
Abstract
Introduction
The present web-based national survey aims to assess the clinician's perspective toward (1) the indications to perform positron emission tomography/computed tomography (PET/CT) in cancer patients, (2) the utility of the interaction with the referring nuclear medicine physician, and (3) their perception of the clarity, usefulness, and the impact of the PET/CT report.
Methods
We conducted a prospective web-based survey consisting of 31 multiple-choice questions and an open-text field. The questionnaire was administered to Italian clinicians or surgeons who managed oncological patients. Data were analyzed using standard diagrams and the values were expressed as numbers (percentages).
Results
A total of 373 physicians completed the questionnaire. Among the 360 responses finally included in the analysis, the majority came from radiation oncologists (46%), followed by oncologists. For half of the respondents (53%), indications to perform PET/CT examination were “often” clear and easily accessible, but only 16% considered them “absolutely” clear and accessible. Additionally, most respondents (43%) considered “absolutely” necessary to facilitate access to PET/CT indications and their update. The interaction with the referring nuclear medicine physician was generally useful and satisfying. Regarding the nuclear medicine report, 74% considered “absolutely” useful to standardize the report structure, and the presence of semi-quantitative parameters was considered of great importance. Finally, in about half of the cases (53%), PET/CT report impacts patient management with major changes.
Conclusion
To sum up, a “still not” complete confidence with PET/CT indications and the need to facilitate access to indications and their update emerged from our results. Moreover, a structured PET/CT report with a clarification on essential PET features is warranted. In this scenario, the participation of nuclear medicine physicians in guideline oncological committees, national and international oncological conferences as well as continuous training among all specialists involved in cancer patients’ management could be effective strategies to resolve clinicians' concerns about PET/CT, thereby improving the management of cancer patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In recent years, hybrid imaging has seen a continuous and steady evolution in terms of technological innovation, introduction of new radiopharmaceuticals, and clinical applications. In this scenario, positron emission tomography/computed tomography (PET/CT) has become an integral part of patient management, particularly in oncology [1]. Translating this powerful tool into routine, clinical practice depends on the consistency of national and international guidelines, on the correct multidisciplinary approach of patients, and on a clear understanding of imaging data within the scan report, which ultimately impacts clinical decision-making [2]. Given the growing body of evidence, PET/CT has now become integrated into numerous national and international oncological guidelines, and several data emerged on its potential applications even in settings outside of currently approved indications [3, 4]. However, its rapid development in terms of clinical indications, imaging protocols, and image interpretation, could create uncertainty about the proper application of PET/CT, leading to the need to assess the perceptions of referring physicians regarding the advantages and drawbacks of this technique. In 2012, Kurantanis et al. published the results of an international survey designed to investigate physicians' perceptions and experience regarding PET/CT indications in oncology, quality, and communication with nuclear physicians, showing a high percentage of uncertainty toward PET/CT [5]. From 2012 to date, literature data that can help us understand the evolution of clinicians’ doubts remain insufficient, especially in the national setting. Namely, physicians' confidence about the indications for performing PET/CT in oncological patients and perception of the nuclear report remain to be addressed. To note, the Italian National Healthcare system is based on Essential Levels of Assistance (the so-called LEA) provided by the National Health Service (Servizio Sanitario Nazionale—SSN) to all citizens and founded by public resources. In this system, the appropriates for a diagnostic PET/CT scan is established by the physicians who requested the examination [6]. Therefore, it becomes essential to be aware of the right indications and appropriateness of a PET/CT clinical request.
The present national web-based survey, developed by the Italian Association of Nuclear Medicine and Molecular Imaging (AIMN), aims to assess the clinicians’ perspective toward the indications to perform PET/CT in cancer patients, the utility of the interaction with the referring nuclear medicine physician, and the clinicians' perception of the clarity and usefulness of the PET/CT report.
Methods
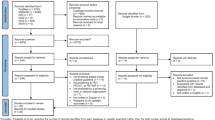
A web-based questionnaire was created by the Young AIMN Working Group and reviewed by the Oncology AIMN Working Group, which includes imaging experts, each with more than 10 years of experience. The questionnaire was structured into three sessions: 1) general demographic information on participants; 2) clinicians’ perspectives on oncological PET/CT indications; 3) clinicians’ perspectives on PET/CT report and relationship with the referring nuclear medicine physician. Finally, the questionnaire was placed in the Google Module consisting of 31 multiple-choice questions and an open-text field for general comments (Supplementary Material). The survey was, then, submitted to Italian physicians managing oncological patients. All subjects were invited to anonymously fill out the electronic form, and only the participants’ email addresses could be voluntarily recorded. On November 15, 2022, an invitation to participate was sent to all AIMN members from different Italian regions to facilitate diffusion to referring physicians at each center. To further increase potential responses, a letter of invitation to contribute was sent by the President of the AIMN (M.L.D.R.) to the Italian Association of Radiotherapy and Clinical Oncology (AIRO) with a request to share the questionnaire with AIRO members, which was then diffused on November 30, 2022, through the AIRO mailing list. The same request was sent to the Italian Association of Medical Oncology (AIOM). Two reminders were sent to the AIMN members within 27–55 days (December 12, 2022–January 9, 2023). The survey was closed on January 27, 2023, and thus ran for 10 weeks. Responses from physicians not involved in cancer care were excluded. The collected data were analyzed quantitatively by creating specific graphs and were expressed as number (percentage). Each result was deeply discussed.
Results
From 15/11/2022 (starting date) to 27/01/2023 (ending date) the survey received a total of 373 responses. Of the recipients who completed the questionnaire, 13 were not eligible for inclusion in the analysis (10 were nuclear medicine physicians and 3 were radiologists). Thus, 360 complete and eligible responses from as many participants were recorded and included in the final analysis.
Session 1: general information—demographics
Of the 360 participants, 46% (n = 165) were radiation oncologists, 25% (n = 90) oncologists, 8% (n = 28) hematologists, and 5% (n = 17) general surgeons. The remaining 16% (n = 60) presented with different backgrounds: 13 pneumologists, 10 thoracic surgeons, 9 gynecologists, 7 internal medicine physicians, 6 endocrinologists, 5 urologists, 2 palliative medicine clinicians, 2 plastic surgeons, 2 neurologists, 1 gastroenterologist, 1 geriatric specialist, 1 infectious disease specialist, and 1 ENT specialist (Fig. 1a). Most of the participants (n = 234, 65%) were between 30 and 60 years old, while among the 126 remaining, 111 (31%) were more than 50 years old, and 15 (4%) were less than 30 years old. Their length of experience with PET/CT imaging was < 5 years in 18% (n = 66) cases and between 5 and 10 years in other 24% (n = 84) cases, whereas the remaining 58% (n = 210) had more than 10 years of experience (Fig. 1b). Considering the geographical distribution, 52% (n = 187) were from the North of Italy, 28% (n = 102) from the South (including the Islands), and 20% (n = 71) from the Centre too. Moreover, 136 clinicians (38%) worked in a Public Hospital, 115 (32%) in a University Hospital, 88 (24%) in a Scientific Institute for Research, Hospitalization and Healthcare (IRCCS), and 21 (6%) in different private facilities (Fig. 1c). Regarding the availability of PET/CT per working center, 42% (n =152) of clinicians were sufficiently satisfied although increased availability is warranted, 37% (n =132) were always satisfied, 11% (n =39) were not satisfied at all for different causes, finally, 10% (n =37) declared the absence of PET/CT in own working center. PET/CT examinations were more frequently requested for patients between 40 and 60 years old (188, 52%), followed by 60–80 years old patients (166, 46%), and only 2% (n = 6) for patients under 40 years old (Fig. 2a). The elderly age did not represent a limitation to the PET/CT request for the great majority of clinicians (322, 89%), (Fig. 2b).

a–c Pie charts showing the main demographic characteristics of survey participants. Graph 1a shows a prevalence of responses from radiation oncologists. In addition, most participants reported having more than 10 years of work experience (1b). Finally, graph 1c shows the prevalence of respondents according to their working place

a, b The bar graphs show the patients’ age (range) for which the clinicians most frequently request a PET/CT scan (2a) and their confidence in prescribing a PET/CT scan to elderly patients (2b)
Session 2: perspective of current indications for the use of oncological PET/CT
First, recipients were surveyed about the reference guidelines for indicating PET/CT examination to oncological patients. Most clinicians (228, 63%) referred exclusively to the national or international oncological guidelines, such as AIOM or European Society for Medical Oncology (ESMO) guidelines, only 1% (n = 5) consulted exclusively nuclear medicine guidelines, while 23% (n = 81) reported consulting both. In contrast, 13% (n = 46) of participants did not refer to guidelines before prescribing, i.e., 35 respondents based their decision on their own clinical experience and 11 deferred the decision to the nuclear medicine physician. For half of the clinicians (191, 53%), information about PET/CT indications was “often” clear and easily accessible, but only 16% (n = 56) considered them “absolutely” clear and accessible (Fig. 3a). However, the level of confidence with PET/CT indications was globally high. Namely, most clinicians claimed to be “absolutely” (104, 29%) or “in most of the cases” (205, 57%) confident with PET/CT indications (Fig. 3b). Nevertheless, most respondents (155, 43%) considered “absolutely” necessary to facilitate access to PET/CT indications and their updating (Fig. 3c). More than half of the participants (202, 56%) stated that they had never referred to the European Association of Nuclear Medicine (EANM) guidelines before indicating the examination, whereas among the remaining 158 (44%) who confirmed that they had referred to EANM guidelines at least once, only 27/158 (17%) found them “absolutely” well-defined and established. When physicians were interviewed about the appropriate use of radiopharmaceuticals other than [18F]Fluorodeoxyglucose (FDG), in 71% (n = 257) of the cases the willingness to use different radiopharmaceuticals emerged, stating full confidence with their indications. To visualize the frequency of non-[18F]FDG radiopharmaceuticals used in clinical practice by 293/360 (81%) of the participants see the Supplementary Materials. Finally, uncertainty about the prescriptive or clinical appropriateness of PET/CT examination occurred “sometimes” in 54% (n = 193) and, in these cases, the doubt was “always” solved by consulting the referring nuclear medicine physicians in 62% (120/193) of cases (21% often, 8% sometimes, 5% rarely, 4% never solved). The whole sample responses as well as those of the two most representative specialists (radiation oncologists and oncologists) are shown in Figs. 3, 4.

a–c The bar graphs show the main results about clinicians’ perspective on oncological PET/CT indications with respect to the total of participants (blue bar), radiation oncologists (red bar), and oncologists (yellow bar) responses

a, b The bar graphs show the main results about clinicians’ perspective on oncological PET/CT indications/prescription (4a) and the relation with the referring nuclear medicine physician (4b) with respect to the total of participants (blue bar), radiation oncologists (red bar), and oncologists (yellow bar) responses
Session 3: clinician's perception of the nuclear medicine report
Almost all the clinicians surveyed (349, 97%) declared to read the whole text of the nuclear medicine report (not just the conclusions), and reading of the report is integrated with imaging review by 336 (93%) of the respondents (232 always, 70 in most of the cases, 34 sometimes). For 63% (n = 225) of participants, “in most of the cases” the nuclear medicine report addressed clinical question. In case of doubts about the report, most clinicians declared to refer to nuclear medicine physicians for clarification (186 always, 93 in most of the cases, 57 sometimes) and the interaction with the interpreting physician was considered helpful in most of the cases (214 always helpful, 104 almost always helpful, 25 sometimes helpful, 1 not helpful). Moreover, the experience of the interpreting physicians was considered of high importance (255 absolutely important, 97 very important, 8 sometimes important) (See supplementary materials).
When the clinicians were questioned about differences observed between reports from different nuclear medicine centers, 36% (n = 131), 31% (n = 112), and 22% (n = 79) observed differences in most of the cases, sometimes and always, respectively. Accordingly, the need to standardize the report structure was underlined by almost all the respondents (267 absolutely important, 70 often important, 15 sometimes important, 8 rarely important). The presence of semi-quantitative parameters (Standardized Uptake Value—SUV, SUVmax, etc.) in the report was considered “absolutely” and “very” important for 45% (n = 162) and 42% (n = 151) of the interviewed clinicians, respectively. Regarding the presence of a qualitative/quantitative score within the report, which is generally used to assess response to treatment (e.g., Deauville, PERCIST), the results showed a wide range of responses, underlining a discontinuous and non-standardized use of such scores (59 always reported, 102 reported in most of the cases, 84 sometimes reported, 81 rarely reported, and 34 never reported). In contrast, the comparison with the previous PET/CT examination was always reported in 78% (n = 282) of cases and it was considered always useful in the same percentage. For most of the interviewed clinicians, 62% (n = 222) resulted sufficiently satisfied by the waiting time (between 24 h and 1 week) to receive the final report. Finally, in about half of all cases (53%) the PET/CT report impacts the patient's management with major changes, in 25% with minor changes, and in 22% only partially. The main results about clinicians' perception of the nuclear medicine report with respect to the whole sample and the two most representative specialists’ respondents are shown in Fig. 5.

a, d The bar graphs show the main results about clinicians’ perspective on PET/CT report with respect to the total of participants (blue bar), radiation oncologists (red bar), and oncologists (yellow bar) responses. Chart 5a shows that most participants review the attached images in reading the report, especially radiation oncologists. The need to standardize the PET/CT report (5b), the importance of semi-quantitative parameters for the referring clinician (5c), and the impact of the PET/CT report on the management of the oncology patient (5d) were also pointed out
Discussion
To the best of our knowledge, this is the first national survey exploring clinicians’ perspectives on oncological PET/CT over the past 10 years. During the last decade, nuclear medical imaging has experienced progressive development in terms of technology and clinical applications. As confirmed by our results, the increasing number of PET/CT scanners across the country has led to covering the required needs, even if an over-increasing availability is warranted probably due to the growing applications in oncological and non-oncological patient work-up [7]. Currently, PET/CT is included in many oncological guidelines as an added value in the clinical-diagnostic pathway of patients, becoming essential in different clinical settings. In this evolving scenario, the clinician’s point of view plays a crucial role in understanding the real integration of PET/CT into clinical practice and how to continue to improve it.
The first interesting result of our survey concerns the not complete clarity on the indications for performing PET/CT in cancer patients. Namely, in half of the cases (53%), these are considered "often" clear and easily accessible, but only 16% of the participants consider them "absolutely" clear and accessible. This issue is not new. In 2012, Karantanis et al. [5] conducted an international web-based survey, highlighting referring physicians’ uncertainty about the appropriate use of PET/CT in oncology. Similarly, they showed that only 25.2% of the respondents felt that the indications for PET/CT were well-defined and established. However, compared with only 3.6% of clinicians who declared a high level of confidence with indications in the 2012 report, in the present analysis 29% of surveyed clinicians felt “absolutely” confident about when to indicate the examination.
Since almost all clinicians referred only to oncological guidelines to indicate PET/CT, it is clear that the inclusion of the nuclear physician in the scientific committee for the development of oncological guidelines is essential to clarify clinical doubts, to establish the exact time point for performing the diagnostic examination, and the most appropriate nuclear medicine technique for different settings and purposes. This finding underscores the great importance of the participation of nuclear medicine physicians in the national guideline committee, and generally in the multidisciplinary management of patients [8, 9]. In the national setting, the participation of the nuclear medicine physician in the oncological committee has also recently been established by the National Oncology Plan [10]. In this context, more efforts could be made by the nuclear medicine community to actively participate in national and international oncological meetings to better communicate to a larger audience about the essential role of PET in cancer patients’ management.
The reason why after 10 years some grades of uncertainty are still detectable among clinicians could be partially explained by the rapidly growing knowledge and data about PET/CT applications, but also by the difficulties in completely understanding the role of functional imaging by other specialists. For instance, the open question of our survey showed the request of some clinicians to provide more morphological details in the PET/CT report. This point raises an important issue regarding the exceptional need to improve training among nuclear medicine physicians but also among radiologists, who are often unaware or unwilling to recommend PET scans despite being aware of the limitations of structural imaging. Therefore, also considering the hybrid nature of PET/CT and the future improvement of PET/magnetic resonance imaging (MRI), hybrid residency training, as well as dedicated educational programs, could be proposed to overcome this point [11, 12]. In addition, the uncertainty about the prescriptive or clinical appropriateness of PET/CT examination can be solved through the consultation of the clinicians with the referring nuclear medicine physician, but also by considering multidisciplinary training as the cornerstone of future practice of medicine. Namely, continuous training among all specialists involved in cancer patients’ management could allow to achieve complete confidence with the functional imaging indications/prescriptions in routine clinical practice. In this scenario, the absolute need to facilitate access to PET/CT indications and their updating should be addressed, also considering the introduction of new radiopharmaceuticals in clinical practice and the progressive diffusion across the country.
Another remarkable issue concerns the standardization and harmonization of the nuclear medicine report. Recently, in 2019, another international web-based survey administered among radiologists and nuclear medicine physicians showed a broad variation in PET/CT reporting strategies adopted for oncological studies. Interestingly, the authors also pointed out a widespread lack of awareness of existing guidelines for PET/CT reporting [2]. The results of our survey confirmed the wide heterogeneity among PET/CT reports between different centers also in a single-nation investigation and the clinical physicians complains about the need to standardize the reports among different centers, speaking one common language. During the last decade, different efforts were made to standardize clinical report structures [13, 14]. In Italy, in 2014, the AIMN proposed a draft document (“LA REFERTAZIONE DELLA PET-TC ONCOLOGICA con [18F]FDG: istruzioni pratiche per un referto standardizzato e di qualità”) regarding the basic principles and the way to have a standardized report for [18F]FDG PET/CT [15]. Similarly, in 2021, a document to harmonize the report of [18F]FDG PET/CT in the specific setting of lymphomas was published to guide, more and more, PET/CT reporting in this setting of patients [16]. More recently the “E-PSMA: the EANM standardized reporting guidelines v1.0 for PSMA-PET” by EANM has seen the light to uniform the report for PSMA PET/CT in prostate cancer patients [17]. However, translation into clinical practice requires additional efforts by the entire nuclear medicine community.
Clinicians, above all radiation oncologists and oncologists, deem essential and useful the inclusion of semi-quantitative parameters within the report of PET/CT. This issue has been debated for a long time. The need for a simple and objective metabolic parameter, rather than a mere qualitative assessment, that can aid to follow the natural history of the disease and the response to treatment is, surely, important. However, the use of the most common parameter—SUV—is debated by both nuclear medicine physicians and clinicians. Although widely available and convenient to use, SUV measurements can be influenced by a variety of biological and technological factors. For example, in the use of serial SUV measurements to assess response to therapy, imaging should be performed on the same scanner using the same image acquisition and reconstruction protocols, and just a consistent variation of the parameters should be interpreted [18, 19]. Consequently, the routine use of response assessment criteria (e.g., Deauville score, PERCIST) belongs to the standardization of protocols and techniques to make serial PET scans comparable. This issue could partly explain the wide range of responses highlighted by our results regarding the use of PET/CT criteria within the report. However, the standardization of imaging protocols should be addressed in clinical practice to systematically use PET response criteria as part of the standardization process, which also assumes great importance in multicenter studies. In this context, the same patient should always perform PET/CT examinations at the same PET/CT center to grant reproducibility and make the comparison more reliable [20,21,22]. One of the most notable findings of this survey is the impact on the clinical management of patients after the results of PET/CT, clear and robust. The final report almost always leads to a clinical change or confirmation of the management of patients, until to 78% (53% major changes and 25% minor changes) in line with other realities.
Finally, a strength of our results is that most of the participants work in a public hospital, which allows for a reliable understanding of clinical reality, as such as the long experience of the participants (58% more than 10 years). Conversely, the results could be partially affected by the prevalence of radiation oncologists compared to the other specialists involved and the wide heterogeneity among interviewed (e.g., oncologists, hematologists, general surgeons…) that depends on the request to AIMN members to reach all the referring physicians involved in cancer management, without any restriction. Another limitation is represented by the relatively small sample size, partially due to the low response rate generally achieved by a web-based survey, which was attempted to be overcome with a double reminder. In this context, the single-nation investigation has to be taken into consideration. On the other hand, however, the national approach of the survey (with homogeneous geographical participation) allowed for the evaluation of the response based on a single healthcare system, which follows the same guidelines, clinical practice, and oncology management, leading to reliable conclusions.
At this stage, the importance of attracting the most talented and highly motivated individuals to nuclear medicine programs is essential considering the expansion of knowledge also in non-oncological fields such as cardiology, neurology, musculoskeletal disorders, infectious and inflammatory disease along with the rapid evolution of theragnostic. This could emphasize the essential role of functional imaging in different settings. Namely, the ability to involve passionate and trained professionals is the key to improving not only the interactions between different specialist figures and resolving existing doubts but also ensuring a bright future for nuclear medicine.
Conclusion
In conclusion, the present web-based National Italian Survey exploring uncertainty toward oncology PET/CT underlined the “still not” complete confidence with PET/CT indications, as well as the need to facilitate access to PET/CT indications and their update. Moreover, a structured PET/CT report with a clarification on essential features within the report is warranted. In this scenario, the increased participation of nuclear physicians in oncological guideline committees, the improvement of the relationship with the referring physicians, as well as the continuous training among all specialists involved in cancer patients’ management could be effective and reliable strategies to solve existing doubts.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
References
Wibmer AG, Hricak H, Ulaner GA, Weber W (2018) Trends in oncologic hybrid imaging. Eur J Hybrid Imaging. https://doi.org/10.1186/S41824-017-0019-6
Freudenberg LS, Hicks RJ, Beyer T (2019) An international survey on clinical reporting of PET/CT examinations: a starting point for cross-specialty engagement. J Nucl Med 60:480–485. https://doi.org/10.2967/JNUMED.118.218073
Boellaard R, Delgado-Bolton R, Oyen WJG et al (2015) FDG PET/CT: EANM procedure guidelines for tumour imaging: version 2.0. Eur J Nucl Med Mol Imaging 42:328–354. https://doi.org/10.1007/S00259-014-2961-X
Fahim-Ul-Hassan CGJ (2012) PET/CT in oncology. Clin Med (Lond) 12:368–372. https://doi.org/10.7861/CLINMEDICINE.12-4-368
Karantanis D, Kalkanis D, Allen-Auerbach M et al (2012) Oncologic 18F-FDG PET/CT: referring physicians’ point of view. J Nucl Med 53:1499–1505. https://doi.org/10.2967/JNUMED.111.102228
Prestazioni garantite dal SSN - LEA (Livelli Essenziali di Assistenza) - Portale della Trasparenza. https://www.portaletrasparenzaservizisanitari.it/prestazioni-garantite-dal-ssn-lea-livelli-essenziali-di-assistenza/. Accessed 29 Jul 2023
Hricak H, Abdel-Wahab M, Atun R et al (2021) Medical imaging and nuclear medicine: a Lancet Oncology Commission. Lancet Oncol 22:e136–e172. https://doi.org/10.1016/S1470-2045(20)30751-8
Dapper H, Dantes M, Herschbach P et al (2023) Relevance of tumor boards for the inclusion of patients in oncological clinical trials. J Cancer Res Clin Oncol. https://doi.org/10.1007/s00432-022-04559-0
Petty JK, Vetto JT (2002) Beyond doughnuts: tumor board recommendations influence patient care. J Cancer Educ 17:97–100. https://doi.org/10.1080/08858190209528807
Piano oncologico nazionale 2023–2027. https://www.salute.gov.it/portale/tumori/dettaglioContenutiTumori.jsp?lingua=italiano&id=6012&area=tumori&menu=vuoto. Accessed 1 Aug 2023
Stokkel MPM, Owers EC (2023) Hybrid training in nuclear medicine: where are we going to? Eur J Nucl Med Mol Imaging 50:2231–2235. https://doi.org/10.1007/S00259-023-06223-2
Velleman T, Kwee TC, Dierckx RAJO et al (2022) The integrated nuclear medicine and radiology residency program in the Netherlands: strengths and potential areas for improvement according to nuclear medicine physicians and radiologists. Eur J Nucl Med Mol Imaging 49:3016–3022. https://doi.org/10.1007/S00259-022-05699-8
Niederkohr RD, Greenspan BS, Prior JO et al (2013) Reporting guidance for oncologic 18F-FDG PET/CT imaging. J Nucl Med 54:756–761. https://doi.org/10.2967/jnumed.112.112177
Donohoe K, Ahuja S (2019) Society of Nuclear Medicine and Molecular Imaging Efforts Toward Standardization: From Procedure Standards to Appropriate Use Criteria. Semin Nucl Med 49:153–160. https://doi.org/10.1053/j.semnuclmed.2018.11.004
Calcagni ML, Castaldi P, Giordano A LA REFERTAZIONE DELLA PET-TC ONCOLOGICA con 18F-FDG: istruzioni pratiche per un referto standardizzato e di qualità
AIMN - gds-14. https://www.aimn.it/site/page/gds/gds-14. Accessed 31 May 2023
Ceci F, Oprea-Lager DE, Emmett L et al (2021) E-PSMA: the EANM standardized reporting guidelines v1.0 for PSMA-PET. Eur J Nucl Med Mol Imaging 48:1626–1638. https://doi.org/10.1007/S00259-021-05245-Y
Adams MC, Turkington TG, Wilson JM, Wong TZ (2010) A systematic review of the factors affecting accuracy of SUV measurements. AJR Am J Roentgenol 195:310–320. https://doi.org/10.2214/AJR.10.4923
Brendle C, Kupferschläger J, Nikolaou K et al (2015) Is the standard uptake value (SUV) appropriate for quantification in clinical PET imaging? - Variability induced by different SUV measurements and varying reconstruction methods. Eur J Radiol 84:158–162. https://doi.org/10.1016/j.ejrad.2014.10.018
Hillner BE, Siegel BA, Liu D et al (2008) Impact of positron emission tomography/computed tomography and positron emission tomography (PET) alone on expected management of patients with cancer: initial results from the National Oncologic PET Registry. J Clin Oncol 26:2155–2161. https://doi.org/10.1200/JCO.2007.14.5631
Larson SM (2008) Practice-based evidence of the beneficial impact of positron emission tomography in clinical oncology. J Clin Oncol 26:2083–2084. https://doi.org/10.1200/JCO.2007.15.6935
Miceli A, Jonghi-Lavarini L, Santo G, et al (2023) [18F]FDG PET/CT criteria for treatment response assessment: EORTC and beyond. Clin Transl Imaging
Acknowledgements
We would like to thank Domenico Albano, Andrea Bianchi, Mohsen Farsad, Luca Guerra, Cristina Nanni, and Luca Urso, members of the AIMN Oncology Working Group, for their critical review of the survey questions and their constructive suggestions. We would also like to thank all AIMN members who contributed to the spread of the survey.
Funding
Open access funding provided by Università degli studi "Magna Graecia" di Catanzaro within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Consortia
Contributions
GS: manuscript writing, data extraction, analysis, and editing; AM: manuscript writing and editing; AL, JG, AGN, LJL, FD, and FLT: survey content planning, data review, and revision of the first draft of the manuscript; AF: coordination, content planning, and revision of the manuscript; MLDR: coordination, survey public outreach, critical revision of the manuscript, and supervision; LE: study conceptualization, content planning, survey public outreach, critical review of the survey and final draft, supervision; SP: survey content planning, survey public outreach, critical revision of survey and final draft, supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Santo, G., Miceli, A., Lazzarato, A. et al. Clinicians’ perspectives on PET/CT in oncological patients: an Italian National Survey. Clin Transl Imaging 12, 99–107 (2024). https://doi.org/10.1007/s40336-023-00591-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40336-023-00591-3