
Abstract
Research on the prevalence of anxiety in children and adolescents with autism remains fragmented due to a reliance on help-seeking populations and differences in anxiety assessment. We present the pooled findings from 15 community studies (N = 4459) sourced from the Embase, PubMed, and PsycINFO databases (1970–2023). Equally high rates of anxiety symptoms and disorders were identified via self-report (33%, CI = 25 to 40%) and diagnostic interview (19%, CI = 7 to 40%). Higher IQ and male gender were identified as significant covariates, although these results may reflect sampling biases. The findings highlight the need for routine screening, with multiple informants, and improved sampling methods. Protocol was registered on Open Science Framework (https://osf.io/7mtca/).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Anxiety disorders and symptoms are common among children and adolescents diagnosed with autism spectrum disorder (ASD). However, this research is characterised by variability in findings, with point-in-time prevalence of individual anxiety disorders ranging from 2% to a staggering 84% (Mutluer et al., 2022; White et al., 2009). The diagnosis of anxiety in ASD is further complicated by inconsistent symptom presentations (e.g. fear of change or novelty, unusual phobias; Mayes et al., 2013), likely related to atypical sensory experiences. Indeed, it has been estimated that up to 46% of these children display anxiety symptoms that do not neatly align with nomenclature systems such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) (Kerns et al., 2014; Mayes et al., 2013).
A reliance on convenience samples from treatment trials or intervention settings could explain these varied estimates (e.g. van Steensel et al., 2011). Such samples may not only overestimate anxiety prevalence but can result in spurious associations, given the increased likelihood of these groups presenting with pronounced anxiety compared to the general populace (Mutluer et al., 2022). Notably, meta-analyses examining psychiatric comorbidities among community-based samples with ASD have reported lower, albeit still high rates of anxiety disorder (e.g. ~ 20% Lai et al., 2019; Mutluer et al., 2022). However, these reviews did not stratify the point prevalence of anxiety across specific anxiety disorders.
The measurement of anxiety is a further consideration. Validated self-report measures (e.g. Liebowitz Social Anxiety Scale; Liebowitz, 1987) should, ideally, be supplemented with parental reports given noted emotional and language impairments in the ASD population (Mazefsky et al., 2011). That said, parental reports carry their own unintended risks, with parents underestimating the prevalence of internalising symptoms (e.g. child worry; Niditch et al., 2012). For this reason, structured diagnostic interview tools, such as the Schedule for Affective Disorders for Children (K-SADS; Chambers et al., 1985), are preferred. Notably, the K-SADS relies on the DSM-V (American Psychiatric Association, 2013) criteria for anxiety disorders. However, the DSM-V includes the additional disorder of agoraphobia, likely broadening the potential number of participants that qualify for caseness. Indeed, Guerrera et al. (2022) identified almost 86% of their ASD sample with an anxiety disorder based on the K-SADS. The impact of recategorisation changes in the DSM-5 on prevalence estimates remains to be determined, although this version is considered to offer a more comprehensive understanding of ASD as a spectrum (Zwaigenbaum et al., 2015) as well as a clear, consistent definition of anxiety disorder .
There has also been considerable traction around the hypothesis that greater cognitive functioning may create a greater vulnerability in self-esteem through increased self-awareness of social and mental deficits (Edirisooriya et al., 2021; Mazurek & Kanne, 2010; Sukhodolsky et al., 2008). Empirical support for this theory is mixed, with individual ASD studies reporting strong positive associations (r = 0.51, Niditch et al., 2012) but also weak to no association between IQ and anxiety symptomology (r = 0.05, Mazurek & Petroski, 2015). Conversely, it has been argued that those with a higher IQ have greater general understanding, knowledge, and adaptability skills that protect against changes in routine or unfamiliar situations (Edirisooriya et al., 2021).
Age-based differences in anxiety prevalence estimates are also inconsistent in ASD research. Whereas Niditch et al. (2012) found that anxiety in ASD youth decreased from toddlerhood (20%) into childhood (9%), Guerrera et al. (2022) identified an increase with chronological age. In comparison, Strang et al’s. (2012) case-control investigation of youth diagnosed with ASD (6–11 and 12–18 years old) revealed that anxiety levels remained unaffected by age.
Finally, the presentation of anxiety symptoms may differ by gender. Despite overall similarities in psychological symptoms (e.g. rigidity of thought, sensory responsivity), physiological arousal appears more pronounced among girls with ASD (Ambrose et al., 2020). There is also evidence of girls with high functioning ASD having increased anxiety risk compared to boys (Lohr et al., 2017). That said, negligible differences between both genders have been reported (Sukhodolsky et al., 2008). Notably, Sukhodolsky et al., (2008) sampled their group from a help-seeking population (i.e., randomized clinical trial of risperidone), likely confounding their data.
The Current Meta-analysis
The available research on anxiety symptoms and disorders among youth with ASD is characterised by methodological inconsistencies and sample heterogeneity. The current review provides an up-to-date quantitative synthesis of available observational studies to answer the following research questions: What is the point prevalence of anxiety in the international literature on youth diagnosed with ASD? and What (if any) are the moderating effects of methodological (e.g. anxiety measurement) and sample (i.e., IQ, mean age, gender) characteristics on prevalence estimates?
Methods
Search Strategy and Data Sources
The Embase, PubMed, and PsycINFO databases were searched, to identify studies that reported the prevalence of anxiety disorders among ASD youth. Search terms related to ASD (e.g. ‘autistic disorder’, ‘Asperger syndrome’) and anxiety (e.g. ‘anxiety disorder’, ‘generalised anxiety disorder’; see Appendix 1) were verified bya research librarian . Search alerts were reviewed until August 1, 2023, to ensure that recent studies were captured. Search results were imported as XML files from each database and then uploaded onto Covidence software for systematic reviews (Covidence systematic review software, Version 1.0, Veritas Health Innovation).The reference lists of previous meta-analyses on ASD youth and anxiety (Mutluer et al., 2022; van Steensel et al., 2012; van Steensel & Heeman, 2017) were manually searched to identify additional studies that may have been inadvertently missed in the initial database searches. A protocol for this review was registered on the Open Science Framework on 8th August 2023 (https://osf.io/7mtca/).
Eligibility Criteria
Eligible studies needed to include a child or adolescent sample (age ≤ 18 years old, consistent with the age bracket for childhood adopted by the World Health Organisation, 2019) that had received a diagnosis of ASD based on the DSM or International Classification of Diseases (e.g. Autism Diagnostic Observation Schedule, Lord et al., 2000; Autism Diagnostic Interview–Revised, Rutter et al., 2003). Studies also needed to include a validated measure of anxiety, whether self-reported or clinician administered. Consideration only applied to studies published in English from 1970, corresponding with the publication of the DSM II—which marked the removal of the notion that mental disorders were solely attributed to personality-driven reactions (American Psychiatric Association, 1980). Only point-in-time prevalence of anxiety was considered, given issues with potential recall bias associated with lifetime prevalence estimates (Merikangas et al., 2009).
Studies that relied on self-report measures to ascertain ASD caseness in their samples (e.g. Autism Spectrum Quotient, Baron-Cohen et al., 2001; Social Responsiveness Scale, Constantino et al., 2004) were excluded given the increased risk of producing false diagnoses due to a lack of self-insight and/or socially desirable responses (Althubaiti, 2016). Studies that exclusively recruited participants who were currently undergoing psychological or psychotropic treatment, or enrolled in a trial, were also ineligible as these settings typically overrepresent the frequency and severity of anxiety diagnoses among the ASD community (Mutluer et al., 2022). Additionally, studies that used single-item questionnaires which cannot capture the full breadth of a complex mental health construct such as anxiety (Allen et al., 2022), or measures that did not define anxiety (i.e., no reference to a cut-off score) were excluded. Studies with prevalence information and co-occurring anxiety disorders or symptoms with fewer than 20 participants with ASD were also excluded. This threshold minimised sample bias and maximised power (Lai et al., 2019). Lastly, qualitative studies, literature reviews, and grey literature were excluded as the focus of this review was on primary, quantitative data from the peer-reviewed literature.
Study Selection
The first author undertook the search process. To ensure that all papers identified were relevant, the second author independently reviewed all 163 full-text articles. The inter-rater reliability (κ = 0.60; Cohen, 1960) indicated substantial agreement on study eligibility. The few discrepant articles were discussed, and a consensus agreement was then made. Studies were also carefully examined to avoid any duplication of samples, although no overlap was found.
Data Extraction
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Page et al., 2021). Key information was extracted from each study by the first author and checked for accuracy by the second: study characteristics (i.e., lead author, recruitment source, sample size, country of study), sample demographics (child age, gender, IQ, years since receiving ASD diagnosis), and measurement (i.e., diagnostic method to confirm both ASD and anxiety diagnoses).
Reporting Quality of Included Studies
The reporting quality of included studies was evaluated using the Joanna Briggs Institute Prevalence Critical Appraisal Tool (Munn et al., 2020). This 9-item checklist assesses the internal and external validity of prevalence studies as a function of sampling, measurement, and analysis. Each item was rated as ‘yes’, ‘no’, ‘unclear’, or ‘not applicable’. The percentage of studies that met each rating was also calculated.
Statistical Analyses
Data were entered into and analysed using Comprehensive Meta-Analysis Software (Version 4, Biostat Inc, Englewood, NJ, USA) and random-effects modelling (DerSimonian & Laird, 1986).
Prevalence estimates were first grouped by anxiety measurement and pooled. This process involved assigning weights to individual effects based on their inverse variance, or the invariance of a square standard error, prior to pooling (Borenstein et al., 2009). In addition, 95% confidence intervals (CIs) were calculated to detect statistical significance.
Between-study heterogeneity was estimated with Tau (T), akin to the pooled effect SD, and I2, the proportion of variance observed across studies due to inter-study heterogeneity as opposed to sampling error (Higgins et al., 2003). The lower the I2 value, the greater the likelihood that there is consistency across each study’s true effect size. Given that the I2 statistic lacks discriminative in prevalence studies, 95% prediction intervals (PI) were also generated (for Nstudies > 5; Spineli & Pandis, 2020) to determine the range of effect estimates that could be expected in further research (Hout et al., 2016). Finally, a one-study-removed sensitivity analysis was conducted to identify statistical outliers.
Publication bias was assessed using a new tool, the Doi plot, considered to be more robust than the traditional funnel plot for prevalence meta-analyses. The Doi plot illustrates the normal quantile (Z-score) plotted against the effect size and is computed using MetaXL (Version 5.3) (Cheema et al., 2022). Plot asymmetry was quantified with the Luis Furuya-Kanamori index: the closer the LFK index to zero, the more symmetrical the plot (Furuya-Kanamori et al., 2018).
The impact of methodological and sample characteristics on anxiety prevalence was then examined in a series of univariate meta-regressions, with publication date, mean IQ and mean sample age entered as covariates. Cochrane’s QB test was then used to examine the association between anxiety prevalence and gender. Initial plans to analyse differences between parent and child ratings did not proceed due to the underrepresentation of child informants (Bellini, 2004; Kuusikko et al., 2008).
Results
Study Selection
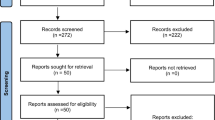
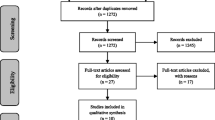
A total of 8084 records were initially identified in the search process. After evaluating the titles and abstracts of each article based on our inclusion and exclusion criteria, a total of 163 reports were identified as potentially meeting the eligibility requirements. Following re-screening and citation searches in Scopus, a final sample of 15 independent studies was identified (Avni & Zachor, 2018; Baribeau et al., 2020; Bellini, 2004; Ben-Itzchak et al., 2020; Boulter et al., 2014; Cholemkery et al., 2014; Dubin et al., 2015; Factor et al., 2017; Guerrera et al., 2022; Kerns et al., 2021; Kim et al., 2000; Kuusikko et al., 2008; Niditch et al., 2012; Simonoff et al., 2008; van Steensel et al., 2012; see Fig. 1).

Flow diagram illustrating study selection process
Reporting Quality of Included Studies
A summary of the JBI critical appraisal ratings is illustrated in Fig. 2, with individual study ratings provided in Appendix 2. None of the studies achieved the highest possible rating, although all recruited their participants via community outreach methods (e.g. dissemination of posters and pamphlets; Nstudies = 6) or registry data (criteria 1). The strict inclusion criteria for this review also ensured that the assessment of both ASD and anxiety was reliable and valid (criteria 6–7). Methodological weaknesses included a reliance on convenience samples and/or limited detail about cluster sampling methods (criterion 2), lack of a priori or post hoc power analyses to justify sample size (criterion 3), and studies not routinely reporting reasons for participant withdrawal—making external validity difficult to assess (criterion 9).

Between-study ratings based on JBI Critical Appraisal Tool (Munn et al., 2020)
Study Characteristics
Included studies spanned the last 23 years (see Table 1) and primarily represented western countries (Nstudies = 10). Most presented cross-sectional data, with three providing baseline estimates derived from longitudinal datasets (Ben-Itzchak et al., 2020; Kerns et al., 2021; van Steensel et al., 2012).
Sample Characteristics
The pooled community sample of 4459 children and adolescents had a mean age of 10 years and 8 months (SD = 2.27, range = 5 to 14 years). Consistent with global patterns of autism, most identified as male (84%, n = 3774; Zablotsky et al., 2019). The sample included youth with severe communication and behavioural deficits (IQ < 75, Nstudies = 3) and those with high-functioning autism (IQ > 75, Nstudies = 8). Autism diagnoses were confirmed through the Autism Diagnostic Interview-Revised (ADI-R; Nstudies = 9) and Autism Diagnostic Observation Schedule (including ADOS-2/G variants; Nstudies = 5), with Bellini (2004) and Dubin et al (2015) relying on medical records. Autism severity was not consistently reported, both in construct and scale. For example, social ineptness was reported as a continuous variable, using the Social Responsiveness Scale (Cholemkery et al., 2014), or based on ordinal frequencies of different behaviours using the Repetitive Behavior Scale (Baribeau et al., 2020)
Publication Bias and Sensitivity Analysis
The pooled findings were robust to publication bias, as suggested by the symmetrical Doi plot and low LFK index (see Fig. 3). A one-study removed sensitive analysis revealed no potential statistical outliers.

Doi plot of normal quantile (Z-score) against the effect size
Prevalence by Anxiety Measure
Fifteen different anxiety measures were used across the included studies (see Table 2). Pooled estimates based on clinician-administered tools (19%, CI = 7 to 40%; Nstudies = 3) were lower than those based on self-reported symptoms (33%, CI = 25 to 40%; PI = 0.110 to 0.657; Nstudies = 12), although this group difference was not significant (QB (1) = 1.633, p = 0.203). Between-study variation was evident, regardless of the focus on anxiety disorders or symptoms. For example, the Kinder-DIPS Diagnostic Interview for Mental Disorders in Children and Adolescents (Cholemkery et al., 2014), based on ICD-10 and DSM-IV-TR criteria, produced the lowest estimate (5%, CI = 2 to 10%), whereas current point prevalence of any anxiety disorder based on the K-SADS for DSM-5 was 43% (CI = 31 to 55%; Guerrera et al., 2022). Similarly, the revised Ontario Child Health Study (OCHS) scale, which corresponds with the DSM-III classification, identified symptoms of concern in 9% of 9- to 14-year-olds with high functioning autism (CI = 5 to 16%; Kim et al., 2000). The highest self-report estimate (60%) was based on the parent version of the Spence Child Anxiety Scale (SCAS-P; Boulter et al., 2014), which aligns with DSM-IIIR and DSM-IV criteria.
Prevalence by Specific Anxiety Disorder
Prevalence estimates for each anxiety disorder, along with the associated heterogeneity statistics, are listed in Table 3. Specific phobia was most common (41%), followed by social anxiety (28%), generalised anxiety (27%), and separation anxiety (14%). Panic attacks (0.6%) and agoraphobia (0.5%) had lower rates, although these estimates were based on considerably fewer studies with smaller sample sizes.
Moderator Analyses
A univariate meta-regression identified IQ as a key sample moderator (R2 = 0.44, p = 0.002): higher IQ explained 44% of the between-study variance across the reported effect sizes. Conversely, mean sample age (R2 = − 0.02, p = 0.4755) and publication date (R2 = − 0.07, p = 0.336) explained very little or none of the variance between studies.
Subgroup analyses revealed an association between gender and anxiety (QB (1) = 35.02, p < .01): anxiety symptoms and disorders had a higher prevalence in boys (0.391, CI = 0.275 to 0.522) compared to girls (0.056, CI = 0.032 to 0.097). This analysis was, however, limited to three studies that provided disaggregated data for gender (Dubin et al., 2015; Factor et al., 2017; Guerrera et al., 2022).
Discussion
This meta-analysis synthesised a body of ASD research that, to date, has encompassed varying perspectives on anxiety prevalence. The findings, based on a community sample of 4459 ASD youth, suggest that 1 in 3 experience clinically elevated anxiety symptoms whilst 1 in 5 are diagnosed with a disorder, most commonly specific phobia, social anxiety, and/or generalised anxiety. These estimates are lower than earlier meta-analyses that included clinical trial populations who may be predisposed to anxiety but also did not adopt strict inclusion criteria relating to the way that ASD diagnosis was established (39.6%, van Steensel et al., 2012), or place restrictions on sample size (42%; White et al., 2009). Notably, the wide prediction intervals reported in this review suggest that more studies are needed to ensure that future meta-analyses in this area can provide more precise estimates of anxiety prevalence.
Not surprisingly, our estimates were characterised by substantial between-study variation—a finding that reflects not only the hallmark heterogeneity associated with ASD (Masi et al., 2017; Mottron & Bzdok, 2020) but also the complexities of measuring mental health as a construct (Migliavaca et al., 2020). Only the SCAS-C and Kinder-DIPS produced narrow confidence intervals (Cholemkery et al., 2014; Kuusikko et al., 2008). In comparison, the SCARED included a confidence interval as low as 13% to as high as 46% (Ben-Itzchak et al., 2020). There is argument that interview schedules and symptom checklists designed for the general population, such as the SCARED, do not accurately capture aspects of anxiety in ASD youth. For example, the item ‘I worry about other people liking me’ conceptualises social fear based on the fear of negative social evaluation; an aspect that tends not to be of concern in ASD populations (Kerns et al., 2014). To date, there remains little consistency and consensus exist around how anxiety in children with ASD should be measured (White et al., 2009). Importantly, progress has been made towards better anxiety measures with sensitivities towards ASD, although these measures still lack widespread use (Mingins et al., 2021). Examples include an adaption of the parent-rated Children’s Yale-Brown Obsessive Compulsive Scale for 5 to 17 year olds, which focuses on behavioural manifestations of anxiety in ASD (Scahill et al., 2019), and a clinician-administered version of the Pediatric Anxiety Rating Scale which was modified based on feedback from a panel of experts, including parents of children with ASD (Maddox et al., 2020). Similarly, the Anxiety Scale for Autism-Adults shows robust psychometrics (Rodgers et al., 2020), although is yet to be adapted for children. Finally, there is the Autism Comorbidity Interview, modified from the K-SADS (Leyfer et al., 2006), which can help contribute to the study of comorbidity in ASD.
The relationship between IQ and anxiety symptom severity should also be interpreted cautiously. Indeed, five of the 10 studies providing these data required participants to have an IQ above 70 (Bellini, 2004; Boulter et al., 2014; Guerrera et al., 2022; Kim et al., 2000; van Steensel et al., 2012), contributing to a high mean IQ for the total pooled sample. That said, there may well be significant differences in anxiety symptomatology between low and high functioning youth with ASD. Greater abstract planning and higher executive functions might facilitate pre-emptive worries that a child may have about the present, their future, or their self-competency (Salazar et al., 2015). An environmental explanation has also been proposed, whereby ASD youth with higher IQ are perceived as more capable and less in need of support to adapt to a neurotypical world (Mingins et al., 2021). However, research has also shown that people with high-functioning ASD may still display poor adaptive behaviours despite not having an intellectual disability (Alvares et al., 2020). Encouraging the use of reliable and valid measures, as discussed above, can certainly aid the inclusion of low-functioning ASD individuals in research.
The relationship between male gender and anxiety identified in this review also needs to be interpreted in the context of the few studies that provided these data. Moreover, two of the three studies in this analysis included samples in the prepubescent phase (age range 8 to 12 years; Dubin et al., 2015; Factor et al., 2017). As important age-related developmental changes occur during adolescence (i.e., pubertal maturation), underrepresenting this older age group can conceal the impact of gender differences (Yoon et al., 2022). Research has shown that as females with ASD transition into later stages of childhood, their levels of anxiety tend to increase at a more accelerated pace than those of males—although girls’ anxiety rates still do not surpass boys’ (Varela et al., 2020). The gender disparity in anxiety noted in the present review may therefore be an overestimate.
Methodological Limitations
Limitations arose during the study screening and data extraction processes that have repercussions for the interpretation of the current findings. First, the reliance on cross-sectional data precludes any inferences about changes in anxiety associated with child age. An observational review across the lifespan can reveal these different developmental manifestations. Second, the findings of this review may not be applicable to developing countries (McConkey, 2022) given the overrepresentation (~ 60%) of studies from western, educated, industrialised, rich, and democratic nations. There remains a need for high-quality, nationally representative epidemiological studies from developing and emerging countries where today’s adolescents primarily reside (United Nations, 2022). That said, whilst included studies were required to be published in the English language, this restriction does not appear to impact the quality or generalisability of meta-analyses, in general (Morrison et al. 2012). Third, the reliance on parental reports may have contributed to inflated estimates. Low to moderate agreement of symptom ratings between parental and ASD children reports have been found, with parent ratings of anxiety often exceeding their child’s (e.g. Kalvin et al., 2020; May et al., 2015). Nonetheless, high child IQ has been shown to attenuate the discrepancy between parental and self-reported anxiety (defined as ≥ 70; Kamp-Becker et al., 2011), an aspect that favours the current findings (Bitsika & Sharpley, 2015). Finally, comparisons between DSM and ICD could not be conducted as only a single study used the latter classification system, despite being well-established in European practice to identify children with an anxiety disorder (Cholemkery et al., 2014; Greaves-Lord et al., 2022). Future research incorporating recent DSM-5 criteria is also needed to determine the level of concordance, and agreement, between DSM versions, depending on the anxiety disorder, given discrepancies among studies that relied on DSM III and DSM-IV tools in this review (e.g. Boulter et al., 2014; Kim et al., 2000). Notably, the DSM-5 has emerged as a highly utilised and reliable diagnostic tool for ASD, potentially contributing to more accurate case identification (Zwaigenbaum et al., 2015).
Conclusions
The current meta-analysis synthesised an extensive body of ASD research that spanned the last 23 years. These data were, however, reliant on clinician and parental reports and based on a sample that primarily included male youth with ASD from westernised countries. Nonetheless, the high estimates for both anxiety symptoms and disorders give impetus to clinicians and researchers to use available tools that can detect ASD-specific symptoms of anxiety and ensure timely and accurate support for those most at risk.
References
*Denotes study included in meta-analysis
Allen, M. S., Iliescu, D., & Greiff, S. (2022). Single item measures in psychological science: A call to action. European Journal of Psychological Assessment: Official Organ of the European Association of Psychological Assessment, 38(1), 1–5. https://doi.org/10.1027/1015-5759/a000699
Althubaiti, A. (2016). Information bias in health research: Definition, pitfalls, and adjustment methods. Journal of Multidisciplinary Healthcare, 9(1), 211–217. https://doi.org/10.2147/JMDH.S104807
Alvares, G. A., Bebbington, K., Cleary, D., Evans, K., Glasson, E. J., Maybery, M. T., Pillar, S., Uljarević, M., Varcin, K., Wray, J., & Whitehouse, A. J. (2020). The misnomer of “high functioning autism”: Intelligence is an imprecise predictor of functional abilities at diagnosis. Autism: The International Journal of Research and Practice, 24(1), 221–232. https://doi.org/10.1177/1362361319852831
Ambrose, K., Adams, D., Simpson, K., & Keen, D. (2020). Exploring profiles of anxiety symptoms in male and female children on the autism spectrum. Research in Autism Spectrum Disorders, 76, 101601. https://doi.org/10.1016/j.rasd.2020.101601
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association.
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.). American Psychiatric Association.
*Avni, Ben-Itzchak E., & Zachor, D. A. (2018). The presence of comorbid ADHD and anxiety symptoms in autism spectrum disorder: Clinical presentation and predictors. Frontiers in Psychiatry, 9, 717–717. https://doi.org/10.3389/fpsyt.2018.00717
*Baribeau, D. A., Vigod, S., Pullenayegum, E., Kerns, C. M., Mirenda, P., Smith, I. M., Vaillancourt, T., Volden, J., Waddell, C., Zwaigenbaum, L., Bennett, T., Duku, E., Elsabbagh, M., Georgiades, S., Ungar, W. J., Zaidman-Zait, A., & Szatmari, P. (2020). Repetitive behavior severity as an early indicator of risk for elevated anxiety symptoms in autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 59(7), 890–899.e3. https://doi.org/10.1016/j.jaac.2019.08.478
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., & Clubley, E. (2001). The Autism-Spectrum Quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. Journal of Autism and Developmental Disorders, 31(1), 5–17. https://doi.org/10.1023/A:1005653411471
*Bellini. S. (2004). Social skill deficits and anxiety in high-functioning adolescents with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 19(2), 78–86. https://doi.org/10.1177/10883576040190020201
*Ben-Itzchak, E., Koller, J., & Zachor, D. A. (2020). Characterization and prediction of anxiety in adolescents with autism spectrum disorder: A longitudinal study. Journal of Abnormal Child Psychology, 48(9), 1239–1249. https://doi.org/10.1007/s10802-020-00673-0
Bitsika, V., & Sharpley, C. F. (2015). Differences in the prevalence, severity and symptom profiles of depression in boys and adolescents with an autism spectrum disorder versus normally developing controls. International Journal of Disability, Development, and Education, 62(2), 158–167. https://doi.org/10.1080/1034912X.2014.998179
Borenstein, M., Hedges, L. V., Higgins, J. P. T., & Rothstein, H. R. (2009). Introduction to meta-analysis. John Wiley & Sons Ltd.
*Boulter, C., Freeston, M., South, M., & Rodgers, J. (2014). Intolerance of uncertainty as a framework for understanding anxiety in children and adolescents with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(6), 1391–1402. https://doi.org/10.1007/s10803-013-2001-x
Chambers, W. J., Puig-Antich, J., Hirsch, M., Paez, P., Ambrosini, P. J., Tabrizi, M. A., & Davies, M. (1985). The assessment of affective disorders in children and adolescents by semi structured interview: Test-retest reliability of the schedule for affective disorders and schizophrenia for school-age children, present episode version. Archives of General Psychiatry, 42(7), 696–702. https://doi.org/10.1001/archpsyc.1985.01790300064008
Cheema, H. A., Shahid, A., Ehsan, M., & Ayyan, M. (2022). The misuse of funnel plots in meta-analyses of proportions: Are they really useful? Clinical Kidney Journal, 15(6), 1209–1210. https://doi.org/10.1093/ckj/sfac035
*Cholemkery, H., Mojica, L., Rohrmann, S., Gensthaler, A., & Freitag, C. M. (2014). Can autism spectrum disorders and social anxiety disorders be differentiated by the Social Responsiveness Scale in children and adolescents? Journal of Autism and Developmental Disorders, 44(5), 1168–1182. https://doi.org/10.1007/s10803-013-1979-4
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational and Psychological Measurement, 20, 37–46.
Constantino, J. N., Gruber, C. P., Davis, S., Hayes, S., Passanante, N., & Przybeck, T. (2004). The factor structure of autistic traits. Journal of Child Psychology & Psychiatry., 2004(45), 719–726. https://doi.org/10.1111/j.1469-7610.2004.00266.x
DerSimonian, R., & Laird, N. (1986). Meta-analysis in clinical trials. Controlled Clinical Trials, 7(3), 177–188. https://doi.org/10.1016/0197-2456(86)90046-2
*Dubin, A. H., Lieberman-Betz, R., & Michele Lease, A. (2015). Investigation of individual factors associated with anxiety in youth with autism spectrum disorders. Journal of Autism and Developmental Disorders, 45(9), 2947–2960. https://doi.org/10.1007/s10803-015-2458-x
Edirisooriya, M., Dykiert, D., & Auyeung, B. (2021). IQ and internalizing symptoms in adolescents with ASD. Journal of Autism and Developmental Disorders, 51(11), 3887–3907. https://doi.org/10.1007/s10803-020-04810-y
*Factor, R. S., Ryan, S. M., Farley, J. P., Ollendick, T. H., & Scarpa, A. (2017). Does the presence of anxiety and ADHD symptoms add to social impairment in children with autism spectrum disorder? Journal of Autism and Developmental Disorders, 47(4), 1122–1134. https://doi.org/10.1007/s10803-016-3025-9
Furuya-Kanamori, L., Barendregt, J. J., & Doi, S. A. R. (2018). A new improved graphical and quantitative method for detecting bias in meta-analysis. International Journal of Evidence-based Healthcare, 16(4), 195–203. https://doi.org/10.1097/XEB.0000000000000141
Greaves-Lord, K., Skuse, D., & Mandy, W. (2022). Innovations of the ICD-11 in the field of autism spectrum disorder: A psychological approach. Clinical Psychology in Europe, 4(Spec Issue), e10005. https://doi.org/10.32872/cpe.10005
*Guerrera, S., Pontillo, M., Tata, M. C., Di Vincenzo, C., Bellantoni, D., Napoli, E., Valeri, G., & Vicari, S. (2022). Anxiety in autism spectrum disorder: Clinical characteristics and the role of the family. Brain Sciences, 12(12), 1597. https://doi.org/10.3390/brainsci12121597
Higgins, J. P., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ (Clinical research ed.), 327(7414), 557–560. https://doi.org/10.1136/bmj.327.7414.557
Hout, J., Ioannidis, J., Rovers, M., & Goeman, J. (2016). Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open, 6(7), e010247–e010247. https://doi.org/10.1136/BMJOPEN-2015-010247
Kalvin, C. B., Marsh, C. L., Ibrahim, K., Gladstone, T. R., Woodward, D., Grantz, H., Ventola, P., & Sukhodolsky, D. G. (2020). Discrepancies between parent and child ratings of anxiety in children with autism spectrum disorder. Autism Research: Official Journal of the International Society for Autism Research, 13(1), 93–103. https://doi.org/10.1002/aur.2220
Kamp-Becker, I., Schröder, J., Muehlan, H., Remschmidt, H., Becker, K., & Bachmann, C. J. (2011). Health-related quality of life in children and adolescents with autism spectrum disorder. Zeitschrift fur Kinder- und Jugendpsychiatrie und Psychotherapie, 39(2), 123–131. https://doi.org/10.1024/1422-4917/a000098
*Kim, J. A., Szatmari, P., Bryson, S. E., Streiner, D. L., & Wilson, F. J. (2000). The prevalence of anxiety and mood problems among children with autism and Asperger syndrome. Autism: The International Journal of Research and Practice, 4(2), 117-132. https://doi.org/10.1177/1362361300004002002
Kerns, C. M., Kendall, P. C., Berry, L., Souders, M. C., Franklin, M. E., Schultz, R. T., Miller, J., & Herrington, J. (2014). Traditional and atypical presentations of anxiety in youth with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44(11), 2851–2861. https://doi.org/10.1007/s10803-014-2141-7
*Kerns, C. M., Winder-Patel, B., Iosif, A. M., Nordahl, C. W., Heath, B., Solomon, M., & Amaral, D. G. (2021). Clinically significant anxiety in children with autism spectrum disorder and varied intellectual functioning. Journal of Clinical Child and Adolescent Psychology, 50(6), 780–795. https://doi.org/10.1080/15374416.2019.1703712
*Kuusikko, S., Pollock-Wurman, R., Jussila, K., Carter, A. S., Mattila, M.-L., Ebeling, H., Pauls, D. L., & Moilanen, I. (2008). Social anxiety in high-functioning children and adolescents with autism and Asperger syndrome. Journal of Autism and Developmental Disorders, 38(9), 1697–1709. https://doi.org/10.1007/s10803-008-0555-9
Lai, M. C., Kassee, C., Besney, R., Bonato, S., Hull, L., Mandy, W., Szatmari, P., & Ameis, S. H. (2019). Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. The Lancet Psychiatry, 6(10), 819–829. https://doi.org/10.1016/S2215-0366(19)30289-5
Leyfer, O. T., Folstein, S. E., Bacalman, S., Davis, N. O., Dinh, E., Morgan, J., Tager-Flusberg, H., & Lainhart, J. E. (2006). Comorbid psychiatric disorders in children with autism: Interview development and rates of disorders. Journal of Autism and Developmental Disorders, 36(7), 849–861. https://doi.org/10.1007/s10803-006-0123-0
Liebowitz, M. R. (1987). Liebowitz Social Phobia Scale. Modern Problems of Pharmacopsychiatry, 22, 143–171.
Lohr, W. D., Daniels, K., Wiemken, T., Williams, P. G., Kelley, R. R., Kuravackel, G., & Sears, L. (2017). The screen for child anxiety-related emotional disorders is sensitive but not specific in identifying anxiety in children with high-functioning autism spectrum disorder: A pilot comparison to the Achenbach System of empirically based assessment scales. Frontiers in Psychiatry, 8. https://doi.org/10.3389/fpsyt.2017.00138
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., DiLavore, P. C., et al. (2000). The autism diagnostic observation schedule – generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223.
Maddox, B. B., Lecavalier, L., Miller, J. S., Pritchett, J., Hollway, J., White, S. W., Gillespie, S., Evans, A. N., Schultz, R. T., Herrington, J. D., Bearss, K., & Scahill, L. (2020). Reliability and validity of the Pediatric Anxiety Rating Scale modified for autism spectrum disorder. Autism: The International Journal of Research and Practice, 24(7), 1773–1782. https://doi.org/10.1177/1362361320922682
Masi, A., DeMayo, M. M., Glozier, N., & Guastella, A. J. (2017). An overview of autism spectrum disorder, heterogeneity and treatment options. Neuroscience Bulletin, 33(2), 183–193. https://doi.org/10.1007/s12264-017-0100-y
May, T., Cornish, K., & Rinehart, N. J. (2015). Parent-child agreement using the Spence Children’s Anxiety Scale and a thermometer in children with autism spectrum disorder. Autism Research and Treatment, 2015, 315495. https://doi.org/10.1155/2015/315495
Mayes, S. D., Calhoun, S. L., Aggarwal, R., Baker, C., Mathapati, S., Molitoris, S., & Mayes, R. D. (2013). Unusual fears in children with autism. Research in Autism Spectrum Disorders, 7(1), 151–158. https://doi.org/10.1016/j.rasd.2012.08.002
Mazefsky, M. O., Anderson, R., Conner, C. M., & Minshew, N. (2011). Child behavior checklist scores for school-aged children with autism: Preliminary evidence of patterns suggesting the need for referral. Journal of Psychopathology and Behavioral Assessment, 33(1), 31–37. https://doi.org/10.1007/s10862-010-9198-1
Mazurek, M. O., & Kanne, S. M. (2010). Friendship and internalizing symptoms among children and adolescents with ASD. Journal of Autism and Developmental Disorders, 40(12), 1512–1520. https://doi.org/10.1007/s10803-010-1014-y
Mazurek, M. O., & Petroski, G. F. (2015). Sleep problems in children with autism spectrum disorder: Examining the contributions of sensory over-responsivity and anxiety. Sleep Medicine, 16(2), 270–279. https://doi.org/10.1016/j.sleep.2014.11.006
McConkey, R. (2022). Responding to autism in low- and middle-income countries (LMIC): What to do and what not to do. Brain Sciences, 12(11), 1475. https://doi.org/10.3390/brainsci12111475
Merikangas, K. R., Nakamura, E. F., & Kessler, R. C. (2009). Epidemiology of mental disorders in children and adolescents. Dialogues in Clinical Neuroscience, 11(1), 7–20. https://doi.org/10.31887/DCNS.2009.11.1/krmerikangas
Migliavaca, C. B., Stein, C., Colpani, V., Barker, T. H., Munn, Z., & Falavigna, M. (2020). How are systematic reviews of prevalence conducted? A methodological study. BMC Medical Research Methodology, 20(1), 96–96. https://doi.org/10.1186/s12874-020-00975-3
Mingins, J. E., Tarver, J., Waite, J., Jones, C., & Surtees, A. D. (2021). Anxiety and intellectual functioning in autistic children: A systematic review and meta-analysis. Autism: The International Journal of Research and Practice, 25(1), 18–32. https://doi.org/10.1177/1362361320953253
Morrison, A., Polisena, J., Husereau, D., Moulton, K., Clark, M., Fiander, M., Mierzwinski-Urban, M., Clifford, T., Hutton, B., & Rabb, D. (2012). The effect of English-language restriction on systematic review-based metaanalyses: a systematic review of empirical studies. International journal of technology assessment in health care, 28(2), 138–144. https://doi.org/10.1017/S0266462312000086
Mottron, L., & Bzdok, D. (2020). Autism spectrum heterogeneity: fact or artifact? Molecular Psychiatry, 25(12), 3178–3185. https://doi.org/10.1038/s41380-020-0748-y
Munn, Z., Moola, S., Lisy, K., Riitano, D., & Tufanaru, C. (2020). Chapter 5: Systematic reviews of prevalence and incidence. In E. Aromataris, & E. Z. Munn (Eds.). JBI Manual for Evidence Synthesis. JBI. https://synthesismanual.jbi.global. https://doi.org/10.46658/JBIMES-20-06. Accessed 24 Sept 2023
Mutluer, T., Aslan Genç, H., Özcan Morey, A., Yapici Eser, H., Ertinmaz, B., Can, M., & Munir, K. (2022). Population-based psychiatric comorbidity in children and adolescents with autism spectrum disorder: A meta-analysis. Frontiers in Psychiatry, 13, 856208–856208. https://doi.org/10.3389/fpsyt.2022.856208
Niditch, L. A., Varela, R. E., Kamps, J. L., & Hill, T. (2012). Exploring the association between cognitive functioning and anxiety in children with autism spectrum disorders: The role of social understanding and aggression. Journal of Clinical Child and Adolescent Psychology, 41(2), 127–137. https://doi.org/10.1080/15374416.2012.651994
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., et al. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Systematic reviews, 10(1), 89. https://doi.org/10.1186/s13643-021-01626-4
Rodgers, J., Farquhar, K., Mason, D., Brice, S., Wigham, S., Ingham, B., Freeston, M., & Parr, J. R. (2020). Development and initial evaluation of the Anxiety Scale for Autism-Adults. Autism in Adulthood: Challenges and Management, 2(1), 24–33. https://doi.org/10.1089/aut.2019.0044
Rutter, M., Le Couteur, A., Lord, C., et al. (2003). Autism diagnostic interview-revised (Vol. 29, p. 30). Western Psychological Services.
Salazar, F., Baird, G., Chandler, S., Tseng, E., O’Sullivan, T., Howlin, P., & Simonoff, E. (2015). Co-occurring psychiatric disorders in preschool and elementary school-aged children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(8), 2283–2294.
Scahill, L., Lecavalier, L., Schultz, R. T., Evans, A. N., Maddox, B. B., Pritchett, J., et al. (2019). Development of the parent-rated anxiety scale for youth with autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 58, 887–896. https://doi.org/10.1016/j.jaac.2018.10.016
*Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 921–929. https://doi.org/10.1097/CHI.0b013e318179964f
Spineli, L. M., & Pandis, N. (2020). Prediction interval in random-effects meta-analysis. American journal of orthodontics and dentofacial orthopedics : official publication of the American Association of Orthodontists, its constituent societies, and the American Board of Orthodontics, 157(4), 586–588. https://doi.org/10.1016/j.ajodo.2019.12.011
Strang, J. F., Kenworthy, L., Daniolos, P., Case, L., Wills, M. C., Martin, A., et al. (2012). Depression and anxiety symptoms in children and adolescents with autism spectrum disorders without intellectual disability. Research in Autism Spectrum Disorders, 6(1), 406–412.
Sukhodolsky, D. G., Scahill, L., Gadow, K. D., Arnold, L. E., Aman, M. G., Mcdougle, C. J., McCracken, J. T., Tierney, E., Williams White, S., Lecavalier, L., & Vitiello, B. (2008). Parent-rated anxiety symptoms in children with pervasive developmental disorders: Frequency and association with core autism symptoms and cognitive functioning. Journal of Abnormal Child Psychology, 36(1), 117. https://doi.org/10.1007/s10802-007-9165-9
United Nations. (2022). World population prospects 2022 (p. 2022). UN Department for Economic and Social Affairs (UN DESA), Population Division.
*van Steensel, F. J. A., Bögels, S. M., & Dirksen, C. D. (2012). Anxiety and quality of life: Clinically anxious children with and without autism spectrum disorders compared. Journal of Clinical Child and Adolescent Psychology, 41(6), 731–738. https://doi.org/10.1080/15374416.2012.698725
van Steensel, F. J. A., Bögels, S., & Perrin, S. (2011). Anxiety disorders in children and adolescents with autistic spectrum disorders: A meta-analysis. Clinical Child and Family Psychology Review, 14(3), 302–317. https://doi.org/10.1007/s10567-011-0097-0
van Steensel, F. J. A., & Heeman, E. (2017). anxiety levels in children with autism spectrum disorder: A meta-analysis. Journal of Child and Family Studies, 26(7), 1753–1767. https://doi.org/10.1007/s10826-017-0687-7
Varela, R. E., DuPont, R., Kamps, J. L., Weems, C. F., Niditch, L., Beaton, E. A., & Pucci, G. (2020). Age differences in expression of generalized and social anxiety among youth with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(3), 730–740. https://doi.org/10.1007/s10803-019-04289-2
White, S. W., Oswald, D., Ollendick, T., & Scahill, L. (2009). Anxiety in children and adolescents with autism spectrum disorders. Clinical Psychology Review, 29(3), 216–229. https://doi.org/10.1016/j.cpr.2009.01.003
World Health Organisation. (2019). The global strategy for women’s, children’s, and adolescents’ health (2016–2030). https://www.who.int/publications/i/item/A71-19. Accessed 24 Sept 2023.
Yoon, N., Huh, Y., Lee, H., Kim, J. I., Lee, J., Yang, C. M., Jang, S., Ahn, Y. D., Oh, M. R., Lee, D. S., Kang, H., & Kim, B. N. (2022). Alterations in social brain network topology at rest in children with autism spectrum disorder. Psychiatry investigation, 19(12), 1055–1068. https://doi.org/10.30773/pi.2022.0174
Zablotsky, B., Black, L. I., Maenner, M. J., Schieve, L. A., Danielson, M. L., Bitsko, R. H., Blumberg, S. J., Kogan, M. D., & Boyle, C. A. (2019). Prevalence and trends of developmental disabilities among children in the United States: 2009-2017. Pediatrics, 144(4), e20190811. https://doi.org/10.1542/peds.2019-0811
Zwaigenbaum, L., Bauman, M. L., Stone, W. L., Yirmiya, N., Estes, A., Hansen, R. L., McPartland, J. C., Natowicz, M. R., Choueiri, R., Fein, D., Kasari, C., Pierce, K., Buie, T., Carter, A., Davis, P. A., Granpeesheh, D., Mailloux, Z., Newschaffer, C., Robins, D., et al. (2015). Early identification of autism spectrum disorder: Recommendations for practice and research. Pediatrics, 136(Suppl 1), S10–S40. https://doi.org/10.1542/peds.2014-3667C
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions
Author information
Authors and Affiliations
Contributions
HNT-S: data curation, methodology, formal analysis, writing original draft, and visualization. DSD: conceptualization, methodology, supervision, writing, review, and editing.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thiele-Swift, H.N., Dorstyn, DS. Anxiety Prevalence in Youth with Autism: A Systematic Review and Meta-analysis of Methodological and Sample Moderators. Rev J Autism Dev Disord (2024). https://doi.org/10.1007/s40489-023-00427-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40489-023-00427-w