
Abstract
Purpose
Hypoxia is a major cause of radioresistance in head and neck cancer (HNC), resulting in treatment failure and disease recurrence. 18F-fluoromisonidazole ([18F]FMISO) PET has been proposed as a means of localising intratumoural hypoxia in HNC so that radiotherapy can be specifically escalated in hypoxic regions. This concept may be challenging to implement in routine clinical practice however, given that [18F]FMISO PET is costly, time consuming and difficult to access. The aim of this review was to summarise clinical studies involving [18F]FMISO PET and to appraise the evidence for its role in guiding radiotherapy treatment in HNC.
Methods
A comprehensive literature search was conducted on PubMed and Web of Science databases. Studies investigating [18F]FMISO PET in newly diagnosed HNC patients were considered eligible for review.
Results
We found the following important results from our literature review: (1) Studies have demonstrated a correlation between [18F]FMISO PET and other hypoxia biomarkers, although the results are not consistent enough to propose a proxy biomarker of [18F]FMISO PET. (2) [18F]FMISO PET uptake changes during a course of radiotherapy treatment, suggesting that imaging should be repeated during treatment. (3) Tumour recurrences do not always occur within the pretreatment hypoxic volume on [18F]FMISO PET. (4) Dose modification studies using [18F]FMISO PET are in a pilot phase.
Conclusions
Our results show that currently there is insufficient evidence to propose [18F]FMISO PET for radiotherapy dose adaptation in HNC in a routine clinical setting. Part of the challenge is that hypoxia is a dynamic phenomenon, and thus areas identified on a single scan may not be representative. At present, it is anticipated that [18F]FMISO PET will remain useful within the research setting only.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Hypoxia has long been identified as a negative prognostic factor in head and neck cancer (HNC) [1]. It renders cancer cells more resistant to therapies [2] and confers an aggressive phenotype on the tumour. A major treatment modality for locally advanced HNC is radiotherapy, but 30–40% of cases will relapse within 5 years [3]. Most recurrences occur within the high dose region of the irradiated field [4], due to the presence of radioresistant clones within the tumor cell population. Hypoxia is a key driver of radioresistance. It has been shown in vitro that hypoxic cancer cells require three times the delivered radiation dose to achieve the same therapeutic effect [5]. Given the deleterious consequences of hypoxia in head and neck cancer, it is important to develop a means to identify this phenomenon upfront, so that treatment can be tailored to overcome it. PET (positron emission tomography) imaging of tumors using hypoxia specific tracers is an attractive method of assessing hypoxia. It is non-invasive, can be easily repeated and provides spatial information across the whole tumor. The last point is especially relevant to locally advanced HNC, where it is feasible to deliver a dose escalation specifically to the hypoxic region identified within a tumour [6]; a concept known as ‘dose painting’. Of all the hypoxic tracers developed, 18F-fluoromisonidazole ([18F]FMISO) is the most widely investigated in head and neck cancers.
Numerous clinical studies have been conducted in HNC patients using [18F]FMISO PET imaging, evaluating different aspects, such as correlation with other hypoxia biomarkers [7,8,9], the ability to prognosticate in HNC patients [10], and the variation in uptake during serial imaging [11, 12]. Although there is a wealth of published literature, it is difficult to summate their outcomes as the studies are heterogenous with regards to study design, image analysis (for example evaluating standardized uptake value (SUV)max versus tumour to background ratio (TBR)) and research question. A significant barrier to clinical adoption of [18F]FMISO PET is expense and access to the tracer. In most countries, [18F]FMISO is not commercially available and is produced only at a handful of research institutions, making it costly to obtain [13]. Furthermore, its lipophilic nature leads to slow clearance of the tracer from blood/normal tissues which makes its use time consuming (as PET images need to be acquired 2—4 h after tracer injection) and results in images with a low signal to background ratio.
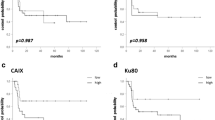
Several studies have reported a prognostic association between [18F]FMISO uptake pretreatment and survival outcomes [10, 12, 14, 15]. A meta-analysis [16] of 4 trials that included a total of 120 HNC patients who had pretreatment [18F]FMISO imaging and subsequently received curative radiotherapy was recently reported. The patient populations varied in T stage, tumour volume and human papilloma virus (HPV) status. Nevertheless, a multivariate analysis (which included T stage and HPV status) found that baseline [18F]FMISO uptake had a significant impact on locoregional control (p = 0.04) and overall survival (p < 0.04) in HNC patients treated with radiotherapy. Despite its role as a potential prognostic biomarker, [18F]FMISO PET has not yet transitioned into the clinic. Clinical use may be more likely if the results of [18F]FMISO PET imaging were to change management in patients, such as by individualizing radiotherapy treatment.
Radiotherapy dose escalation has been investigated as a means to overcome radioresistance [17] with different target volumes proposed to receive dose escalation, such as the FDG avid tumour volume [17] or the radiotherapy planning target volume (PTV) [18]. The hypoxic volume on [18F]FMISO PET imaging has also been suggested as a candidate for radiotherapy dose escalation [6], given that hypoxia is a key driver of radioresistance. Several planning studies have demonstrated that it is technically possible to increase the radiotherapy dose to the [18F]FMISO hypoxic volume without exceeding normal tissue tolerance doses [6, 19, 20]. However, whether [18F]FMISO will progress into the clinic to routinely guide radiotherapy treatment for HNC patients remains to be seen. The justification and evidence to support radiotherapy dose escalation to [18F]FMISO PET based hypoxia need to be considered, along with the practicalities of conducting these scans.
The purpose of this narrative review is to summarize the key findings from clinical studies of [18F]FMISO PET in HNC patients so far, to help understand its utility and whether it could realistically be used to guide radiotherapy ‘dose painting’ in HNC. To achieve this, four key questions will be addressed:
-
(1)
Is there a surrogate and ‘easy to perform’ biomarker for the [18F]FMISO hypoxia phenotype on imaging? This would help select patients for [18F]FMISO imaging and avoid the cost and inefficiency of scanning all patients.
-
(2)
Is [18F]FMISO PET imaging reproducible and repeatable?
-
(3)
Do locoregional recurrences occur within the initial hypoxic volume on [18F]FMISO PET, such that we could justify dose escalation to the hypoxic volume specifically?
-
(4)
What have we learned so far from dose escalation/de-escalation studies?
Of note, we have not included studies investigating the prognostic potential of [18F]FMISO PET, given this has been addressed in a meta-analysis
Methods
We performed a comprehensive search of Pubmed and Web of Science Databases up to 15 November 2023 to identify relevant articles published from 1992 onwards. The year 1992 was chosen as it is when the first-in-man imaging of [18F]FMISO was reported [21]. We searched for academic scientific papers whose abstracts included any of the following terms: ‘fluoromisonidazole’, ‘misonidazole’, ‘F-MISO’, ‘[18F]FMISO, ‘18F-MISO’ or ‘FMISO’. Studies were included which investigated [18F]FMISO PET imaging (either at baseline or during treatment) in newly diagnosed HNC patients. The articles were reviewed for applicability to our ‘key questions’ and overall, 40 publications were selected for inclusion. Figure 1 shows the PRISMA flowchart for study selection.

PRISMA flowchart for study selection
Data were consistently recorded for each study and included the number of patients, [18F]FMISO imaging parameters, time course of [18F]FMISO scanning and the time point during treatment when scans were conducted. The key findings of the studies are summarized here as a narrative review as this was felt to be the most suitable format to provide an overarching view of [18F]FMISO in HNC.
Results
A comprehensive literature review was undertaken and the details and focus of the resulting studies are illustrated in Fig. 2. The majority (58%) were studies correlating [18F]FMISO PET either with tissue or blood hypoxic biomarkers, or other imaging biomarkers. Figure 3 maps out the studies geographically. The 40 studies included in this review were performed at just 13 institutions, across 8 countries, and 18 of the published studies were from Germany alone.

Studies included in this narrative review

Geographical illustration to show where the studies have been conducted
The studies have been summarised in evidence tables (see Tables 1, 2, 3, 4, 5, 6, 7 and 8), with some entered twice if they addressed 2 topics (for example repeat imaging and correlation with 18F-fluorodeoxyglucose (18F-FDG)). The results are discussed in detail below, in line with our ‘key questions’.
Correlation of [18F]FMISO PET with other biomarkers—is there a surrogate?
[18F]FMISO PET scans are both expensive and time consuming to conduct (as images are acquired 2–4 h after tracer injection), therefore an easily accessible ‘surrogate’ hypoxia biomarker, which could help select patients who would benefit from [18F]FMISO imaging, would be desirable. Alternative biomarkers include hypoxia-associated protein immunohistochemistry (IHC), hypoxic gene expression, oxygen electrode measurement (all tumour based) and serum osteopontin. Since all patients undergo a biopsy and blood tests at diagnosis, it would be ideal if one of these investigations could be applied to select patients for [18F]FMISO PET imaging. The studies correlating [18F]FMISO PET with other hypoxia biomarkers are summarised in Tables 1 and 2.
Studies correlating hypoxia protein immunohistochemistry with [18F]FMISO uptake
Immunohistochemical markers of hypoxia include hypoxia-inducible factor 1-alpha (HIF1α), carbonic anhydrase 9 (CaIX) and glucose transporter 1 (Glut-1). These are endogenous proteins whose expression is upregulated in hypoxic conditions [22] and can be measured using IHC on tumour biopsy specimens. Table 1 outlines the six studies [8, 13, 19, 23,24,25] which assessed the relationship between hypoxia on [18F]FMISO PET and IHC markers of hypoxia. Overall, the results are mixed, with three studies [8, 13, 23] reporting a positive correlation between hypoxia IHC markers and hypoxia on [18F]FMISO PET, and two studies [19, 25] concluding that there was no association. Nicolay et al. [24] conducted the largest study, assessing the relationship with hypoxia IHC (both CaIX and HIF1α) and [18F]FMISO PET conducted at different time points (week 0, 2 and 5) in 49 patients undergoing chemoradiotherapy. There was no correlation between either HIF1a or CaIX expression and [18F]FMISO hypoxia in treatment-naïve patients. They did however find an association between hypoxia IHC and ‘adverse hypoxia dynamics’ on [18F]FMISO PET, i.e., delayed resolution of hypoxia on PET scans during radiotherapy treatment.
It appears that there may be a relationship between HIF1α /CaIX/Glut-1 expression and [18F]FMISO imaging, but current evidence is insufficient to propose a proxy biomarker of [18F]FMISO uptake. This question could be answered more fully using archival tumour samples from previous [18F]FMISO trials to assess correlation with HIF1α or CaIX. Ideally, quantification of hypoxia IHC would be consistent; at present some studies look at ‘positive’ versus ‘negative’ expression using a cutoff level, whereas others assess the degree of protein expression as a continuous variable resulting in difficulties interpreting the results of the various studies. It should be noted that a caveat of using tumour IHC is sampling bias. Hypoxia is typically heterogeneously distributed across a tumour, so a single biopsy sample may not be representative of the whole tumour. Furthermore, the markers measure different aspects of hypoxia and may not correlate with each other. For example, HIF1α expression represents the transcriptional changes that occur in response to a chronically hypoxic tumour microenvironment whereas [18F]FMISO uptake is a direct indicator of intracellular hypoxia, both acute and chronic. Hence, the lack of any correlation should not be interpreted as[18F]FMISO having an inferior ability to detect hypoxia.
Studies correlating other hypoxia biomarkers with [18F]FMISO uptake
The other hypoxia biomarkers which have been studied in relation to [18F]FMISO imaging are oxygen electrode measurements, gene signatures, and plasma hypoxia markers. The details of these studies are summarised in Table 2. Oxygen electrodes allow direct measurement of hypoxia by inserting small needles into tumours to measure the partial pressure of oxygen (pO2). Three studies [26,27,28] correlated pO2 readings with [18F]FMISO hypoxia (in a total of 58 patients) and all found a strong correlation. Given that oxygen electrodes are considered the gold standard for detecting intratumoural hypoxia, these results are promising in validating [18F]FMISO PET as a means of detecting hypoxia. They do not, however, provide a practical representative biomarker of [18F]FMISO hypoxia as oxygen electrode measurement is an invasive procedure which requires directly accessible tumours and cannot be used in a routine clinical setting.
Hypoxic gene signatures [29,30,31] refer to a collection of genes whose expression is upregulated or downregulated in response to hypoxia. They can be measured from a tumour biopsy specimen and are thought to represent the hypoxic phenotype of the overall tumour. Signatures are able to prognosticate in HNC [32] and also predict the benefit of hypoxia modification therapy in HNC [30]. To date, there is only one published study [9] analysing the relationship between hypoxia gene expression and [18F]FMISO uptake in a cohort of 42 HNC patients treated with radiotherapy. Correlations were assessed at baseline and at different time points during radiotherapy. There was a weak association between hypoxic gene signatures and [18F]FMISO uptake at baseline (r = 0.20) which increased at weeks 1 (r = 0.38) and 2 (r = 0.43) during radiotherapy.
The final study [33] in Table 2 investigated the association between [18F]FMISO PET imaging and plasma hypoxia markers (osteopontin, vascular endothelial growth factor (VEGF), galectin-3 and circulating tumour growth factor (CTGF)). The most promising result was obtained with serum osteopontin, a protein whose plasma concentration has been shown to increase in conditions of tumour hypoxia [33]. There was a moderate correlation between osteopontin levels and the baseline hypoxic volume (r = 0.579), and residual hypoxia on [18F]FMISO PET imaging (p < 0.05) during treatment. Of note, osteopontin has been shown to inversely correlate with pO2 in HNC and also to prognosticate and predict benefit from hypoxia modification therapy in HNC [34]. Given that it is easily obtained by a blood test, it could potentially be an ideal ‘screening’ biomarker to select patients who would benefit from [18F]FMISO PET, but further studies are required to validate this concept.
Correlation of [18F]FMISO PET with other imaging modalities
Correlation with 18F-FDG PET
18F-FDG PET is a routine investigation for many newly diagnosed HNC patients and hence it is convenient to assess correlation with [18F]FMISO PET. 18F-FDG PET provides assessment of glycolysis in tissue, which is a process affected by hypoxia [35]. HIF1α (activated in areas of low oxygen) upregulates both glucose transporters (GLUTs) and glycolytic enzymes [36], and therefore it is conceivable that 18F-FDG PET could be a surrogate marker of hypoxia. Table 3 details the studies correlating 18F-FDG and [18F]FMISO PET. The majority of these studies showed a weak to moderate correlation between the two imaging modalities [8, 13, 26, 28, 35, 37,38,39], one showing no association between 18F-FDG and [18F]FMISO PET [40], and two a strong association (r = 0.81) [41, 42]. Two other studies [41, 43] that demonstrated a strong relationship used ‘second order’ features on 18F-FDG PET; one looked at ‘total lesion glycolysis’ (SUVmean multiplied by metabolic tumour volume on 18F-FDG PET) and found a correlation coefficient of 0.85 with ‘total lesion hypoxia’ (SUVmean multiplied by hypoxic volume) on [18F]FMISO PET. The other study [43], used a radiomics signature from the CT, and found that this, in combination with 18F-FDG PET, improved the ability to predict for hypoxia on [18F]FMISO PET (with an area under the curve (AUC) of 0.83). In contrast, Kroenke et al. [38] used ‘texture analysis’ of the tumour on 18F-FDG PET and found that this did not improve the ability of 18F-FDG PET to predict [18F]FMISO uptake.
The outcomes from these studies do not support the use of 18F-FDG PET to select which patients should undergo 18F-FMISO PET for subsequent hypoxia imaging to delineate a hypoxic target volume for radiotherapy dose adaptation.
Correlation with MRI
In recent years, attention has turned to multiparametric MRI (mpMRI) and its ability to provide information about tissue perfusion (dynamic contrast enhanced/DCE-MRI), cellularity (diffusion weighted imaging/DWI-MRI), and oxygenation (transverse relaxation time/T2*MRI).
These are all processes central to the development of tumour hypoxia. The six studies which have compared mpMRI with [18F]FMISO PET are summarised in Table 4. Two studies [44, 45] identified a relationship between DCE-MRI and [18F]FMISO uptake, with reduced Ktrans (a measure of perfusion) in the hypoxic volume. Data on ADC are conflicting, with both decreased [46] and increased [47, 48] values being reported in the hypoxic volume. Of these modalities, T2* MRI is the most direct marker of hypoxia, as it measures the concentration of deoxygenated haemoglobin. The study which compared T2* MRI to [18F]FMISO PET [42] did not find a correlation, which again can be explained by the fact that they measure different processes; blood oxygenation versus intracellular oxygenations. MRI has the benefit of higher resolution compared to PET and would be ideal to identify tumour hypoxia for radiotherapy planning, but currently we do not have sufficient evidence to propose it for this role.
Is [18F]FMISO imaging repeatable and reproducible?
Studies repeating [18F]FMISO PET at baseline.
Three studies [49,50,51] repeated [18F]FMISO PET scans within a short time frame (2–3 days) of each other (without interval treatment) to assess repeatability. They are described in Table 5. Okamoto et al. [50] demonstrated that [18F]FMISO imaging is highly repeatable and that the maximum uptake location of [18F]FMISO varied by only 4 mm between two repeat scans. Lin [49] and Nehmeh et al. [51] also reported similar hypoxic volumes in ~ 50% of their patients, although there was a significant variation in the location of tumour hypoxia in the other half of patients. The proposed explanation is that [18F]FMISO captures both acute and chronic hypoxia [51], and so stable uptake may be representative of chronic hypoxia only. Although patient numbers in these studies were small (7–14), the findings lend caution to the concept of dose escalating to a hypoxic volume generated from a single [18F]FMISO PET study in a patient. This is well displayed in the study by Lin et al. [49] (a dose planning study), which showed a decrease in the prescribed uniform dose to the hypoxic volume of up to 12 Gy, between two serials scans (which were separated by 3 days), due to instability of the hypoxic region.
Studies repeating [18F]FMISO PET during radiotherapy treatment
Several studies interrogated hypoxia dynamics during radiotherapy treatment and are displayed in Table 6. All the studies showed that in the majority of patients, reoxygenation occurs and the degree of hypoxia, measured by [18F]FMISO PET, reduces through the course of treatment. These findings suggest that hypoxia observed on a single, pre-treatment, scan may not be sufficiently representative to guide treatment adaptation and serial scans ought to be considered when designing clinical studies of hypoxia guided dose escalation/adaptation Interestingly, although several studies comment on ‘residual’ hypoxia during treatment, only two formally reported on the geographical stability of the hypoxic volume [52, 53]. Bittner et al. [52] found a 72% overlap of the hypoxic volume from week 0 to week 2, suggesting that ‘residual hypoxia’ is an appropriate term. In contrast, Carles et al. [53] looked at spatial variation of hypoxia and found that only 24% of patients had geographically ‘stable’ hypoxia throughout their treatment, and that these patients had a better prognosis in terms of locoregional control. The other studies did not report on the geographical location of the hypoxic region during radiotherapy treatment.
Where do locoregional recurrences occur in relation to the initial hypoxic volume?
Despite the wealth of published studies on [18F]FMISO PET in HNC, only four were identified which correlated recurrence patterns to the initial hypoxic volume (see Table 7). From these, one study [54] concluded that recurrences arise from the original hypoxic subvolumes, with a median overlap of 42% between recurrence volume and the initial hypoxic volume. Two studies [11, 55] showed that a significant proportion of recurrences (33–50%) occur outside the pretreatment hypoxic volume. Nishikawa et al. [56] analysed pretreatment [18F]FMISO PET images from 21 patients with nasopharyngeal carcinoma (of whom nine recurred) to generate a risk model. They found that within the imaged tumour region, voxels with [18F]FMISO tumour to muscle ratio (TMR) > 2.42 predicted a recurrence rate of 30% within the same voxel. The AUC for this prediction model was only 0.59 however, and the authors concluded that the predictive value of pretreatment [18F]FMISO PET was insufficient for up-front dose escalation to the regions with high uptake, i.e. the hypoxic volume.
Overall, these findings suggest that although hypoxia is a known cause of radioresistance, there is not enough evidence to suggest that recurrences arise from the hypoxic regions identified on pretreatment imaging, especially when determined from a single scan. It should be noted, however, that the recurrence data stem from a total of only 70 patients, across 4 studies. Further knowledge is therefore required on disease recurrence and its relation to hypoxic volumes.
What have we learned so far from dose modification studies?
Given that the hypoxic uptake on [18F]FMISO PET carries important prognostic information [16], trials are underway to determine if radiotherapy can be dose de-escalated for patients with a good prognosis (absence or early resolution of hypoxia) and conversely escalated for patients with hypoxic tumours. So far 3 dose modification trials using [18F]FMISO PET as a biomarker have been published; see Table 8.
Dose de-escalation studies
The first [18F]FMISO de-escalation study was published in 2016 [19] on 33 patients with human papilloma virus (HPV)-positive oropharyngeal cancer. The radiotherapy dose to the metastatic lymph nodes was reduced by 10 Gy to 60 Gy in patients who had resolution of hypoxia at week one of radiotherapy. Ten patients had their radiotherapy dose de-escalated and remained recurrence free at two years. The second de-escalation study [57] was in a cohort of 19 HPV-positive oropharyngeal cancer patients who were treated with resection of the primary tumour and radiotherapy to the nodes followed four months later by a neck dissection. The radiotherapy dose was reduced to 30 Gy in 15 patients who had no hypoxia at either pre- or intra-treatment [18F]FMISO PET imaging. Eleven of the 15 patients had a pathological complete response. As these were pilot studies, neither had a comparative cohort in which patients received radiotherapy dose de-escalation despite hypoxia on PET. Given that the tumours were HPV-positive, it is possible their outcomes would have still been favourable, despite the observed hypoxia on PET.
A larger scale de-escalation study (clinical trial identifier NCT03323463; n = 300) at Memorial Sloane Kettering is currently underway using [18F]FMISO PET to select patients to receive a de-escalated dose of radiation (30 Gy) if no hypoxia is observed on pre/intra-treatment imaging. In this study, all patients will receive two cycles of concomitant chemotherapy and surgical resection is no longer mandatory. The results from this trial will help determine if it is safe to deescalate radiation dose in non-hypoxic tumours. However, this trial will not determine if it is the absence of hypoxia (on [18F]FMISO PET) that renders the patients suitable for treatment de-escalation as no randomisation to standard treatment vs. de-escalation is planned.
Dose escalation trial
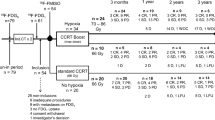
So far one randomized phase II study has been published [58], which looked at dose escalation to the hypoxic volume alone on [18F]FMISO PET. Patients with a hypoxic volume pretreatment were randomised to receive standard chemoRT (70 Gy in 35 fractions) or escalation of up to 10% with 77 Gy to the hypoxic volume only. The trial closed prematurely due to slow accrual (53 patients over 8 years). Thirty-nine patients had hypoxic tumours, of whom 19 received dose-escalation. The authors reported a non-significant improvement of 25% in local control for the dose escalation arm. Furthermore, of the patients treated with dose escalation, only a 2% mean elevation of radiotherapy dose was achieved, rather than the planned 10%. This trial highlights the difficulties of carrying out large-scale prospective imaging trials with [18F]FMISO. One of the reasons given for poor recruitment was scanner and tracer availability. In addition, the modest 2% dose escalation is much smaller than the 10% frequently quoted in planning studies and highlights the need to use real life patient data.
Conclusion
Hypoxia PET imaging has been proposed for many years as a potential method to specifically target hypoxic tumour regions with higher doses of radiotherapy to improve outcomes. The results of our review are mixed, and whilst some findings support the use of [18F]FMISO PET, a number of challenges are identified:
-
(1)
A number of studies have looked at the correlation between [18F]FMISO PET and other hypoxia biomarkers and, overall, the most promising results were found with tumour HIF1α and serum osteopontin. It should be noted that hypoxia is an umbrella term referring to different biological processes on different assays, i.e., intracellular hypoxia versus interstitial and blood hypoxia, or acute versus chronic hypoxia. As such, the different hypoxia biomarkers described should not necessarily be expected to correlate with each other. Currently, there is no clinically deliverable surrogate biomarker to predict for the [18F]FMISO hypoxic phenotype and that would enable patient selection for [18F]FMISO imaging. This is a significant barrier as the routine use of [18F]FMISO PET scans in all locally advanced HNC patients is hampered by cost and availability.
-
(2)
The results of [18F]FMISO PET imaging are not necessarily repeatable and the location of uptake may vary during treatment. This highlights that hypoxia is a dynamic phenomenon and a single snapshot [18F]FMISO PET imageis unlikely to provide all the information required for radiotherapy dose modification. Some of the presented studies suggest that maybe radiotherapy adaptation should be based on residual hypoxia after the initiation of radiotherapy treatment, at weeks 1–2.
-
(3)
Tumour recurrences do not necessarily occur within the pretreatment hypoxic volume on [18F]FMISO PET. Only a few studies have looked at recurrence patterns with regard to the FMISO hypoxic volume pre-treatment. Future work is needed in this area, both with reference to pre-treatment and intra-treatment scans.
-
(4)
Dose modification studies published thus far are pilot studies and, therefore, do not provide sufficient evidence about the efficacy of dose painting or modification based on [18F]FMISO PET imaging. The de-escalation studies have not proved that it was the absence of hypoxia on [18F]FMISO PET which made treatment de-escalation safe. Furthermore, the single dose escalation study illustrated the challenges of carrying out [18F]FMISO PET in a large-scale trial and the difficulties for dose escalation in real-world patients.
In summary, [18F]FMISO PET has been extensively investigated in HNC addressing various research questions. Pre-treatment uptake has been shown to relate to prognosis in HNC patients treated with radiotherapy, highlighting the clinical importance and relevance of hypoxia denoted on [18F]FMISO PET. Planning studies have demonstrated that it is technically feasible to escalate the radiotherapy dose to hypoxic regions, without exceeding normal tissue tolerance doses. The positive correlation with other hypoxia biomarkers (in particular oxygen electrodes) validate [18F]FMISO PET as a reliable means of detecting intra tumoral hypoxia.
The findings from this review suggest, however, that there is insufficient evidence to support dose escalation to a hypoxic region using a single pretreatment scan and further work is required to identify if residual hypoxia would be more appropriate to guide radiotherapy dose escalation. Cost and access to [18F]FMISO PET remain an issue, especially for patients on a curative chemoradiotherapy treatment pathway for whom additional investigations need to be easily accessible and carried out promptly to avoid treatment delay. If dose escalation is to be investigated as a management strategy to overcome radioresistance, then currently [18F]FDG PET or MRI are more accessible and less costly options to delineate the target volume. The studies included in this review were based on HNC but the findings could potentially be extrapolated to other tumour sites as many of the issues mentioned are related to the biology of hypoxia and the different assays used to measure it.
References
Isa AY, Ward TH, West CM, Slevin NJ, Homer JJ (2006) Hypoxia in head and neck cancer. Br J Radiol 79:791–798. https://doi.org/10.1259/bjr/17904358
Hockel M, Schlenger K, Aral B, Mitze M, Schaffer U, Vaupel P (1996) Association between tumor hypoxia and malignant progression in advanced cancer of the uterine cervix. Cancer Res 56:4509–4515
Rwigema JC, Heron DE, Ferris RL, Andrade RS, Gibson MK, Yang Y et al (2011) The impact of tumor volume and radiotherapy dose on outcome in previously irradiated recurrent squamous cell carcinoma of the head and neck treated with stereotactic body radiation therapy. Am J Clin Oncol 34:372–379. https://doi.org/10.1097/COC.0b013e3181e84dc0
Leeman JE, Li JG, Pei X, Venigalla P, Zumsteg ZS, Katsoulakis E et al (2017) Patterns of treatment failure and postrecurrence outcomes among patients with locally advanced head and neck squamous cell carcinoma after chemoradiotherapy using modern radiation techniques. JAMA Oncol 3:1487–1494. https://doi.org/10.1001/jamaoncol.2017.0973
Gray LH, Conger AD, Ebert M, Hornsey S, Scott OC (1953) The concentration of oxygen dissolved in tissues at the time of irradiation as a factor in radiotherapy. Br J Radiol 26:638–648. https://doi.org/10.1259/0007-1285-26-312-638
Hendrickson K, Phillips M, Smith W, Peterson L, Krohn K, Rajendran J (2011) Hypoxia imaging with [F-18] FMISO-PET in head and neck cancer: potential for guiding intensity modulated radiation therapy in overcoming hypoxia-induced treatment resistance. Radiother Oncol 101:369–375. https://doi.org/10.1016/j.radonc.2011.07.029
Bittner MI, Wiedenmann N, Bucher S, Hentschel M, Mix M, Rücker G et al (2016) Analysis of relation between hypoxia PET imaging and tissue-based biomarkers during head and neck radiochemotherapy. Acta Oncol 55:1299–1304. https://doi.org/10.1080/0284186x.2016.1219046
Norikane T, Yamamoto Y, Maeda Y, Kudomi N, Matsunaga T, Haba R et al (2014) Correlation of (18)F-fluoromisonidazole PET findings with HIF-1α and p53 expressions in head and neck cancer: comparison with (18)F-FDG PET. Nucl Med Commun 35:30–35. https://doi.org/10.1097/MNM.0000000000000010
Löck S, Linge A, Seidlitz A, Bandurska-Luque A, Nowak A, Gudziol V et al (2019) Repeat FMISO-PET imaging weakly correlates with hypoxia-associated gene expressions for locally advanced HNSCC treated by primary radiochemotherapy. Radiother Oncol 135:43–50. https://doi.org/10.1016/j.radonc.2019.02.020
Tachibana I, Nishimura Y, Hanaoka K, Inada M, Fukuda K, Tatebe H et al (2018) Tumor Hypoxia Detected by (18)F-fluoromisonidazole Positron Emission Tomography (FMISO PET) as a Prognostic Indicator of Radiotherapy (RT). Anticancer Res 38:1775–1781. https://doi.org/10.21873/anticanres.12415
Zschaeck S, Haase R, Abolmaali N, Perrin R, Stützer K, Appold S et al (2015) Spatial distribution of FMISO in head and neck squamous cell carcinomas during radio-chemotherapy and its correlation to pattern of failure. Acta Oncol 54:1355–1363. https://doi.org/10.3109/0284186x.2015.1074720
Eschmann SM, Paulsen F, Bedeshem C, Machulla H-J, Hehr T, Bamberg M et al (2007) Hypoxia-imaging with 18F-misonidazole and PET: changes of kinetics during radiotherapy of head-and-neck cancer. Radiother Oncol 83:406–410. https://doi.org/10.1016/j.radonc.2007.05.014
Sato J, Kitagawa Y, Watanabe S, Asaka T, Ohga N, Hirata K et al (2017) (18)F-Fluoromisonidazole positron emission tomography (FMISO-PET) may reflect hypoxia and cell proliferation activity in oral squamous cell carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol 124:261–270. https://doi.org/10.1016/j.oooo.2017.05.506
Kikuchi M, Yamane T, Shinohara S, Fujiwara K, Hori SY, Tona Y et al (2011) 18F-fluoromisonidazole positron emission tomography before treatment is a predictor of radiotherapy outcome and survival prognosis in patients with head and neck squamous cell carcinoma. Ann Nucl Med 25:625–633. https://doi.org/10.1007/s12149-011-0508-9
Rajendran JG, Schwartz DL, O’Sullivan J, Peterson LM, Ng P, Scharnhorst J et al (2006) Tumor hypoxia imaging with [F-18] fluoromisonidazole positron emission tomography in head and neck cancer. Clin Cancer Res 12:5435–5441. https://doi.org/10.1158/1078-0432.Ccr-05-1773
Zschaeck S, Löck S, Hofheinz F, Zips D, Saksø Mortensen L, Zöphel K et al (2020) Individual patient data meta-analysis of FMISO and FAZA hypoxia PET scans from head and neck cancer patients undergoing definitive radio-chemotherapy. Radiother Oncol 149:189–196. https://doi.org/10.1016/j.radonc.2020.05.022
Michaelidou A, Adjogatse D, Suh Y, Pike L, Thomas C, Woodley O et al (2021) 18F-FDG-PET in guided dose-painting with intensity modulated radiotherapy in oropharyngeal tumours: a phase I study (FiGaRO). Radiother Oncol 155:261–268. https://doi.org/10.1016/j.radonc.2020.10.039
Nutting CM, Griffin CL, Sanghera P, Foran B, Beasley M, Bernstein D et al (2021) Dose-escalated intensity-modulated radiotherapy in patients with locally advanced laryngeal and hypopharyngeal cancers: ART DECO, a phase III randomised controlled trial. Eur J Cancer 153:242–256. https://doi.org/10.1016/j.ejca.2021.05.021
Lee N, Schoder H, Beattie B, Lanning R, Riaz N, McBride S et al (2016) Strategy of using intratreatment hypoxia imaging to selectively and safely guide radiation dose de-escalation concurrent with chemotherapy for locoregionally advanced human papillomavirus-related oropharyngeal carcinoma. Int J Radiat Oncol Biol Phys 96:9–17. https://doi.org/10.1016/j.ijrobp.2016.04.027
Henriques de Figueiredo B, Zacharatou C, Galland-Girodet S, Benech J, De Clermont-Gallerande H, Lamare F et al (2015) Hypoxia imaging with [18F]-FMISO-PET for guided dose escalation with intensity-modulated radiotherapy in head-and-neck cancers. Strahlenther Onkol 191:217–224. https://doi.org/10.1007/s00066-014-0752-8
Koh WJ, Rasey JS, Evans ML, Grierson JR, Lewellen TK, Graham MM et al (1992) Imaging of hypoxia in human tumors with [F-18]fluoromisonidazole. Int J Radiat Oncol Biol Phys 22:199–212. https://doi.org/10.1016/0360-3016(92)91001-4
Loncaster JA, Harris AL, Davidson SE, Logue JP, Hunter RD, Wycoff CC et al (2001) Carbonic anhydrase (CA IX) expression, a potential new intrinsic marker of hypoxia: correlations with tumor oxygen measurements and prognosis in locally advanced carcinoma of the cervix. Cancer Res 61:6394–6399
Chen L, Zhang Z, Kolb HC, Walsh JC, Zhang J, Guan Y (2012) 18F-HX4 hypoxia imaging with PET/CT in head and neck cancer: a comparison with 18F-FMISO. Nucl Med Commun 33:1096–1102. https://doi.org/10.1097/MNM.0b013e3283571016
Nicolay NH, Wiedenmann N, Mix M, Weber WA, Werner M, Grosu AL et al (2020) Correlative analyses between tissue-based hypoxia biomarkers and hypoxia PET imaging in head and neck cancer patients during radiochemotherapy-results from a prospective trial. Eur J Nucl Med Mol Imaging 47:1046–1055. https://doi.org/10.1007/s00259-019-04598-9
Kunder S, Chatterjee A, Manna S, Mahimkar M, Patil A, Rangarajan V et al (2021) Correlation between imaging and tissue biomarkers of hypoxia in squamous cell cancer of the head and neck. World J Nucl Med 20:228–236. https://doi.org/10.4103/wjnm.WJNM_91_20
Gagel B, Piroth M, Pinkawa M, Reinartz P, Zimny M, Kaiser HJ et al (2007) pO polarography, contrast enhanced color duplex sonography (CDS), [18F] fluoromisonidazole and [18F] fluorodeoxyglucose positron emission tomography: validated methods for the evaluation of therapy-relevant tumor oxygenation or only bricks in the puzzle of tumor hypoxia? BMC Cancer 7:113. https://doi.org/10.1186/1471-2407-7-113
Gagel B, Reinartz P, Dimartino E, Zimny M, Pinkawa M, Maneschi P et al (2004) pO(2) Polarography versus positron emission tomography ([(18)F] fluoromisonidazole, [(18)F]-2-fluoro-2’-deoxyglucose). An appraisal of radiotherapeutically relevant hypoxia. Strahlenther Onkol 180:616–622. https://doi.org/10.1007/s00066-004-1229-y
Zimny M, Gagel B, DiMartino E, Hamacher K, Coenen HH, Westhofen M et al (2006) FDG–a marker of tumour hypoxia? a comparison with [18F]fluoromisonidazole and pO2-polarography in metastatic head and neck cancer. Eur J Nucl Med Mol Imaging 33:1426–1431. https://doi.org/10.1007/s00259-006-0175-6
Eustace A, Mani N, Span PN, Irlam JJ, Taylor J, Betts GN et al (2013) A 26-gene hypoxia signature predicts benefit from hypoxia-modifying therapy in laryngeal cancer but not bladder cancer. Clin Cancer Res 19:4879–4888. https://doi.org/10.1158/1078-0432.Ccr-13-0542
Toustrup K, Sørensen BS, Nordsmark M, Busk M, Wiuf C, Alsner J et al (2011) Development of a hypoxia gene expression classifier with predictive impact for hypoxic modification of radiotherapy in head and neck cancer. Cancer Res 71:5923–5931. https://doi.org/10.1158/0008-5472.Can-11-1182
Lendahl U, Lee KL, Yang H, Poellinger L (2009) Generating specificity and diversity in the transcriptional response to hypoxia. Nat Rev Genet 10:821–832. https://doi.org/10.1038/nrg2665
Winter SC, Buffa FM, Silva P, Miller C, Valentine HR, Turley H et al (2007) Relation of a hypoxia metagene derived from head and neck cancer to prognosis of multiple cancers. Cancer Res 67:3441–3449. https://doi.org/10.1158/0008-5472.Can-06-3322
Rühle A, Grosu AL, Wiedenmann N, Ruf J, Bieber B, Stoian R et al (2022) The value of plasma hypoxia markers for predicting imaging-based hypoxia in patients with head-and-neck cancers undergoing definitive chemoradiation. Clin Transl Radiat Oncol 33:120–127. https://doi.org/10.1016/j.ctro.2022.02.008
Overgaard J, Eriksen JG, Nordsmark M, Alsner J, Horsman MR (2005) Plasma osteopontin, hypoxia, and response to the hypoxia sensitiser nimorazole in radiotherapy of head and neck cancer: results from the DAHANCA 5 randomised double-blind placebo-controlled trial. Lancet Oncol 6:757–764. https://doi.org/10.1016/S1470-2045(05)70292-8
Rajendran JG, Mankoff DA, O’Sullivan F, Peterson LM, Schwartz DL, Conrad EU et al (2004) Hypoxia and glucose metabolism in malignant tumors: evaluation by [18F]fluoromisonidazole and [18F]fluorodeoxyglucose positron emission tomography imaging. Clin Cancer Res 10:2245–2252. https://doi.org/10.1158/1078-0432.ccr-0688-3
Zhao S, Kuge Y, Mochizuki T, Takahashi T, Nakada K, Sato M et al (2005) Biologic correlates of intratumoral heterogeneity in 18F-FDG distribution with regional expression of glucose transporters and hexokinase-II in experimental tumor. J Nucl Med 46:675–682
Mönnich D, Thorwarth D, Leibfarth S, Pfannenberg C, Reischl G, Mauz PS et al (2017) Overlap of highly FDG-avid and FMISO hypoxic tumor subvolumes in patients with head and neck cancer. Acta Oncol 56:1577–1582. https://doi.org/10.1080/0284186x.2017.1363910
Kroenke M, Hirata K, Gafita A, Watanabe S, Okamoto S, Magota K et al (2019) Voxel based comparison and texture analysis of 18F-FDG and 18F-FMISO PET of patients with head-and-neck cancer. PLoS ONE 14:e0213111. https://doi.org/10.1371/journal.pone.0213111
Nehmeh SA, Moussa MB, Lee N, Zanzonico P, Gönen M, Humm JL et al (2021) Comparison of FDG and FMISO uptakes and distributions in head and neck squamous cell cancer tumors. EJNMMI Res 11:38. https://doi.org/10.1186/s13550-021-00767-w
Thorwarth D, Eschmann SM, Holzner F, Paulsen F, Alber M (2006) Combined uptake of [18F]FDG and [18F]FMISO correlates with radiation therapy outcome in head-and-neck cancer patients. Radiother Oncol 80:151–156. https://doi.org/10.1016/j.radonc.2006.07.033
Cegla P, Kazmierska J, Gwozdz S, Czepczynski R, Malicki J, Cholewinski W (2020) Assessment of biological parameters in head and neck cancer based on in vivo distribution of (18)F-FDG-FLT-FMISO-PET/CT images. Tumori 106:33–38. https://doi.org/10.1177/0300891619868012
Wiedenmann N, Bunea H, Rischke HC, Bunea A, Majerus L, Bielak L et al (2018) Effect of radiochemotherapy on T2* MRI in HNSCC and its relation to FMISO PET derived hypoxia and FDG PET. Radiat Oncol 13:159. https://doi.org/10.1186/s13014-018-1103-1
Crispin-Ortuzar M, Apte A, Grkovski M, Oh JH, Lee NY, Schöder H et al (2018) Predicting hypoxia status using a combination of contrast-enhanced computed tomography and [(18)F]-Fluorodeoxyglucose positron emission tomography radiomics features. Radiother Oncol 127:36–42. https://doi.org/10.1016/j.radonc.2017.11.025
Jansen JF, Schöder H, Lee NY, Wang Y, Pfister DG, Fury MG et al (2010) Noninvasive assessment of tumor microenvironment using dynamic contrast-enhanced magnetic resonance imaging and 18F-fluoromisonidazole positron emission tomography imaging in neck nodal metastases. Int J Radiat Oncol Biol Phys 77:1403–1410. https://doi.org/10.1016/j.ijrobp.2009.07.009
Simoncic U, Leibfarth S, Welz S, Schwenzer N, Schmidt H, Reischl G et al (2017) Comparison of DCE-MRI kinetic parameters and FMISO-PET uptake parameters in head and neck cancer patients. Med Phys 44:2358–2368. https://doi.org/10.1002/mp.12228
Wiedenmann N, Grosu AL, Büchert M, Rischke HC, Ruf J, Bielak L et al (2020) The utility of multiparametric MRI to characterize hypoxic tumor subvolumes in comparison to FMISO PET/CT. Consequences for diagnosis and chemoradiation treatment planning in head and neck cancer. Radiother Oncol 150:128–135. https://doi.org/10.1016/j.radonc.2020.06.013
Shima T, Fujima N, Yamano S, Kudo K, Hirata K, Minowa K (2020) Evaluation of non-Gaussian model-based diffusion-weighted imaging in oral squamous cell carcinoma: comparison with tumour functional information derived from positron-emission tomography. Clin Radiol 75:397.e15-e21. https://doi.org/10.1016/j.crad.2019.12.018
Gouel P, Callonnec F, Obongo-Anga FR, Bohn P, Lévêque E, Gensanne D et al (2023) Quantitative MRI to characterize hypoxic tumors in comparison to FMISO PET/CT for radiotherapy in oropharynx cancers. Cancers (Basel). 15:1918. https://doi.org/10.3390/cancers15061918
Lin Z, Mechalakos J, Nehmeh S, Schoder H, Lee N, Humm J et al (2008) The influence of changes in tumor hypoxia on dose-painting treatment plans based on 18F-FMISO positron emission tomography. Int J Radiat Oncol Biol Phys 70:1219–1228. https://doi.org/10.1016/j.ijrobp.2007.09.050
Okamoto S, Shiga T, Yasuda K, Ito YM, Magota K, Kasai K et al (2013) High reproducibility of tumor hypoxia evaluated by 18F-fluoromisonidazole PET for head and neck cancer. J Nucl Med 54:201–207. https://doi.org/10.2967/jnumed.112.109330
Nehmeh SA, Lee NY, Schröder H, Squire O, Zanzonico PB, Erdi YE et al (2008) Reproducibility of intratumor distribution of (18)F-fluoromisonidazole in head and neck cancer. Int J Radiat Oncol Biol Phys 70:235–242. https://doi.org/10.1016/j.ijrobp.2007.08.036
Bittner MI, Wiedenmann N, Bucher S, Hentschel M, Mix M, Weber WA et al (2013) Exploratory geographical analysis of hypoxic subvolumes using 18F-MISO-PET imaging in patients with head and neck cancer in the course of primary chemoradiotherapy. Radiother Oncol 108:511–516. https://doi.org/10.1016/j.radonc.2013.06.012
Carles M, Fechter T, Grosu AL, Sörensen A, Thomann B, Stoian RG et al (2021) (18)F-FMISO-PET hypoxia monitoring for head-and-neck cancer patients: radiomics analyses predict the outcome of chemo-radiotherapy. Cancers (Basel) 13:3449. https://doi.org/10.3390/cancers13143449
Boeke S, Thorwarth D, Mönnich D, Pfannenberg C, Reischl G, La Fougère C et al (2017) Geometric analysis of loco-regional recurrences in relation to pre-treatment hypoxia in patients with head and neck cancer. Acta Oncol 56:1571–1576. https://doi.org/10.1080/0284186x.2017.1372626
Dirix P, Vandecaveye V, De Keyzer F, Stroobants S, Hermans R, Nuyts S (2009) Dose painting in radiotherapy for head and neck squamous cell carcinoma: value of repeated functional imaging with (18)F-FDG PET, (18)F-fluoromisonidazole PET, diffusion-weighted MRI, and dynamic contrast-enhanced MRI. J Nucl Med 50:1020–1027. https://doi.org/10.2967/jnumed.109.062638
Nishikawa Y, Yasuda K, Okamoto S, Ito YM, Onimaru R, Shiga T et al (2017) Local relapse of nasopharyngeal cancer and Voxel-based analysis of FMISO uptake using PET with semiconductor detectors. Radiat Oncol 12:148. https://doi.org/10.1186/s13014-017-0886-9
Riaz N, Sherman E, Pei X, Schöder H, Grkovski M, Paudyal R et al (2021) Precision radiotherapy: reduction in radiation for oropharyngeal cancer in the 30 ROC Trial. J Natl Cancer Inst 113:742–751. https://doi.org/10.1093/jnci/djaa184
Welz S, Paulsen F, Pfannenberg C, Reimold M, Reischl G, Nikolaou K et al (2022) Dose escalation to hypoxic subvolumes in head and neck cancer: A randomized phase II study using dynamic [(18)F]FMISO PET/CT. Radiother Oncol 171:30–36. https://doi.org/10.1016/j.radonc.2022.03.021
Lee N, Nehmeh S, Schöder H, Fury M, Chan K, Ling CC et al (2009) Prospective trial incorporating pre-/mid-treatment [18F]-misonidazole positron emission tomography for head-and-neck cancer patients undergoing concurrent chemoradiotherapy. Int J Radiat Oncol Biol Phys 75:101–108. https://doi.org/10.1016/j.ijrobp.2008.10.049
Okamoto S, Shiga T, Yasuda K, Watanabe S, Hirata K, Nishijima KI et al (2016) The reoxygenation of hypoxia and the reduction of glucose metabolism in head and neck cancer by fractionated radiotherapy with intensity-modulated radiation therapy. Eur J Nucl Med Mol Imaging 43:2147–2154. https://doi.org/10.1007/s00259-016-3431-4
Löck S, Perrin R, Seidlitz A, Bandurska-Luque A, Zschaeck S, Zöphel K et al (2017) Residual tumour hypoxia in head-and-neck cancer patients undergoing primary radiochemotherapy, final results of a prospective trial on repeat FMISO-PET imaging. Radiother Oncol 124:533–540. https://doi.org/10.1016/j.radonc.2017.08.010
Kazmierska J, Cholewinski W, Piotrowski T, Sowinska A, Bak B, Cegła P et al (2020) Assessment of tumour hypoxia, proliferation and glucose metabolism in head and neck cancer before and during treatment. Br J Radiol 93:20180781. https://doi.org/10.1259/bjr.20180781
Funding
For Professor Sally Barrington:This work was supported by the National Institute for Health and Care Research (NIHR) [RP-2016–07-001]. This work was also supported by core funding from the Wellcome/EPSRC Centre for Medical Engineering at King’s College London [WT203148/Z/16/Z]. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. For Dr Tim Witney: Funding was provided through a Wellcome Trust Senior Research Fellowship (220,221/Z/20/Z). For Dr Teresa Guerrero Urbano: This work was supported by the Radiation Research Unit at the Cancer Research UK City of London Centre Award [C7893/A28990].
Author information
Authors and Affiliations
Contributions
KS—literature search, literature review, manuscript writing, editing, and content planning. SFB—manuscript writing and editing. SEJC—manuscript writing and editing. THW—manuscript writing and editing. PJB—manuscript writing, editing, content planning. TGU—literature search, literature review, manuscript writing, editing. “All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by KS and TGU. The first draft of the manuscript was written by KS and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.”
Corresponding author
Ethics declarations
Conflict of interest
“The authors have no relevant financial or non-financial interests to disclose.”
Research involving human and animal participants
‘This article does not contain any studies with human or animal subjects performed by the any of the authors.’ ‘For the purpose of open access, the authors have applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission.’
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sambasivan, K., Barrington, S.F., Connor, S.E.J. et al. Is there a role for [18F]-FMISO PET to guide dose adaptive radiotherapy in head and neck cancer? A review of the literature. Clin Transl Imaging 12, 137–155 (2024). https://doi.org/10.1007/s40336-023-00607-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40336-023-00607-y