
Abstract
Overwhelming evidence suggests that a diagnosis of attention deficit/hyperactivity disorder (ADHD) in childhood has profound and far-reaching effects on children’s functioning in the school environment. In this article, we draw on a wide range of research studies to summarize the state of our knowledge about the academic functioning of children with ADHD and discuss intervention approaches that align with these areas. We use ecological systems theory to outline the various factors that are related to school functioning for children with ADHD at the child, classroom, and family levels. We place a particular emphasis on the importance of high-quality relationships within the delivery of interventions and highlight the need for sustainable, collaborative, and contextual interventions if we are to meet the complex and heterogeneous needs of children with ADHD in the school setting.
Similar content being viewed by others

Introduction
Children with attention deficit/hyperactivity disorder (ADHD) have significant impairments in the educational domain [1]. Most students with ADHD drastically perform below their skill level at school and have poor test performance, achievement scores, and report card grades [2, 3]. Importantly, children with ADHD also are rated below their peers on behaviors that enable academic success, such as motivation, engagement, interpersonal skills, and study skills [3, 4]. The academic difficulties experienced by children with ADHD at school are chronic and are associated with substantial social, health, and economic problems later in life [5–9]. Because of these well-documented serious and persistent educational difficulties, a multidimensional academic risk model has been identified for children with ADHD [10]. It is therefore important to consider several pertinent influences when attempting to understand and support children with ADHD in the classroom and in the home.
A useful model for understanding such influences is the ecological systems theory [11, 12]. This model conceptualizes a child’s functioning as a complex interaction between the child’s own characteristics and the factors in their environment. As such, this approach calls for a focus on the relational aspects of working with children with ADHD in the context of learning, namely relationships with and between the students themselves, peers, teachers, and parents. We present the current research on school problems experienced by children with ADHD while critically examining influences within the child, the family, and the classroom, and how together they may contribute to academic underachievement. We provide an overview of recent empirical investigations that offer promising methods for supporting the whole child with ADHD in the school context, with a focus on collaborative efforts between home and school.
Ecological Systems Theory
Ecological systems theory describes the child as an active and evolving system that develops by means of their individual ontogeny as well as through reciprocal interactions with people and things in their environments [11, 12]. Within this model, a child’s own characteristics and the various environmental influences are organized into various levels. Specifically, factors that originate from the child themselves make up the first level of the system, the child-level factors. Next are environmental influences within which the child operates directly, such as home and school. The last two levels consist of more distal factors that can influence the child’s functioning, such as neighborhood and cultural influences. Research suggests that there is a cumulative effect of multiple risk indicators within the individual person and their various “systems” of development [13]. Increasingly, ecological system models are being applied to educational research attempting to understand the complexity of children’s school functioning [14].
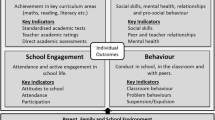
This theoretical backdrop is valuable in understanding the academic problems experienced by children with ADHD by focusing on the various factors that influence academic achievement and their interaction with one another. In this article, we will present an overview of the latest research on influences within the various systems in the lives of children with ADHD, including individual or child-centered influences, teacher/classroom influences, and parent/family influences, with a focus on how these systems interact to impact the development of learning problems for children and youth with ADHD (see Fig. 1). In addition to this, we will present the clinical implications of this research by presenting evidence from recent treatment studies. Finally, while the ecological systems theories also includes distal influences, such as public policy and neighborhood influences, the current review will focus solely on proximal or direct influences on the school functioning of children with ADHD, namely the child, family, and classroom.

An ecological systems model illustrating the interaction of variables influencing school functioning for children with ADHD
Child-Level Variables
By the time children with ADHD start school, they are likely to be behind their typically developing peers in basic math concepts, early literacy skills, and behavioral readiness [15, 16]. These academic difficulties endure throughout childhood and adolescence and are observed across subject areas regardless of the type of measurement or sample studied [17]. Significant effects remain after controlling for comorbid learning disabilities [5] and behavioral problems [18]. Mounting evidence suggests that the academic impairments seen in children with ADHD are primarily related to symptoms of inattention, rather than symptoms of hyperactivity and impulsivity [19–22]. Children who exhibit elevated inattentive behavior are likely to underachieve in reading [23, 24] and mathematics [25, 26]. Some evidence suggests that children with ADHD inattentive type may be more impaired academically than those with ADHD combined type (e.g., [27]).
A number of authors have proposed mechanisms to explain the association between ADHD and achievement [27–31], with both cognitive and behavioral pathways highlighted as contributing factors. A model that provides valuable insight was developed by Fergusson and colleagues [28, 29] and later replicated and expanded [30]. The authors hypothesized that there are both cognitive and behavioral pathways that predict scholastic achievement in children with ADHD. Specifically, they proposed that classroom performance mediates a behavioral pathway to scholastic achievement and that vigilance and memory mediate a cognitive pathway to scholastic achievement. Findings indicated that this dual pathway model was a good fit to the data, with both behavioral and cognitive pathways mediating the relationship between IQ and ADHD with scholastic achievement. These findings indicated that both cognitive and behavioral mediating variables account for the relationship between ADHD and scholastic achievement, accounting for approximately 77 % of the variance in achievement.
From a cognitive perspective, children with ADHD as a group demonstrate lower cognitive performance than their typically developing peers [32, 33]. Impairments in working memory—the ability to briefly store and manipulate information—appear to be particularly crucial in adversely affecting the learning of children with ADHD [34, 35].
Within the behavioral pathway, one possible mechanism by which ADHD influences achievement is by affecting learning-related behaviors (i.e., academic enablers or approaches to learning). In other words, a student’s motivation, engagement, and interpersonal skills may influence their exposure to academic material and their approaches to learning. Elementary-age students with ADHD have lower academic enabling behaviors than their non-ADHD peers [4]. For example, academic engagement is lower and off-task behavior is significantly higher among youth with ADHD than peers without ADHD [36, 37].
Youth with ADHD are at higher risk for experiencing comorbid psychopathology than their peers without an ADHD diagnosis [38]. Anxiety, mood disorders, and conduct problems are some of the most common comorbid diagnoses associated with ADHD. Children and adolescents who meet the criteria for an ADHD-PI diagnosis are more likely to experience comorbid internalizing symptoms, whereas children and adolescents who meet the criteria for an ADHD-HI diagnosis are more likely to experience comorbid externalizing symptoms. Considering and treating comorbid diagnoses associated with ADHD is essential given that researchers have determined that the clinical course of ADHD is typically worsened by the presence of comorbid disorders [39].
At the individual level, the prescription of psychotropic medication is the most common treatment approach for ADHD [40]. A recent meta-analysis reveals that stimulant medication is associated with moderate to large effects on behavioral and social functioning of children with ADHD [41], yet the effects on academic functioning are considerably lower [42]. Although used frequently, pharmacological treatment rarely is sufficient in addressing the multiple difficulties faced by students with ADHD in the school setting [4], and many parents report uncertainty about using medication as a first approach to treatment [43]. Computerized cognitive training programs, such as working memory training, have been studied extensively for children with ADHD, but recent meta-analytic findings suggest that there is minimal support that this treatment modality improves behavioral, social, or academic outcomes for children with ADHD [44]. Therefore, it is important to consider contextual influences within a child’s life that may be targeted for more comprehensive treatment. Indeed, experts in this field are now calling for research that addresses such contextual factors if we are to advance our understanding of ADHD referral, assessment, and treatment practices [45].
Classroom-Level Variables
It is evident how the core symptoms of ADHD would interfere within a traditional classroom setting. Because academic achievement is directly associated with attention during instruction [46], ADHD can have a profound influence on students’ outcomes in the classroom. Children with ADHD are typically less engaged during classroom instruction [37], show avoidance for working collaboratively with their peers [47], display frequent off-task behavior [48], have short attentive states during classroom teaching [49], and underachieve dramatically compared to their peers [16]. Children with ADHD approach classroom work with less effort [50] and less persistence and report less enjoyment in their academic work [51].
Recent research suggests that behavior-based interventions that are focused on teacher training are effective for addressing ADHD in the classroom setting [52–54] and are also deemed to be most helpful by students themselves [55]. School-based interventions include positive reinforcement procedures, reward programs, response cost strategies, teaching self-monitoring, daily report cards, provision of a quiet working environment and extra time, chunking material, giving frequent feedback, and organizational skills training [52, 54]. In order for these classroom interventions to be effective, they must be targeted to students’ specific needs, be implemented consistently, and continue until students are able to internalize self-control strategies [54]. Unfortunately, current research suggests that this rarely happens in practice [56].
All teacher-mediated interventions rely on a strong and collaborative relationship between teacher and student; however, an emerging body of research suggests that the teacher–student relationship may be less than optimal for children with ADHD. Researchers asked children with and without clinical levels of ADHD symptoms about their perceptions of their classroom environments [57•]. Controlling for age, co-occurring conduct problems, and reading abilities, children in the ADHD group perceived their teachers as more controlling, reported feelings of incompetence in the classroom, and reported feeling less connected with their teachers. More recently, researchers have investigated the “working alliance” between students with ADHD symptomatology and their teachers [58]. In the classroom setting, the working alliance not only refers to the emotional connection between teacher and student (i.e., bond) but also considers aspects of the teacher–student relationship that involve work and learning goals and tasks (i.e., collaborative interactions around learning) [59]. Children with ADHD had lower scores on both teacher–student bond and collaboration than the non-ADHD group, according to both teacher and student reports. Girls in the ADHD group were especially likely to report a weaker bond and less collaboration in their relationship with their teachers. Conduct problems and academic difficulties did not significantly affect these differences. Importantly, for the ADHD group, a strong teacher–student bond was associated with increased academic motivation. Certainly, these studies point to the important role that teachers play in the well-being and academic success for children with ADHD at school, with implications for the success of intervention programs.
Although a variety of empirically supported interventions are available for use in schools [60], they are employed rarely and when implemented are frequently ineffective [61–63]. It has been proposed that this may be due to various obstacles facing teachers in the effective implementation of such programs [64]. To address these obstacles, a recently developed intervention, The Teacher Help for ADHD Program, uses an online format and a coach to provide teachers with knowledge about ADHD and its etiology and treatment and to discuss misconceptions about ADHD and facilitate collaboration between the family and the school [64]. The program, which has promising preliminary results, focuses on improving instructional and behavioral management practices and aims to make evidence-based treatments easy to understand and implement. There is also a focus on teacher–student–parent communication, as well as providing support to teachers to reduce their own stress [64, 65].
Family-Level Variables
Until recently, the role of the family was not addressed in research about the academic functioning of children with ADHD. This is despite a vast body of literature on typically developing children demonstrating that family involvement in children’s learning is associated with a host of positive school outcomes, both concurrently and over time [66]. Family involvement in the education of children is associated with several benefits for the child, including improvements in school engagement, attitudes toward school, and academic performance [67].
An abundance of research demonstrates that parents of children with ADHD experience significant struggles in parenting efforts [68]. Recent research suggests that these parenting difficulties extend to learning-related interactions as well. For instance, homework problems are common among children and youth with ADHD, including problems in homework completion and accuracy [69, 70]. Rogers and colleagues found that, compared to parents of children with no ADHD diagnosis, parents of children with ADHD reported lower self-efficacy in their ability to help their children with their school work and felt they had less time and energy available to participate in their children’s learning [71]. When mothers and fathers are examined separately, interesting differences emerge. Mothers of children with and without ADHD reported similar types and levels of involvement behaviors in the home. Fathers of children with ADHD reported being more disengaged from their children’s learning and using more coercive and punitive interactions regarding their children’s achievement compared to fathers of children without ADHD [71]. Importantly, negative control strategies around learning have been found to be associated with both increases in parenting stress for both mothers and fathers, and more severe ADHD symptoms [72]. Unfortunately, most family-based interventions for ADHD (e.g., parent behavioral training) focus on behavioral problems in the home and do not target learning- or school-related interactions.
Family-School Collaboration
Conflict between the family and school is common among children and youth with ADHD [73, 74]. In comparison to parents of typically developing children, parents of children with clinical diagnoses of ADHD perceive that their children’s school as less inviting [71]. Specifically, parents of children with ADHD report that their children’s schools are less welcoming and perceive more demands from teachers, compared to control families. These differences were significant beyond the influence of family socio-economic status, as well as children’s comorbid oppositional behavior problems. In a recent investigation, it was found that the quality of the parent–teacher relationship was associated with the effectiveness of parent–teacher communications related to homework [74].
In light of these studies, researchers have been turning with increasing frequency to the family–school partnership as an important target for intervention. A daily report card (DRC) system is an example of a commonly used and effective family–school communication program, with several studies documenting their effectiveness [75]. A DRC contains a list of goals on which teachers indicate a child’s performance on a Likert scale (e.g., 1 = superior performance and 5 = unacceptable performance). Teacher ratings are provided throughout the day and parents then provide home-based reinforcement contingent on daily and weekly goals. As progress is documented, goals can be raised. DRC programs have been successful in enhancing classroom behavior and academic performance of students with ADHD, particularly for those with mild symptoms. In an important study documenting the promise of DRC, Fabiano and colleagues demonstrated that the use of DRC can reduce the number of students who require stimulant medication and can reduce the size of the therapeutic dose for those students receiving medication [76].
Pfiffner and colleagues took an existing evidence-based behavior modification and skill development program and adapted it from a clinic-based implementation model to a school-based model [77, 78]. This multisystemic program, called the Collaborative Life Skills Program (CLS), employs various strategies: teacher consultation, daily report cards, behavioral parent training, and child social and life skills training. CLS is streamlined in such a way that parents, children, and teachers are trained using the same terminology, timelines, and methods. Results from the CLS demonstrated improvements on ratings of ADHD symptoms, organizational skills, homework problems, academic skills, report card grades, academic achievement, and classroom observations of student engagement [79]. A more recent evaluation of the CLS program found that the strength of the treatment gains was proportional to the level of engagement by the parents, that is, greater parent treatment adherence and support of child skills were independently associated with positive treatment outcomes [80].
The Family–School Success [81•] program is a collaborative treatment approach for ADHD that focuses on building family–school partnerships through the use of conjoint-behavioral consultation and DRC and via systematic homework interventions. A unique element of this program is its focus on bringing teachers and parents together as partners in the child’s education. Rigorous randomized control trial data suggest that the Family-School Success (FSS) program had a significant effect on the quality of the family–school relationship, homework performance, and parenting behavior [82]. Like the CLS program, Clarke and colleagues found that parental program attendance and adherence to the FSS program predicted response to intervention, suggesting again that parent engagement in treatment programs is essential for improving child outcomes [82].
Conclusions
The evidence is unequivocal: a diagnosis of ADHD in childhood has profound adverse effects on many aspects of children’s school functioning. Using an ecological systems framework, we reviewed functional deficits at the child, family, and classroom levels, and the treatment approaches that have been devised to address them. In reviewing the pertinent issues, treatments, and challenges, it is clear that ADHD has far-reaching effects on the children’s functioning and that unilateral approaches to treatment are likely insufficient to address the many difficulties facing these children at school. If we are to meet the multidimensional needs within the various systems in which these children develop and learn, there must be a commitment to ADHD treatment programs that are collaborative and that carefully consider the nature and quality of the relationships with and between all people involved. Furthermore, due to the inherent heterogeneity of difficulties and comorbidities that is typical of this population, there is no “one size fits all” approach that will work. Rather, treatments must be individually tailored and targeted at the points of performance, be it a lagging academic skill or ineffective teacher–parent communication. Finally, it is important to note that ADHD is a chronic condition, and interventions must be sustainable over time and implemented collaboratively between home and school.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
DuPaul GJ, Stoner G. ADHD in the schools: assessment and intervention strategies. 3rd ed. New York: Guilford; 2014.
Langberg JM, Epstein JN, Altaye M, Molina BSG, Arnold LE, Hinshaw SP, et al. Patterns and predictors of adolescent academic achievement and performance in a sample of children with attention-deficit/hyperactivity disorder. J Clin Child Adolesc Psychol. 2011;40:519–31.
Schultz BK, Evans SW, Serpell ZN. Preventing failure among middle school students with attention deficit hyperactivity disorder. A Survival Analysis School Psychology Review. 2009;38:14–27.
DuPaul GJ, Volpe RJ, Jitendra AK, Lute G, Lorah KS, Gruber R. Elementary school students with AD/HD. J Sch Psych. 2004;42:285–301.
Currie J, Stabile M. Child mental health and human capital accumulation. The case of ADHD J Health Econ. 2006;25:1094–118.
Barkley RA, Fischer M, Smallish L, Fletcher K. Young adult outcome of hyperactive children: adaptive functioning in major life activities. J Am Acad Child Adolesc Psychiatry. 2006;45:192–202.
Biederman J, Petty C, Fried R, Fontanella J, Doyle AE, Seidman LJ, et al. Impact of psychometrically defined deficits of executive functioning in adults with attention deficit hyperactivity disorder. Am J Psych. 2006;163:1730–8.
Harpin VA. The effect of ADHD on the life of an individual their family and community from preschool to adult life (attention deficit/hyperactivity disorder). Arch Dis Child. 2005;90:i2.
Pelham WE, Robb JA, Foster EM. The economic impact of attention-deficit/hyperactivity disorder in children and adolescents Ambulatory Pediatrics. 2007;7:121–131
Martin AJ. The role of ADHD in academic adversity: disentangling ADHD effects from other personal and contextual factors. Sch Psychol Q. 2014;29:395–408.
Bronfenbrenner U. In N J Smelser & B Baltes (eds) International encyclopedia of the social and behavioral sciences. 2001;10:6963.
Sameroff AJ. General systems theories and developmental psychopathology. In: Cicchett D, Cohen DJ, editors. Developmental psychopathology: vol 1 theory and methods. New York: Wiley; 1995.
Gutman LM, Sameroff AJ, Eccles SJ. The academic achievement of African American students during early adolescence: an examination of multiple risk promotive and protective factors American. J Comm Psych. 2002;3:367–99.
Ysseldyke J, Lekwa A, Klingbeil D, Cormier D. Assessment of ecological factors as an integral part of academic and mental health consultation. J Educ Psychol Consult. 2012;22:21–43.
DuPaul GJ, McGoey KE, Eckert TL, VanBrakle J. Preschool children with ADHD: impairments in behavioral social and school functioning. J Am Acad Child Adolesc Psychiatry. 2001;40:508–15.
Massetti GM, Lahey BB, Pelham WE, Loney J, Ehrhardt A, Lee SS, et al. Academic achievement over 8 years among children who met modified criteria for attention-deficit/hyperactivity disorder at 4–6 years of age. J Abnorm Child Psychol. 2008;36:399–410.
Frazier TW, Youngstrom EA, Glutting JJ, Watkins MW. A DHD and achievement: meta-analysis of the child adolescent and adult literatures and a concomitant study with college students. J Learn Disabil. 2007;40:49–65.
Giannopulu I, Escolano S, Cusin F, Citeau H, Dellatolas G. Teachers’ reporting of behavioural problems and cognitive-academic performances in children aged 5–7 years. Br J Educ Psychol. 2008;78:127–47.
Breslau J, Miller E, Breslau N, Bohnert K, Lucia V, Schweitzer J. The impact of early behavior disturbances on academic achievement in high school. Pediatrics. 2009;123:1472–6.
Pingault JB, Cote SM, Vitaro F, Falissard B, Genolini C, Tremblay RE. The developmental course of childhood inattention symptoms uniquely predicts educational attainment: a 16-year longitudinal study. Psychiatry Res. 2014;219:707–9.
Pingault JB, Tremblay RE, Vitaro F, Carbonneau R, Genolini C, Falissard B, et al. Childhood trajectories of inattention and hyperactivity and prediction of educational attainment in early adulthood: a 16-year longitudinal population-based study. Am J Psychiatry. 2011;168:1164–70.
Rabiner D, Coie JD. Early attention problems and children’s reading achievement: a longitudinal investigation. J Am Acad Child Adolesc Psychiatry. 2000;39:859–67.
Warner-Rogers J, Taylor A, Taylor E, Sandberg S. Inattentive behavior in childhood: epidemiology and implications for development. J Learn Disabil. 2000;33:520–36.
Willcutt EG, Pennington BF. Comorbidity of reading disability and attention deficit/ hyperactivity disorder: differences by gender and subtype. J Learn Disabil. 2000;33:179–91.
Marshall RM, Hynd GW, Handwrek MJ, Hall J. Academic underachievement in ADHD subtypes. J Learn Disabil. 1997;30:635–42.
Raghubar K, Cirino P, Barnes M, Ewing-Cobbs L, Fletcher J, Fuchs L. Errors in multi-digit arithmetic and behavioral inattention in children with math difficulties. J Learn Disabil. 2009;42:356–71.
Weiss MD, Worling DE, Wasdell MD. A chart review study of the inattentive and combined types of ADHD. J Atten Disord. 2003;7:1–9.
Fergusson DM, Horwood LJ. Early disruptive behavior IQ and later school achievement and delinquent behavior. J Abnorm Child Psychol. 1995;23:183–99.
Fergusson DM, Horwood LJ, Linksey MT. The effects of conduct disorder and attention deficit in middle childhood on offending and scholastic ability at age 13. J Child Psychol Psychiatry. 1993;34:899–916.
Rapport MD, Scanlon SW, Denney CB. Attention-deficit/hyperactivity disorder and scholastic achievement: a model of dual developmental pathways. J Child Psychol Psychiatry. 1999;40:1169–83.
Volpe RJ, DuPaul GJ, DiPerna JC, Jitendra AK, Lutz JG, Tresco K, et al. Attention deficit hyperactivity disorder and scholastic achievement: a model of mediation via academic enablers school. Psychol Rev. 2006;35:47–61.
Frazier TW, Demaree HA, Youngstrom EA. Meta-analysis of intellectual and neuropsychological test performance in attention-deficit/hyperactivity disorder. Neuropsychology. 2004;18:543–55.
Barkley RA. Attention-deficit hyperactivity disorder. 3rd ed. New York: Guilford; 2006.
Martinussen R, Hayden J, Hogg-Johnson S, Tannock R. A meta-analysis of working memory impairments in children with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2005;44:377–84.
Willcutt E, Doyle A, Nigg J, Faraone S, Pennington B. Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biol Psychiatry. 2005;57:1336–46.
Abikoff H, Jensen PS, Arnold LL, Hoza B, Hechtman L, Pollack S, et al. Observed classroom behavior of children with ADHD: relationship to gender and comorbidity. Journal of Abnormal Child Psychology. 2002;30:349–59.
Junod RE, DuPaul GJ, Jitendra AK, Volpe RJ, Cleary KS. Classroom observations of students with and without ADHD: differences across types of engagement. J Sch Psychol. 2006;44:87–104.
Szatmari P, Offord DR, Boyle MH. Correlates associated impairments and patterns of service utilization of children with attention deficit disorder: findings from the Ontario child health study. J Child Psychol Psychiatry. 1989;30:205–17.
Jensen PS, Martin D, Cantwell DP. Comorbidity in ADHD: implications for research practice and DSM-V. J Am Acad Child Adolesc Psychiatry. 1997;36:1065–79.
Zito J, Safer D, de Jong-van den Berg L, Janhsen K, Fegert J, Gardner J … Valuuri SC. A three-country comparison of psychotropic medication prevalence in youth. Child and Adolescent Psychiatry and Mental Health. 2008;2
Faraone S, Buitelaar J. Comparing the efficacy of stimulants for ADHD in children and adolescents using meta-analysis. Eur Child Adolesc Psychiatry. 2010;19:353–64.
Van der Oord S, Prins PJM, Oosterlaan J, Emmelkamp PMG. Efficacy of methylphenidate psychosocial treatments and their combination in school-aged children with ADHD: a meta-analysis. Clin Psychol Rev. 2008;28:783–800.
Johnston C, Hommersen P, Seipp C. Acceptability of behavioral and pharmacological treatments for attention-deficit/hyperactivity disorder: relations to child and parent characteristics. Behav Ther. 2008;39:22–32.
Rapport MD, Orban SA, Friedman LM, Kofler MJ. Do programs designed to train working memory other executive functions and attention benefit children with ADHD? A meta-analytic review of cognitive academic and behavioral outcomes. Clin Psychol Rev. 2013;1237–1252.
DuPaul GJ, Jimmerson SR. Assessing understanding and supporting students with ADHD at school: contemporary science practice and policy. Sch Psychol Q. 2014;29:379–84.
Gest SD, Gest JM. Reading tutoring for students at academic and behavioral risk: effects on time-on-task in the classroom. Educ Treat Child. 2005;28:25–47.
Zentall SS, Beike SM. Achievement of social goals of younger and older elementary students: response to academic and social failure. Learn Disabil Q. 2012;35:39–53.
Kofler MJ, Rapport MD, Alderson RM. Quantifying ADHD classroom inattentiveness its moderators and variability: a meta-analytic review. J Child Psychol Psychiatry. 2008;49:59–69.
Rapport MD, Kofler MJ, Alderson RM, Timko Jr T, DuPaul GJ. Variability of attention processes in ADHD: observations from the classroom. J Atten Disord. 2009;12:563–73.
Egeland J, Johansen SN, Ueland T. Differentiating between ADHD sub-types on CCPT measures of sustained attention and vigilance. Scand J Psychol. 2010;50:347–54.
Carlson C, Booth J, Shin M, Canu W. Parent- teacher- and self-related motivational styles in ADHD subtypes. J Learn Disabil. 2002;35:104–13.
DuPaul GJ, Weyandt LL, Janusis GN. ADHD in the classroom: effective intervention strategies. Theory Pract. 2011;50:35–42.
Evans SW, Owens JS, Bunford N. Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. J Clin Child Adolesc Psychol. 2014;43:527–51.
Rajwan E, Chacko A, Moeller M. Nonpharmacological interventions for preschool ADHD: state of the evidence and implications for practice. Prof Psych: Res Pract. 2012;43:520–6.
Walker-Noack L, Corkum P, Elik N, Fearon I. Youth perceptions of attention-deficit/hyperactivity disorder and barriers to treatment. Can J Sch Psychol. 2013;28:193–218.
Parker J, Wales G, Chalhoub N, Harpin V. The long-term outcomes of interventions for the management of attention-deficit hyperactivity disorder in children and adolescents: a systematic review of randomized controlled trials. Psychological Research and Behavior Management. 2013;6:87–99.
Rogers M, Tannock R. Are classrooms meeting the basic psychological needs of children with ADHD symptoms? A self-determination theory perspective. J Atten Disord. 2013;1–7. This article highlights difficulties in the classroom environment from the perspective of children with ADHD.
Rogers M, Belanger V, Toste J, Heath N. Mismatched: an investigation of ADHD symptoms in the classroom and the teacher-student relationship. Emotional and Behavioural Difficulties. In press.
Toste JR. Reconceptualizing teacher-student relationships to foster school success: working alliance within classroom contexts. Educ Can. 2012;52.
Eckert TL, DuPaul GJ, Vilardo B. The effects of school-based interventions for attention deficit hyperactivity disorder: a meta-analysis 1996–2010. Sch Psychol Rev. 2012;41:387–412.
Fabiano GA, Pelham Jr WE. Improving the effectiveness of behavioral classroom interventions for attention-deficit/hyperactivity disorder: a case study. J Emot Behav Disord. 2003;11:122–8.
Leslie LK, Wolraich ML. ADHD service use patterns in youth. J Pediatr Psychol. 2007;32:695–710.
Repie MS. A school mental health issues survey from the perspective of regular and special education teachers school counselors and school psychologist. Educ Treat Child. 2005;28:279–98.
Elik N, Corkum P, Blotnicky-Gallant P, McGonnell M. Overcoming the barriers to teachers’ utilization of evidence-based interventions for children with ADHD: the teacher help for ADHD program. Perspectives in Language and Literacy. In press.
Elik N, Corkum P, Blotnicky P, McGrath P, Kutcher S. Randomized-controlled trial of a classroombased distance intervention for teachers of elementary school-aged children with ADHD. Symposium Presentation at American Academy of Child and Adolescent Psychiatry. Orlando, Florida; 2013, October.
Christenson S, Sheridan SM. Schools and families: creating essential connections for learning. New York NY: Guilford; 2001.
Jeynes WH. A meta-analysis of the relation of parental involvement to urban elementary school student achievement. Urban Educ. 2005;40:237--269.
Johnston C, Mash EJ. Families of children with attention-deficit/hyperactivity disorder: review and recommendations for future research. Clin Child Fam Psychol Rev. 2001;4:183–207.
Langberg JM, Epstein JN, Girio-Herrera E, Vaughn AJ, Becker SP. Evaluation of the homework organization and planning skills (hops) intervention for middle school students with attention deficit hyperactivity disorder as implemented by school mental health providers. Sch Psychol Rev. 2012;41:342–64.
Power TJ, Werba BE, Watkins MW, Angelucci JG, Eiraldi RB. Patterns of parent-reported homework problems among ADHD-referred and non-referred children. 2006;21:12–33
Rogers M, Wiener J, Marton I, Tannock R. Parental involvement in children's learning: comparing parents of children with and without ADHD. J Sch Psychol. 2009;47:167–85.
Rogers M, Wiener J, Marton I, Tannock R. Supportive and controlling parental involvement as predictors of children’s academic achievement: relations to children’s ADHD symptoms and parenting stress. Sch Ment Heal. 2009;1:89–102.
Mautone JA, Lefler EK, Power TJ. Promoting family and school success for children with ADHD: strengthening relationships while building skills. Theory Pract. 2011;50:43–51.
Mautone JA, Marcelle E, Tresco KE, Power J. Assessing the quality of parent-teacher relationships for students with ADHD. Psychology in the Schools. 2014:DOI: 101002/pits21817
Volpe RJ, Fabiano GA. Daily behavior report cards: an evidence-based system of assessment and intervention. New York NY: Guilford; 2013.
Fabiano GA, Pelham Jr WE, Gnagy EM, Burrows-MacLean L, Coles EK, Chacko A, Robb JA. The single and combined effects of multiple intensities of behavior modification and methylphenidate for children with attention deficit hyperactivity disorder in a classroom setting School Psychology Review. 2007;36:195–216
Pfiffner LJ, Kaiser NM, Burner C, Zalecki C, Rooney M, Setty P, et al. From clinic to school: translating a collaborative school-home behavioral intervention for ADHD. Sch Ment Heal. 2011;3:127–42.
Pfiffner LJ, Villodas M, Kaiser N, Rooney M, McBurnett K. Educational outcomes of a collaborative school-home behavior intervention for ADHD. Sch Psychol Q. 2013;28:25–36.
Villodas MT, McBurnett K, Kaiser N, Rooney M, Pfiffner LJ. Effects of parent adherence on social and behavioral outcomes of a collaborative school-home behavioral intervention for ADHD. Child Psychiatry Hum Dev. 2014;45:348–60.
Mautone J, Marshall SA, Sharman J, Eiraldi R, Jawad A, Power T. Development of a family school intervention for young children with attention deficit hyperactivity disorder. Sch Psychol Rev. 2012;41:447–66.
Power TJ, Clarke AT, Mautone JA, Soffer SL, Marshall SA, Jaward AF SJ. Family-school intervention for children with ADHD: results of a randomized clinical trial. Journal of Counselling and Clinical Psychology. 2012;80:611–23. This paper presents compelling results from an RCT highlighting family-school collaboration as a promising target for intervention for children with ADHD.
Clarke AT, Marshall SA, Mautone JA, Soffer SL, Jones HA, Costigan TE, et al. Parent attendance and homework adherence predict response to a family-school intervention for children with ADHD. J Clin Child Adolesc Psychol. 2013. doi:https://doi.org/10.1080/153744162013794697.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Compliance with Ethics Guidelines
Additional information
Conflict of Interest
Maria Rogers, Julia Boggia, Julia Ogg, and Robert Volpe declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
This article is part of the Topical Collection on ADHD
Rights and permissions
About this article

Cite this article
Rogers, M., Boggia, J., Ogg, J. et al. The Ecology of ADHD in the Schools. Curr Dev Disord Rep 2, 23–29 (2015). https://doi.org/10.1007/s40474-015-0038-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40474-015-0038-6