
Abstract
Purpose of Review
Mayaro virus is an arbovirus that circulates in a wild cycle transmitted by Haemagogus janthinomys; however, case reports in urban areas suggest that other arthropods could be acting as vectors. It shares several similarities with Chikungunya virus, being highly probable that many cases are being misdiagnosed. The disease caused by this pathogen is known as Mayaro fever, which is restricted to regions of Central and South America, mainly the Amazon rainforest. Cases of Mayaro fever have continuously been increasing, suggesting that Mayaro virus would become another major epidemic arbovirus in America.
Recent Findings
Four electronic databases were searched for articles in English and Spanish using the keywords “Mayaro” and “case.” A total of 234 cases were retrieved in the 23 selected manuscripts. Of all cases, most of them were male young adults, reported as autochthonous cases occurring mainly in Peru and Brazil, who were performing activities in wild rural areas. Fever, arthralgia, headache, myalgia, and retro-orbital pain were the main clinical manifestations. Most of the patients had laboratory parameters within the normal range, joint complications were evidenced in few cases, and all of them recovered without specific treatment.
Summary
Mayaro fever appears to be a mild self-limited disease that affects mainly males at productive age that are in contact with wild environments. However, further studies are required to establish its true pathogenic potential of Mayaro virus.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Arboviral infections, or arthropod-borne viral infections, are one of the most important causes of disease in tropical and subtropical regions worldwide and one of the most critical global public health problems [1]. Arboviruses belong to five families: Bunyaviridae, Flaviviridae, Orthomyxoviridae, Reoviridae, and Togaviridae, and they are transmitted by a wide range of arthropod vectors such as mosquitoes and ticks, which can be circulating in an urban environment or their biological cycle is restricted to wildlife [2,3,4]. Dengue virus (DENV), Chikungunya virus (CHIKV), and Zika virus (ZIKV) are the most known and the main arboviruses of public health importance for local surveillance systems worldwide [2, 5]. However, there are several other neglected arboviral species for which particular attention must be given due to their fast spreading as a result of the geographical expansion of mosquitoes due to climate change and the increase in land use [6, 7].
Three arboviruses, Venezuelan equine encephalitis virus (VEEV), Oropouche virus, and Mayaro virus (MAYV), have been proposed as candidates for the next arboviral epidemic, at least in the Americas [8]. MAYV (Alphavirus genus, Togaviridae family) is a single-stranded RNA virus that forms part of the Semliki complex along with CHIKV, Bebaru, Getah, O’nyong-nyong, Ross River, Semliki Forest, and Una viruses [9]. This arbovirus circulates in a natural wild cycle among different animal species through the bite of female mosquitoes of the genus Haemagogus, being Haemagogus janthinomys its main important vector [10]. However, reports of the disease in urban areas have suggested that MAYV might have been introduced into urban environments in which other mosquito species, such as Aedes and Culex spp., could be acting as vectors, since vector competence has already been evaluated and demonstrated for some species [11].
MAYV was first detected in 1954 in Trinidad and Tobago in the serum of forest workers [12]. It shares biological, epidemiological, and clinical similarities with other arboviruses from the Americas, of which the most closely related is CHIKV; being highly probable that cases due to MAYV may have been misdiagnosed as CHIKV for a long time as both of them share similar geographical distribution and other features [13, 14]. The disease caused by MAYV is usually denominated as Mayaro fever, and it has been restricted to several countries of Central and South America, which territories form part or surrounds the Amazon rainforest, which is considered the main important region where MAYV is actively circulating [15, 16]. During the last years, cases due to MAYV have continuously been increasing, and reports of the disease have been more frequent, suggesting that MAYV is close to becoming another major epidemic arbovirus in Americas soon [17].
Likely, the global burden of Mayaro fever is still underestimated, mainly due to the health personnel’s lack of accurate diagnostic methods and clinical suspicion [18]. MAYV laboratory confirmatory diagnosis can be made using different virological, serological, or molecular methods. The virus can be detected through viral isolation in cell cultures; however, this method can only be performed in reference laboratories [19]. Another alternative is the detection of the viral RNA through reverse transcription (RT) polymerase chain reaction (PCR), being highly useful during the acute phase of infection [20]. Additionally, the detection of antibodies to MAYV through serological methods such as enzyme-linked immunoassay (ELISA) and indirect immunofluorescence assay (IFA) can be used as indirect diagnosis; however, its interpretation must be carefully made since cross-reactivity can occur with other alphaviruses; thus, usually, detection of antibodies needs a confirmation method such as plaque reduction neutralization testing (PRNT) or the evidence of seroconversion between acute and convalescent serum samples [21, 22].
Descriptions of clinical, epidemiological, and laboratory features of MAYV infection have been done in some narrative reviews; however, since its first description, several reports of cases of the disease were done by many authors contributing to the knowledge of the disease behavior; nevertheless, to our knowledge, no systematic review related to MAYV infection has been published to date, being essential to characterize the disease before its burden to improve its suspicion among clinicians. Thus, this systematic review aims to evaluate all available evidence regarding the clinical, epidemiological, and laboratory features of MAYV infection.
Methods
Search Strategy and Selection Criteria
We followed the recommendations made by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) to guide all the steps of this review. Searching for scientific literature was carried out on June 8th 2023, in four scientific literature databases: PubMed MEDLINE, EMBASE, Scopus, and BVS. A search using the terms [“Mayaro” AND “case”] was performed in all four databases. The references of all the articles were extracted and collected in a library created in the “EndNoteX8” program combining all different searches. Once the reference list was created, the elimination of duplicate articles was carried out using the automatic tool of the program. The procedure results provided a list of potentially valuable articles for analysis and selection.
We reviewed all the literature managed in the eligible list to choose those that would be part of this review. The inclusion criteria were case reports, clinical cases, and other papers written in English or Spanish, with reports of confirmed human cases of Mayaro fever and information regarding epidemiological data, clinical manifestations, and laboratory results available. Those publications that did not fulfill inclusion criteria were excluded.
Data Extraction
We independently screened the titles and abstracts to identify relevant reports. Possible disagreements were resolved through the author’s discussion. Data were extracted from all the included studies and tabulated in Excel. For each article, we extracted information related to the clinical features of all confirmed cases. Additionally, we also performed the data extraction related to the country of the patient’s origin, country of travel where the infection was presumed to have occurred, sex and age of the reported patients, working and leisure activities, hematological and biochemical laboratory findings, complications, treatment, need for hospitalization, and clinical outcome.
Definitions
Following the recommendations of the Pan American Health Organization (https://www.paho.org, accessed on June 8th 2023), we defined a confirmed case of Mayaro fever as a disease caused by MAYV, which diagnosis was made by at least one of the following methodologies recommended: detection of viral RNA in serum samples through conventional or real-time RT-PCR, viral isolation with later confirmation by molecular methods, detection of IgM or IgG antibodies through ELISA or IFA in a single serum sample confirmed by PRNT panel with negative results against other alphaviruses, or seroconversion of IgG antibodies of more than four titers (fourfold change) between paired acute and convalescent serum samples without seroconversion against other alphaviruses.
Results
Scientific Literature Search
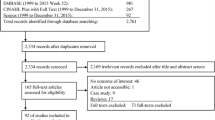
Figure 1 summarizes our search procedure. Using the terms [“Mayaro” AND “case”], 28, 44, 107, and 311 publications were found in the PubMed MEDLINE, EMBASE, Scopus, and BVS databases, respectively, giving a total of 490 scientific manuscripts, which were extracted and loaded in the EndNoteX8 program to eliminate duplicate publications, giving a total of 410 eligible scientific manuscripts.

Search strategy for the systematic review
Literature Selection
From the eligible list of 410 scientific manuscripts, we selected 23 as they fulfilled our inclusion criteria and case definition. A total of 387 publications were discarded as they were manuscripts in which the central topic was not MAYV, studies regarding the biology or epidemiology of MAYV or its vectors, repeated publications which were not automatically removed by the EndNoteX8 tool, review articles, publications in a language other than English or Spanish, and book chapters.
Demographic and Epidemiological Data
A total of 234 clinical cases were reported in the 23 selected publications [12, 19, 23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40, 41•, 42, 43]. Data related to age, sex, autochthonous cases, imported cases detailing country of origin and country of travel, and working and leisure activities are shown in Table 1. Regarding age, 39% were young adults, 25.8% were middle-aged adults, 10.1% were teenagers and senior adults, 8.1% were children, and 6.9% were infants. Most patients, 56.1%, were males, and the remaining 43.9% were females. Almost all (96.6%) were autochthonous cases, occurring mainly in Peru (54.9%) and Brazil (38.1%), followed by Venezuela (4.4%), Trinidad and Tobago (2.2%), and Haiti (0.4%) (Fig. 2). The remaining 3.4% were imported cases among patients from the Netherlands (37.5%), France, Germany (25%), and Switzerland (12.5%), which acquired the disease while traveling to Brazil, French Guiana, Surinam (25%), Bolivia, and Peru (12.5%) (Fig. 3). Several working and leisure activities were identified among some patients as follows: 22.5% were housekeepers; 12.5% were forest workers, lumberjacks, and people who were doing ecotourism; 10% were farmers and people fishing; 7.5% were having dinner outside while camping; 5% were people doing butterfly hunting and military personnel; and 2.5% were biologists performing research and wildlife volunteers.

Countries and regions where autochthonous cases of Mayaro fever have been reported. Countries in red are the ones in which cases of Mayaro fever occurred. Yellow dots refer to specific sites where one or more autochthonous cases of the disease were reported

Countries where imported cases of Mayaro virus infection have been reported and region where the disease was probably acquired. Countries in emerald green marked with a yellow cross refer to the patients’ origin. Countries in red are the ones in which the infection may have acquired. Yellow dots refer to specific sites where the infection may have acquired. Segmented lines with the figure of an airplane refer to the pathway from the probable site of infection to the site where the disease was imported. Asterisk (*) symbol means two cases
Clinical Data
The most frequent clinical manifestations are included in Table 2. Of all reported cases, 90.6% had fever, 63.7% had arthralgia, 61.5% reported headache, 50% had myalgia, and 47.4% reported retro-orbital pain. Other relevant signs and symptoms included body pain in 33.3%, nausea in 26.5%, any rash in 23.9%, chills and hyporexia in 15.4%, vomiting in 15%, joint swollen and sore throat in 12.4%, abdominal pain in 10.3%, diarrhea in 6.8%, and cough in 6.4%. Several other clinical manifestations such as jaundice, conjunctival injection, joint tenderness, fatigue, nasal congestion, asthenia, somnolence, and dizziness, among others, were also reported in some patients, but they were present in less than ten patients; therefore, they were not considered in the present review.
Laboratory Features
Hematologic and biochemical laboratory available data were extracted from all Mayaro fever cases included in the present study (Table 3). From all reported cases, excluding those in which data were unavailable, most of the patients (82.8%) had their laboratory parameters within the normal range. Only 17.2% of cases had an abnormal alteration in any of these hematologic or biochemical parameters, which included leukocytosis (39.1%), leukopenia (34.8%), elevated alanine aminotransferase, thrombocytopenia (21.7%), prolonged erythrocyte sedimentation rate, lymphocytosis (17.4%), elevated aspartate aminotransferase (8.7%), elevated C-reactive protein, hematocrit, lactate dehydrogenase, and lymphopenia (4.3%).
Treatment and Outcomes
Treatment, complications, need for hospitalization, and clinical outcomes data were retrieved and analyzed for the present manuscript (Table 4). From all reported cases, data regarding treatment (96.2% [n = 225]), complications (95.7% [n = 224]), need for hospitalization (82.9% [n = 194]), and clinical outcome (64.1% [n = 150]) were not reported in most of the cases. When information was available, supportive therapy with hydration and anti-inflammatory drugs was administered in 88.9% of cases, and 11.1% did not receive any therapy; persistent chronic arthralgia and joint symptoms were reported as the only complications identified; most of the patients, 95% in total, did not require hospitalization, and only 5% were hospitalized during the course of their disease; and finally, total recovery was reported in all cases without any evidence of the fatal outcome.
Discussion
MAYV is closest to becoming the next arbovirus of epidemiological importance, at least in the American continent [18]; it is necessary to know more about the pathogen and the disease it causes. The present review analyzed several epidemiological, clinical, and laboratory features among reported cases of Mayaro fever in scientific literature. The analysis revealed that more than half of reported cases were males, young adults, and middle-aged adults, which comprise the majority of the working-age population [44] in tropical rural areas, and are the leading group that is exposed to wild environments due to the economic activities performed in these regions [45]. Rural working activities in the tropics, such as agriculture, farming, and others performed in wild environments (e.g., forest workers, lumberjacks, biologists), have been identified as significant risk factors for the emergence of a wide range of zoonotic pathogens due to extensive land use change, livestock revolution increase, and human invasion of wild ecosystems, which lead to tropical deforestation and displacement of wildlife [46, 47]. Some of these working activities have been identified in the present review among patients with Mayaro fever, and leisure and fun activities related to ecotourism, such as camping, fishing, and butterfly hunting, have also been identified among cases of Mayaro fever. Ecotourism has critical ecological consequences; although activities related to ecotourism do not produce deforestation, human presence in natural environments disturbs the behavior of animals, affecting the structure of ecological communities favoring the contact human-wildlife, which represents a high-risk factor for the emergence of pathogens circumscribed to wildlife to which humans have never been previously exposed, similar to what probably occurred with MAYV [48, 49].
Although MAYV was first isolated from human symptomatic cases in Trinidad and Tobago [12] and few probable and confirmed cases have been reported in countries of the Caribbean region such as Panama, Mexico, and Haiti [35, 50, 51], the present review identified that most of the reported cases had acquired the disease in the Amazon rainforest and surrounding areas of Brazil, Peru, and Venezuela. Furthermore, imported cases have also been identified among European travelers. They all got infected by MAYV while visiting some countries that form part of the Amazon rainforest (e.g., Bolivia, French Guiana, Surinam). Studies performed in the Amazon rainforest have identified that several arboviruses pathogenic for humans are actively circulating in this region, producing local outbreaks [52•], and incidence rates have increased in recent times due to extensive deforestation [53]. MAYV is usually circulating in a wild cycle within its sylvatic vectors. Several were wild animal species [54], but due to human invasion of wildlife, MAYV is in transition, adapting its biological cycle to an urban ecosystem; this virus may probably be linked to rural and urban autochthonous cases [55]. MAYV may adapt to urban and peri-urban mosquitoes, or the classical vectors change their habits and adapt to an urban ecosystem. In that case, MAYV may become urbanized, establishing and spreading in human settlements [56].
Since its emergence, Mayaro fever has formed part of the etiology of acute undifferentiated febrile illness (AUFI), a syndrome caused by a broad range of pathogens which generate a fever of less than 2 weeks of duration accompanied by a great variety of non-specific signs and symptoms, in several regions of Central and South America [43, 57], being essential to understand its clinical presentation. Through the present review, 53 clinical manifestations were identified among reported cases of Mayaro fever, of which 36 were present in less than ten cases. They were not taken into account for the present review. Four of the remaining 17 clinical manifestations (fever, arthralgia, headache, and myalgia) were present in at least half of the cases, being the most frequent and relevant signs and symptoms of Mayaro fever. Among all clinical manifestations described, the development of abrupt fever, arthralgia or arthritis, and maculopapular rash have been described as a clinical triad highly indicative of Mayaro fever [9, 18]; however, this triad may not be helpful as through the present review. It has been identified that only fever and arthralgia are common clinical manifestations, and only less than one-quarter of patients develop any rash. Arthralgia is probably the most essential symptom that could help to suspect the disease.
The presence of joint manifestations in a febrile patient in the tropics is highly indicative of alphavirus infection (e.g., O’nyong-nyong virus, Sindbis virus), and in South America and the Caribbean region, besides MAYV, CHIKV is another etiology that must simulate an arthritogenic AUFI [58, 59]. CHIKV, along with DENV and ZIKV, are the main arboviruses worldwide whose diseases are of significance for the surveillance systems of a large number of countries across the globe, and for which, there are still many challenges to improve their control [5, 60]. Notwithstanding, there are several neglected arboviruses, such as MAYV, which importance remains underestimated. Several cases of Mayaro fever have probably been misdiagnosed as CHIKV due to similar clinical presentation and geographic distribution [61]. Cases of co-infection between MAYV and CHIKV are not rare and can occur [62••]; however, the correct diagnosis is not always performed due to the greater importance of CHIKV over MAYV for epidemiological surveillance systems [18].
Only narrative reviews have suggested that leukopenia and thrombocytopenia are the main laboratory alterations that could suggest a Mayaro infection [9, 63]. The present review is the first one in which the laboratory profile of MAYV infection was characterized, identifying that most cases had their biochemical and hematological parameters within normal ranges, probably due to the mild course of the disease [9, 64]. According to our analysis, if laboratory alterations occur, neither leukopenia nor thrombocytopenia could suggest Mayaro fever and do not help the clinical suspicion. Other altered laboratory parameters, such as prolonged erythrocyte sedimentation rate and elevated liver enzymes, have been identified among a few Mayaro fever cases, which have also been identified during the disease of other alphaviruses [65].
Finally, information regarding treatment, complications, and the need for hospital management was not available in more than three-quarters of reported cases; the authors probably considered this information irrelevant due to the mild course of Mayaro fever. However, available information regarding these topics confirms that Mayaro fever is a mild, self-limited disease. Even without supportive treatment, all patients have recovered completely without needing hospitalization in most cases, with chronic arthralgia the only complication reported in a few patients. Through this review, any fatal outcome due to MAYV infection has been identified; however, in Mexico, a likely fatal outcome due to encephalopathy caused by MAYV infection was reported [50]; nevertheless, evidence regarding its confirmatory diagnosis (positive ELISA IgM in convalescent serum sample without evaluation of other alphaviruses) is insufficient to be considered a Mayaro fever case, being probable that other not evaluated alphaviruses, such as Venezuelan encephalitis virus [66, 67] or even CHIKV [68], were linked to this fatal outcome.
Mayaro fever appears to be a mild self-limiting disease with underestimated importance due to its benign behavior; however, it is very likely that the true potential of MAYV as a human pathogen is not fully elucidated, as was the case with ZIKV in the past, which was considered a mild and minor disease until cases of congenital malformations and neurodegenerative diseases were reported [69,70,71]. Thus, MAYV requires further studies to establish its true pathogenic potential and its importance within infectious diseases.
Conclusions
The present review has identified that Mayaro fever is one of the causes of AUFI in several countries in South America and the Caribbean region, and the Amazon rainforest is the main endemic region in which MAYV is actively circulating. Males at productive age are the higher-risk group due to the economic activities performed in rural areas, such as agriculture and farming. Moreover, leisure activities related to ecotourism are also crucial for acquiring the disease in endemic areas, and imported cases of Mayaro fever in other regions are essential travel medicine diseases. Clinically, it forms part of the etiology of AUFI in South America and the Caribbean region; however, the presence of fever, arthralgia, headache, and myalgia could give a slight suspicion of the disease. Laboratory parameters are usually normal, and when alterations occur, none of them can help to reach the diagnosis or at least suspect Mayaro fever. Fortunately, to date, MAYV is a mild AUFI that can even be self-limited without needing any supportive therapy or hospitalization; however, few patients can develop chronic arthralgia without compromising their life.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Girard M, Nelson CB, Picot V, Gubler DJ. Arboviruses: a global public health threat. Vaccine. 2020;38(24):3989–94. https://doi.org/10.1016/j.vaccine.2020.04.011.
Jones R, Kulkarni MA, Davidson TMV, RADAM-LAC Research Team, Talbot B. Arbovirus vectors of epidemiological concern in the Americas: a scoping review of entomological studies on Zika, dengue and chikungunya virus vectors. PLoS One. 2020;15(2):e0220753. https://doi.org/10.1371/journal.pone.0220753.
Valentine MJ, Murdock CC, Kelly PJ. Sylvatic cycles of arboviruses in non-human primates. Parasit Vectors. 2019;12(1):463. https://doi.org/10.1186/s13071-019-3732-0.
Weaver SC. Urbanization and geographic expansion of zoonotic arboviral diseases: mechanisms and potential strategies for prevention. Trends Microbiol. 2013;21(8):360–3. https://doi.org/10.1016/j.tim.2013.03.003.
Paixão ES, Teixeira MG, Rodrigues LC. Zika, chikungunya and dengue: the causes and threats of new and re-emerging arboviral diseases. BMJ Glob Health. 2018;3(1):e000530. https://doi.org/10.1136/bmjgh-2017-000530.
Rocklöv J, Dubrow R. Climate change: an enduring challenge for vector-borne disease prevention and control. Nat Immunol. 2020;21(5):479–83. https://doi.org/10.1038/s41590-020-0648-y.
Rodriguez-Morales AJ, Bonilla-Aldana, DK. Neglected arboviruses in Latin America. In: New advances in neglected tropical diseases; Rijeka D.M.A.S. Ed.; IntechOpen: London, UK, 2022.
Rodríguez-Morales AJ, Paniz-Mondolfi AE, Villamil-Gómez WE, Navarro JC. Mayaro, Oropouche and Venezuelan equine encephalitis viruses: following in the footsteps of Zika? Travel Med Infect Dis. 2017;15:72–3. https://doi.org/10.1016/j.tmaid.2016.11.001.
Acosta-Ampudia Y, Monsalve DM, Rodríguez Y, Pacheco Y, Anaya JM, Ramírez-Santana C. Mayaro: an emerging viral threat? Emerg Microbes Infect. 2018;7(1):163. https://doi.org/10.1038/s41426-018-0163-5.
Ali R, Mohammed A, Jayaraman J, Nandram N, Feng RS, Lezcano RD, Seeramsingh R, Daniel B, Lovin DD, Severson DW, Ramsubhag A. Changing patterns in the distribution of the Mayaro virus vector Haemagogus species in Trinidad. West Indies Acta Trop. 2019;199:105108. https://doi.org/10.1016/j.actatropica.2019.105108.
Pereira TN, Carvalho FD, De Mendonça SF, Rocha MN, Moreira LA. Vector competence of Aedes aegypti, Aedes albopictus, and Culex quinquefasciatus mosquitoes for Mayaro virus. PLoS Negl Trop Dis. 2020;14(4):e0007518. https://doi.org/10.1371/journal.pntd.0007518.
Anderson CR, Downs WG, Wattley GH, Ahin NW, Reese AA. Mayaro virus: a new human disease agent. II. Isolation from blood of patients in Trinidad, B.W.I. Am J Trop Med Hyg. 1957;6(6):1012–6. https://doi.org/10.4269/ajtmh.1957.6.1012.
Mattar S, González M. Mayaro and chikungunya; two alphaviruses with clinical and epidemiological similarities. Revista MVZ Córdoba. 2015;20:4861–3.
Hotez PJ, Murray KO. Dengue, West Nile virus, chikungunya, Zika-and now Mayaro? PLoS Negl Trop Dis. 2017;11(8):e0005462. https://doi.org/10.1371/journal.pntd.0005462.
Azevedo RS, Silva EV, Carvalho VL, Rodrigues SG, Nunes-Neto JP, Monteiro H, Peixoto VS, Chiang JO, Nunes MR, Vasconcelos PF. Mayaro fever virus, Brazilian Amazon. Emerg Infect Dis. 2009;15(11):1830–2. https://doi.org/10.3201/eid1511.090461.
Halsey ES, Siles C, Guevara C, Vilcarromero S, Jhonston EJ, Ramal C, Aguilar PV, Ampuero JS. Mayaro virus infection, Amazon Basin region, Peru, 2010–2013. Emerg Infect Dis. 2013;19(11):1839–42. https://doi.org/10.3201/eid1911.130777.
Esposito DLA, Fonseca BALD. Will Mayaro virus be responsible for the next outbreak of an arthropod-borne virus in Brazil? Braz J Infect Dis. 2017;21(5):540–4. https://doi.org/10.1016/j.bjid.2017.06.002.
de Mota OMT, Avilla CM, Nogueira ML. Mayaro virus: a neglected threat could cause the next worldwide viral epidemic. Future Virol. 2019;14(6):375–7.
Terzian AC, Auguste AJ, Vedovello D, Ferreira MU, da Silva-Nunes M, Sperança MA, Suzuki RB, Juncansen C, Araújo JP Jr, Weaver SC, Nogueira ML. Isolation and characterization of Mayaro virus from a human in Acre, Brazil. Am J Trop Med Hyg. 2015;92(2):401–4. https://doi.org/10.4269/ajtmh.14-0417.
Waggoner JJ, Rojas A, Mohamed-Hadley A, de Guillén YA, Pinsky BA. Real-time RT-PCR for Mayaro virus detection in plasma and urine. J Clin Virol. 2018;98:1–4. https://doi.org/10.1016/j.jcv.2017.11.006.
Figueiredo LT, Nogueira RM, Cavalcanti SM, Schatzmayr H, da Rosa AT. Study of two different enzyme immunoassays for the detection of Mayaro virus antibodies. Mem Inst Oswaldo Cruz. 1989;84(3):303–7. https://doi.org/10.1590/s0074-02761989000300003.
Fumagalli MJ, de Souza WM, Romeiro MF, de Souza Costa MC, Slhessarenko RD, Figueiredo LTM. Development of an enzyme-linked immunosorbent assay to detect antibodies targeting recombinant envelope protein 2 of Mayaro virus. J Clin Microbiol. 2019;57(5):e01892-e1918. https://doi.org/10.1128/JCM.01892-18.
Causey OR, Maroja OM. Mayaro virus: a new human disease agent. III. Investigation of an epidemic of acute febrile illness on the river Guama in Pará, Brazil, and isolation of Mayaro virus as causative agent. Am J Trop Med Hyg. 1957;6(6):1017–23.
Torres JR, Russell KL, Vasquez C, Barrera R, Tesh RB, Salas R, Watts DM. Family cluster of Mayaro fever. Venezuela Emerg Infect Dis. 2004;10(7):1304–6. https://doi.org/10.3201/eid1007.030860.
Coimbra TL, Santos CL, Suzuki A, Petrella SM, Bisordi I, Nagamori AH, Marti AT, Santos RN, Fialho DM, Lavigne S, Buzzar MR, Rocco IM. Mayaro virus: imported cases of human infection in São Paulo State, Brazil. Rev Inst Med Trop Sao Paulo. 2007;49(4):221–4. https://doi.org/10.1590/s0036-46652007000400005.
Hassing RJ, Leparc-Goffart I, Blank SN, Thevarayan S, Tolou H, van Doornum G, van Genderen PJ. Imported Mayaro virus infection in the Netherlands. J Infect. 2010;61(4):343–5. https://doi.org/10.1016/j.jinf.2010.06.009.
Receveur MC, Grandadam M, Pistone T, Malvy D. Infection with Mayaro virus in a French traveller returning from the Amazon region, Brazil, January 2010. Euro Surveill. 2010;15(18):19563.
Mourão MP, Bastos Mde S, de Figueiredo RP, Gimaque JB, Galusso Edos S, Kramer VM, de Oliveira CM, Naveca FG, Figueiredo LT. Mayaro fever in the city of Manaus, Brazil, 2007–2008. Vector Borne Zoonotic Dis. 2012;12(1):42–6. https://doi.org/10.1089/vbz.2011.0669.
Neumayr A, Gabriel M, Fritz J, Günther S, Hatz C, Schmidt-Chanasit J, Blum J. Mayaro virus infection in traveler returning from Amazon Basin, northern Peru. Emerg Infect Dis. 2012;18(4):695–6. https://doi.org/10.3201/eid1804.111717.
Theilacker C, Held J, Allering L, Emmerich P, Schmidt-Chanasit J, Kern WV, Panning M. Prolonged polyarthralgia in a German traveller with Mayaro virus infection without inflammatory correlates. BMC Infect Dis. 2013;13:369. https://doi.org/10.1186/1471-2334-13-369.
Friedrich-Jänicke B, Emmerich P, Tappe D, Günther S, Cadar D, Schmidt-Chanasit J. Genome analysis of Mayaro virus imported to Germany from French Guiana. Emerg Infect Dis. 2014;20(7):1255–7. https://doi.org/10.3201/eid2007.140043.
Slegers CA, Keuter M, Günther S, Schmidt-Chanasit J, van der Ven AJ, de Mast Q. Persisting arthralgia due to Mayaro virus infection in a traveler from Brazil: is there a risk for attendants to the 2014 FIFA World Cup? J Clin Virol. 2014;60(3):317–9. https://doi.org/10.1016/j.jcv.2014.04.020.
Auguste AJ, Liria J, Forrester NL, Giambalvo D, Moncada M, Long KC, Morón D, de Manzione N, Tesh RB, Halsey ES, Kochel TJ, Hernandez R, Navarro JC, Weaver SC. Evolutionary and ecological characterization of Mayaro virus strains isolated during an outbreak, Venezuela, 2010. Emerg Infect Dis. 2015;21(10):1742–50. https://doi.org/10.3201/eid2110.141660.
Estofolete CF, Mota MT, Vedovello D, Góngora DV, Maia IL, Nogueira ML. Mayaro fever in an HIV-infected patient suspected of having chikungunya fever. Rev Soc Bras Med Trop. 2016;49(5):648–52. https://doi.org/10.1590/0037-8682-0093-2016.
Lednicky J, De Rochars VM, Elbadry M, Loeb J, Telisma T, Chavannes S, Anilis G, Cella E, Ciccozzi M, Okech B, Salemi M, Morris JG Jr. Mayaro virus in child with acute febrile illness, Haiti, 2015. Emerg Infect Dis. 2016;22(11):2000–2. https://doi.org/10.3201/eid2211.161015.
Llagonne-Barets M, Icard V, Leparc-Goffart I, Prat C, Perpoint T, André P, Ramière C. A case of Mayaro virus infection imported from French Guiana. J Clin Virol. 2016;77:66–8. https://doi.org/10.1016/j.jcv.2016.02.013.
Blohm GM, Márquez-Colmenarez MC, Lednicky JA, Bonny TS, Mavian C, Salemi M, Delgado-Noguera L, Morris JG, Paniz-Mondolfi AE. Isolation of Mayaro virus from a Venezuelan patient with febrile illness, arthralgias, and rash: further evidence of regional strain circulation and possible long-term endemicity. Am J Trop Med Hyg. 2019;101(6):1219–25. https://doi.org/10.4269/ajtmh.19-0357.
De La Cruz CH, Martínez SLA, Failoc-Rojas VE, Aguilar-Gamboa FR. Time to consider other arbovirus diseases after Mayaro virus. Revista Cubana de Medicina General Integral. 2019;35(2):1–7.
Aguilar-Luis MA, Del Valle-Mendoza J, Silva-Caso W, Gil-Ramirez T, Levy-Blitchtein S, Bazán-Mayra J, Zavaleta-Gavidia V, Cornejo-Pacherres D, Palomares-Reyes C, Del Valle LJ. An emerging public health threat: Mayaro virus increases its distribution in Peru. Int J Infect Dis. 2020;92:253–8. https://doi.org/10.1016/j.ijid.2020.01.024.
da Silva Pessoa Vieira CJ, José Ferreira da Silva D, Rigotti Kubiszeski J, Ceschini Machado L, Pena LJ, Vieira de Morais Bronzoni R, da Luz Wallau G. The emergence of chikungunya ECSA lineage in a Mayaro endemic region on the southern border of the Amazon forest. Trop Med Infect Dis. 2020;5(2):105. https://doi.org/10.3390/tropicalmed5020105
• Aguilar-Luis MA, Del Valle-Mendoza J, Sandoval I, Silva-Caso W, Mazulis F, Carrillo-Ng H, Tarazona-Castro Y, Martins-Luna J, Aquino-Ortega R, Peña-Tuesta I, Cornejo-Tapia A, Del Valle LJ. A silent public health threat: emergence of Mayaro virus and co-infection with dengue in Peru. BMC Res Notes. 2021;14(1):29. https://doi.org/10.1186/s13104-021-05444-8. This study provides evidence that symptoms in co-infected patients are also non-specific and that disease severity may not be associated with co-infections.
de Paula Silveira-Lacerda E, Laschuk Herlinger A, Tanuri A, Rezza G, Anunciação CE, Ribeiro JP, Tannous IP, Abrantes GR, da Silva EG, Arruda KF, de Sousa ARV, Romero Rebello Moreira F, Santana Aguiar R, Corrêa JF, Dos Santos MM, Silva HD, Garcia-Zapata MTA, do Nascimento NS, Talon de Menezes M, Araujo Maia R, Ferreira CO, Barbosa R, Brindeiro R, Cardoso C, Brunini SM. Molecular epidemiological investigation of Mayaro virus in febrile patients from Goiania City, 2017–2018. Infect Genet Evol. 2021;95:104981. https://doi.org/10.1016/j.meegid.2021.104981.
Watts DM, Russell KL, Wooster MT, Sharp TW, Morrison AC, Kochel TJ, Bautista CT, Block K, Guevara C, Aguilar P, Palermo PM, Calampa C, Porter KR, Hayes CG, Weaver SC, de Rosa AT, Vinetz JM, Shope RE, Gotuzzo E, Guzman H, Tesh RB. Etiologies of acute undifferentiated febrile illnesses in and near Iquitos from 1993 to 1999 in the Amazon River Basin of Peru. Am J Trop Med Hyg. 2022;107(5):1114–28. https://doi.org/10.4269/ajtmh.22-0259.
Snashall D. Health of the working age population. BMJ. 2008;336(7646):682. https://doi.org/10.1136/bmj.39532.509815.80.
Johnson TG. The rural economy in a new century. Int Reg Sci Rev. 2001;24(1):21–37.
Jones BA, Grace D, Kock R, Alonso S, Rushton J, Said MY, McKeever D, Mutua F, Young J, McDermott J, Pfeiffer DU. Zoonosis emergence linked to agricultural intensification and environmental change. Proc Natl Acad Sci U S A. 2013;110(21):8399–404. https://doi.org/10.1073/pnas.1208059110.
Vonesch N, Binazzi A, Bonafede M, Melis P, Ruggieri A, Iavicoli S, Tomao P. Emerging zoonotic viral infections of occupational health importance. Pathog Dis. 2019;77(2):ftz018. https://doi.org/10.1093/femspd/ftz018.
Chomel BB, Belotto A, Meslin FX. Wildlife, exotic pets, and emerging zoonoses. Emerg Infect Dis. 2007;13(1):6–11. https://doi.org/10.3201/eid1301.060480.
Shannon G, Larson CL, Reed SE, Crooks KR, Angeloni LM. Ecological consequences of ecotourism for wildlife populations and communities. Ecotourism’s promise and peril: a biological evaluation. 2017:29–46.
Navarrete-Espinosa J, Gómez-Dantés H. Arbovirus causales de fiebre hemorrágica en pacientes del Instituto Mexicano del Seguro Social. Rev Med Inst Mex Seguro Soc. 2006;44(4):347–53.
Srihongse S, Stacy HG, Gauld JR. A survey to assess potential human disease hazards along proposed sea level canal routes in Panamà and Colombia. IV. Arbovirus surveillance in man. Mil Med. 1973;138(7):422–6.
• Carvalho VL, Azevedo RSS, Carvalho VL, Azevedo RS, Henriques DF, Cruz ACR, Vasconcelos PFC, Martins LC. Arbovirus outbreak in a rural region of the Brazilian Amazon. J Clin Virol. 2022;150–151:105155. https://doi.org/10.1016/j.jcv.2022.105155. This is study evidence that Mayaro and other arboviruses can be responsible for outbreaks of febrile illnesses in the Amazon region.
da Silva CFA, Dos Santos AM, do Bonfim CV, da Silva Melo JL, Sato SS, Barreto EP. Deforestation impacts on dengue incidence in the Brazilian Amazon. Environ Monit Assess. 2023;195(5):593. https://doi.org/10.1007/s10661-023-11174-0.
de Thoisy B, Gardon J, Salas RA, Morvan J, Kazanji M. Mayaro virus in wild mammals, French Guiana. Emerg Infect Dis. 2003;9(10):1326–9. https://doi.org/10.3201/eid0910.030161.
Gonzalez-Escobar G, Churaman C, Rampersad C, Singh R, Nathaniel S. Mayaro virus detection in patients from rural and urban areas in Trinidad and Tobago during the chikungunya and Zika virus outbreaks. Pathog Glob Health. 2021;115(3):188–95. https://doi.org/10.1080/20477724.2021.1878445.
Mackay IM, Arden KE. Mayaro virus: a forest virus primed for a trip to the city? Microbes Infect. 2016;18(12):724–34. https://doi.org/10.1016/j.micinf.2016.10.007.
Mittal G, Ahmad S, Agarwal RK, Dhar M, Mittal M, Sharma S. Aetiologies of acute undifferentiated febrile illness in adult patients - an experience from a tertiary care hospital in Northern India. J Clin Diagn Res. 2015;9(12):DC22-4. https://doi.org/10.7860/JCDR/2015/11168.6990.
Kumar R, Ahmed S, Parray HA, Das S. Chikungunya and arthritis: an overview. Travel Med Infect Dis. 2021;44:102168. https://doi.org/10.1016/j.tmaid.2021.102168.
Suhrbier A, Jaffar-Bandjee MC, Gasque P. Arthritogenic alphaviruses–an overview. Nat Rev Rheumatol. 2012;8(7):420–9. https://doi.org/10.1038/nrrheum.2012.64.
Fritzell C, Rousset D, Adde A, Kazanji M, Van Kerkhove MD, Flamand C. Current challenges and implications for dengue, chikungunya and Zika seroprevalence studies worldwide: a scoping review. PLoS Negl Trop Dis. 2018;12(7):e0006533. https://doi.org/10.1371/journal.pntd.0006533.
Figueiredo MLGD, Figueiredo LTM. Emerging alphaviruses in the Americas: chikungunya and Mayaro. Rev Soc Bras Med Trop. 2014;47:677–83.
•• Dos Santos Souza Marinho R, Duro RLS, Bellini Caldeira D, Galinskas J, Oliveira Mota MT, Hunter J, Rodrigues Teles MDA, de Pádua Milagres FA, Sobhie Diaz R, Shinji Kawakubo F, Vasconcelos Komninakis S. Re-emergence of Mayaro virus and coinfection with chikungunya during an outbreak in the state of Tocantins/Brazil. BMC Res Notes. 2022;15(1):271. https://doi.org/10.1186/s13104-022-06153-6. This study reinforces the importance of Mayaro virus as a re-emergent pathogen that is expanding its geographical range to urban areas.
Yadav R, Jha M, Prasad S, Jat D, Jain DK. Mayaro virus (MAYV) disease: past, present and future. J Pharm Biol Sci. 2022;10(1):7–16.
Diagne CT, Bengue M, Choumet V, Hamel R, Pompon J, Missé D. Mayaro virus pathogenesis and transmission mechanisms. Pathogens. 2020;9(9):738. https://doi.org/10.3390/pathogens9090738.
Rahman MM, Been Sayed SJ, Moniruzzaman M, Kabir AKMH, Mallik MU, Hasan MR, Siddique AB, Hossain MA, Uddin N, Hassan MM, Chowdhury FR. Clinical and laboratory characteristics of an acute chikungunya outbreak in Bangladesh in 2017. Am J Trop Med Hyg. 2019;100(2):405–10. https://doi.org/10.4269/ajtmh.18-0636.
Adams AP, Navarro-Lopez R, Ramirez-Aguilar FJ, Lopez-Gonzalez I, Leal G, Flores-Mayorga JM, da Travassos Rosa AP, Saxton-Shaw KD, Singh AJ, Borland EM, Powers AM, Tesh RB, Weaver SC, Estrada-Franco JG. Venezuelan equine encephalitis virus activity in the Gulf Coast region of Mexico, 2003–2010. PLoS Negl Trop Dis. 2012;6(11):e1875. https://doi.org/10.1371/journal.pntd.0001875.
Morilla-Gonzales A, de Mucha-Macias J. Estudio de una epizootia de encefalitis equina de Venezuela ocurrida en Tamaulipas, Mexico. Rev Invest Salud Publica. 1969;29:3–20.
Mehta R, Gerardin P, de Brito CAA, Soares CN, Ferreira MLB, Solomon T. The neurological complications of chikungunya virus: a systematic review. Rev Med Virol. 2018;28(3):e1978. https://doi.org/10.1002/rmv.1978.
Costello A, Dua T, Duran P, Gülmezoglu M, Oladapo OT, Perea W, Pires J, Ramon-Pardo P, Rollins N, Saxena S. Defining the syndrome associated with congenital Zika virus infection. Bull World Health Organ. 2016;94(6):406-406A. https://doi.org/10.2471/BLT.16.176990.
Duffy MR, Chen TH, Hancock WT, Powers AM, Kool JL, Lanciotti RS, Pretrick M, Marfel M, Holzbauer S, Dubray C, Guillaumot L, Griggs A, Bel M, Lambert AJ, Laven J, Kosoy O, Panella A, Biggerstaff BJ, Fischer M, Hayes EB. Zika virus outbreak on Yap Island, Federated States of Micronesia. N Engl J Med. 2009;360(24):2536-43. https://doi.org/10.1056/NEJMoa0805715.
Nascimento OJM, da Silva IRF. Guillain-Barré syndrome and Zika virus outbreaks. Curr Opin Neurol. 2017;30(5):500–7. https://doi.org/10.1097/WCO.0000000000000471.
Funding
Open Access funding provided by Colombia Consortium
Author information
Authors and Affiliations
Contributions
Conceptualization: C.R.S.-R. and Á.A.F.-M.; writing and preparation of original draft: C.R.S.-R.; writing including review and editing: C.R.S.-R., J.A.M.-F., M.H., A.J.R.-M., and Á.A.F.-M.; visualization: J.A.M.-F.; supervision: Á.A.F.-M. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Silva-Ramos, C.R., Mejorano-Fonseca, J.A., Hidalgo, M. et al. Clinical, Epidemiological, and Laboratory Features of Mayaro Virus Infection: a Systematic Review. Curr Trop Med Rep 10, 309–319 (2023). https://doi.org/10.1007/s40475-023-00308-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40475-023-00308-6