
Abstract
Purpose
Amyloid-β (Aβ) peptides, the main component of amyloid plaques found in the Alzheimer's disease (AD) brain, are implicated in its pathogenesis, and are considered a key target in AD therapeutics. We herein propose a reliable strategy for non-invasively delivering a specific anti-Aβ antibody in a mouse model of AD by microbubbles-enhanced Focused Ultrasound (FUS)-mediated Blood–brain barrier disruption (BBBD), using a simple single stage MR-compatible positioning device.
Methods
The initial experimental work involved wild-type mice and was devoted to selecting the sonication protocol for efficient and safe BBBD. Pulsed FUS was applied using a single-element FUS transducer of 1 MHz (80 mm radius of curvature and 50 mm diameter). The success and extent of BBBD were assessed by Evans Blue extravasation and brain damage by hematoxylin and eosin staining. 5XFAD mice were divided into different subgroups; control (n = 1), FUS + MBs alone (n = 5), antibody alone (n = 5), and FUS + antibody combined (n = 10). The changes in antibody deposition among groups were determined by immunohistochemistry.
Results
It was confirmed that the antibody could not normally enter the brain parenchyma. A single treatment with MBs-enhanced pulsed FUS using the optimized protocol (1 MHz, 0.5 MPa in-situ pressure, 10 ms bursts, 1% duty factor, 100 s duration) transiently disrupted the BBB allowing for non-invasive antibody delivery to amyloid plaques within the sonicated brain regions. This was consistently reproduced in ten mice.
Conclusion
These preliminary findings should be confirmed by longer-term studies examining the antibody effects on plaque clearance and cognitive benefit to hold promise for developing disease-modifying anti-Aβ therapeutics for clinical use.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Blood–Brain-Barrier (BBB) protects the central nervous system (CNS) from drugs and toxins. It is composed of microvascular endothelial cells. Tight junctions (TJs) are formed between these cells, with several transporters regulating the influx and efflux of compounds, such as nutrients and small peptides [1]. Generally, paracellular permeability is limited to substances with a molecular weight up to 400–500 Da, thus prohibiting the delivery of most therapeutic agents into the brain [2]. The highly selective nature of BBB is the main obstacle against the application of potential disease-modifying therapies for diseases of the CNS, including neurodegenerative diseases such as the Alzheimer's disease (AD) [3, 4]. Accordingly, drug delivery into the brain tissue has been a major challenge for researchers over a long period.
It is by now generally accepted that pulsed FUS in synergy with microbubbles (MBs) can cause temporal BBBD by causing alterations in the cell-to-cell interactions and endothelial cell cytoskeleton. In fact, MBs-enhanced FUS was shown to loosen the endothelial cell tight junctions (TJs) through a mechanism known as cavitation [5, 6]. The junctions’ disruption is mainly attributed to changes in the level of related trans- and peripheral membrane proteins [7]. In addition, FUS treatment was found to cause stimulation of transcytosis, sonoporation of the vascular endothelium, and increase in the paracellular diffusion due to the TJs disruption [7]. FUS can further cause disruption of drug efflux by temporally suppressing the expression of the permeability-glycoprotein (Pgp) [8].
BBBD by pulsed FUS in the presence of gaseous MBs has emerged as a feasible method of delivering large molecules normally hampered by the BBB to the brain. This strategy has been confirmed by numerous preclinical studies to enhance the penetration of therapeutic agents, such as therapeutic peptides, genes, and antibodies into the CNS of non-transgenic and transgenic mouse models of neurological diseases, with an increasing number of clinical trials exploring clinical utility [9,10,11,12,13]. Typically, initial evidence of the success and extend of BBBD is obtained by contrast-enhanced MRI and the well-known Evans Blue (EB) dye method [10, 11, 13].
AD is the prevalent neurodegenerative disorder and cause of dementia and is characterized by the presence of intracellular neurofibrillary tangles and extracellular amyloid plaques owing to Amyloid β peptides (Aβ) aggregation [14, 15]. Available treatments are not curative but may slow disease progression and alleviate symptoms. Given the urgent demand for disease-modifying therapies, the development of FUS therapeutics for AD receives remarkable research interest.
The ability of MBs-enhanced FUS without exogenous agents to reduce the Aβ pathology has been well demonstrated [16,17,18]. A single trans-skull MRgFUS treatment was shown to increase the levels of endogenous immunoglobulins (IgM and IgG) in the cortex of the TgCRND8 mouse model [16]. FUS-mediated endogenous antibody delivery and glia cells activation were considered as the mechanisms responsible for the observed plaque burden reduction [16]. Later, Shen et al. [17] reported that FUS in synergy with MBs applied twice a week for 6 weeks triggered behavioral changes and improved the spatial memory of triple transgenic AD mice. These changes were associated with reduced Aβ pathology and tau phosphorylation, as well as improved neuronal health of the sonicated hippocampus compared to the sham group.
The positive effects of FUS in the mitigation of AD pathological features can be enhanced by administrating exogenous therapeutic agents. According to a study by Hsu et al. [19], the effects of FUS on plaque reduction were enhanced using a specific inhibitor of the glycogen synthase kinase-3 (GSK-3); a key molecule in the onset of AD. Administration of this inhibitor in APPswe/PSEN1-dE9 transgenic mice prior to MBs-enhanced FUS reduced the Aβ plaque synthesis by suppressing the GSK-3 protein activity [19]. Another study targeted an Aβ peptide species deposited in AD brain termed Pyroglutamate-3 Aβ (pGlu-3 Aβ) [20]. The FUS-mediated administration of an anti-pGlu-3 Aβ vaccine was found to promote plaque clearance and partial protection from cognitive decline in APPswe/PS1ΔE9 mice [20]. Others attempted to support neuronal health as a measure for disease mitigation [21]. The repeated MRgFUS-mediated delivery of a pharmacological agent termed D3 (TrkA agonist) that promotes neuronal function was found to impart numerous therapeutic effects, including enhanced hippocampal neurogenesis and positive cognitive effects in TgCRND8 AD mice [21].
Several studies aimed to investigate the efficiency of FUS-mediated BBBD to facilitate the supply of large disease-specific antibodies in the brain and the resultant therapeutic effects. The feasibility of delivering an anti-Ab antibody called BAM-10 into the brain of the TgCRND8 mouse model using transcranial MRgFUS and reducing the plaque pathology has been demonstrated by Jordao et al. [22]. FUS-induced BBBD was also shown to facilitate the supply of an anti-pyroglutamate-3 Aβ monoclonal antibody (mAb) called 07/2a in the brain of aged APP/PS1dE9 transgenic mice [23]. Sun et al. [24] further demonstrated that three successive weekly treatments with the 07/2a mAb combined with FUS resulted in a faster improvement of spatial learning and memory of a higher percentage of aged APP/PS1dE9 mice compared to the mice group receiving only antibody.
Another anti-Αβ antibody tested for its efficacy to improve cognition in AD mice is the Aducanumab. Leinenga et al. [25] compared the effects of this antibody when administered alone or in synergy with MBs-enhanced scanning ultrasound in APP23 AD mice. The combined approach resulted in a five-fold increase in the antibody amount compared to the non-sonicated mice a few days post-treatment and significant improvement in spatial memory. Notably, Aducanumab is the first therapeutic agent to be tested in combination with FUS in AD patients in a phase I ongoing clinical trial [26].
The Aβ (1–40) antibody targets the amyloid peptides Aβ (1–40) that represent the most abundant Aβ isoform in the AD brain [27]. The FUS-mediated delivery of the specific antibody was previously tested in a very small mice population (n = 3) [28]. A three-fold increase in fluorescence intensity of the antibody staining was observed in the brain regions treated with MBs-enhanced MRgFUS in comparison with the non-sonicated regions, with hematoxylin and eosin (H&E) staining providing evidence of hemorrhages in the sonicated brain tissue [28]. While this study provides promising results on FUS-mediated enhanced Aβ (1–40) antibody delivery, further experiments in a larger mouse population are needed to confirm these early findings and optimize the therapeutic protocol for safe and efficient Aβ (1–40) antibody delivery.
In this study, we aimed to evaluate whether the application of FUS in synergy with MBs using an in-house manufactured manual positioning device comprising a single element FUS transducer of 1 MHz can facilitate the penetration of the Aβ (1–40) antibody into the brain of 5XFAD transgenic mice. We initially attempted to define the sonication protocol for safe and efficient BBBD. The success and extent of BBBD was assessed by EB extravasation while brain damage was assessed by H&E staining. We then examined the capability of the Aβ (1–40) antibody to consistently enter the brain parenchyma when administered alone and prior to MBs-enhanced FUS using the optimized protocol in a large 5XFAD mice group.
Materials and methods
All mice experiments were carried out at the premises of the Cyprus Institute of Neurology and Genetics under national guidelines and protocols authorized by the Veterinary Services of Cyprus under the study license CY/EXP/PR.L05/2021.
FUS system
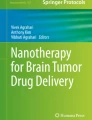
FUS was delivered using a manual positioning system [29] comprising a single element, spherically focused, ultrasound transducer (Piezo Hannas, Wuhan, Hubei, China, 1 MHz central frequency, 80 mm radius of curvature, 50 mm diameter, and 32.5% acoustic efficiency) tuned to an RF amplifier (AG 1016, AG series, T&G Power conversion Inc., Rochester, NY). This system was specially designed to facilitate transcranial FUS studies in rodents. The transducer is hosted in a conical water tank whose bottom opening is sealed with a silicone membrane. The tank can be moved vertically via a manual positioning mechanism coupled to the mouse platform to attach to the mouse head via a top to bottom approach. A laser pointer accessory was implemented into the system to facilitate consistent targeting among experiments. The positioning device and animal placement on the dedicated platform can be seen in Fig. 1.

a CAD drawing of the 1-DOF manual positoning device comprising a FUS transducer of 1 MHz with a mouse positioned on the dedicated platform, b Indicative photo from experiment
Protocol optimization for efficient and safe Blood–brain barrier disruption
Thirty-two (32) WT B6/SJL mice were used for protocol calibration/optimization. Intraperitoneal injection of Avertin (Sigma Aldrich, St. Louis, Missouri, United States) was used to cause rapid and deep anesthesia in mice and ensure no suffering. The dose of Avertin was weight-dependent for each animal (20 μL/g). The hair was removed from the mouse head using a commercial hair removal cream (Veet Hair Removal cream). Retro-orbital injection was then used to deliver a mixture of 5 μL of SonoVue® MBs (Bracco Imaging, Turin, Italy, 2 × 108 microbubbles/ mL suspension) along with 5 mL/kg of 3% w/v EB solution (Sigma, St. Louis, MO, USA). Anesthetized animals were positioned in prone position on the platform as shown in Fig. 1. The tank was filled with degassed, deionized water and US coupling gel (Quick-Eco Gel, AB Medica group S.A., Barcelona, Spain) was applied on the mouse head to achieve efficient acoustic coupling. The position of the mouse was adjusted so that the FUS beam was targeted on the left hemisphere centrally with the assistance of the laser system. All mice received a single sonication within 3–4 min following the injection of MBs and EB using 1 MHz pulsed FUS of 10 ms bursts at a duty factor (DF) of 1% for a total duration of 100 s.
For protocol calibration purposes, electric power values of 20 to 70 W were tested (10 W step; 6 groups of 5 mice each). The relevant acoustic power ranged from 6.5 to 22.8 W, corresponding to in situ focal acoustic pressure in the range of 0.3–0.6 MPa. The output acoustic power was estimated based on the acoustic efficiency of the transducer of 32.5%. The respective focal pressures were initially determined in water using a needle hydrophone (HNC, ONDA, Sunnyvale, CA, USA) placed at the focal distance of the transducer. In-situ pressures were then calculated accounting for the transmission loss through the mouse skull. The transmission coefficient of a skull sample was measured according to the well-established through-transmission immersion technique [30] at the operating frequency of the transducer of 1 MHz. One mouse received only EB and one neither EB nor FUS, thus serving as the control mice.
Mice were sacrificed by transcardial perfusion with saline followed by 4% paraformaldehyde (PFA) 40 min post-treatment. This time period is well within the 4-h window that the BBB was found to maintain open after FUS. Therefore it was considered sufficient for successful entry of EB into the brain, but also to allow for acute FUS-induced physiological responses to be resolved [31]. The brain tissue was then collected and preserved in paraformaldehyde (4%) and then sucrose (20%) diluted in Phosphate Buffer (0.1%) according to our protocol. Brain sections were prepared for fluorescence imaging. Slides containing brain sections were visualized using a Nikon eclipse-Nἱ (Tokyo, Japan) fluorescence microscope to visualize EB extravasation and determine the BBB-opened region.
Trans-BBB Aβ (1–40) antibody delivery in a mouse model of AD
Animals
5XFAD transgenic mice recapitulating major pathological features of AD were utilized. 5XFAD mice were bred as single transgenics. Male 5XFAD mice were crossed with female SJL/B6 F1 mice to give hemizygous or wild-type offspring's, which were used for the purpose of the study. The pathologic phenotype of this mouse model consists of gliosis, amyloid plaques, neurodegeneration, memory deficits (at 4–5 months), as well as intraneuronal Aβ and neuron loss. Beginning at 8 weeks of age, amyloid deposition and gliosis become increasingly widespread, especially in the deep cortical layers and subiculum.
Experimental design
5XFAD transgenic mice of 5-months of age (n = 21) were used to test the feasibility and efficacy of FUS-mediated delivery of the Aβ (1–40) antibody (150 kDa, Anti-β-Amyloid Protein (1–40) antibody produced in rabbit whole antiserum, A8326, Sigma Aldrich, 3050 Spruce Street, Saint Louis, MO 63103, USA) into the brain. The ability of the antibody to pass through the BBB and bind to the Aβ plaques when administered alone and in combination with FUS was investigated using a constant antibody amount of 50 μL (2.85 mg), which is the half quantity of the previously tested antibody dose [28].
Twenty one (21) mice were divided into 4 sub-groups: A. Staining with the Aβ (1–16) and Aβ (1–40) antibodies without injected antibody or FUS + MBs to confirm the presence of amyloid plaques in the cortex (referred to as control, n = 1), B. Saline (50 μL) administration followed by FUS + MB-induced BBB opening (referred to as saline; n = 5), C. Aβ (1–40) antibody (50 μL) administration alone (referred to as antibody, n = 5), and D. Aβ (1–40) antibody (50 μL) administration followed by FUS + MB-induced BBB opening (referred to as FUS + MBs plus Ab; n = 10).
The anesthesia protocol and treatment timeline were similar to that used for the calibration study. The Aβ (1–40) antibody was delivered instead of the EB dye via retro-orbital injection along with the MBs. Based on the data gathered from the protocol optimization study, an acoustic power of 16 W (in situ focal acoustic pressure of 0.5 MPa) was considered optimum and used in this experimental part while the rest sonication parameters remained the same. The treatment protocol is summarized in the diagram of Fig. 2. Note that following FUS, a time window of 4 h was left before mice sacrifice.

Protocol timeline for FUS-mediated Aβ (1–40) antibody delivery in 5XFAD mice
Mouse sacrifice and tissue preparation
Transcardial perfusion was used to clear blood and preserve the brain for immunostaining analysis. Following perfusion, the mouse head was dissected, and the skull was carefully removed using scissors and forceps, exposing the brain. The brain was washed in Phosphate Buffer Saline (PBS) and then placed for 2 h in 4% Paraformaldehyde (PFA) solution. Subsequently, it was again washed with PBS and placed into 20% sucrose solution (diluted in Phosphate Buffer 0.1 M) overnight at 4 °C for cryoprotection prior to embedding and freezing. For tissue embedding, the cryomould containing the brain tissues, was filled with OCT, and placed into acetone-dry ice bath. Finally, the frozen OCT containing the brain tissue was removed from the cryomould and stored in a − 80 °C freezer.
Immunohistochemistry
Double immunostaining of coronal brain Sects. (16 brain sections / mouse) was performed to determine whether the injected Aβ (1–40) antibody passed the BBB and bound to Aβ plaques. Staining with the Aβ (1–16) antibody (6E10, green colour) was used to identify the amyloid plaques. The tissue was permeabilized by immersing the frozen sections in acetone for 10 min at − 20 °C. It was then washed three times with 1X PBS and blocking solution (5% Bovine Serum Albumin + 0.5% Triton X-100) was applied for 1 h on the sections at room temperature in a humidified chamber. The blocking solution was then removed and the primary antibody; anti-β-amyloid primary monoclonal 6E10 (1 mg/mL) (diluted in blocking solution, 1:400) was applied to the tissue sections and incubated overnight at 4 °C. The following day, the primary antibody was removed, and the tissue sections were washed three times with 1X PBS. The secondary antibodies; Fluorescein (FITC) goat anti-mouse (1.5 mg/mL), 1:100 and Alexa Fluor® 594 goat anti-rabbit (2 mg/mL), 1:500 (diluted in blocking solution) were next applied for 1 h at room temperature for the detection of the injected antibody in the examined brain tissue, followed by three washes with 1X PBS and incubation for 30 s with 4ʹ,6-diamidino-2-phenylindole (DAPI, Sigma-Aldrich) for nuclear staining. The tissues were washed two times for 5 min with 1X PBS, dried and mounted with mounting media in order to prepare them for microscopy.
H&E staining
We also checked the tissue integrity and the lack of hemorrhage with H&E staining for the tested acoustic pressures ranging from 0.3 to 0.6 MPa. Tissue sections in OCT were stained with Harris's haematoxylin (freshly filtered) for 3 min, and then washed with distilled water and stained with aqueous eosin for 6 min. Next, they were dehydrated in ascending concentrations of alcohol and cleared in xylene (70%, 95%, 100% × 2 and xylene × 3). Finally, the tissue slides were mounted with Dibutylphthalate Polystyrene Xylene (DPX).
Results
Protocol optimization for efficient and safe Blood–brain barrier disruption
According to fluorescence microscopy all tested power levels in the range of 6.5–22.8 W (0.3−0.6 MPa in situ pressure) combined with 5 μL of MBs (for the specific sonication parameters employed) caused BBBD since increased fluorescence intensity of EB was observed compared to the control mouse (receiving only EB). Indicative fluorescence images for the various acoustic powers tested are presented in Fig. 3, revealing the power effect on the extent of EB extravasation. Note that a gradual increase of fluorescence intensity (indicating increase in the extent of BBBD) occurred as the power in the tested range was increased.

Fluorescence images (10 × magnification) of unstained brain sections at the level of the lateral ventricles of mice injected with EB: a No FUS, b FUS at 6.5 W, c FUS at 9.7 W, d FUS at 13 W, e FUS at 16 W, and f FUS at 19.5 W (acoustic power)
The optimal power was selected as the one resulting in the highest EB leakage (ideally spread throughout the sonicated region) without causing any adverse effects on tissue and having consistent behavior among subjects. The power value of 16 W (0.5 MPa in situ pressure) showed consistent EB leakage in all examined brain regions and no evidence of damage and was thus selected for follow-up experiments in the AD mouse model. Figure 4 shows representative fluorescence microscopy images for the selected power taken from to cortex region. Photos of the freshly perfused excised brain of a mouse treated with the selected protocol and a brain section after fixation in OCT can be seen in Fig. 4b and c, respectively. Note that the EB dye was diffused throughout the entire left hemisphere that was sonicated. Figure 4d and e compare magnified fluorescence images of unstained brain sections at the level of the cortex between a non-sonicated mouse and a sonicated mouse (pulsed FUS with 10 ms burst length and 1% DF at 16 W for 100 s duration and 5 μL MBs) both injected with equal amount of EB solution (5 mL/kg of 3% w/v). Note that no leakage was observed in the brain of the control mouse (EB only), whereas FUS-induced BBBD resulted in high levels of EB dye covering the examined cortex area. Indicative histological slides from H&E examination for the selected acoustic power (16 W) from two different brain areas can be seen in Fig. 5. No difference between the FUS treated and control cases in terms of tissue integrity was observed and there was no evidence of hemorrhage in none of the tested brain regions.

a FUS beam targeting centrally at the left hemisphere, b Freshly perfused excised mouse brain treated with the selected protocol (5 μL MBs and 16 W acoustic power), c brain section after fixation in OCT revealing the distribution pattern of EB extravasation, d–e Fluorescence images (5 × magnification) of unstained brain sections at the level of the cortex taken from perfused mice injected with EB and 5 μL MBs followed by sonication at 16 W (EB + FUS+MB) and injected with EB only (control)

Representative photos (10 × and 40 × magnification) of H&E staining from mice treated with MBs-enhanced pulsed FUS at 16 W for two different brain areas; corpus callosum (CC) and inferior colliculus (IC)
Trans-BBB Aβ (1–40) antibody delivery in a mouse model of AD
Indicative results of immunohistochemistry analysis of brain tissue sections from 5XFAD mice are presented in Figs. 6 and 7. Co-localization of red (injected Aβ (1–40) antibody) and green (Αβ (1–16) antibody) fluorescence in multiple brain regions of the sonicated hemisphere confirmed successful BBBD, as well as entry and binding of the injected Αβ (1–40) antibody to Αβ plaques. Indicative fluorescence images of brain sections at the level of the cortex for the various mice groups are shown in Fig. 6. As expected, the 5XFAD mice that were injected with saline following FUS + MBs (saline group) did not have any signs of the Aβ (1–40) antibody in their brain. Similarly, the antibody was not present in any of the brain sections of the mice injected only with the Aβ (1–40) antibody (antibody group), confirming the inability of the specific therapeutic agent to normally pass through the BBB. On the contrary, immunohistochemistry analysis of brain sections from the FUS + MBs plus Ab group showed entry of the Aβ (1–40) antibody in the brain parenchyma. Note that the control mouse was not injected with the antibody neither received FUS + MBs; it was just stained with the Aβ (1–16) and Aβ (1–40) antibodies to confirm the presence of amyloid plaques (green & red) in the cortex. These findings qualify the selected treatment protocol (50 μL antibody & 1 MHz pulsed FUS with 10 ms burst length and 1% DF at 16 W for 100 s) as an efficient BBBD method for the delivery of the specific anti-Aβ antibody into the mouse brain. The repeatability of obtained results was investigated in ten mice, which all showed successful antibody entry and specific binding to plaques. Indicative brain sections from six mice are shown in Fig. 7 revealing co-localization of antibodies (white circles) in the cortex.

Immunohistochemistry analysis of brain tissue sections of 5xFAD mice. a Control staining; brain tissue without any injected antibody or FUS + MBs stained with Aβ (1–16) and Aβ (1–40) antibodies to confirm the presence of amyloid plaques (green & red) in the cortex. b Mouse injected with saline followed by FUS + MBs. c Mouse injected with the Aβ (1–40) antibody alone. d Mouse injected with 50 μL of Aβ (1–40) antibody followed by FUS + MBs. Amyloid plaques (green) were stained with Aβ (1–16). The Aβ (1–40) antibody was stained red. Co-localization of antibodies (white circles) in the cortex of the FUS + MBs plus Ab group (MERGE) confirmed successful entry and binding of the Aβ (1–40) with amyloid plaques (Sonication parameters: f = 1 MHz, burst length = 10 ms, DF = 1%, acoustic power = 16 W, and sonication duration = 100 s)

Immunohistochemistry analysis of brain tissue sections of 5XFAD mice injected with 50 μL of Aβ (1–40) and 5 μL MBs followed by pulsed FUS (f = 1 MHz, burst length = 10 ms, DF = 1%, acoustic power = 16 W, and sonication duration = 100 s). Fluorescence images (20 × magnification) from (6) different mice at the cortex level where plaques are stained green; Αβ (1–16) and the antibody red; Αβ (1–40). Co-localization of antibodies (white circles) in the cortex confirmed the successful entry and specific binding of the Aβ (1–40) antibody
Discussion
FUS in combination with MBs has been confirmed by numerous studies [10, 32, 33] as an effective method for overcoming the BBB to deliver exogenous therapeutic agents to the brain at present. AD is the most common cause of dementia [14] with Aβ immunotherapy belonging to the most promising therapeutics to alter its course [27]. Several antibodies such as Aducanumab and Lecanemab/BAN2401 were used for targeting Aβ at different epitopes (3–7 and 1–16, respectively) in order to promote amyloid plaque clearance [34]. However, drug efficacy is low as only 0.1% of antibodies can pass the BBB [35]. This study aimed to investigate whether FUS-mediated BBB opening with an optimized protocol can be used to safely and efficiently deliver a specific anti-Aβ antibody; Aβ (1–40) into the brain of 5XFAD AD mice using a custom-made FUS positioning device. The specific antibody is directed against the amyloid peptides Aβ (1–40) that represent the most abundant Aβ isoform in the AD brain [27], thus promoting plaque clearance. Unfortunately, its entrance in the brain is prohibited by the BBB due to its large molecular weight (150 KDa).
To our knowledge, this is the second study to report the use of the anti-Aβ antibody Aβ (1–40). In fact, there is a previous study that examined the feasibility of delivering this antibody into 3 mice by FUS-mediated BBBD. Authors report a three-fold increase in fluorescence intensity of the antibody staining in brain regions treated with MRgFUS (in comparison to non-sonicated regions), with the H&E staining revealing hemorrhage in the sonicated brain tissue [28]. We have verified these preliminary findings in a larger mice population (n = 10) showing that FUS-mediated BBBD facilitates antibody penetration into the brain. In this study, non-sonicated mice showed zero fluorescence intensity indicating complete absence of the exogenous antibody in the examined brain tissue. It is worth mentioning that the absence of fluorescence intensity in the non-sonicated mice confirms that the anaesthetic (Avertin) used during the experimental procedure did not affect the BBB permeability, whereas other anaesthetics such as propofol affect BBB permeability [36]. Additionally, our current results go beyond previous findings further demonstrating that the use of an optimized protocol allows for efficient BBBD and delivery of the specific antibody without any tissue damage and probably the use of a smaller antibody dose (half compared to the dose used previously [28]). However, this requires further investigation.
The first experimental part was carried out in WT mice (n = 32) and was devoted to selecting the acoustic power/pressure for optimized BBBD. Notably, at sufficiently high acoustic pressure, the administered MBs begin to oscillate stably causing transient increase of permeability in the targeted area while above a threshold of pressure inertial cavitation occurs where MBs collapse violently [37, 38]. In the former case, the endothelial ligaments recover completely within a few hours post-sonication [39]. Inertial cavitation is responsible for the majority of adverse effects observed with this strategy, such as micro-hemorrhages [38]. Therefore, the various acoustic pressure levels were tested both in terms of BBBD extent using the EB dye method and sonication-related tissue effects using H&E staining.
The EB dye technique allowed visual confirmation of BBBD with the naked eye directly after brain exposure and ease assessment of BBBD using a fluorescence microscope. A potential limitation of this methodology is that it does not provide any quantitative information on the magnitude of BBBD [40]. The FUS + MBs treated mice showed higher levels of EB dye in all examined brain areas, whereas for the control mouse (EB only) the dye remained in the extracellular matrix. The in situ peak pressure amplitude of 0.5 MPa (16 W acoustic power) applied at a frequency of 1 MHz in the presence of MBs (5 μL) was selected as offering safe and efficient BBBD and employed in follow-up studies involving the antibody. The results of H&E histology revealed no structural damage and no signs of hemorrhage in none of the sonicated hemispheres.
These results are consistent with what has been found in previous state-of-the-art studies. In fact, pressure levels of up to 0.5 MPa have been previously proposed by Hynynen et al. [39] as suitable for consistent and safe BBBD in rabbits, where the observed side effects were mostly limited to few tiny extravasations of red blood cells. Above that value and up to 1.4 MPa more severe effects such as hemorrhages and mild damage to the brain parenchyma were observed. Herein, none of the tested focal pressures ranging from 0.3 to 0.6 MPa (in situ) showed evidence of FUS-related effects on tissue integrity. The efficiency of the selected pressure level (0.5 MPa) to disrupt the BBB with negligible effects on brain tissue has been confirmed by other studies as well, with McDannold et al. [41, 42] reporting an estimated minimum threshold of 0.36 MPa for BBB opening. When comparing results, it must be pointed out that similar pulsed FUS parameters (10 ms burst length at 1 Hz repetition frequency) were employed in these studies, but a quite smaller frequency of 0.7 MHz.
Transgenic mouse models of AD constitute the main research tool in such studies since they are inexpensive, reproducible, and exhibit abundant plaque load. Herein, 5XFAD mice were bred for the antibody study (n = 21). This is an excellent model since it recapitulates major features of the AD amyloid pathology at a very early age with a rapid amyloid beta plaque formation and severe gliosis [43, 44]. This is advantageous compared to other mouse models of AD that develop the pathology at a slower rate [45, 46]. It should be though noted that the absence of tau pathology that is a hallmark of AD can be a limitation of this model. Given that the interplay of Aβ and tau plays a major role in the development and acceleration of the disease, the disease mechanisms are not fully demonstrated [47].
The combined treatment involved retro-orbital injection of 50 μL of Aβ (1–40) antibody (2.85 mg), which is half the amount used in a previous study [28], and 5 μL of MBs (1 × 106 MBs) followed by pulsed FUS (16 W) at 1 MHz. Retro-orbital injection was used as an alternative to tail vein intravenous administration. Based on the literature, there is no difference in the drug delivery, absorption or pharmacokinetic activity of therapeutic agents such as drugs or antibodies [48, 49]. Following FUS treatment, the mouse was left 4 h before it was sacrificed, which is considered the reliable post-treatment time window during which the BBB remains open [50, 51], to allow the maximum amount of antibody to enter and distributed in the brain. Immunohistochemistry analysis of brain tissue sections confirmed that the antibody cannot normally enter the brain parenchyma. Specifically, no fluorescent was observed in the microscope indicating absence of the antibody when administered alone owing to its prohibitively large molecular weight of 150 kDa. A single treatment with the selected sonication protocol (1 MHz pulsed FUS with 10 ms burst length, 1% DF, 16 W power, and 100 s duration) allowed the injected Aβ (1–40) antibody to enter the brain. In merged images, co-localization the Aβ (1–40) and Aβ (1–16) antibodies confirmed the presence of cortical plaques, successful trans-BBB entry of the injected anti-Aβ antibody in the sonicated brain, as well as the specificity of the Aβ (1–40) antibodies to bind to the amyloid plaques. The results showed excellent consistency and reproducibility of BBBD and FUS-mediated antibody delivery by single sonication in the treated hemispheres of all mice (n = 10, FUS + MBs plus Ab group). It is expected that antibody binding to amyloid plaques will enhance their clearance from the brain by facilitating recognition and uptake by glial and peripheral immune cells, thus leading to reduction of amyloid (1–40) loading and subsequently inhibiting toxic oligomerization of Aβ [52].
This is a preliminary study that was focused on the feasibility of safely and efficiently delivering the Αβ (1–40) antibody into the mouse brain following BBB opening by FUS. Although the antibody was widely distributed through the sonicated brain and bound to Aβ plaques, it remains unclear to which degree the selected antibody amount promotes plaque clearance and positive cognitive effects nor whether the antibody amount can be further decreased. Accordingly, longer-term studies are required to assess the effects of the antibody and dose on suppressing AD pathology, which may require repeated treatments.
The positioning device employed in the study was proven an ergonomic tool for trans-cranial FUS applications in mice. The special design of the system allowed attaching the water-filled cone to the mouse head with visual confirmation of proper coupling following easy targeting with the assistance of the laser system. The suitability of the single element FUS transducer of 1 MHz for the particular application of transcranial BBBD in rodents was demonstrated, being in agreement with other field studies where 1 MHz burst FUS was predominantly selected for similar applications [9, 53,54,55]. Since this was a feasibility study, we did not attempt targeting a specific brain region. A global targeting approach was instead used where the beam was focused in the center of the left hemisphere. The blue dyed area in the perfused brain slice of Fig. 4 covers almost the entire targeted hemisphere. This is reasonable since the beam of the selected transducer is wide with focal point dimensions (≈ 2.5 mm lateral diameter) comparable with the hemisphere dimensions. Of course, the extend of BBBD and EB extravasation depend on multiple other factors, such as the applied pressure and burst duration [56], as well as the type and dose of MBs [57]. Notably, the connectivity of the brain and the changes in the local environment (e.g., blood flow) after the FUS treatment might also contribute to this phenomenon. Generally, as evidenced by the extend of EB dye extravasation, FUS of 1 MHz applied with the specific transducer and proposed sonication parameters affected almost the entire targeted hemisphere, also provided the small size of the mouse brain. Follow up studies may use ultrasonic sources with stronger focusing and account for such parameters to enable a more specific delivery of the antibody in brain regions of interest.
Conclusions
Overall, the study findings demonstrated that the Αβ (1–40) antibody that is normally hampered by the BBB can efficiently and safely enter the brain parenchyma and bind to Aβ plaques of the 5XFAD mouse model of AD by FUS + MBs-mediated BBB opening with the proposed optimized protocol. Follow-up studies will examine the effects of this antibody on Aβ clearance and plaque load reduction, as well as whether repeated treatments can impart significant positive effects on cognition. These results hold promise for the development of disease modifying therapies for AD patients via the non-invasive anti-Aβ antibody delivery in future clinical applications.
Data availability
All data generated or analysed in the present study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
References
Kadry H, Noorani B, Cucullo L (2020) A blood–brain barrier overview on structure, function, impairment, and biomarkers of integrity. Fluids Barriers CNS 17:1–24. https://doi.org/10.1186/s12987-020-00230-3
Pandit R, Chen L, Götz J (2020) The blood-brain barrier: physiology and strategies for drug delivery. Adv Drug Deliv Rev 165–166:1–14. https://doi.org/10.1016/j.addr.2019.11.009
Ebrahimi Z, Talaei S, Aghamiri S, Goradel NH, Jafarpour A, Negahdari B (2020) Overcoming the blood–brain barrier in neurodegenerative disorders and brain tumours. IET Nanobiotechnol 14:441–448. https://doi.org/10.1049/iet-nbt.2019.0351
Harilal S, Jose J, Parambi DGT, Kumar R, Unnikrishnan MK, Uddin MS et al (2020) Revisiting the blood-brain barrier: a hard nut to crack in the transportation of drug molecules. Brain Res Bull 160:121–140. https://doi.org/10.1016/j.brainresbull.2020.03.018
Mesiwala AH, Farrell L, Wenzel HJ, Silbergeld DL, Crum LA, Winn HR et al (2002) High-intensity focused ultrasound selectively disrupts the blood-brain barrier in vivo. Ultrasound Med Biol 28:389–400. https://doi.org/10.1016/S0301-5629(01)00521-X
Yang Y, Zhang X, Ye D, Laforest R, Williamson J, Liu Y et al (2019) Cavitation dose painting for focused ultrasound-induced blood-brain barrier disruption. Sci Rep 9:1–10. https://doi.org/10.1038/s41598-019-39090-9
Gosselet F, Loiola RA, Roig A, Rosell A, Culot M (2021) Central nervous system delivery of molecules across the blood-brain barrier. Neurochem Int 144:104952. https://doi.org/10.1016/j.neuint.2020.104952
Aryal M, Fischer K, Gentile C, Gitto S, Zhang YZ, McDannold N (2017) Effects on P-glycoprotein expression after blood-brain barrier disruption using focused ultrasound and microbubbles. PLoS ONE 12:1–15. https://doi.org/10.1371/journal.pone.0166061
Choi JJ, Wang S, Tung Y-S, Morrison B, Konofagou EE (2010) Molecules of various pharmacologically-relevant sizes can cross the ultrasound-induced blood-brain barrier opening in vivo. Ultrasound Med Biol 36:58–67. https://doi.org/10.1016/j.ultrasmedbio.2009.08.006
Chen K, Wei K, Liu H (2019) Theranostic strategy of focused ultrasound induced blood-brain barrier opening for CNS disease treatment. Front Pharmacol. https://doi.org/10.3389/fphar.2019.00086
Ghali MGZ, Srinivasan VM, Kan P (2019) Focused ultrasonography-mediated blood-brain barrier disruption in the enhancement of delivery of brain tumor therapies. World Neurosurg 131:65–75. https://doi.org/10.1016/j.wneu.2019.07.096
Fishman PS, Fischell JM (2021) Focused ultrasound mediated opening of the blood-brain barrier for neurodegenerative diseases. Front Neurol 12:1–5. https://doi.org/10.3389/fneur.2021.749047
Lin CY, Hsieh HY, Pitt WG, Huang CY, Tseng IC, Yeh CK et al (2015) Focused ultrasound-induced blood-brain barrier opening for non-viral, non-invasive, and targeted gene delivery. J Control Release 212:1–9. https://doi.org/10.1016/j.jconrel.2015.06.010
Alzheimer’s disease. Alzheimer’s Dis Int (2023). https://www.alzint.org/about/dementia-facts-figures/types-of-dementia/alzheimers-disease/ Accessed 16 Jan 2023
Choi JJ, Wang S, Brown TR, Small SA, Duff KEK, Konofagou EE (2008) Noninvasive and transient blood-brain barrier opening in the Hippocampus of Alzheimer ’ s double transgenic mice using focused ultrasound. Ultrason Imaging 30:189–200
Jordão JF, Thévenot E, Markham-Coultes K, Scarcelli T, Weng Y-Q, Xhima K et al (2013) Amyloid-β plaque reduction, endogenous antibody delivery and glial activation by brain-targeted, transcranial focused ultrasound. Exp Neurol 248:16–29. https://doi.org/10.1016/j.expneurol.2013.05.008
Shen Y, Hua L, Yeh C, Shen L, Ying M, Zhang Z (2020) Ultrasound with microbubbles improves memory, ameliorates pathology and modulates hippocampal proteomic changes in a triple transgenic mouse model of Alzheimer’ s disease. Theranostics 10:11794–11819. https://doi.org/10.7150/thno.44152
Poon CT, Shah K, Lin C, Tse R, Kim KK, Mooney S et al (2018) Time course of focused ultrasound effects on β-amyloid plaque pathology in the TgCRND8 mouse model of Alzheimer’s disease. Sci Rep 8:1–11. https://doi.org/10.1038/s41598-018-32250-3
Hsu PH, Lin YT, Chung YH, Lin KJ, Yang LY, Yen TC et al (2018) Focused ultrasound-induced blood-brain barrier opening enhances GSK-3 inhibitor delivery for amyloid-beta plaque reduction. Sci Rep 8:1–9. https://doi.org/10.1038/s41598-018-31071-8
Frost JL, Liu B, Rahfeld J-U, Kleinschmidt M, O’Nuallaina B, Le KX et al (2015) An anti-pyroglutamate-3 Aβ vaccine reduces plaques and improves cognition in APPswe/PS1ΔE9 mice. Neurobiol Aging 36:3187–3199. https://doi.org/10.1016/j.neurobiolaging.2015.08.021
Xhima K, Markham-Coultes K, Hahn Kofoed R, Saragovi HU, Hynynen K, Aubert I (2022) Ultrasound delivery of a TrkA agonist confers neuroprotection to Alzheimer-associated pathologies. Brain 145:2806–2822. https://doi.org/10.1093/brain/awab460
Jordão JF, Ayala-Grosso CA, Markham K, Huang Y, Chopra R, McLaurin JA et al (2010) Antibodies targeted to the brain with image-guided focused ultrasound reduces amyloid-β plaque load in the TgCRND8 mouse model of Alzheimer’s disease. PLoS ONE 5:4–11. https://doi.org/10.1371/journal.pone.0010549
Bathini P, Sun T, Schenk M, Schilling S, Mcdannold NJ, Lemere CA (2022) Acute effects of focused ultrasound-induced blood-brain barrier opening on anti-pyroglu3 abeta antibody delivery and immune responses. Biomolecules 12:951. https://doi.org/10.3390/biom12070951
Sun T, Shi Q, Zhang Y, Power C, Hoesch C, Antonelli S et al (2021) Focused ultrasound with anti-pGlu3 Aβ enhances efficacy in Alzheimer’s disease-like mice via recruitment of peripheral immune cells. J Control Release 336:443–456. https://doi.org/10.1016/j.jconrel.2021.06.037
Leinenga G, Koh WK, Götz J (2021) A comparative study of the effects of Aducanumab and scanning ultrasound on amyloid plaques and behavior in the APP23 mouse model of Alzheimer disease. Alzheimer’s Res Ther 13:1–14. https://doi.org/10.1186/s13195-021-00809-4
Safety and Feasibility of Exablate Blood-Brain Barrier Disruption for Mild Cognitive Impairment or Mild Alzheimer’s Disease Undergoing Aduhelm Therapy. Clin Identifier NCT05469009 (2023). https://beta.clinicaltrials.gov/study/NCT05469009. Accessed 10 Jan 2023
Fu HJ, Liu B, Frost JL, Lemere CA (2010) Amyloid-β immunotherapy for Alzheimer’s disease. CNS Neurol Disord Drug Targets 9:197–206. https://doi.org/10.2174/187152710791012017
Raymond SB, Treat LH, Dewey JD, Mcdannold NJ, Hynynen K, Bacskai BJ (2008) Ultrasound enhanced delivery of molecular imaging and therapeutic agents in Alzheimer’s disease mouse models. PLoS ONE 3:1–7. https://doi.org/10.1371/journal.pone.0002175
Antoniou A, Giannakou M, Georgiou E, Kleopa KA, Damianou C (2022) Robotic device for transcranial focussed ultrasound applications in small animal models. Int J Med Robot Comput Assist Surg. https://doi.org/10.1002/rcs.2447
Madsen EL, Dong F, Frank GR, Garra BS, Wear KA, Wilson T et al (1999) Interlaboratory comparison of ultrasonic backscatter, attenuation, and speed measurements. J Ultrasound Med 18:615–631. https://doi.org/10.7863/jum.1999.18.9.615
Todd N, Zhang Y, Arcaro M, Becerra L, Borsook D, Livingstone M et al (2018) Focused ultrasound induced opening of the blood-brain barrier disrupts inter-hemispheric resting state functional connectivity in the rat brain. Neuroimage 178:414–422. https://doi.org/10.1016/j.neuroimage.2018.05.063
Burgess A, Kullervo HH (2014) Drug delivery across the blood-brain barrier using focused ultrasound. Expert Opin Drug Deliv 11:711–721. https://doi.org/10.1517/17425247.2014.897693
Gandhi K, Barzegar-Fallah A, Banstola A, Rizwan SB, Reynolds JNJ (2022) Ultrasound-mediated blood-brain barrier disruption for drug delivery: a systematic review of protocols, efficacy, and safety outcomes from preclinical and clinical studies. Pharmaceutics. https://doi.org/10.3390/pharmaceutics14040833
Plotkin SS, Cashman NR (2020) Passive immunotherapies targeting Aβ and tau in Alzheimer’s disease. Neurobiol Dis. https://doi.org/10.1016/j.nbd.2020.105010
Lemere CA (2013) Immunotherapy for Alzheimer’s disease: hoops and hurdles. Mol Neurodegener 8:1–6. https://doi.org/10.1186/1750-1326-8-36
Hughes JM, Neese OR, Bieber DD, Lewis KA, Ahmadi LM, Parsons DW et al (2022) The effects of propofol on a human in vitro blood-brain barrier model. Front Cell Neurosci 16:1–13. https://doi.org/10.3389/fncel.2022.835649
Sheikov N, McDannold N, Vykhodtseva N, Jolesz F, Hynynen K (2004) Cellular mechanisms of the blood-brain barrier opening induced by ultrasound in presence of microbubbles. Ultrasound Med Biol 30:979–989. https://doi.org/10.1016/j.ultrasmedbio.2004.04.010
Wasielewska JM, White AR (2022) Focused ultrasound-mediated drug delivery in humans – a path towards translation in neurodegenerative diseases. Pharm Res 39:427–439. https://doi.org/10.1007/s11095-022-03185-2
Hynynen K, Mcdannold N, Sheikov NA, Jolesz FA, Vykhodtseva N (2005) Local and reversible blood – brain barrier disruption by noninvasive focused ultrasound at frequencies suitable for trans-skull sonications. Neuroimage 24:12–20. https://doi.org/10.1016/j.neuroimage.2004.06.046
Saunders NR, Dziegielewska KM, Møllgård K, Habgood MD (2015) Markers for blood-brain barrier integrity: how appropriate is Evans blue in the twenty-first century and what are the alternatives? Front Neurosci 9:1–16. https://doi.org/10.3389/fnins.2015.00385
McDannold N, Vykhodtseva N, Hynynen K (2007) Use of ultrasound pulses combined with definity for targeted blood-brain barrier disruption: a feasibility study. Ultrasound Med Biol 33:584–590. https://doi.org/10.1016/j.ultrasmedbio.2006.10.004
McDannold N, Vykhodtseva N, Hynynen K (2008) Effects of acoustic parameters and ultrasound contrast agent dose on focused-ultrasound induced blood-brain barrier disruption. Ultrasound Med Biol 34:930–937. https://doi.org/10.1016/j.ultrasmedbio.2007.11.009
Oakley H, Cole SL, Logan S, Maus E, Shao P, Craft J et al (2006) Intraneuronal β-amyloid aggregates, neurodegeneration, and neuron loss in transgenic mice with five familial Alzheimer’s disease mutations: Potential factors in amyloid plaque formation. J Neurosci 26:10129–10140. https://doi.org/10.1523/JNEUROSCI.1202-06.2006
Angeli S, Kousiappa I, Stavrou M, Sargiannidou I, Georgiou E, Papacostas SS et al (2020) Altered expression of glial gap junction proteins Cx43, Cx30, and Cx47 in the 5XFAD model of Alzheimer’s disease. Front Neurosci 14:1–20. https://doi.org/10.3389/fnins.2020.582934
Jankowsky JL, Fadale DJ, Anderson J, Xu GM, Gonzales V, Jenkins NA et al (2004) Mutant presenilins specifically elevate the levels of the 42 residue β-amyloid peptide in vivo: evidence for augmentation of a 42-specific γ secretase. Hum Mol Genet 13:159–170. https://doi.org/10.1093/hmg/ddh019
Radde R, Bolmont T, Kaeser SA, Coomaraswamy J, Lindau D, Stoltze L et al (2006) Aβ42-driven cerebral amyloidosis in transgenic mice reveals early and robust pathology. EMBO Rep 7:940–946. https://doi.org/10.1038/sj.embor.7400784
Claeysen S, Giannoni P, Ismeurt C (2020) The 5xFAD mouse model of Alzheimer ’ s disease. The neuroscience of dementia. Diagnosis and management in dementia. Academic Press, pp 207–221. https://doi.org/10.1016/B978-0-12-815854-8.00013-6f
Schoch A, Thorey IS, Engert J, Winter G, Emrich T (2014) Comparison of the lateral tail vein and the retro-orbital venous sinus routes of antibody administration in pharmacokinetic studies. Lab Anim (NY) 43:95–99. https://doi.org/10.1038/laban.481
Steel CD, Stephens AL, Hahto SM, Singletary SJ (2008) Comparison of the lateral tail vein and the retro-orbital venous sinus as routes of intravenous drug delivery in a transgenic mouse model. Lab Anim (NY). https://doi.org/10.1038/laban0108-26
Sheikov N, McDannold N, Sharma S, Hynynen K (2008) Effect of focused ultrasound applied with an ultrasound contrast agent on the tight junctional integrity of the brain microvascular endothelium. Ultrasound Med Biol 34:1093–1104. https://doi.org/10.1016/j.ultrasmedbio.2007.12.015
Downs ME, Buch A, Sierra C, Karakatsani ME, Chen S, Konofagou EE et al (2015) Long-term safety of repeated blood-brain barrier opening via focused ultrasound with microbubbles in non-human primates performing a cognitive task. PLoS ONE 10:1–26. https://doi.org/10.1371/journal.pone.0125911
Suzuki K, Iwata A, Iwatsubo T (2017) The past, present, and future of disease-modifying therapies for Alzheimer’s disease. Proc Jpn Acad Ser B 93:757–771. https://doi.org/10.2183/pjab.93.048
Choi JJ, Pernot M, Small SA, Konofagou EE (2007) Noninvasive, transcranial and localized opening of the blood-brain barrier using focused ultrasound in mice. Ultrasound Med Biol 33:95–104. https://doi.org/10.1016/j.ultrasmedbio.2006.07.018
Choi JJ, Selert K, Gao Z, Samiotaki G, Baseri B, Konofagou EE (2011) Noninvasive and localized blood—brain barrier disruption using focused ultrasound can be achieved at short pulse lengths and low pulse repetition frequencies. J Cereb Blood Flow Metab 31:725–737. https://doi.org/10.1038/jcbfm.2010.155
Wang S, Samiotaki G, Olumolade O, Feshitan JA, Konofagou EE (2014) Microbubble type and distribution dependence of focused ultrasound-induced blood-brain barrier opening. Ultrasound Med Biol 40:130–137. https://doi.org/10.1016/j.ultrasmedbio.2013.09.015
Shin J, Kong C, Cho JS, Lee J, Koh CS, Yoon MS et al (2018) Focused ultrasound-mediated noninvasive blood-brain barrier modulation: preclinical examination of efficacy and safety in various sonication parameters. Neurosurg Focus 44:1–10. https://doi.org/10.3171/2017.11.FOCUS17627
Song KH, Fan AC, Hinkle JJ, Newman J, Borden MA, Harvey BK (2017) Microbubble gas volume: a unifying dose parameter in blood-brain barrier opening by focused ultrasound. Theranostics 7:144–152. https://doi.org/10.7150/thno.15987
Acknowledgements
The study was co-funded by the European Structural & Investment Funds (ESIF) and the Republic of Cyprus through the Research and Innovation Foundation (RIF) under the project SOUNDPET (INTEGRATED/0918/0008).
Funding
Open access funding provided by the Cyprus Libraries Consortium (CLC). This research was funded by the Research and Innovation Foundation of Cyprus, under the project SOUNDPET (INTEGRATED/0918/0008).
Author information
Authors and Affiliations
Contributions
AA contributed to the data collection, interpretation of results, and drafting of manuscript. MS contributed to the data collection and analysis, as well as the drafting of manuscript. NE and EG contributed to data collection. IK, AK, and SSP contributed to the study conception and design and interpretation of results. KAK contributed to the study conception and design. CD had the overall supervision of the study.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no conflict of interest.
Ethical approval
All animal experiments were approved by the authorities of Veterinary Services, Ministry of Agriculture, Cyprus under the study license CY/EXP/PR.L05/2021.
Consent to participate
Not applicable. The study does not include data on patients.
Consent to publish
Not applicable. The study does not include data on patients.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Antoniou, A., Stavrou, M., Evripidou, N. et al. FUS-mediated blood–brain barrier disruption for delivering anti-Aβ antibodies in 5XFAD Alzheimer’s disease mice. J Ultrasound 27, 251–262 (2024). https://doi.org/10.1007/s40477-023-00805-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40477-023-00805-4