
Abstract
Introduction
Hypertension (SBP/DBP > 130/80 mmHg) is a leading risk factor for cardiovascular disease worldwide.
Aim
To determine the prevalence of hypertension in a homeless community during an interprofessional education (IPE)-based health fair.
Methods
Homeless participants were recruited between August 2019–September 2019. Faculty, nursing, and pharmacist students, educated 477 participants, aged 18–80 years, on the risk factors associated with untreated hypertension. Then, participants self-completed the consented demographic survey questionnaire. Finally, the sitting blood pressure (BP) was recorded three times based on a standardized procedure, using Omron BPN monitor with cuff.
Results
Seven pharmacy students, nine nursing students, two registered nurses, five registered pharmacists, and two medical doctors collaboratively provided health education to the homeless community and screened their sitting BP. 390/477 (81.8%) of participants satisfied the inclusion criteria. Participants (54.7%) of the reported education level was at the high School level or less. More than the half of the participants (average age of 51 ± 13 years) had hypertension (median SBP/DBP ≥ 130/82.7 mmHg), respectively. The prevalence of hypertension for the overall cohort was 61.52% (95% CI, 56.59–66.35). Age (p value = 0.000) was significantly associated with hypertension based on the binary logistic analysis.
Conclusion
This study demonstrated a high prevalence of hypertension in the homeless community in Long Beach, California with high risk of cardio-vascular events or strokes. This works sheds new light on an issue of major public health significance and points to the need for fostering IPE community-based health fairs intervention program for the US homeless population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Interprofessional education (IPE) is widely recognized as a collaborative valuable education for healthcare students [1]. American University of Health Sciences (AUHS) IPE’s hosted health fair such as screening for hypertension aligns with the 2016 update of the core competencies for Interprofessional Collaborative (IPEC) such as interprofessional practice, roles/responsibilities, communication and teamwork [2].
High blood pressure (HBP) or hypertension remains the leading risk factor of cardiovascular disease (CVD) and stroke according to the recent American Heart Association (AHA) 2019 report [3]. In 2019, CVD remains the major cause of death in both men and women in the United States of America [3]. Based on the new blood pressure (BP) thresholds from the 2017 American College of Cardiology (ACC)/AHA guidelines, the age-adjusted prevalence of HBP in an American adult is approximately forty six percent (46%) which is an estimate of 116.4 million of adults aged greater than or equal to 20 years [4]. A patient is hypertensive whenever, his or her systolic blood pressure (SBP) is greater than or equal to 130 mmHg and/or his or her diastolic blood pressure (DBP) is greater than or equal to 80 mmHg, based on the 2017 ACC/AHA guidelines. HBP is generally nicknamed the silent killer because it is symptomless unless until it has made significant damage to the heart and arteries [5].
The mortality rate of homeless people is 3–4 times greater than the Unites States’ general population [6]. Similarly, to the US general population, CVD associated death is remarkably high in the US homeless population [7, 8]. The purpose of this study is to estimate the age adjusted direct standardized prevalence of hypertension in a homeless community during a dual cross-sectional study and an IPE community-based health fair event in Long Beach, California.
2 Methods
Homeless participants were recruited between August 2019–September 2019. AUHS students and faculty provided health education to the homeless community on the risk’s factors associated with HBP. Then, participants received a consent form prior to their participation in this study. Participants are homeless adults ranging 18–80 years old. Explanation on the early screening for hypertension was provided to the participants prior to the measurement of the blood pressure. All participants signed a free and informed consent form. The size of the participants was 477/1894 (25.2%) of the total homeless population living in Long Beach, CA [9]. The total number of people experiencing homelessness was estimated to 1894 people based on the 2019 Point-in-Time Homeless Count Results in Long Beach, CA [9]. Participants self-reported demographic information (e.g., age, ethnicity, gender, education level), disability status, residential status, health insurance status, marital status, and reason for coming biweekly to the IPE Site location (Second Samoan Congregational Church of Long Beach CA). Then, faculty, nursing, and pharmacist students measured the sitting blood pressure (BP) of the participants following a standardized procedure using Omron BPN series Upper Blood Pressure monitor with cuffs.
AUHS Institutional Review Board reviewed and approved the study. Exclusion criteria were failures to report age or screening for hypertension. A total of 390/477 participants (81.8%) of the total cohort satisfied the inclusion criteria and was used for the prevalence and the multivariate analysis.
2.1 Statistical Analysis
SBP/DBP were measured three times and the results were presented as a means (SD). The results were reported as numbers (and their corresponding percentages) for categorical variables. Age was direct-standardized based on the 2018 United States of America census population [10]. The directly standardized prevalence of hypertension (DSP) was given by the following equation [11]:
where, \(\hat{p}_{i}\) was the prevalence of hypertension in the ith age group of the population. ni is the mid-year population in the ith age group.
\(\hat{p} = y/p\), with y the number of participants having hypertension, and p, the sample size. \(\hat{p}\) is the crude (unadjusted) prevalence of hypertension.
The confidence interval (CI) for the prevalence of hypertension was expresses as followed [12]:
where, z = 1.96, is the value from the standard normal distribution for a 95% confidence level.
A paired t-test was used to compared means. The 2019 United States prevalence of hypertension was used as a control.
Binary logistic regression in IBM SPSS statistics version 26.0, was used to assess factors (age, race/ethnicity, gender, shelter status and, health insurance) association with hypertension set as a categorical dependent variable (hypertensive participant = 1, non-hypertensive participant = 0). The binary logistic regression was fitted and all independent factors with a p-value less than 0.25 were used in the model [13].
Demographic information comprised age stratified, sex, gender, race/ethnicity, education, disability, marital status, shelter status and reasons for visiting the Church. Means of continuous variable were compared with t-test. A p-value below 0.05 was considered statistically significant and warranted rejection of the null hypothesis.
3 Results
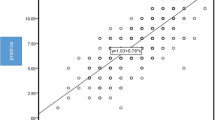
Seven pharmacy students, nine nursing students, two registered nurses, five registered pharmacists, and two medical doctors collaboratively provided health education to the homeless community and screened their sitting blood pressure and explained the importance for earlier screening for high blood pressure. The average age, median age and mode age were 51 ± 13, 53, and 57 years, respectively. Moreover, 70.8% of the participants had 45 years old or greater. As shown, in Fig. 1, the following variables age (p = 0.000), race/ethnicity (p = 0.119), gender (p = 0.195), and insurance status (p = 0.234) were included in the fitted model and age (p = 0.000) was strongly associated with hypertension based the binary logistic analysis. In addition, as shown, in Fig. 1, age (B = 0.472) and race/ethnicity (B = 0.369) are positively correlated with hypertension. Thus, the regression function is:
where the categorical variables, Y = hypertension (hypertensive participant = 1, non-hypertensive participant = 0), is the dependent variable. The independent variables X1 = age group ([18, 44] = 1, [45–54] = 2, [55, 64] = 3, and 65 and above = 4), X2 = insurance status (insured participant = 1, uninsured participant 0), X3 = ethnicity (black ethnicity = 1, others ethnicity = 0), and X4 = gender (male = 1 and, other genders = 0).

Binary logistic regression analysis predicting factors associated with hypertension
The sociodemographic characteristic of the homeless participants is shown in Table 1. Out of 320 participants who reported their education level, ~ 54.75% of participants had high school level or less. Participants were mostly male with high representation of Black ethnicity (48.7%).
The DBP ranged from 49.0–118.7 mmHg. The overall mean, median and mode of the DBP were 84.02 ± 12.38, 82.7 and 75.0 mmHg, respectively. Likewise, the SBP ranged from 79.7–199.5 mmHg. The overall mean, median and mode of the SBP were 132.41 ± 20.00, 130, and 127 mmHg, respectively. According to the median value of the SBP/DBP (130/82.7 mmHg), more than half of the participants had hypertension. A flyer was provided to participants who needed immediate medical attention due to SBP/DBP greater than or equal to 180/120 mmHg. Age and racial/ethnicity were factors associated with hypertension based on the binary logistic analysis and t-test. The prevalence of hypertension according to sociodemographic characteristics is shown in (Table 2).
4 Discussion
In this study, the prevalence of hypertension among the homeless population in Long Beach, CA was elucidated during a dual cross-sectional study during the IPE health fair community-based event. Students and faculty used the blood pressure threshold to educate the homeless participants on hypertension associated with cardiovascular disease or stroke events. They performed basic clinical blood pressure monitoring and asked participants their medication history. Nursing and pharmacy students and faculty displayed excellent teamwork. The prevalence of hypertension of this cohort of homeless population 61.5 (95% CI 56.7–66.4) was extremely high compared to that of the 2019 US general population 46% (95% CI 44–48) [3]. This result was consistent with the finding of Giuliano Tocci et al. who demonstrated that the prevalence of hypertension for a cohort of homeless people in Italy was greater than that of the housed people [14]. Many factors explained the higher rate of hypertension. For instance, the lack of physical activity, aging of the population, poor diet and stress are major risk factors of hypertension and could explain the higher prevalence of hypertension in this homeless population [15]. Seven participants had SBP/DBP ≥ 180/90 mmHg suggesting that they were in a state of hypertensive crisis and were strongly advised to seek immediate medical assistance. Hypertension potentiates current COVID-19 patient risk of death [16, 17]. Thus, there is a critical need to provide emergency shelter and health support [18] for this vulnerable homeless community to prevent the spread of COVID-19 among this underserved and vulnerable population [16, 19]. Most importantly, the availability of affordable permanent housing which is intrinsically income-dependent will ultimately be a sustainable and durable solution to end homelessness and health disparities associated with homelessness [7].
There were several limitations in this study. The size of the cohort was only 477/1894 (25.2%) total of the Long Beach, CA homeless population [9]. Participants failed to answer all the questionnaire resulting in only 81.8% response rate. A future direction involves the use of the eight-item Morisky Medication Adherence Scale (MMAS-8) to monitor the blood pressure of hypertensive participants over a long period of time [20]. The adherence to prescribed BP medications has shown to be an effective mean to reduce hypertension [14].
5 Conclusion
There was a high prevalence of hypertension in the homeless community. Interprofessional education-based health fair is a steppingstone to facilitate collaboration and teamwork among future health care workers. This work sheds new light on an issue of major public health significance and points to the need for fostering IPE community-based health fairs intervention program for the US homeless population.
References
Bridges DR, Davidson RA, Odegard PS, Maki IV, Tomkowiak J. Interprofessional collaboration: three best practice models of interprofessional education. Med Educ Online. 2011;8:16.
Collaborative I. Core competencies for interprofessional collaborative practice: 2016 update. Washington, DC: Interprofessional Education Collaboration; 2016.
Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56–528.
Miedema MD, Sidebottom AC, Sillah A, Benson G, Knickelbine T, VanWormer JJ. Clinical implications of the American College of Cardiology/American Heart Association guidelines for the treatment of blood cholesterol for a rural community: data from the Heart of New Ulm Project. J Clin Lipidol. 2017;11(1):94–101.
Wei LK, Au A, Teh LK, Lye HS. Recent advances in the genetics of hypertension. Adv Exp Med Biol. 2017;956:561–81.
Henwood BF, Byrne T, Scriber B. Examining mortality among formerly homeless adults enrolled in Housing First: an observational study. BMC Public Health. 2015;4(15):1209.
Ngo AN, Turbow DJ. Principal component analysis of morbidity and mortality among the united states homeless population: a systematic Review and Meta-Analysis. Inter Arch Public Health. Community Med. 2019;3:025. https://doi.org/10.23937/2643-4512/1710025.
Baggett TP, Liauw SS, Hwang SW. Cardiovascular disease and homelessness. J Am Coll Cardiol. 2018;71(22):2585–97.
Kelly C. Homeless Services Update: 2019 Point-in-Time Homeless Count Results. In: media-library/documents/memos-to-the-mayor-tabbed-file-list-folders.2019. http://www.longbeach.gov/globalassets/city-manager/media-library/documents/memos-to-the-mayor-tabbed-file-list-folders/2019/june-3--2019---homeless-services-update---2019-point-in-time-homeless-count-results_. Accessed June 2019.
U.S. Census Bureau. Age and Sex Composition in the United States 2018. 2019. https://www.census.gov/data/tables/2019/demo/age-and-sex/2019-age-sex-composition.html. Accessed 11 Jul 2019.
Inoue OBACB-PADLCJMRLM. Age standardization of rates: a new WHO standard. GPE Discussion Paper Series No 31 EIP/GPE/EBD World Health Organizationn 2001. 2001.
Sullivian L. Confidence Interval for one sample, dichotomous outcome. 2017. Boston University School of Public Health. https://sphweb.bumc.bu.edu/otlt/mph-modules/bs/bs704_confidence_intervals/bs704_confidence_intervals4.html. Accessed 27 Oct 2017.
Mohamed SF, Mutua MK, Wamai R, Wekesah F, Haregu T, Juma P, et al. Prevalence, awareness, treatment and control of hypertension and their determinants: results from a national survey in Kenya. BMC Public Health. 2018;18(Suppl 3):1219.
Tocci G, Presta V, Schiavello F, Miceli F, Citoni B, Battistoni A, et al. Immigration emergency in Italy: the impact of socioeconomic status on blood pressure levels and control. High Blood Press Cardiovasc Prev. 2019;26(6):467–73.
Kornitzer M, Dramaix M, De Backer G. Epidemiology of risk factors for hypertension: implications for prevention and therapy. Drugs. 1999;57(5):695–712.
Ji HL, Zhao R, Matalon S, Matthay MA. Elevated plasmin (ogen) as a common risk factor for COVID-19 susceptibility. Physiol Rev. 2020;100(3):1065–75.
Guo T, Fan Y, Chen M, Wu X, Zhang L, He T, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(7):811–8.
Parker RD, Cima MJ, Brown Z, Regier M. Expanded medicaid provides access to substance use, mental health, and physician visits to homeless and precariously housed persons. J Community Health. 2018;43(2):207–11.
Mosites E, Parker EM, Clarke KEN, Gaeta JM, Baggett TP, Imbert E, et al. Assessment of SARS-CoV-2 infection prevalence in homeless shelters—four U.S. cities, March 27–April 15, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(17):521–2.
Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens (Greenwich). 2008;10(5):348–54.
Acknowledgements
This work was supported by the American University of Health Sciences Foundation, Signal Hill, CA, USA, Grant# IG020719C.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Author contributions
All authors participated to the IPE community-based health fairs event hosted by Second Samoan Church under the leadership of Pastor Gregory A. Johnson. ANN crafted the research proposal and ANN designed and analyzed the data and drafted the first manuscript. MI, JA, and SS generated additional ideas to improve the quality of the manuscript. All authors edited the manuscript, reviewed, and approved the final version, and agreed to be accountable for all aspects of the work. The authors would like to thank all nursing and pharmacy students, and registered nurses for making the IPE community-based health fairs successful. The views expressed in this article are those of the authors and do not necessarily represent the views of American University of Health Sciences.
Conflict of interest
All authors declared no conflict of interest.
Human participant protection
Research was conducted in compliance with the principles of the declaration of Helsinki. Privacy and confidentiality were considered. Informed written consents were obtained from literate participants in the study. The study was approved by the Institutional Research Board of American University of Health Sciences IRB Log #001.
Consent for publication
Participants signed informed consent regarding publishing their data if any report of this research which is made available to the public will not include their names or any individual information by which they could be individually identified.
Data availability
The raw data that support the findings of this study are available upon reasonable request from the corresponding author, [ANN]. The data are not publicly available due to The Health Insurance Portability and Accountability Act of 1996 (HIPAA) law restrictions. Raw Data contain information that could compromise the privacy of research participants.
Rights and permissions
About this article

Cite this article
Ngo, A.N., Islam, M.A., Aoyagi, J. et al. Prevalence of Hypertension in Homeless Adults: An Interprofessional Education Community-Based Health Fairs Cross-Sectional Study in Urban Long Beach, California. High Blood Press Cardiovasc Prev 28, 63–68 (2021). https://doi.org/10.1007/s40292-020-00424-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40292-020-00424-8