
Abstract
Purpose of review
The purpose of this review is to provide a comprehensive update of literature published between January 2018 and April 2024, examining suicidal thoughts and behavior (STB) prevalence, risk factors, theoretical models, and interventions in autism.
Recent findings
We identified four recent meta-analyses and two systematic reviews. Pooled prevalence estimates in autism ranged from 34.2% for suicide ideation to 24.3% for suicide attempts. Autistic traits, interpersonal factors, and depressive symptoms were identified as STB risk factors, with elevated risk observed across the lifespan.
Summary
We included 80 studies examining STB in diagnosed autistic people or autistic traits in non-clinical samples. Autistic people were found to have an up to eightfold increased risk of death by suicide compared to non-autistic people, although reported rates varied considerably between studies; co-occurring mental health conditions, social, psychological, and cognitive factors exacerbated risk. Validated STB assessment tools and interventions for autistic people were notably scarce.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the 6 years following the publication of our initial review, Systematic Review of Suicide in Autism Spectrum Disorder: Current Trends and Implications [1], an increasing body of literature has demonstrated that individuals diagnosed with Autism Spectrum Disorder (ASD, henceforth autism, autistic peopleFootnote 1) are at significant increased risk of suicidal thoughts and behavior (STB), including premature death by suicide, relative to the general population [2,3,4]. In our 2018 review, we identified four systematic reviews and 13 research articles that met our inclusion criteria, all were published between 2012 and 2017. Six years on, we reflect on the progress of the field, new research findings, and remaining knowledge gaps.
Autism is an enduring neurodevelopmental condition occurring in about 1 in 100 people globally [5], and an estimated prevalence of 1 in 36 children in the United States (USA) [6]. Autism is characterized by differences in social communication and interaction styles, a range of sensory processing sensitivities, deep interests, and a preference for predictability and routine [7]. While autism is highly heterogeneous in presentation and functional impact [8, 9], co-occurring mental health conditions are common; an estimated 55% to 70% of autistic people experience at least one co-occurring condition, with many experiencing several conditions resulting in a complex clinical presentation [10, 11]. As observed in the general population, depression and anxiety are among the most prevalent co-occurring mental health diagnoses [12, 13], though the frequency with which autistic people experience these conditions is disproportionately high [14, 15]. The prevalence of co-occurring mental health conditions within the autistic population likely underpins the high rate of STB [15], although this is not to ignore the importance of environmental and autism specific risk factors, as well as barriers to healthcare access [16, 17].
Non-suicidal Self-injury (NSSI)
Given our focus on STB, as well as conceptual ambiguities outlined below, we excluded non-suicidal self-injury (NSSI) from our literature search. However, it is useful to provide a brief overview of NSSI, and the relationship between NSSI and STB. NSSI is a form of self-harm which includes socially unsanctioned and deliberate self-injury that, unlike a suicide attempt, is inflicted without intent to end life [18]. Research suggests up to 54% of autistic people experience NSSI in their lifetime [19, 20]. Despite historically being conceptualized as a repetitive or challenging behavior associated with the diagnostic criteria of autism––accounting for the presentation of some self-injurious behaviors––it is important to acknowledge that engagement in NSSI by autistic people is not dissimilar to non-autistic people in terms of age of onset, methods used, and functions (e.g., regulating affective states) [21,22,23]. NSSI represents one of the strongest risk factors for STB in the general population [24, 25], a finding replicated in autistic populations, particularly those who engage in specific types of NSSI (e.g., cutting) [26, 27]. There are debates in the wider literature about whether self-harm with suicidal intent (i.e., STB) is distinct from self-harm without suicidal intent (i.e., NSSI), or if these exist along a continuum [25, 28]. Both STB and NSSI, and the relationship between them, are currently poorly understood in autistic populations [29].
Published Systematic Reviews and Meta-analyses
We identified several recent (since 2018) systematic reviews and meta-analyses examining STB and autism. Four recent meta-analyses examined the prevalence of STB [3, 4, 30, 31] provided the most comprehensive analysis, including studies of autistic and possibly autistic individuals (identified as self-identified autism or high autistic traits) without a co-occurring intellectual disability (ID) (N = 36 studies, published 1992 to 2022, N = 48,186 individuals). They reported a pooled prevalence of 34.2%, 95% CI [27.9, 40.5] for suicidal ideation, 21.9% [13.4, 30.4] for suicide plans, and 24.3% [18.9, 29.6] for suicidal attempts and behavior, noting no significant differences in estimated prevalence of STB between autistic and possibly autistic individuals. Huntjens et al. [30] reported the pooled prevalence of suicide ideation and suicide attempts in autistic individuals (N = 52 studies published 1990–2022, N = 88,509 individuals). Lifetime rates of suicide ideation and suicide attempts were 37.2% [25.3, 50.8] and 15.3% [9.5, 23.6] respectively, with 12-month point estimates falling within these ranges (ideation = 25.4% [19.0, 33.2], attempts = 14.1% [7.4, 25.2]). However, they did not examine the impact of co-occurring psychiatric conditions, cognitive ability, or socioeconomic and environmental factors.
Other studies examined subsets of the autistic population. O’Halloran et al. [4] focused on autistic youth with and without a co-occurring ID (≤ 25 years; N = 29 studies, published prior to 2021, N = 34,011). Pooled prevalence estimates were lower in this age group, with 25.2%, 95% CI [18.2, 33.8] reporting suicide ideation, 8.3% [3.6, 18.2] reporting suicide attempts, and suicide deaths recorded in 0.2% [0.05, 0.52] of the pooled sample. Finally, Polidori et al. [31••] examined rates of suicide attempts among gender diverse autistic individuals (identified as gender incongruence or dysphoria; N = 6 studies, published prior to 2022, N = 65,456), reporting a pooled prevalence rate of 4.5% [4.35, 4.67]. Further, they highlighted that while gender diverse individuals were at the highest risk of suicide attempts relative to non-gender diverse controls, the combined impact of being autistic and gender-diverse compounded STB risk, with these individuals experiencing around threefold higher risk than non-autistic gender diverse individuals (OR = 2.99 [1.72, 5.21]).
Two systematic reviews included an exploration of predictors of STB in autistic adults. Mournet et al. [32] (N = 45 studies, published prior to 2022) found that interpersonal constructs aligned with the Interpersonal Theory of Suicide (IPTS) [33, 34], such as perceived burdensomeness and thwarted belongingness, were the most frequently studied risk factors for STB in autism, followed by the impact of depressive symptomology, and loneliness. Howe et al. [35] examined risk assessment tools used with autistic youth (≤ 21 years; N = 2 studies, published prior to 2019, N = 65). The authors identified no consistently used tools and it is furthermore notable that neither of the two measures identified in their review, Eskin’s Suicide Screening Questionnaire [36] and the Suicidal Ideation Questionnaire-JR (SIQ) [37], had been validated for use in autistic populations. Indeed, our own review (see also Newell et al.) [29] identified a lack of validated instruments for assessing STB within this population [1, 26].
Current Review
Our aim was to provide a comprehensive update of research concerning STB and autism since our previous review [1]. Given the surge in published studies, we kept the scope broad, focusing on the major themes and areas that have been the subject of investigation, the study sample (e.g., autistic participants vs studies of autistic traits within clinical or other non-autistic samples) and other primary demographics (e.g., age, sex/gender, intellectual ability), the type of autism and STB measures used, and to provide an overview of main findings and remaining gaps in knowledge.
Method
Search Strategy
In accordance with Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) [38] guidelines, we conducted a systematic literature search of the following databases, for articles published between January 1, 2018, and April 25, 2024: MEDLINE Complete, APA PsycInfo, CINAHL, Cochrane, and Scopus. Searches were conducted for studies involving (1) individuals formally diagnosed, suspected, or self-identified as autistic, and those with high levels of autistic traits, and (2) studies examining STB, including self-harm with suicidal intent, risk factors for STB, and death by suicide. Search terms for these areas are displayed in Table 1.
Eligibility Criteria
We limited our search to quantitative or qualitative peer-reviewed articles, published in English. No limits on participant age or proxy respondents (i.e., parents/carers) were applied. We excluded grey literature, studies involving a single case or animal model, and studies examining genetic or biological factors associated with STB. Our population of interest was autistic individuals, including those formally diagnosed in accordance with DSM (DSM-III through to current DSM-5-TR) or ICD [9, 10] criteria, self-identified autistic individuals or suspected autistic individuals. We also included studies with non-autistic samples where autistic traits had been assessed using common screening measures, i.e., autistic traits had been examined as a dimensional or transdiagnostic trait. No restrictions were applied for study setting (e.g., community, clinical, population based), or studies involving co-occurring conditions (e.g., mental illness, ID, gender dysphoria). The primary outcomes of interest were the presence or prevalence of STB, risk factors for STB, death by suicide, and theoretical models of STB. Where STB was not the primary outcome assessed, only findings relevant to the aims of the review were reported. No restrictions on measures of STB were applied (e.g., health records, self-report measures, standardized/non-standardized interviews or survey questions), though as previously indicated, we excluded studies that focused exclusively on NSSI (i.e., where no suicidal intent was established).
Study Selection and Data Extraction
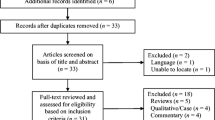
Electronic database searching was undertaken by the first author (C.M.B), returning a total of N = 2054 records (MEDLINE Complete, N = 426; APA PsycInfo, N = 317; CINAHL, N = 164; Cochrane, N = 97; Scopus, N = 1050). After removing duplicates (N = 827), two reviewers screened the remaining N = 1227 reports by title and abstract (C.M.B., E.S.). A further N = 1129 records were excluded as they did not meet our inclusion criteria (593 were not relevant, 209 review articles, 69 case studies, 66 editorials, 58 book chapters, 51 trial registrations, 23 dissertations, 22 conference proceedings, 16 comment/letter to the editor, 9 corrections to articles, 8 animal models, 2 non-English studies, 2 research briefs, and 1 non-peer reviewed article). Full-text review of all remaining articles was undertaken by all authors (C.M.B., V.N., E.S., D.H.), with any ambiguous articles discussed and consensus on whether to include or exclude reached as a group. Data extraction was completed and checked by a minimum of two authors using Covidence [39], which is a web-based software used to manage systematic review articles and data, according to predefined categories based on our previous review [1] and current aims. Figure 1 details the study selection process, and reasons for exclusions at each stage.

PRISMA Flow Diagram
Preprints
We identified a small number of preprints that are not included in the main review but nonetheless are likely to be of interest to readers. To source preprints, we contacted key researchers in the field (via email to international groups, and personally) and conducted a supplementary internet search. We found that while many researchers reported having new work under review, there were only a few that had provided access to their studies as preprints (i.e., prior to peer review). Identified preprints include a multinational study reporting suicidality in autistic children through to adults from the USA, Canada, and Australia [20], an investigation of the type and triggers for self-harming behaviors in young autistic people from the USA [40], an adapted suicide clinical interview codeveloped with and for autistic adults [41], a study examining depression, positive wellbeing and self-harm in autistic adults (note this paper has been now been published) [42], a multinational (United Kingdom [UK], Australia) investigation of the impact of gender and lifetime exposure to interpersonal stressors on STB risk [43], and a qualitative study with autistic adults with lived experience of STB concerning their access and use of healthcare services [17].
Results
Study Characteristics
The characteristics of included studies varied across several dimensions (Table 2).]Geographically, most studies were conducted in the UK (n = 26, 32.5%) and USA (n = 20, 25.0%), with other countries represented to lesser degrees, Canada (n = 6, 7.5%), Australia (n = 5, 6.3%), Netherlands (n = 5, 6.3%), Italy (n = 4, 5.0%), Taiwan (n = 4, 5.0%), and Sweden (n = 3, 3.8%). The remaining studies (n = 9, 11.3%) each arose from a different country. Total output was concentrated among a small number of researchers in the UK (Cassidy, S. A., n = 15, 18.8%; Baron-Cohen, S., n = 9, 11.3%; Rodgers, J., n = 7, 8.8%; Moseley R. L., n = 5, 6.3%) and Australia (Hedley, D., n = 5, 6.3%), while the USA involved a more dispersed range of contributors (see link for full bibliographic map: https://tinyurl.com/54a59428).
Sample characteristics also showed considerable variability between studies, with sample size ranging from N = 14–N = 145,929 participants. Most studies involved formally diagnosed autistic individuals (n = 63 studies, 78.8%), while others examined autistic traits in non-autistic samples (general population, n = 16 studies, 20.0%; other clinical samples, n = 8, 10.0%). Individuals with a co-occurring ID were explicitly excluded in 31.3% (n = 25) of studies and explicitly included in 22.5% (n = 18). Details of intellectual ability (i.e., intelligence quotient [IQ]) were not provided in most studies (n = 51, 63.8%). Just over half (n = 44, 55.0%) of included studies utilized a non-autistic comparison group.
With respect to sex and gender reporting, 46.3% (n = 37) of studies reported sex assigned at birth, 45.0% (n = 36) reported self-reported gender identity, 5.0% (n = 4) included both rates, and 5.0% (n = 4) of studies did not specify whether demographic categories corresponded to sex or gender identity. This was also the case for comparison and control groups.
Prevalence and Incidence of STB in Autism
We identified 27 studies (33.8%) reporting on the prevalence or incidence of STB. Of these, six (7.5%) utilized population or national registry data. Kõlves et al. [44] examined Danish national hospital and cause of death registries, demonstrating a threefold increased risk of suicide attempt (adjusted incidence rate ratio [aIRR] = 3.19; 95% CI [2.93, 3.46]) and suicide death (aIRR = 3.75 [2.85, 4.92]) in autistic compared to non-autistic people, after adjusting for sex, age, and time period. Risk was relatively higher in autistic females compared to autistic males (aIRR = 4.41 [3.74, 5.19]). Hirvikoski et al. [2] analyzed Swedish national patient and cause of death registers, finding autistic individuals without ID had an eightfold (without ADHD: odds ratio [OR] = 8.13 [6.23, 10.60]) to 13-fold (with ADHD: OR = 13.09 [8.54, 20.08]) risk of death by suicide, and autistic individuals with co-occurring ID had an overall threefold increased risk of suicide death (with ADHD: OR = 2.31 [1.16, 4.57]) compared to non-autistic people. Risk of STB was highest in autistic females with ADHD and without ID, compared to general population controls (OR = 13.42 [11.87,15.18]).
Using Finnish cause of death register data, Jokiranta-Olkoniemi et al. [45] found that risk of death by suicide for autistic individuals was double that of non-autistic people (unadjusted hazard ratio [HR] = 2.1 [1.02, 4.1]), though after adjusting for co-occurring psychiatric disorders, risk of intentional self-harm group differences between autistic and matched non-autistic controls were no longer statistically significant (adjusted HR = 0.8 [0.4, 1.6]). Utilizing health-care data from the Taiwanese population, Tsai et al. [46] found that autistic individuals had increased likelihood of suicide mortality (HR = 3.67 [2.37, 5.68]) compared to non-autistic individuals, and autistic males were more likely to die by suicide than non-autistic males (HR = 3.81 [2.37, 6.13]).
Using surveillance data from Utah (USA), Kirby et al. [47] reported that cumulative incidence rates of suicide death in autistic (0.17%) compared to non-autistic (0.11%) people differed significantly during the period 2013 to 2017 (relative risk [RR] = 1.56, 95% CI [1.08, 2.26]). This difference was attributed to deaths among autistic females, whose risk of suicide death was threefold that of non-autistic females (RR = 3.42 [1.63,7.20]). In two Canadian population-based cohorts, Lai et al. [48] did not find autism diagnosis was associated with suicide death but was independently associated with self-harm events (intent not specified) among both sexes after accounting for income, rurality, ID, and psychiatric diagnoses (females: RR = 1.83 [1.61, 2.08]; males: RR = 1.47 [1.28, 1.69]). Risk was higher for autistic versus non-autistic males (crude RR = 5.38 [4.29, 6.76]) and autistic versus non-autistic females (crude RR = 9.46 [7.83, 11.43]), whereas Lunsky et al. [49] found that over a period of 6-years, nine autistic adults (85/100,000) died by suicide, compared to six individuals with other developmental disabilities (57/100,000) and 33 without developmental disabilities (77/100,000).
Cuplin et al. [50] found no evidence of an association between autism diagnosis and STB using birth cohort data from the UK. However, children with social communication differences, a core feature of autism, had a higher relative risk of suicide attempts (RR = 2.14 [1.28, 3.58]), thoughts (RR = 1.42 [1.06, 1.91]) and plans (RR = 1.95 [1.09–3.47]). Using the National Pupil database of residents ages 11–17 years in the UK, Widnall et al. [51] reported an increased risk of self-harm (intent not specified) associated with autism diagnosis in males only (adjusted HR = 2.79, [1·40–5·57]).
In non-population-based samples that included formally diagnosed autistic individuals, prevalence of suicidal ideation varied from 9.6% when using parent reported outcomes for children [52] to 86% for lifetime estimates in autistic adult psychiatric outpatients [53]. Only one study separately reported prevalence of suicide plans (38.7%) [54]. Prevalence of suicide attempts or behavior was between 15% in autistic adults [54] and 45.5% in autistic prisoners [55]. Two studies which did not differentiate suicidal ideation from self-injury reported prevalence rates of 5.1% [56] and 14.6% [52], with the latter study reporting data for autistic children and youth.
Utilizing three epidemiologically ascertained samples of Korean children who either had an autism diagnosis or met cut-off criteria on an autism screening questionnaire, Bal et al. [57] reported that suicidal ideation was significantly higher in autistic (14%) and screen positive (16.6–27.4%) than screen negative (3.4–6.9%) children (OR: 2.87–5.67). Chaplin et al. [55] found that prisoners who scored above the cut-off for autistic traits on the AQ-20 (≥ 10) were more likely to report having attempted suicide in their life compared to neurotypical prisoners, 11.6% and 64.9% respectively. Similarly, Richards et al. [58] found that 40.6% of individuals with previous suicide attempts met the clinical cut-off on the AQ (≥ 26). In the UK and applying a checklist to coroners’ inquest records, Cassidy et al. [59] identified 10.8% of people who died by suicide over a 4-year period as having diagnosed autism or undiagnosed possible autism. Follow-up interviews with next of kin using validated autism screening and diagnostic tools identified “possible autism” in a total of 41.4% of individuals, although none met the threshold for autism on the Autism Diagnostic Interview, revised (ADI-R) [60].
Risk and Protective Factors
Very few studies (n = 3, 3.8%) explicitly explored protective factors for STB. Those that did included a qualitative examination of dog ownership [61], the impact of greater satisfaction with social support [62], and higher personal wellbeing [16]. By contrast, investigations of risk factors for STB were the most frequently identified study aim, with 58 studies identified overall (72.5%).
Results were mixed regarding the relationship between autistic traits and STB risk. While many studies found positive associations between higher overall autistic traits [57, 63,64,65,66,67], specific subdomains (e.g., social communication difficulties, restricted and repetitive behaviors) [50, 58, 68,69,70], or autism diagnosis and increased STB risk [26, 54, 57, 71,72,73], other studies found negative associations [52] or no significant relationship between autistic traits and STB [16, 50], highlighting the complexity of this relationship.
Psychological and cognitive factors were also salient. Mood disorders, particularly depression and anxiety, were associated with increased STB risk across multiple studies [57, 74, 75]. Other psychiatric conditions, including Borderline Personality Disorder, Bipolar Disorder, psychosis, and adjustment disorder also showed positive associations with elevated STB risk [54, 76,77,78,79]. However, findings on cognitive factors were more varied. Some studies associated higher cognitive ability with increased risk [80], while others found lower adaptive functioning or executive functioning difficulties [74] to be STB risk factors. Findings on cognitive tendencies such as rumination [68, 81], cognitive flexibility [82], perfectionism [83], and intolerance of uncertainty [84] were inconsistent across studies. Physiological factors were less frequently investigated, though shorter sleep duration and medical concerns were identified as STB risk factors in some studies [73, 85].
Emotional and behavioral concerns were also identified as STB risk factors. These included low self-esteem, higher alexithymia, adjustment disorder, emotion dysregulation, internalizing and externalizing problems, NSSI, lower levels of cognitive control, and camouflaging of autistic traits [52, 63, 68, 72, 79, 81, 86, 87]. Alcohol and substance misuse, and conduct problems, were also associated with increased STB risk [53, 85]. Social and environmental factors were not uniform across studies. Loneliness, bullying victimization, interpersonal conflicts, and unmet support needs were generally associated with higher STB risk [16, 62, 82, 84, 88, 89]. However, some found indirect associations, with depression symptoms mediating the relationship between loneliness, satisfaction with social support, and STB [62] while others found no significant relationship between social support and STB [27].
Sex/Gender Effects
Results from population-based cohort studies that examined sex and gender effects are reported above. Six studies (7.5%) examined sex and gender effects [46, 48, 49, 79, 90, 91], and one further study provided some limited information about sex or gender-based differences [92]. Two studies found that those who report suicide attempts were more likely to be male, and less likely to have engaged in treatment programs [79], and that males were more likely to present at emergency departments for self-harm (adjusted HR = 2.79, [1.40, 5.57]) (intent not specified) [51]. One study [90•] found that autistic adolescents had a higher rate of lifetime suicide ideation compared to non-autistic adolescents but did not identify any significant sex-based effects.
Theory Testing
Most of the 14 studies (n = 17.5%) that examined suicide theories explored the relationship of autism-related factors (i.e., traits, diagnosis) and components of the IPTS [33]. Findings were mixed, with some reporting that thwarted belongingness and perceived burdensomeness predicted self-harm [93], suicidal ideation [94, 95] and mediated the relationship between autistic traits and self-harm [93], suicidal ideation [70] and STB [96]. Others found significant associations only with thwarted belongingness [69] or perceived burdensomeness and acquired capability with STB [97], or significant associations between thwarted belongingness and perceived burdensomeness only in non-autistic adults [96], or that perceived burdensomeness and thwarted belonginess mediated the relationship between autistic traits and suicidal ideation but emotion dysregulation did not [70]. Specific risk factors such as anxiety, depression [67, 95] and NSSI [87] were also positively associated with Interpersonal Theory of Suicide factors and STB. Two studies examined the Integrated Volitional Model of Suicide (IMV), finding that defeat and entrapment mediated the relationship between autistic traits and lifetime STB [98], and that entrapment mediated the relationship between defeat and suicidal ideation but camouflaging and intolerance of uncertainty did not [84].
Measure Development and Validation
Five studies (6.3%) focused on the development or testing of STB assessment measures. Of these, two studies demonstrated measurement invariance when testing suicidality assessment tools such as the Suicide behaviors Questionnaire-Revised (SBQ-R) [26] and Interpersonal Needs Questionnaire, 10 item (INQ-10) [99] in autistic and non-autistic samples. Mournet et al. [100] however, did not find differences in the concordance of Ask Suicide Screening Questions (ASQ) and Self-Injurious Thoughts and Behaviors Interview, Self-Report (SITBI-SR) between autistic and non-autistic individuals. Two further studies developed and validated tools to assess STB specifically for autistic people; the Suicidal Behaviors Questionnaire-Autism Spectrum Conditions (SBQ-ASC) [101] and the Suicidal Ideation Attributes Scale, Modified (SIDAS-M) [102].
Intervention
Only three studies (3.75%) examined suicide prevention interventions. One study developed autism-adapted safety plans with autistic adults [103], one found dialectical behavior therapy (DBT) to be effective for reducing suicidal thoughts and behavior in autistic adults [104]. The third implemented universal suicide risk screening in pediatric clinics for neurodevelopmental disabilities [105], finding higher rates of STB risk in autistic children (38.5%) than in all other clinic attendees.
Discussion
In this systematic review we provided a comprehensive update on research related to suicidal thoughts and behavior (STB) and autism, published in the six years following our initial review [1]. We identified 80 studies that met our inclusion criteria, published between January 1, 2018 and April 25, 2024, representing a substantial increase in research interest compared to the 13 studies included in our original review. Our updated review encompassed studies focusing on clinical samples, as well as those employing dimensional or transdiagnostic approaches, examining relationships between STB and autistic traits in, or in addition to, clinical autistic samples. This broad approach allowed us to identify new research findings, areas in which substantial progress has been made, and remaining gaps in the literature.
Diversity in characteristics across the included studies reflects growth in the field, while highlighting areas where more standardized approaches could be beneficial. Inclusion of participants with a co-occurring ID, reporting of sex versus gender identity, and sample sizes varied widely. Most studies involved formally diagnosed autistic individuals, while others examined autistic traits as a dimensional or transdiagnostic risk factor for STB. Global spread of research output has also shifted substantially since our initial review, where the most prominent research hubs were the USA (n = 5 studies), Japan (n = 3 studies), and several other countries including the UK and Australia which each produced a single article each. Studies included in the present review by contrast, were primarily conducted in the UK (n = 26) and USA (n = 20), with substantial output from Canada (n = 6), Australia (n = 5), and the Netherlands (n = 5).
Prevalence/Incidence
Population and register-based studies demonstrated consistently elevated rates of STB in autistic individuals, both relative to the general population, and within subsets of the autistic population where additional risk factors were identified. The reviewed studies reported an increased risk of death by suicide among autistic people between two- and eightfold that of non-autistic individuals [2, 44, 45]. While autistic people with a co-occurring ID returned a lower overall risk, the rate was still mostly found to be higher relative to non-autistic people [2]. Specific populations at greater risk included psychiatric outpatients [53] and autistic prisoners [55]. Rates of STB were also elevated in children and adolescents [90], highlighting the need for a lifespan approach to preventing STB in the autistic population [52].
Risk & Protective Factors
Most included studies (77.5%) focused on exploring risk and protective factors for STB, though associations were complex and sometimes contradictory. Many studies reported a positive association between higher autistic traits or an autism diagnosis and suicidal ideation [50, 54, 57, 64]. However, some studies found negative associations [52] or no relationship [16]. This variability suggests a need for more nuanced research into the specific aspects of autism that may contribute to STB risk. Co-occurring mental health and neurodevelopmental conditions, particularly depression, anxiety, and ADHD, were also consistently identified as significant risk factors for STB [57, 74, 75]. Given the disproportionately high rates of mental health concerns experienced by autistic people [14, 15], this line of enquiry remains crucial for informing STB prevention approaches.
Social, cognitive, and behavioral factors also emerged as important contributors to STB risk. Some reflected social dynamics that autistic people frequently experience and underscore the importance of social support and inclusion for autistic individuals. These include loneliness [62, 106], bullying or peer victimization [82, 107], and camouflaging of autistic traits [84]. Other factors such as executive function difficulties, higher cognitive ability, lower adaptive functioning, and emotion dysregulation were also identified as STB risk factors [52, 63, 74, 80]. While each of these domains are reflective of autistic experiences, the high degree of heterogeneity in autism [8, 9] limits insight into how addressing these factors will reduce STB risk across individuals. As such, these areas warrant further investigation.
Theoretical Models of STB
We identified a growing subset of studies (n = 14) that tested established suicide theories in the context of autism, focusing primarily on the IPTS [33, 34], with some attention to the IMV model [108, 109]. Thwarted belongingness and perceived burdensomeness (IPTS) showed mixed relationships with STB, with some studies finding positive associations with STB [93, 94], while others found partial or no support for a relationship between these factors and STB [69, 96]. This variability suggests that while IPTS may offer insights into STB in autism, its applicability may not be universal across autistic experiences. Strikingly however, the salient role of relational and cognitive factors in STB appears to be frequently underrecognized. Jachyra et al. [89] reported that interpersonal conflicts and life transitions were frequently identified as precursors to STB by autistic adults (see also [43]), but that STB was not identified as a presenting problem in 50% of autistic adults arriving at the emergency department. Thus, while existing theories provide valuable frameworks, it’s possible they require modification to fully capture the unique experiences of autistic people, and the STB risk they may confer.
Measurement Development and Intervention
Despite our previous review identifying a lack of validated instruments for assessing STB within the autistic population [1], these areas received little research attention. The two available examples, the SBQ-ASC [101] and the SIDAS-M [102] (see also, pre-print) [41], which both represent adaptations to existing tools, were co-designed with autistic people, and thus better meet the communication and cognitive styles of this population. However, these tools need further validation studies, with larger and more diverse samples. Nonetheless, given the availability of modified or adapted tools for autistic people, we recommend these be incorporated into future research designs where it is appropriate to do so.
Strengths and Limitations
Strengths of this review include the broad selection criteria, wide range of study designs and populations, and our focus on both diagnosed autism and autistic traits. This comprehensive approach allowed us to capture the rapid growth in research over the past six years and provided a broad understanding of advancements in autism and STB research. However, the present review was not without limitations. Heterogeneity in study design, populations of interest, and the use of measures that have not been validated in autistic populations made direct comparisons challenging. Further, the predominance of cross-sectional study design (N = 51) limits our ability to draw causal inferences about risk factors for STB.
We identified notable geographic disparity in the distribution and methodology of included studies. Population and register-based studies were primarily conducted in Nordic countries (i.e., Denmark, Finland, Sweden) [2, 44, 45, 47,48,49, 56], highlighting the importance of establishing robust data systems and integrated healthcare records to facilitate these types of studies in other contexts. Non-Western regions were underrepresented (n = 6 studies), with four of the six included studies coming from Taiwan [46, 71, 82, 110]. Collectively, Asian studies provided some insight into cross-cultural differences, primarily reflecting different research priorities rather than differences in STB outcomes. For example, three studies from Taiwan and Hong Kong focused on interpersonal dynamics, specifically examining the role of family relationships and bullying [71, 110, 111]. However, the applicability of our findings to non-Western cultural contexts remains largely limited due to this lack of diverse representation.
Future Directions
Our review highlights several areas of ongoing need. Intervention studies represented a very small portion of the total number of included studies, highlighting a critical gap in the literature. Improved services and clearer pathways to support are crucial, as is greater involvement of autistic people through co-produced research (see pre-print) [17]. More longitudinal studies are needed to understand the developmental trajectories of suicidality in autism across the lifespan (see pre-print) [20]. Broader recognition of autistic people as a priority population in suicide prevention efforts, such as those recently announced in the UK government’s Suicide Prevention Strategy for England (2023–2028) [112], will be essential for promoting policy reform, increasing research funding opportunities, and greater resourcing within mental health systems across global contexts. Further investigation of intersectionality, including sex and gender differences, and co-occurring mental health conditions is needed given the potential for compounding STB risk factors [31, 113]. As is the urgent need for continued development and validation of autism-specific assessment tools (see pre-print) [41]. Finally, efforts to diversify the geographic spread of research could lead to a more globally representative understanding of STB in autism, while accounting for diverse cultural contexts and healthcare systems. Addressing these gaps will be crucial in developing more effective, targeted approaches to preventing and addressing STB in the autistic population.
Conclusion
The volume and scope of studies included in this review demonstrate that substantial progress has been made over the last six years [1]. Rigorous population-based investigations have allowed us to quantify the disproportionately high rate of STB and premature death by suicide faced by autistic people, while diverse explorations of STB correlates and risk factors provide essential insight into possible mechanisms for support. When reflecting on current approaches for identifying and preventing STB in autism, however, the existing body of literature is notably less developed. While some promising examples of autism-specific screening measures [101, 102], and interventions for STB [52, 41, 103, 114], advancements in these domains must be prioritized going forward. It is imperative that researchers, clinicians, and policymakers collaborate to build upon these foundations, developing and validating more autism-specific STB prevention and intervention strategies to ultimately improve outcomes and quality of life for autistic individuals at risk of suicide.
Data Availability
No datasets were generated or analysed during the current study.
Notes
In accordance with community preferences, this article uses identity first language, e.g., autistic person, autistic traits (Bury et al., 2023).
References
Hedley D, Uljarević M. Systematic review of suicide in autism spectrum disorder: current trends and implications. Curr Devel Disord Rep. 2018;5:65–76. https://doi.org/10.1007/s40474-018-0133-6.
Hirvikoski T, Boman M, Chen Q, D’Onofrio BM, Mittendorfer-Rutz E, Lichtenstein P, Bölte S, Larsson H. Individual risk and familial liability for suicide attempt and suicide in autism: a population-based study. Psychol Med. 2020;50(9):1463–74. https://doi.org/10.1017/S0033291719001405.
Newell V, Phillips L, Jones C, Townsend E, Richards C, Cassidy S. A systematic review and meta-analysis of suicidality in autistic and possibly autistic people without co-occurring intellectual disability. Mol Autism. 2023;14(1):12. https://doi.org/10.1186/s13229-023-00544-7.
O’Halloran L, Coey P, Wilson C. Suicidality in autistic youth: A systematic review and meta-analysis. Clin Psychol Rev. 2022;93:102144. https://doi.org/10.1016/j.cpr.2022.102144.
Zeidan J, Fombonne E, Scorah J, Ibrahim A, Durkin MS, Saxena S, Yusuf A, Shih A, Elsabbagh M. Global prevalence of autism: A systematic review update. Autism Res. 2022;15(5):778–90. https://doi.org/10.1002/aur.2696.
Maenner MJ. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2020. MMWR Surveill Summs. 2023;72. https://doi.org/10.15585/mmwr.ss7202a1.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed., text rev.) 2022. https://doi.org/10.1176/appi.books.9780890425787.
Lombardo MV, Lai MC, Baron-Cohen S. Big data approaches to decomposing heterogeneity across the autism spectrum. Mol Psychiatry. 2019;24(10):1435–50. https://doi.org/10.1038/s41380-018-0321-0.
Lord C. Recognising the heterogeneity of autism. Lancet Psychiatry. 2019;6(7):551–2. https://doi.org/10.1016/S2215-0366(19)30220-2.
Hossain MM, Khan N, Sultana A, Ma P, McKyer ELJ, Ahmed HU, Purohit N. Prevalence of comorbid psychiatric disorders among people with autism spectrum disorder: An umbrella review of systematic reviews and meta-analyses. Psychiatry Res. 2020;287:112922. https://doi.org/10.1016/j.psychres.2020.112922.
Lugo-Marin J, Magan-Maganto M, Rivero-Santana A, Cuellar-Pompa L, Alviani M, Jenaro-Rio C, Diez E, Canal-Bedia R. Prevalence of psychiatric disorders in adults with autism spectrum disorder: A systematic review and meta-analysis. Res in Autism Spectr Disord. 2019;59:22–33. https://doi.org/10.1016/j.rasd.2018.12.004.
Moreno-Agostino D, Wu YT, Daskalopoulou C, Hasan MT, Huisman M, Prina M. Global trends in the prevalence and incidence of depression: a systematic review and meta-analysis. J Affect Disord. 2021;281:235–43. https://doi.org/10.1016/j.jad.2020.12.035.
Yang X, Fang Y, Chen H, Zhang T, Yin X, Man J, Yang L, Lu M. Global, regional and national burden of anxiety disorders from 1990 to 2019: results from the Global Burden of Disease Study 2019. Epidemiol Psychiatr Sci. 2021;30:e36. https://doi.org/10.1017/S2045796021000275.
Hollocks MJ, Lerh JW, Magiati I, Meiser-Stedman R, Brugha TS. Anxiety and depression in adults with autism spectrum disorder: a systematic review and meta-analysis. Psychol Med. 2019;49(4):559–72. https://doi.org/10.1017/S0033291718002283.
Lai MC, Kassee C, Besney R, Bonato S, Hull L, Mandy W, Szatmari P, Ameis SH. Prevalence of co-occurring mental health diagnoses in the autism population: a systematic review and meta-analysis. Lancet Psychiatry. 2019;6(10):819–29. https://doi.org/10.1016/S2215-0366(19)30289-5.
Hedley D, Uljarevic M, Foley KR, Richdale A, Trollor J. Risk and protective factors underlying depression and suicidal ideation in Autism Spectrum Disorder. Depress Anxiety. 2018;35(7):648–57. https://doi.org/10.1002/da.22759.
Wilson J, Brown CM, Hayward SM, Stokes MA, Nicholas DB. Autistic adults' experiences seeking and receiving support for mental health and suicidality. OSF Preprints; 2024. Available from: https://doi.org/10.31219/osf.io/y27pz.
Nock MK, Favazza AR. Nonsuicidal self-injury: Definition and classification. In Nock MK, editor. Understanding nonsuicidal self-injury: Origins, assessment, and treatment. Am Psychol Assoc. 2009;9–18. https://doi.org/10.1037/11875-001.
Maddox BB, Trubanova A, White SW. Untended wounds: Non-suicidal self-injury in adults with autism spectrum disorder. Autism. 2017;21(4):412–22. https://doi.org/10.1177/1362361316644731.
Schwartzman J, McMorris CA, Williams ZJ, Brown CM, Trollor JN, Uljarević M, Stokes MA, Hedley D. Elevated suicidal thoughts and behaviors and self-injury in autism across the lifespan: A multinational study. Research Gate preprints; 2024. Available from: https://doi.org/10.13140/RG.2.2.11256.66568
Duerden EG, Oatley HK, Mak-Fan KM, McGrath PA, Taylor MJ, Szatmari P, Roberts SW. Risk factors associated with self-injurious behaviors in children and adolescents with autism spectrum disorders. J Autism Dev Disord. 2012;42:2460–70. https://doi.org/10.1007/s10803-012-1497-9.
South M, Ozonoff S, McMahon WM. Repetitive behavior profiles in Asperger syndrome and high-functioning autism. J Autism Dev Disord. 2005;35:145–58. https://doi.org/10.1007/s10803-004-1992-8.
Moseley R, Gregory NJ, Smith P, Allison C, Baron-Cohen S. A ‘choice’, an ‘addiction’, a way ‘out of the lost’: exploring self-injury in autistic people without intellectual disability. Mol Autism. 2019;10:1–23. https://doi.org/10.1186/s13229-019-0267-3.
Favril L, Yu R, Uyar A, Sharpe M, Fazel S. Risk factors for suicide in adults: systematic review and meta-analysis of psychological autopsy studies. BMJ Ment Health. 2022;25(4):148–55. https://doi.org/10.1136/ebmental-2022-300549.
Hawton K, Bale L, Brand F, Townsend E, Ness J, Waters K, Clements C, Kapur N, Geulayov G. Mortality in children and adolescents following presentation to hospital after non-fatal self-harm in the multicentre study of self-harm: a prospective observational cohort study. Lancet Child Adolesc Health. 2020;4(2):111–20. https://doi.org/10.1016/S2352-4642(19)30373-6.
Cassidy S, Bradley L, Shaw R, Baron-Cohen S. Risk markers for suicidality in autistic adults. Mol Autism. 2018;9:42. https://doi.org/10.1186/s13229-018-0226-4.
Moseley RL, Gregory NJ, Smith P, Allison C, Baron-Cohen S. Links between self-injury and suicidality in autism. Mol Autism. 2020;11:1–5. https://doi.org/10.1186/s13229-020-0319-8.
Kapur N, Cooper J, O’Connor RC, Hawton K. Non-suicidal self-injury v. attempted suicide: new diagnosis or false dichotomy? Br J Psychiatry. 2013;202(5):326-8.29. https://doi.org/10.1192/bjp.bp.112.116111.
Newell V, Townsend E, Richards C, Cassidy S. Measurement properties of tools used to assess self-harm in autistic and general population adults. Clin Psychol Rev. 2024:102412. https://doi.org/10.1016/j.cpr.2024.102412
Huntjens A, Landlust A, Wissenburg S, van der Gaag M. The prevalence of suicidal behavior in autism spectrum disorder: A meta-analysis. CRISIS. 2024;1;45(2). https://psycnet.apa.org/doi/10.1027/0227-5910/a000922
Polidori L, Sarli G, Berardelli I, Pompili M, Baldessarini RJ. Risk of suicide attempt with gender diversity and neurodiversity. Psychiatry Res. 2023:115632. https://doi.org/10.1016/j.psychres.2023.115632
Mournet AM, Wilkinson E, Bal VH, Kleiman EM. A systematic review of predictors of suicidal thoughts and behaviors among autistic adults: Making the case for the role of social connection as a protective factor. Clin Psychol Rev. 2023;99:102235. https://doi.org/10.1016/j.cpr.2022.102235.
Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, Joiner TE Jr. The interpersonal theory of suicide. Psychol Rev. 2010;117(2):575. https://doi.org/10.1037/a0018697.
Joiner T. Why people die by suicide: Harvard University Press; 2005.
Howe SJ, Hewitt K, Baraskewich J, Cassidy S, McMorris CA. Suicidality among children and youth with and without autism spectrum disorder: a systematic review of existing risk assessment tools. J Autism Dev Disord. 2020;50:3462–76. https://doi.org/10.1007/s10803-020-04394-7.
Eskin M. Suicidal behavior as related to social support and assertiveness among Swedish and Turkish high school students: A cross-cultural investigation. J Clin Psychol. 1995;51(2):158–72. https://doi.org/10.1002/1097-4679(199503)51:23C158::aid-jclp22705102043E3.0.co;2-h.
Reynolds WM, Mazza JJ. Assessment of suicidal ideation in inner-city children and young adolescents: Reliability and validity of the Suicidal Ideation Questionnaire-JR. School Psychol Rev. 1999;28(1):17–30. https://doi.org/10.1080/02796015.1999.12085945.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;29:372. https://doi.org/10.1136/bmj.n71.
Innovation VH. Covidence Systematic Review Software Melbourne, Australia. 2024
Schwartzman J, Rubin A, Fox K, Hedley D, Bettis A. Understanding the type, content, and triggers for self-injurious thoughts and behaviors in autistic youth and their disclosure to caregivers. Research Gate Preprints; 2024. Available from: https://doi.org/10.13140/RG.2.2.23128.10243
Hedley D, Williams ZJ, Deady M, Batterham P, Bury S, Brown CM, et al. The Suicide Assessment Kit-Modified Interview (SAK-MI): Development and Validation of a Modified Clinical Interview for the Assessment of Suicidal Thoughts and Behavior in Autistic Adults. OSF Preprints; 2024. Available from: https://doi.org/10.31219/osf.io/xqd9b
Hedley D, Uljarević M, Bury SM, Haschek A, Richdale AL, Trollor JN, Stokes MA. Examination of the potential moderating role of psychological wellbeing in the relationship between depression and thoughts of self-harm in autistic adolescents and adults: A two-year longitudinal study. J Autism Dev Disord. 2024;30:1–13. https://doi.org/10.1007/s10803-024-06489-x.
Moseley R, Hedley D, Gamble-Turner J, Uljarevic M, Bury S, Shields G, et al. Lifetime stressor exposure and suicidality in autistic adults: a multinational study examining the role of gender in interpersonal life stress. OSF Preprints; 2024. Available from: https://doi.org/10.31219/osf.io/ytpks
Kõlves K, Fitzgerald C, Nordentoft M, Wood SJ, Erlangsen A. Assessment of suicidal behaviors among individuals with autism spectrum disorder in Denmark. JAMA Netw Open. 2021;4(1):e2033565-e. https://doi.org/10.1001/jamanetworkopen.2020.33565.
Jokiranta-Olkoniemi E, Gyllenberg D, Sucksdorff D, Suominen A, Kronstrom K, Chudal R, Sourander A. Risk for premature mortality and intentional self-harm in autism spectrum disorders. J Autism Dev Disord. 2021;51(9):3098–108. https://doi.org/10.1007/s10803-020-04768-x.
Tsai SJ, Chang WH, Cheng CM, Liang CS, Bai YM, Hsu JW, Huang KL, Su TP, Chen TJ, Chen MH. All-cause mortality and suicide mortality in autistic individuals: An entire population longitudinal study in Taiwan. Autism. 2023;27(8):2496–506. https://doi.org/10.1177/13623613231167287.
Kirby AV, Bakian AV, Zhang Y, Bilder DA, Keeshin BR, Coon H. A 20-year study of suicide death in a statewide autism population. Autism Res. 2019;12(4):658–66. https://doi.org/10.1002/aur.2076.
Lai MC, Saunders NR, Huang A, Artani A, Wilton AS, Zaheer J, Ameis SH, Brown HK, Lunsky Y. Self-harm events and suicide deaths among autistic individuals in Ontario, Canada. JAMA Netw Open. 2023;6(8):e2327415. https://doi.org/10.1001/jamanetworkopen.2023.27415.
Lunsky Y, Lai MC, Balogh R, Chung H, Durbin A, Jachyra P, Tint A, Weiss J, Lin E. Premature mortality in a population-based cohort of autistic adults in Canada. Autism Res. 2022;15(8):1550–9. https://doi.org/10.1002/aur.2741.
Culpin I, Mars B, Pearson RM, Golding J, Heron J, Bubak I, Carpenter P, Magnusson C, Gunnell D, Rai D. Autistic traits and suicidal thoughts, plans, and self-harm in late adolescence: population-based cohort study. J Am Acad Child Adolesc Psychiatry. 2018;57(5):313-20.e6. https://doi.org/10.1016/j.jaac.2018.01.023.
Widnall E, Epstein S, Polling C, Velupillai S, Jewell A, Dutta R, Simonoff E, Stewart R, Gilbert R, Ford T, Hotopf M. Autism spectrum disorders as a risk factor for adolescent self-harm: a retrospective cohort study of 113,286 young people in the UK. BMC Med. 2022;20(1). https://doi.org/10.1186/s12916-022-02329-w
Hunsche MC, Saqui S, Mirenda P, Zaidman-Zait A, Bennett T, Duku E, Elsabbagh M, Georgiades S, Smith IM, Szatmari P, Ungar WJ. Parent-reported rates and clinical correlates of suicidality in children with autism spectrum disorder: A longitudinal study. J Autism Dev Disord. 2020;50:3496–509. https://doi.org/10.1007/s10803-020-04373-y.
Nyrenius J, Waern M, Eberhard J, Ghaziuddin M, Gillberg C, Billstedt E. Autism in adult psychiatric out-patients: self-reported suicidal ideation, suicide attempts and non-suicidal self-injury. BJPsych Open. 2023;9(5). https://doi.org/10.1192/bjo.2023.553
Bentum JV, Sijbrandij M, Huibers M, Begeer S. Occurrence and predictors of lifetime suicidality and suicidal ideation in autistic adults. Autism. 2024:13623613231225901. https://doi.org/10.1177/13623613231225901
Chaplin E, McCarthy J, Allely CS, Forrester A, Underwood L, Hayward H, Sabet J, Young S, Mills R, Asherson P, Murphy D. Self-harm and mental health characteristics of prisoners with elevated rates of autistic traits. Res Dev Disabil. 2021;114:103987. https://doi.org/10.1016/j.ridd.2021.103987.
Cervantes PE, Li A, Sullivan KA, Seag DEM, Baroni A, Horwitz SM. Assessing and managing suicide risk in autistic youth: findings from a clinician survey in a pediatric psychiatric emergency setting. J Autism Dev Disord. 2023;53(5):1755–63. https://doi.org/10.1007/s10803-022-05448-8.
Bal VH, Leventhal BL, Carter G, Kim H, Koh YJ, Ha M, Kwon HJ, Hong P, Kim YS. Parent-reported suicidal ideation in three population-based samples of school-aged Korean children with autism spectrum disorder and autism spectrum screening questionnaire screen positivity. Arch Suicide Res. 2022;26(3):1232–49. https://doi.org/10.1080/13811118.2020.1868367.
Richards G, Kenny R, Griffiths S, Allison C, Mosse D, Holt R, O’Connor RC, Cassidy S, Baron-Cohen S. Autistic traits in adults who have attempted suicide. Mol Autism. 2019;10(1). https://doi.org/10.1186/s13229-019-0274-4
Cassidy S, Au-Yeung S, Robertson A, Cogger-Ward H, Richards G, Allison C, Bradley L, Kenny R, O’Connor R, Mosse D, Rodgers J. Autism and autistic traits in those who died by suicide in England. Br J Psychiatry. 2022;221(5):683–91. https://doi.org/10.1192/bjp.2022.21.
Rutter M, Le Couteur A, Lord C. Autism diagnostic interview-revised. Los Angeles, CA: Western Psychological Services. 2003;29(2003):30.
Barcelos AM, Kargas N, Packham C, Mills DS. Understanding the impact of dog ownership on autistic adults: implications for mental health and suicide prevention. Sci. 2021;11(1):23655. https://doi.org/10.1038/s41598-021-02504-8.
Hedley D, Uljarević M, Wilmot M, Richdale A, Dissanayake C. Understanding depression and thoughts of self-harm in autism: A potential mechanism involving loneliness. Res Autism Spectr Disord. 2018;46:1–7. https://doi.org/10.1016/j.rasd.2017.11.003.
Conner CM, Golt J, Righi G, Shaffer R, Siegel M, Mazefsky CA. A comparative study of suicidality and its association with emotion regulation impairment in large ASD and US census-matched samples. J Autism Dev Disord. 2020;50(10):3545–60. https://doi.org/10.1007/s10803-020-04370-1.
Dell’Osso L, Carpita B, Muti D, Morelli V, Salarpi GI, Salerni AN, Scotto J, Massimetti G, Gesi C, Ballerio M, Signorelli MS. Mood symptoms and suicidality across the autism spectrum. Compr Psychiatry. 2019;91:34–8. https://doi.org/10.1016/j.comppsych.2019.03.004.
Giannouchos TV, Beverly J, Christodoulou I, Callaghan T. Suicide and non-fatal self-injury-related emergency department visits among individuals with autism spectrum disorder. Autism. 2023;27(7):1983–96. https://doi.org/10.1177/13623613221150089.
Moses T. Suicide attempts among adolescents with self-reported disabilities. Child Psychiatry Hum Dev. 2018;49(3):420–33. https://doi.org/10.1007/s10578-017-0761-9.
Pelton MK, Crawford H, Bul K, Robertson AE, Adams J, De Beurs D, Rodgers J, Baron-Cohen S, Cassidy S. The role of anxiety and depression in suicidal thoughts for autistic and non-autistic people: A theory-driven network analysis. Suicide Life Threat Behav. 2023;53(3):426–42. https://doi.org/10.1111/sltb.12954.
Hedley D, Uljarević M, Cai RY, Bury SM, Stokes MA, Evans DW. Domains of the autism phenotype, cognitive control, and rumination as transdiagnostic predictors of DSM-5 suicide risk. PLoS ONE. 2021;16(1):e0245562. https://doi.org/10.1371/journal.pone.0245562.
Smith AR, Hunt RA, Grunewald W, Jeon ME, Stanley IH, Levinson CA, Joiner TE. Identifying central symptoms and bridge pathways between autism spectrum disorder traits and suicidality within an active duty sample. Arch Suicide Res. 2023;27(2):307–22. https://doi.org/10.1080/13811118.2021.1993398.
Stanley IH, Day TN, Gallyer AJ, Shelef L, Kalla C, Gutierrez PM, Joiner TE. Autism-related traits and suicide risk among active duty US military service members. Psychological services. 2021;18(3):377. https://psycnet.apa.org/doi/https://doi.org/10.1037/ser0000418
Chen YY, Chen YL, Gau SSF. Suicidality in children with elevated autistic traits. Autism Res. 2020;13(10):1811–21. https://doi.org/10.1002/aur.2333.
Costa AP, Loor C, Steffgen G. Suicidality in adults with autism spectrum disorder: the role of depressive symptomatology, alexithymia, and antidepressants. J Autism Dev Disord. 2020;50(10):3585–97. https://doi.org/10.1007/s10803-020-04433-3.
Hochard KD, Pendrous R, Mari T, Flynn S. Examining the relationship between autism traits and sleep duration as predictors of suicidality. J Autism Dev Disord. 2020;50(10):3575–84. https://doi.org/10.1007/s10803-020-04405-7.
Cook ML, Tomaszewski B, Lamarche E, Bowman K, Klein CB, Stahl S, Klinger LG. Suicide risk in transition-aged autistic youth: The link among executive function, depression, and autistic traits. Autism. 2024:13623613241227983. https://doi.org/10.1177/13623613241227983
Hedley D, Hayward SM, Denney K, Uljarević M, Bury S, Sahin E, Brown CM, Clapperton A, Dissanayake C, Robinson J, Trollor J. The association between COVID-19, personal wellbeing, depression, and suicide risk factors in Australian autistic adults. Autism Res. 2021;14(12):2663–76. https://doi.org/10.1002/aur.2614.
Chabrol H, Raynal P. The co-occurrence of autistic traits and borderline personality disorder traits is associated to increased suicidal ideation in nonclinical young adults. Compr Psychiatry. 2018;82:141–3. https://doi.org/10.1016/j.comppsych.2018.02.006.
Dell’Osso L, Cremone IM, Amatori G, Cappelli A, Cuomo A, Barlati S, Massimetti G, Vita A, Fagiolini A, Carmassi C, Carpita B. Investigating the relationship between autistic traits, ruminative thinking, and suicidality in a clinical sample of subjects with bipolar disorder and borderline personality disorder. Brain Sci. 2021;11(5):621. https://doi.org/10.3390/brainsci11050621.
Holden R, Mueller J, McGowan J, Sanyal J, Kikoler M, Simonoff E, Velupillai S, Downs J. Investigating bullying as a predictor of suicidality in a clinical sample of adolescents with autism spectrum disorder. Autism Res. 2020;13(6):988–97. https://doi.org/10.1002/aur.2292.
Mikami K, Inomata S, Onishi Y, Orihashi Y, Yamamoto K, Matsumoto H. Gender differences in the suicide attempts of adolescents in emergency departments: Focusing on individuals with autism spectrum disorder. Adolesc Psychiatry. 2019;9(3):232–40. https://doi.org/10.2174/2210676609666190617144453.
Casten LG, Thomas TR, Doobay AF, Foley-Nicpon M, Kramer S, Nickl-Jockschat T, Abel T, Assouline S, Michaelson JJ. The combination of autism and exceptional cognitive ability is associated with suicidal ideation. Neurobiol Learn Mem. 2023;197:107698. https://doi.org/10.1016/j.nlm.2022.107698.
Arwert TG, Sizoo BB. Self-reported suicidality in male and female adults with autism spectrum disorders: rumination and self-esteem. J Autism Dev Disord. 2020;50(10):3598–605. https://doi.org/10.1007/s10803-020-04372-z.
Chang JC, Lai MC, Chang SS, Gau SS. Factors mediating pre-existing autism diagnosis and later suicidal thoughts and behaviors: A follow-up cohort study. Autism. 2024;30:13623613231223626. https://doi.org/10.1177/13623613231223626.
Ellison KS, Jarzabek E, Jackson SL, Naples A, McPartland JC. Brief report: exploratory evaluation of clinical features associated with suicidal ideation in youth with autism spectrum disorder. J Autism Dev Disord. 2024;54(2):803–10.
Graham J, Rodgers J, Cassidy S. Why Are Autistic People More Likely to Experience Suicidal Thoughts? Applying the Integrated Motivational-Volitional Model with Autistic Adults. Autism in Adulthood. 2023. https://doi.org/10.1089/aut.2023.0039.
McDonnell CG, DeLucia EA, Hayden EP, Anagnostou E, Nicolson R, Kelley E, Georgiades S, Liu X, Stevenson RA. An exploratory analysis of predictors of youth suicide-related behaviors in autism spectrum disorder: Implications for prevention science. J Autism Dev Disord. 2020;50(10):3531–44. https://doi.org/10.1007/s10803-019-04320-6.
Masi G, Scullin S, Narzisi A, Muratori P, Paciello M, Fabiani D, Lenzi F, Mucci M, D’Acunto G. Suicidal ideation and suicidal attempts in referred adolescents with high functioning autism spectrum disorder and comorbid bipolar disorder: A pilot study. Brain Sci. 2020;10(10):750. https://doi.org/10.3390/brainsci10100750.
Moseley RL, Gregory NJ, Smith P, Allison C, Cassidy S, Baron-Cohen S. Non-suicidal self-injury and its relation to suicide through acquired capability: investigating this causal mechanism in a mainly late-diagnosed autistic sample. Mol Autism. 2022;13(1):45. https://doi.org/10.1186/s13229-022-00522-5.
Camm-Crosbie L, Bradley L, Shaw R, Baron-Cohen S, Cassidy S. “People like me don’t get support”: Autistic adults’ experiences of support and treatment for mental health difficulties, self-injury and suicidality. Autism. 2019;23(6):1431–41. https://doi.org/10.1177/1362361318816053.
Jachyra P, Lai M-C, Zaheer J, Fernandes N, Dale M, Sawyer A, Lunsky Y. Suicidal thoughts and behaviours among autistic adults presenting to the psychiatric emergency department: An exploratory chart review. J Autism Dev Disord. 2022;52(5):2367–75. https://doi.org/10.1007/s10803-021-05102-9.
Schwartzman JM, Muscatello RA, Corbett BA. Assessing suicidal thoughts and behaviors and nonsuicidal self-injury in autistic and non-autistic early adolescents using the Columbia Suicide Severity Rating Scale. Autism. 2023;27(8):2310–23. https://doi.org/10.1177/13623613231162154.
Wijnhoven LA, Niels-Kessels H, Creemers DH, Vermulst AA, Otten R, Engels RC. Prevalence of comorbid depressive symptoms and suicidal ideation in children with autism spectrum disorder and elevated anxiety symptoms. J Child Adolesc Ment Health. 2019Jan 2;31(1):77–84. https://doi.org/10.2989/17280583.2019.1608830.
Orm S, Wood J, Corbett B, Fjermestad K. suicidal risk behaviors in adolescents with rare neurodevelopmental disorders: the role of sex, autistic traits, and mental health difficulties. J Pediatr Psychol. 2023;48(10):852–60. https://doi.org/10.1093/jpepsy/jsad051.
Aral A, Usta MB, Aral AE. Autistic traits and self-harm in adolescents: a study on interpersonal psychological theory of suicide. Egypt J Neurol Psych. 2023;59(1). https://doi.org/10.1186/s41983-023-00658-y
Cassidy SA, Gould K, Townsend E, Pelton M, Robertson AE, Rodgers J. Is camouflaging autistic traits associated with suicidal thoughts and behaviours? Expanding the interpersonal psychological theory of suicide in an undergraduate student sample. J Autism Dev Disord. 2019;50(10):3638–48. https://doi.org/10.1007/s10803-019-04323-3.
Dow D, Morgan L, Hooker JL, Michaels MS, Joiner TE, Woods J, Wetherby AM. Anxiety, depression, and the interpersonal theory of suicide in a community sample of adults with autism spectrum disorder. Arch Suicide Res. 2021;25(2):297–314. https://doi.org/10.1080/13811118.2019.1678537.
Pelton MK, Crawford H, Robertson AE, Rodgers J, Baron-Cohen S, Cassidy S. Understanding suicide risk in autistic adults: Comparing the interpersonal theory of suicide in autistic and non-autistic samples. J Autism Dev Disord. 2020;50:3620–37. https://doi.org/10.1007/s10803-020-04393-8.
Moseley RL, Gregory NJ, Smith P, Allison C, Cassidy S, Baron-Cohen S. The relevance of the interpersonal theory of suicide for predicting past-year and lifetime suicidality in autistic adults. Mol Autism. 2022;13(1):14. https://doi.org/10.1186/s13229-022-00495-5.
Cassidy S, McLaughlin E, McGranaghan R, Pelton M, O’Connor R, Rodgers J. Is camouflaging autistic traits associated with defeat, entrapment, and lifetime suicidal thoughts? Expanding the Integrated Motivational Volitional Model of Suicide. Suicide Life Threat Behav. 2023;53(4):572–85. https://doi.org/10.1111/sltb.12965.
Pelton MK, Crawford H, Robertson AE, Rodgers J, Baron-Cohen S, Cassidy S. A measurement invariance analysis of the Interpersonal Needs Questionnaire and Acquired Capability for Suicide Scale in autistic and non-autistic adults. Autism Adulthood. 2020;2(3):193–203. https://doi.org/10.1089/aut.2019.0055.
Mournet AM, Bal VH, Kleiman EM. concordance between the Ask Suicide Screening Questions (ASQ) and Self-Injurious Thoughts and Behaviors Interview-Self Report (SITBI-SR) among autistic and non-autistic adults. Arch Suicide Res. 2023;1–2. https://doi.org/10.1080/13811118.2023.2252027
Cassidy SA, Bradley L, Cogger-Ward H, Rodgers J. Development and validation of the suicidal behaviours questionnaire - autism spectrum conditions in a community sample of autistic, possibly autistic and non-autistic adults. Mol Autism. 2021;12(1):46. https://doi.org/10.1186/s13229-021-00449-3.
Hedley D, Batterham PJ, Bury SM, Clapperton A, Denney K, Dissanayake C, Fox P, Frazier TW, Gallagher E, Hayward SM, Robinson J. The Suicidal Ideation Attributes Scale-Modified (SIDAS-M): Development and preliminary validation of a new scale for the measurement of suicidal ideation in autistic adults. Autism. 2023;27(4):1115–31. https://doi.org/10.1177/13623613221131234.
Goodwin J, Gordon I, O’Keeffe S, Carling S, Berresford A, Bhattarai N, Heslop P, Nielsen E, O’Connor RC, Ogundimu E, Pelton M. Adapting Safety Plans for Autistic Adults with Involvement from the Autism Community. Autism Adulthood. 2024. https://doi.org/10.1089/aut.2023.0124.
Huntjens A, Van Den Bosch Wies LMC, Sizoo B, Kerkhof A, Smit F, Van Der Gaag M. The effectiveness and safety of dialectical behavior therapy for suicidal ideation and behavior in autistic adults: A pragmatic randomized controlled trial. Psychol Med. 2024. https://doi.org/10.1017/S0033291724000825.
Rybczynski S, Ryan TC, Wilcox HC, Van Eck K, Cwik M, Vasa RA, Findling RL, Slifer K, Kleiner D, Lipkin PH. Suicide risk screening in pediatric outpatient neurodevelopmental disabilities clinics. J Dev Behav Pediatr. 2022May 1;43(4):181–7. https://doi.org/10.1097/DBP.0000000000001026.
La Buissonniere AV, Schneider SC, Cepeda SL, Wood JJ, Kendall PC, Small BJ, Wood KS, Kerns C, Saxena K, Storch EA. Predictors of suicidal thoughts in children with autism spectrum disorder and anxiety or obsessive-compulsive disorder: The unique contribution of externalizing behaviors. Child Psychiatry Hum Dev. 2022;53(2):223–36. https://doi.org/10.1007/s10578-020-01114-1.
Shtayermman O. A brief report on suicidal ideation in adolescents diagnosed with Asperger Syndrome. Adv Neurodev Disord. 2020;4(1):46–50. https://doi.org/10.1007/s41252-019-00142-w.
O'Connor RC, Cleare S, Eschle S, Wetherall K, Kirtley OJ. The integrated motivational‐volitional model of suicidal behavior: An update. The international handbook of suicide prevention. 2016:220–40. https://doi.org/10.1002/9781118903223.ch13
O’Connor RC, Kirtley OJ. The integrated motivational–volitional model of suicidal behaviour. Phil Trans Royal Soc B: Biol Sci. 2018;373(1754):20170268. https://doi.org/10.1027/0227-5910/a000120.
Hu HF, Liu TL, Hsiao RC, Ni HC, Liang SH, Lin CF, Chan HL, Hsieh YH, Wang LJ, Lee MJ, Chou WJ. Cyberbullying victimization and perpetration in adolescents with high-functioning autism spectrum disorder: Correlations with depression, anxiety, and suicidality. J Autism Dev Disord. 2019;49(10):4170–80. https://doi.org/10.1007/s10803-019-04060-7.
Chou WJ, Wang PW, Hsiao RC, Hu HF, Yen CF. Role of school bullying involvement in depression, anxiety, suicidality, and low self-esteem among adolescents with high-functioning autism spectrum disorder. Front Psychiatry. 2020;11:9. https://doi.org/10.3389/fpsyt.2020.00009.
Care DoHS. Suicide prevention in England: 5-year cross-sector strategy [Internet]. GOV.UK2023 [Available from: https://www.gov.uk/government/publications/suicide-prevention-strategy-for-england-2023-to-2028/suicide-prevention-in-england-5-year-cross-sector-strategy.
Kirby AV, Conner CM, Mazefsky CA. Are autistic females at greater risk of suicide? A call for clarity to advance suicide prevention for the whole community. Autism Res. 2024;17(5):898–905. https://doi.org/10.1002/aur.3120.
Rodgers J, Goodwin J, Nielsen E, Bhattarai N, Heslop P, Kharatikoopaei E, O’Connor RC, Ogundimu E, Ramsay SE, Steele K, Townsend E. Adapted suicide safety plans to address self-harm, suicidal ideation, and suicide behaviours in autistic adults: protocol for a pilot randomised controlled trial. Pilot Feasibility Stud. 2023;9(1):31. https://doi.org/10.1186/s40814-023-01264-8.
Acknowledgements
C.M.B and D.H gratefully acknowledge the financial support provided by Suicide Prevention Australia. We also wish to acknowledge Mirko Uljarević, author of our original review, for his continued and valuable discussions and advice on the topic of suicidality and mental health concerns in the autistic population. Additionally, we thank Alex Haschek for creating the bibliographic map presented in this article, which greatly enhanced our literature review and understanding of advancements in the field.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
D.H, C.M.B and V.N contributed to the study conception and design. C.M.B and E.S identified and screened the included articles. All authors completed full-text review and data extraction. C.M.B prepared Fig. 1, and Tables 1 and 2. The main manuscript text was written by C.M.B, D.H and V.N. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Human and Animal Rights and Informed Consent
All reported studies/experiments involving human or animal subjects performed by the authors were in accordance with the ethical standards of institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Brown, C.M., Newell, V., Sahin, E. et al. Updated Systematic Review of Suicide in Autism: 2018–2024. Curr Dev Disord Rep (2024). https://doi.org/10.1007/s40474-024-00308-9
Accepted:
Published:
DOI: https://doi.org/10.1007/s40474-024-00308-9