 56:49–52
Istituto Nazionale di Statistica (2021). Popolazione Residente per età, sesso e stato civile al 1° gennaio 2018 [Internet]. Available from: http://demo.istat.it/pop2018/index. (Accessed September 15, 2021)
Onder G, Rezza G, Brusaferro S (2020) Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 323:1775–1776
Declercq A, de Stampa M, Geffen L, et al. (2020) Why, in almost all countries, was residential care for older people so badly affected by COVID-19? Opin Pap Obs Soc Eur. 23.
Malara A, Noale M, Abbatecola AM et al (2022) Clinical features of SARS-CoV-2 infection in Italian long-term care facilities: GeroCovid LTCFs observational Study. J Am Med Dir Assoc 23:15–18
Lombardo FL, Salvi E, Lacorte E et al (2020) adverse events in italian nursing homes during the COVID-19 epidemic: a national survey. Front Psychiatry 30:578465
Gulliford MC, Prevost AT, Clegg A et al (2022) Mortality of care home residents and community-dwelling controls during the COVID-19 pandemic in 2020: matched cohort study. J Am Med Dir Assoc 23:923-929.e2
Morciano M, Stokes J, Kontopantelis E et al (2021) Excess mortality for care home residents during the first 23 weeks of the COVID-19 pandemic in England: a national cohort study. BMC Med 19:71
Lombardo FL, Bacigalupo I, Salvi E et al (2021) The Italian national survey on Coronavirus disease 2019 epidemic spread in nursing homes. Int J Geriatr Psychiatry 36:873–882
Dorrucci M, Minelli G, Boros S et al (2021) Excess mortality in Italy during the COVID-19 pandemic: assessing the differences between the first and the second wave, Year 2020. Front Public Health 16:669209
Martinsson L, Strang P, Bergstrom J et al (2021) Dying from COVID-19 in nursing homes-sex differences in symptom occurrence. BMC Geriatr 21:294
World Health Organization. Palliative care [Internet]. Available from: https://www.who.int/health-topics/palliative-care. (Accessed December 8, 2022)
Powell RA, Schwartz L, Nouvet E et al (2017) Palliative care in humanitarian crises: always something to offer. Lancet 389:1498–1499
Etkind SN, Bone AE, Lovell N et al (2020) The role and response of palliative care and hospice services in epidemics and pandemics: a rapid review to inform practice during the COVID-19 pandemic. J Pain Symptom Manage 60:e31–e40
Mitchell S, Maynard V, Lyons V et al (2020) The role and response of primary healthcare services in the delivery of palliative care in epidemics and pandemics: a rapid review to inform practice and service delivery during the COVID-19 pandemic. Palliat Med 34:1182–1192
Riva L, Caraceni A, Vigorita F et al (2020) COVID-19 emergency and palliative medicine: An intervention model’. BMJ Support Palliat Care. bmjspcare-2020–002561
Hall S, Petkova H, Tsouros AD, Costantini M, Higginson IJ(2011) Palliative care for older people: better practices. World Health Organization. Regional Office for Europe. https://apps.who.int/iris/handle/10665/326378
Gobber G, Antonione R, Orsi L, et al. Gruppo di lavoro SICP – FCP Ruolo delle cure palliative durante una pandemia. 2020. Available from: https://www.sicp.it/documenti/sicp/2020/10/ruole-delle-cure-palliative-durante-una-pandemia/
World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). 2016 [Internet]. Available from: https://icd.who.int/browse10/2016/en. (Accessed December 8, 2022)
World Health Organization. International Guidelines for Certification and Classification (Coding) of COVID-19 as Cause of Death. 2020. [Internet]. Available from: https://www.who.int/publications/m/item/international-guidelines-for-certification-and-classification-(coding)-of-covid-19-as-cause-of-death (Accessed December 8, 2022)
Istituto Nazionale di Statistica. Impatto dell'epidemia COVID-19 sulla mortalità totale della popolazione residente - anni 2020–2021 e Gennaio 2022. 2022. [Internet]. Available from: https://www.istat.it/it/archivio/266865 (Accessed November 15, 2022).
Levere M, Rowan P, Wysocki A (2021) The adverse effects of the COVID-19 pandemic on nursing home resident well-being. J Am Med Dir Assoc 22:948-954.e2
Sepulveda ER, Stall NM, Sinha SK (2020) A comparison of COVID-19 mortality rates among long-term care residents in 12 OECD countries. J Am Med Dir Assoc 21:1572-1574.e3
Heckman GA, Kay K, Morrison A et al (2021) Proceedings from an International Virtual Townhall: reflecting on the COVID-19 pandemic: themes from long-term care. J Am Med Dir Assoc 22:1128–1132
Rogers JEB, Constantine LA, Thompson JM et al (2021) COVID-19 Pandemic Impacts on U.S. hospice agencies: a national survey of hospice nurses and physicians. Am J Hosp Palliat Care 38:521–527
Funding
Open access funding provided by Università Cattolica del Sacro Cuore within the CRUI-CARE Agreement. This research received no specific grant from any funding agency in the public, commercial, or no-profit sectors.
Author information
Authors and Affiliations
Contributions
GO and GM designed and supervised the study. GM and AM carried out data analysis and contributed to data extraction. MBZ and GB contributed to the literature search, the interpretation of results, and the writing of the manuscript. GO critically revised the analyses and the performance of the findings and contributed to report of the manuscript. GM, IP, AM, AB, SD, EM, and MAR critically revised the manuscript. All the co-authors reviewed the manuscript and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
None of the authors has any conflict of interest to disclose.
Ethical approval
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements.
Informed consent
Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Statement of human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zazzara, M.B., Colloca, G.F., Maraschini, A. et al. Causes of deaths in long-term care and hospice care facilities during the first year of COVID-19 pandemic: a snapshot of Italy during 2020. Aging Clin Exp Res 35, 1385–1392 (2023). https://doi.org/10.1007/s40520-023-02426-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-023-02426-7