
Abstract
Introduction
Chronic graft-versus-host disease (GVHD) following hematopoietic stem cell transplantation (HSCT) is associated with poor health-related quality of life (HRQoL) and functional status. However, few studies have evaluated chronic GVHD–related disability and specific activity limitations from a patient perspective. The objective of this analysis was to assess physical, cognitive, and work disability, and describe factors predictive of disability in patients with chronic GVHD in the potentially employable general workforce.
Methods
The cross-sectional, online, Living With Chronic GVHD Patient Survey was administered in 2020 to adult US patients who reported an active chronic GVHD diagnosis (i.e., within the previous 5 years) following HSCT. Data included demographics, diagnosis, work status, chronic GVHD symptoms per the Lee Symptom Scale (LSS), and effects on daily living activities. Descriptive and correlational analyses informed composite disability definitions: (1) severe cognitive disability, (2) severe physical disability, and (3) work disability.
Results
Of 137 respondents with GVHD included in this analysis, 47.0% reported severe cognitive disability, and approximately two-thirds each reported severe physical disability (67.4%) and work disability (62.8%). Chronic GVHD severity/duration, symptoms (Lee Symptom Scale), and number of transplant specialists consulted were associated with all types of disability (univariable analyses). Severe cognitive disability was associated with the number of transplant specialists consulted, severe physical disability with female sex, and work disability with nonwhite race.
Conclusions
In this analysis, we found that the presence of specific symptoms and the number of transplant specialists consulted were associated with all types of severe disability; female sex was predictive of severe physical disability and nonwhite race of work disability. These findings add to the understanding of chronic GVHD-associated disability, suggest a need for improved social support for patients, and highlight potential indicators for those most in need.
Plain Language Summary
Chronic graft-versus-host disease (GVHD) is a possible serious complication that can occur after someone has received a bone marrow or stem cell transplant from another person. Symptoms of chronic GVHD can be severe and can affect quality of life. To better understand exactly how chronic GVHD affects quality of life, we asked adults in the USA with chronic GVHD to fill out a survey. The objective of this research was to find out how chronic GVHD affects daily activities and work. The survey asked about physical activities including personal hygiene, eating, shopping, and ability to use the restroom, and the survey asked about mental tasks including managing personal finances and interactions with other people. The survey also asked questions about work, such as the need to take disability leave or to leave a job due to chronic GVHD. Many people with chronic GVHD who completed the survey said they had severe difficulty with mental and/or physical tasks, and many had work-related disability. People with more severe chronic GVHD who had met with many transplant specialists were more likely to have difficulty with mental and physical tasks and also to have work disability. Women who completed the survey were more likely to report severe physical disability than men, and nonwhite participants were more likely to report work disability. The results of this survey highlight a need for improved social support for patients with chronic GVHD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? | |
Chronic graft-versus-host disease (GVHD) following hematopoietic stem cell transplantation (HSCT) is associated with poor health-related quality of life (HRQoL) and functional status. | |
Data are lacking on GVHD-related disability, particularly regarding activity limitations from the patient perspective. | |
The objective of this analysis is to assess physical, cognitive, and work disability and describe factors predictive of disability in patients with chronic GVHD in the potentially employable general workforce using patient-reported data. | |
What was learned from the study? | |
Severe cognitive, severe physical, and work disability were associated with chronic GVHD, and symptom burden, sex, race, and transplant history were predictive of disability. | |
These findings help to define and better understand chronic GVHD-associated disability. |
Introduction
Allogeneic hematopoietic stem cell transplantation (HSCT) represents the only potentially curative treatment modality for many high-risk hematologic malignancies and bone marrow disorders [1,2,3]. Despite routine use of immunosuppressive prophylaxis, chronic graft-versus-host disease (GVHD) develops in approximately 30% to 50% of HSCT recipients [4,5,6,7,8] and is a leading cause of late morbidity and mortality post-transplant [7, 9,10,11]. Chronic GVHD is characterized by multiorgan pathology and burdensome symptoms that negatively impact health-related quality of life (HRQoL) and physical function [12, 13]. Studies of long-term HSCT survivors have demonstrated that active chronic GVHD is associated with significantly impaired physical function compared with patients without chronic GVHD or those with resolved chronic GVHD [14, 15]. Further, patients with chronic GVHD may be unable to return to work [16, 17], which further underlines the potential impact of GVHD-related disability.
Despite the growing evidence of physical and functional impairment associated with chronic GVHD, there are limited data on disability as an outcome measure of disease burden or response to treatment in clinical trials [18]. The World Health Organization defines disability as any physical or mental impairment that limits people’s ability to do certain activities or interact with their environment and encompasses impairment in physical or mental functioning, activity limitation, and participation restrictions [18, 19]. Few studies have evaluated disability specifically in the context of chronic GVHD, and attempts to describe disability have focused largely on physician-assessed clinical manifestations [e.g., Flowers criteria (bronchiolitis obliterans, keratoconjunctivitis sicca, scleroderma, joint/fascia involvement, and esophageal stricture)] [16, 18]. A previous study from the Chronic GVHD Consortium explored definitions of disability among patients with chronic GVHD based on Flowers criteria as well as general health status (Karnofsky performance status) and patient-reported measures (Human Activity Profile) [18]. Disability as defined by Flowers was associated with worsening Human Activity Profile and Karnofsky performance status scores over an 18-month follow-up period. Further, progressive disability correlated with low response to therapies [18].
Chronic GVHD–related disability in the context of specific activity limitations and restrictions from a patient perspective still needs to be better characterized. Further, identification of factors associated with chronic GVHD–related disability could aid in (1) recognition of patients most at risk for limitations and (2) optimization of disease management strategies. Previously reported findings from the online Living With Chronic GVHD Patient Survey have demonstrated that chronic GVHD symptoms severely interfere with patients’ ability to perform activities of daily living [20, 21]. Many respondents reported adverse employment and economic outcomes due to their chronic GVHD [20, 21]. Notably, in a separate study, inability to work was significantly associated with mortality among patients with chronic GVHD based on a multivariable analysis of sociodemographic factors [17]. Thus, our objective was to assess physical, cognitive, and work disability and identify factors contributing to disability in patients with chronic GVHD in the potentially employable general workforce using direct patient input from the Living With Chronic GVHD Patient Survey.
Methods
Study Design and Respondents
The Living With Chronic GVHD Patient Survey was an online, noninterventional, cross-sectional survey administered in May–August 2020 to adults living in the USA. Participants were recruited through consumer panels (survey providers) and patient advocacy groups via email blasts, newsletters, and Facebook posts [20]. Further details regarding advocacy groups have been described [20]. Survey eligibility criteria included respondent self-reports of receipt of prior allogeneic HSCT, chronic GVHD diagnosis from a healthcare provider, and active chronic GVHD within the past 5 years. Full survey details have been previously published [20]. In brief, the survey had 74 questions, and respondents were asked to provide information on demographics, disease diagnosis, chronic GVHD symptoms per the Lee Symptom Scale (LSS), impact of the respondent’s most severe chronic GVHD symptoms on activities of daily living, and work status. The LSS assesses 30 individual symptoms grouped into seven subdomains (eyes, energy, lung, mouth, nutrition, psychological, and skin); total LSS score ranges from 0 to 100, with higher scores indicating greater symptom burden [22]. Activities of daily living were graded on a scale of 0 (“chronic GVHD had no effect on my daily activities”) to 10 (“chronic GVHD completely prevented me from doing my daily activities”).
Definitions of Cognitive, Physical, and Work Disability
Descriptive and correlational analyses were used to create three composite definitions of disability: (1) severe cognitive disability, (2) severe physical disability, and (3) work disability. Assessment of cognitive disability included evaluation of the impact of chronic GVHD on specific activities of daily living, including managing personal finances, using a computer, and interacting socially with friends and family. Analysis of physical disability included effects on personal hygiene, dressing, eating, ability to use the restroom, ability to move around the house, and ability to get around outside the house as well as ability to prepare meals, shop, and do housework. A score of at least 7 (0–10 scale) on any item related to cognitive or physical disability was considered a severe limitation in the respective domain. Work disability was assessed based on two questions related to work status (“ever taken disability leave because of chronic GVHD” and “ever left a job because of chronic GVHD”). Respondents who answered “yes” to at least 1 of these questions were considered to have experienced work disability. Composite disability in each of the three subdomains was calculated as the percentage of respondents meeting the criteria for severe limitation on any individual item in the cognitive or physical domains or any disability in the work domain when symptoms were at their worst.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice. The survey was reviewed and approved by the New England Institutional Review Board before administration. All respondents provided informed consent via an online consent form before initiation of the survey. All study participants from the initial study consented to their data being used for further research purposes.
Statistical Analyses
Only respondents who were employed (reporting full- or part-time employment at time of transplant) or considered potentially employable in the general workforce (responses of unemployed and seeking employment, unemployed and not seeking employment, disabled or unable to work, or other) at the time of transplant were included in this analysis. Respondents identifying as self-employed, retired, or homemaker were excluded. Exclusion of self-employed respondents was based on the potential lack of required work hours, and therefore, the impact on employment may be different between self-employed versus standard employed participants. Respondent demographics and clinical characteristics were summarized using descriptive statistics.
To identify factors associated with disability, a two-step regression analysis was undertaken. First, univariable regression models were used to estimate the unconditional (marginal) association between each disability outcome and each predictor variable, with likelihood-ratio tests against the null model (excluding the variable) used to estimate the association. At the second step, predictor variables meeting threshold (P < 0.2) were considered for inclusion in a multivariable logistic regression model to estimate conditional associations. A backward step selection approach was adopted for the final model, with application of a 0.05 significance level.
Results
Respondents
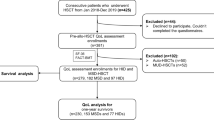
As published previously [20], of 580 participants who entered the survey screener, 165 met all eligibility criteria and completed the survey (full analysis set). Briefly, primary reasons for study exclusion among initial survey respondents included declined or missing consent (n = 186), not having received prior HSCT (n = 111 including unknown/missing response), and not having a diagnosis of chronic GVHD (n = 48 including unknown). The majority of included respondents were recruited from BMT InfoNet (n = 110). Twenty-eight respondents in the full analysis set reported being self-employed, retired, or a homemaker at the time of their most recent transplant and were excluded from this analysis; the remaining 137 respondents were considered part of the potentially employable general workforce (i.e., employed or potentially interested in employment at the time of most recent transplant) and were included in this analysis. Demographics and clinical characteristics of the potentially employable respondent population were similar to those previously reported for the full analysis set (Table 1) [20]. Among the 137 respondents in the potentially employable analysis set, median (range) age was 54.0 (18–76) years, 88 (64.2%) were women, and 110 (80.3%) were white. More than half of respondents [n = 81 (59.1%)] had a bachelor’s degree [n = 44 (32.1%)] or advanced degree [n = 37 (27.0%)]. Among respondents considered potentially employable at the time of transplant, 59 (43.1%) reported being disabled or unable to work, and 28 (20.4%) and 12 (8.8%) reported being employed full- and part-time, respectively, at the time they completed the survey. Median (range) chronic GVHD duration was 4.5 (0.1–36.7) years. Respondents reported seeing a median (range) of 4.0 (0–10) specialists for their chronic GVHD, which most frequently included hematologists/oncologists (n = 128 [93.4%]) and ophthalmologists [n = 88 (64.2%)].
Disability
Nearly half of evaluable respondents [63/134 (47.0%)] met the study criteria for severe cognitive limitations based on their ability to perform specific tasks, and approximately two-thirds each met the criteria for severe physical disability [91/135 (67.4%)] and work disability [86/137 (62.8%)] associated with chronic GVHD (Fig. 1). With respect to cognitive disability, the greatest percentage of survey respondents met study criteria for severe limitations in their ability to interact socially with friends or family members [56/137 (40.9%); Fig. 2]. The highest rates of study-defined physical disability occurred for subdomains of shopping [60/137 (43.8%)], housework [57/137 (41.6%)], and eating [51/137 (37.2%); Fig. 3]. More than half of survey respondents [78/137 (56.9%)] reported taking at least one disability leave owing to chronic GVHD (Fig. 4).

Respondents reporting severe cognitive, severe physical, or work disability. The analysis was conducted in the potentially employable general workforce subset (N = 137). Respondents were asked to consider impact of chronic GVHD at the time symptoms were at their worst. Missing observations [i.e., respondents reporting that any of the activity limitation items were not applicable with no report of severe disability (≥ 7 on a 0–10 scale in any of the other items)] were not included in the percentage calculations; data labels above bars indicate n/N evaluable. Severe cognitive disability was defined as severe limitation (≥ 7 on a 0–10 scale) in ≥ 1 of the specified items (managing personal finances, social interaction, and computer use). Severe physical disability was defined as severe limitation (≥ 7 on a 0–10 scale) in ≥ 1 of the specified items (personal hygiene, dressing, eating, using the restroom, moving around the house, preparing meals, shopping, doing housework, and getting around outside the house). Work disability was defined as response of “yes” on ≥ 1 of the specified items (took disability leave or left a job). GVHD graft-versus-host disease

Respondents reporting limitations in specific cognitive activities. The analysis was conducted in the potentially employable general workforce subset (N = 137). Respondents were asked to consider impact of chronic GVHD at the time symptoms were at their worst. Severe limitation was defined as a score of ≥ 7 on a 0–10 scale. GVHD graft-versus-host disease

Respondents reporting limitations in specific physical activities. The analysis was conducted in the potentially employable general workforce subset (N = 137). Respondents were asked to consider impact of chronic GVHD at the time symptoms were at their worst. Severe limitation was defined as a score of ≥ 7 on a 0–10 scale. GVHD graft-versus-host disease

Respondents reporting limitations in specific work ability. The analysis was conducted in the potentially employable general workforce subset (N = 137). Respondents were asked to consider impact of chronic GVHD at the time symptoms were at their worst. Severe limitation was defined as a score of ≥ 7 on a 0–10 scale. GVHD graft-versus-host disease
Factors Associated with Disability
Results of a univariable analysis demonstrated that chronic GVHD severity/duration, LSS symptoms (eye, mouth, lung, skin, nutrition, energy, and psychological), and number of transplant specialists consulted were associated with all types of disability (Table 2). Furthermore, number of treatments was associated with both severe cognitive and physical disability. Nonwhite race was predictive of work disability. Age, sex, education, employment, and annual income were not associated with any type of disability in the univariable analysis, although female sex was associated with the physical disability attributes of preparing meals, shopping, and housework (chi-square test, 8.0; P = 0.005).
Findings from a multivariable analysis of factors associated with disability demonstrated that LSS skin and psychological symptoms as well as number of transplant specialists consulted remained significantly associated with severe cognitive disability (Table 3). Female sex and LSS mouth, nutrition, and energy symptoms were associated with physical disability. Nonwhite race and LSS energy symptoms were associated with work disability.
Discussion
Among HSCT survivors who completed the Living With Chronic GVHD Patient Survey and were considered part of the potentially employable general workforce at the time of their most recent transplant, nearly half of respondents (47.0%) met the study criteria for severe cognitive limitations based on their ability to perform specific tasks, and approximately two-thirds met the criteria for severe physical disability and work disability (67.4% and 62.8%, respectively) associated with their chronic GVHD. In particular, more than one-third of respondents were categorized in this analysis as having severe limitations in the individual domains of interacting socially with friends/family members, shopping, housework, eating, and ability to get around outside of the house. More than half (57%) took disability leave from work, with 28% leaving a job due to chronic GVHD. These findings highlight the immense burden of chronic GVHD on activities of daily living that may be underappreciated with respect to its impact on HRQoL. Our findings are largely consistent with previous studies that demonstrated the negative overall impact of chronic GVHD on HRQoL, including the impact on psychological state, mental functioning, social interactions, and physical functioning and functional status [12,13,14,15, 23,24,25,26]. Furthermore, two longitudinal studies of patients who underwent HSCT demonstrated neurocognitive and motor dexterity deficits 80 days after transplant that often improved by 1 year, although deficits persisted for at least 40% of survivors at 5 years [27, 28]. Although neither study focused on patients with chronic GVHD, those receiving chronic GVHD treatment experienced impaired motor dexterity but not cognitive ability 1 year following HSCT [28].
Data that address the association between disability and chronic GVHD are limited. Previous analyses have begun to explore definitions of disability in chronic GVHD, demonstrating associations with chronic GVHD organ impairment, functional status, activity, and employment, as well as response to therapy. Analyses from the Living With Chronic GVHD Patient Survey have demonstrated that patients frequently experience protracted and severe symptoms that interfere with both basic and instrumental activities of daily living [20]. Moreover, many survey respondents reported adverse employment outcomes including missed time as well as lost career opportunities and income as a result of their chronic GVHD [21]. Findings from the present analysis build upon these previous reports to further delineate the effects of physical, cognitive, and work disability among patients with chronic GVHD. Exploratory analyses revealed several factors potentially associated with composite disability, including specific symptoms as assessed by the LSS and the number of transplant specialists consulted, which were generally predictive of all types of disability in the univariable analysis. Interestingly, on multivariable analysis, the number of transplant specialists consulted remained significantly associated with severe cognitive disability only, female sex with severe physical disability, and nonwhite race with work disability. It remains unclear what factors contributed to the disproportionate effects of chronic GVHD on physical disability in women versus men as the survey did not collect information on the physical demands of respondents’ lives. The effects of nonwhite race on work disability may reflect the diminished capacity to leverage support networks and provisions allowing access to work (e.g., remote home-based work) that minority communities face in general [29,30,31]. However, these explanations are speculative. Additional studies are needed to confirm and further explore the relationships.
This study was potentially limited by several factors. Recruitment was restricted to patient advocacy groups and consumer panels. Additionally, self-employed respondents were excluded based on the assumption that set working hour requirements differed from those of standard employed respondents. Therefore, the potential for selection bias exists regarding who completed the survey. Further, representation of racial and ethnic minorities was relatively low. A greater percentage of the survey respondents held a bachelor’s or advanced degree than in the general US population [32]. As a result, respondent demographics may not be reflective of the transplant and chronic GVHD patient population at large. These limitations may impact the findings as demographics including race, ethnicity, and level of education are known to be associated with disability [33, 34]. For example, disability rates are higher among individuals with lower levels of education and non-Hispanic Black adults than those with higher levels of education and white or Hispanic adults [33, 34]. Additionally, associations between disability and race identified in the current analysis were based on small population sizes. Chronic GVHD diagnoses and clinical characteristics were self-reported by survey respondents and were not confirmed by a physician. Finally, the survey may have been subject to recall bias, as respondents were asked about the time when symptoms were at their worst over a potentially long recall period. Additional investigations, including longitudinal studies of patients at the same stage of their clinical course, analyzing the impact of work type, sex and racial disparities, and specific chronic GVHD symptoms are needed to further understand this relationship and improve the overall HRQoL of long-term HSCT survivors.
Conclusions
In the potentially employable subset of survey respondents with chronic GVHD, nearly half met the study criteria for severe cognitive disability based on their ability to perform specific tasks, and two-thirds each met the study criteria for severe physical disability and work-related disability associated with chronic GVHD. Furthermore, our findings suggest that factors, including presence of specific symptoms and the number of transplant specialists consulted, may be associated with severe disability. These observations reveal a need for improved social support for patients with chronic GVHD, highlighting potential indicators for those most in need.
Data Availability
Access to individual patient-level data is not available for this study. Information on Incyte’s clinical trial data sharing policy and instructions for submitting clinical trial data requests are available at: https://www.incyte.com/Portals/0/Assets/Compliance%20and%20Transparency/clinical-trial-data-sharing.pdf?ver=2020-05-21-132838-960
References
Duarte RF, Labopin M, Bader P, et al. Indications for haematopoietic stem cell transplantation for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2019. Bone Marrow Transplant. 2019;54(10):1525–52.
Magenau J, Couriel DR. Hematopoietic stem cell transplantation for acute myeloid leukemia: to whom, when, and how. Curr Oncol Rep. 2013;15(5):436–44.
Passweg JR, Baldomero H, Basak GW, et al. The EBMT activity survey report 2017: a focus on allogeneic HCT for nonmalignant indications and on the use of non-HCT cell therapies. Bone Marrow Transplant. 2019;54(10):1575–85.
Sarantopoulos S, Cardones AR, Sullivan KM. How I treat refractory chronic graft-versus-host disease. Blood. 2019;133(11):1191–200.
Arai S, Arora M, Wang T, et al. Increasing incidence of chronic graft-versus-host disease in allogeneic transplantation: a report from the Center for International Blood and Marrow Transplant Research. Biol Blood Marrow Transplant. 2015;21(2):266–74.
Arora M, Cutler CS, Jagasia MH, et al. Late acute and chronic graft-versus-host disease after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2016;22(3):449–55.
Boyiadzis M, Arora M, Klein JP, et al. Impact of chronic graft-versus-host disease on late relapse and survival on 7489 patients after myeloablative allogeneic hematopoietic cell transplantation for leukemia. Clin Cancer Res. 2015;21(9):2020–8.
Sun CL, Francisco L, Kawashima T, et al. Prevalence and predictors of chronic health conditions after hematopoietic cell transplantation: a report from the Bone Marrow Transplant Survivor Study. Blood. 2010;116(17):3129–39 (quiz 3377).
Sun C-L, Kersey JH, Francisco L, et al. Burden of morbidity in 10+ year survivors of hematopoietic cell transplantation: report from the Bone Marrow Transplantation Survivor Study. Biol Blood Marrow Transplant. 2013;19(7):1073–80.
Atsuta Y, Hirakawa A, Nakasone H, et al. Late mortality and causes of death among long-term survivors after allogeneic stem cell transplantation. Biol Blood Marrow Transplant. 2016;22(9):1702–9.
Solh MM, Bashey A, Solomon SR, et al. Long term survival among patients who are disease free at 1-year post allogeneic hematopoietic cell transplantation: a single center analysis of 389 consecutive patients. Bone Marrow Transplant. 2018;53(5):576–83.
Lee SJ, Kim HT, Ho VT, et al. Quality of life associated with acute and chronic graft-versus-host disease. Bone Marrow Transplant. 2006;38(4):305–10.
Fiuza-Luces C, Simpson RJ, Ramirez M, Lucia A, Berger NA. Physical function and quality of life in patients with chronic GvHD: a summary of preclinical and clinical studies and a call for exercise intervention trials in patients. Bone Marrow Transplant. 2016;51(1):13–26.
Kurosawa S, Yamaguchi T, Oshima K, et al. Resolved versus active chronic graft-versus-host disease: impact on post-transplantation quality of life. Biol Blood Marrow Transplant. 2019;25(9):1851–8.
Lee SJ, Onstad L, Chow EJ, et al. Patient-reported outcomes and health status associated with chronic graft-versus-host disease. Haematologica. 2018;103(9):1535–41.
Fatobene G, Storer BE, Salit RB, et al. Disability related to chronic graft-versus-host disease after alternative donor hematopoietic cell transplantation. Haematologica. 2019;104(4):835–43.
Hamilton BK, Rybicki L, Arai S, et al. Association of socioeconomic status with chronic graft-versus-host disease outcomes. Biol Blood Marrow Transplant. 2018;24(2):393–9.
Hamilton BK, Storer BE, Wood WA, et al. Disability related to chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2020;26(4):772–7.
World Health Organization. International Classification of Functioning, Disability and Health (ICF). Available at: https://www.who.int/classifications/international-classification-of-functioning-disability-and-health. Accessed February 9, 2024.
Yu J, Hamilton BK, Turnbull J, et al. Patient-reported symptom burden and impact on daily activities in chronic graft-versus-host disease. Cancer Med. 2022;12:3623–33.
Yu J, Khera N, Turnbull J, et al. Impact of chronic graft-versus-host disease (GVHD) on patients’ employment, income, and informal caregiver burden: findings from the Living With Chronic GVHD Patient Survey. Transplant Cell Ther. 2023;29(7):470.e1-470.e9.
Lee S, Cook EF, Soiffer R, Antin JH. Development and validation of a scale to measure symptoms of chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2002;8(8):444–52.
Jacobs JM, Fishman S, Sommer R, et al. Coping and modifiable psychosocial factors are associated with mood and quality of life in patients with chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2019;25(11):2234–42.
El-Jawahri A, Pidala J, Khera N, et al. Impact of psychological distress on quality of life, functional status, and survival in patients with chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2018;24(11):2285–92.
Mitchell SA, Leidy NK, Mooney KH, et al. Determinants of functional performance in long-term survivors of allogeneic hematopoietic stem cell transplantation with chronic graft-versus-host disease (cGVHD). Bone Marrow Transplant. 2010;45(4):762–9.
Kurosawa S, Oshima K, Yamaguchi T, et al. Quality of life after allogeneic hematopoietic cell transplantation according to affected organ and severity of chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2017;23(10):1749–58.
Syrjala KL, Artherholt SB, Kurland BF, et al. Prospective neurocognitive function over 5 years after allogeneic hematopoietic cell transplantation for cancer survivors compared with matched controls at 5 years. J Clin Oncol. 2011;29(17):2397–404.
Syrjala KL, Dikmen S, Langer SL, Roth-Roemer S, Abrams JR. Neuropsychologic changes from before transplantation to 1 year in patients receiving myeloablative allogeneic hematopoietic cell transplant. Blood. 2004;104(10):3386–92.
Lindsay S, Varahra A, Ahmed H, et al. Exploring the relationships between race, ethnicity, and school and work outcomes among youth and young adults with disabilities: a scoping review. Disabil Rehabil. 2022;44(25):8110–29.
US Bureau of Labor Statistics. Ability to work from home: evidence from two surveys and implications for the labor market in the COVID-19 pandemic. Available at: https://www.bls.gov/opub/mlr/2020/article/ability-to-work-from-home.htm. Accessed February 9, 2024.
US Bureau of Labor Statistics. Job Flexibilities and Work Schedules—2017–2018 Data From the American Time Use Survey Available at: https://www.bls.gov/news.release/pdf/flex2.pdf. Accessed February 9, 2024.
Census Bureau Releases New Educational Attainment Data: Press Release Number CB22-TPS.02. United Stated Census Bureau. Available at: https://www.census.gov/newsroom/press-releases/2022/educational-attainment.html. Accessed May 17, 2023.
Disability Rates and Employment Status by Educational Attainment. The National Center for Education Statistics (NCES). Available. Accessed May 17, 2024.
Racial/Ethnic Disparities in Disability by Health Condition. United States Census Bureau. Available at: https://www.census.gov/library/stories/2023/07/disparities-in-disabilities.html. Accessed May 17, 2024.
Acknowledgements
The authors thank all participants involved in the Living with Chronic GVHD Patient Survey.
Authorship
All authors made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data; or the creation of new software used in the work; drafted the work or revised it critically for important intellectual content; approved the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy of integrity of any part of the work are appropriately investigated and resolved.
Medical Writing, Editorial, and Other Assistance
We thank Guilo Flore (Patient Centered Solutions, IQVIA, Amsterdam, Netherlands) for contributions to study conceptualization, analysis, and review of the manuscript. Writing assistance was provided by Nicole Farra, PhD and editorial assistance was provided by Samantha Locke, PhD, both employees of ICON (Blue Bell, PA). This was funded by Incyte.
Funding
This study was funded by Incyte Corporation (Wilmington, DE). Incyte is funding the journal’s Rapid Service Fee.
Author information
Authors and Affiliations
Contributions
Betty K. Hamilton contributed to conceptualization and methodology; writing - review and editing. Paul Williams contributed to investigation; methodology; resources; supervision; writing - review and editing. James Turnbull contributed to conceptualization; data curation; formal analysis; investigation; writing - review & editing. John Galvin contributed to conceptualization; data curation; formal analysis; investigation; writing - review & editing. Jingbo Yu contributed to conceptualization; formal analysis; investigation; methodology; writing - review & editing.
Corresponding author
Ethics declarations
Conflict of Interest
Betty K. Hamilton has served on an advisory board for Sanofi, Rigel, NKARTA, and Maat, and has received consultancy fees from the ACI Group and Incyte and webinar fees from Therakos, and served on the data safety monitoring board for Angiocrine and the adjudication committee for CSL Behring. Paul Williams and James Turnbull are employees of IQVIA, the company commissioned by Incyte Corporation to conduct this study. John Galvin and Jingbo Yu are employees and shareholders of Incyte. Incyte was involved in the design of the study and data collection. Authors employed at Incyte participated in the analysis and interpretation of data as well as writing the manuscript. Other Incyte employees reviewed the manuscript and provided comments.
Ethical Approval
The study was conducted in accordance with the ethical principles embodied by the Declaration of Helsinki and Good Clinical Practice. The survey, including revisions based on a pilot survey with three participants, was reviewed and approved by the New England Institutional Review Board before implementation. All respondents provided informed consent via an online consent form before initiation of the survey. All study participants from the initial study consented to their data being used for further research purposes.
Additional information
Prior presentation of study data: this manuscript is based on work that has been previously presented: J.Y., J.T., S.K.S., L.D.W., P.W., A.T., et al. Impact of Chronic Graft-Versus-Host Disease on Patients’ Quality of Life, Employment, Productivity, Income, and Caregivers. 2021 Tandem Meetings | Transplantation and Cellular Therapy Meetings of ASTCT and CIBMTR—The 2021 TCT Meetings Digital Experience; 8–12 February 2021; Poster number 344. J.Y., J.T., S.K.S., L.D.W., A.V., V.B., et al. Symptoms and Impact on Daily Activities and Functions in Patients With Chronic Graft-Versus-Host Disease (GVHD): Findings From the Living With Chronic GVHD Patient Survey. 2021 Tandem Meetings | Transplantation and Cellular Therapy Meetings of ASTCT and CIBMTR—The 2021 TCT Meetings Digital Experience; 8–12 February 2021; Poster number 354. B.K.H., P.W., G.F., J.G., J.T., and J.Y. Disability Associated With Chronic Graft-Versus-Host Disease After Allogeneic Hematopoietic Cell Transplantation. 63rd American Society of Hematology Annual Meeting and Exposition; 11–14 December 2021; Atlanta, GA, USA; Poster number 4060. B.K.H., P.W., G.F., J.G., J.T., and J.Y. Disability Associated With Chronic Graft-Versus-Host Disease After Allogeneic Hematopoietic Cell Transplantation. 2022 Tandem Meetings | Transplantation and Cellular Therapy Meetings of ASTCT and CIBMTR; 2–6 February 2022; Salt Lake City, UT, USA; Poster number 507.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Hamilton, B.K., Williams, P., Galvin, J. et al. Disability Associated with Chronic Graft-Versus-Host Disease After Allogeneic Hematopoietic Stem Cell Transplantation: Analysis of a Cross-Sectional US Patient Survey. Oncol Ther (2024). https://doi.org/10.1007/s40487-024-00288-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40487-024-00288-1