
Abstract
Background
Preterm birth and low birthweight (LBW) might be associated with reduced physical fitness, although evidence remains inconclusive.
Objective
To examine the influence of preterm birth and LBW on physical fitness, as well as to assess whether variables such as gestational age, birthweight, or age at assessment moderate these effects.
Methods
PubMed, Scopus, and PsycINFO were systematically searched from inception to 7 December 2023 for case–control and cohort studies analyzing the association between preterm birth or LBW (or gestational age or birthweight as continuous variables) with at least one physical fitness-related outcome (i.e., cardiorespiratory fitness (CRF), muscle strength, flexibility, speed, agility). Random-effects meta-analysis and meta-regression models were used to estimate the pooled effect size, as well as to examine potential associations between the magnitude of the effect and gestational age, birthweight, or age at assessment.
Results
Fifty-two studies (n = 920,603 participants, average age ranging from 4.7 to 34.4 years) were included. Preterm birth was associated with reduced CRF (standardized mean difference (SMD) = −0.38, 95% confidence interval (CI) = −0.51 to −0.25) and muscle strength (SMD = −0.44, 95% CI = −0.79 to −0.08). LBW was associated with reduced CRF (SMD = −0.40, 95% CI = −0.64 to −0.17), muscle strength (SMD = −0.18, 95% CI = −0.24 to −0.13), flexibility (SMD = −0.11, 95% CI = −0.22 to −0.01), and agility (SMD = −0.99, 95% CI = −1.91 to −0.07). Meta-regression analyses showed that a lower gestational age or birthweight were associated with larger reductions in physical fitness, whereas no consistent association was found for the age at assessment.
Conclusion
Both preterm birth and LBW seem associated with reduced physical fitness regardless of age, with larger reductions overall observed in individuals with lower gestational age or birthweight. These findings might support the implementation of preventive strategies (e.g., fitness monitoring and physical exercise interventions) in these populations through the life course.
PROSPERO registration: CRD42021231845.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
In this systematic review and meta-analysis, which included 52 studies (n = 920,603 participants, average age ranging from 4.7 to 34.4 years), both preterm birth and low birthweight were associated with reduced physical fitness (e.g., cardiorespiratory fitness, muscle strength). | |
Meta-regression analyses revealed that a lower gestational age or birthweight were overall associated with larger reductions in physical fitness, whereas no consistent associations were found between participants’ age at assessment and the magnitude of the reductions in physical fitness (i.e., similar reduction from childhood to adulthood). | |
These findings might support the implementation of preventive strategies (e.g., fitness monitoring, physical exercise interventions) in these populations through the life course. |
1 Introduction
Preterm birth (conventionally defined as < 37 weeks of gestation) and low birthweight (LBW) (birthweight < 2.5 kg) are highly prevalent conditions [1, 2]. It is estimated that ~ 15 million children are born preterm every year, representing 10% of births worldwide [3], whereas approximately 20 million children are born with LBW, representing 15.5% of all births [4]—of note, although prematurity and LBW are two different conditions, they are highly interrelated, as many preterm individuals are born with LBW. Although advances in neonatal medicine have improved survival rates in preterm children and in those with LBW [5], these conditions are still linked to a higher risk of morbidity and mortality [6,7,8]. Indeed, one-quarter of all early deaths in newborns that are not produced by congenital malformations are due to preterm birth [9]. It is worth noting, however, that these conditions are not only associated with a higher morbidity risk during early childhood [10, 11], but also later in life. For instance, children with LBW have a 40-fold higher risk of mortality during the first month of life compared to those born with normal birthweight, with both preterm birth and LBW being linked to, for example, a higher risk of respiratory and cardiovascular conditions during adulthood [11,12,13,14,15,16].
Physical fitness (including different components such as cardiorespiratory fitness (CRF), muscle strength, speed, flexibility, or agility) is an important health indicator and a predictor of both short- and long-term morbidity and mortality risk in children and adolescents [17]. For instance, a reduced CRF during childhood is associated with a higher risk of developing conditions such as obesity and cardiometabolic diseases later in life [18, 19], and similar findings have been reported for muscle strength [20]. Moreover, CRF and muscle strength are strong predictors of morbidity and mortality in adults [21, 22].
A reduced physical fitness might play a role in the adverse effects associated with preterm birth and LBW. Growing evidence does indeed suggest that individuals born preterm [23, 24] or with LBW [25] present a reduced physical fitness, although meta-analytical evidence is scarce. In a meta-analysis of 22 studies, Edwards et al. [26] also found that preterm participants aged between 5 and 21 years had a lower maximum oxygen uptake (VO2max) compared with their peers born at term. Moreover, Dodds et al. [27] meta-analyzed 19 studies and found a positive association between birthweight and muscle strength, which was maintained across the life course. In a meta-analysis of ten studies, Poole et al. recently reported that participants aged over 18 years with LBW had a reduced CRF (as assessed by VO2max) compared with their term-born peers [28]. However, to our knowledge no meta-analytical evidence exists on the effect of preterm birth on muscle strength, nor for the effects of these conditions on other physical fitness outcomes such as flexibility, agility, or speed. Moreover, whether a lower birthweight or gestational age might be associated with greater reductions in physical fitness remains unclear, as well as whether the magnitude of these reductions might vary depending on the individuals’ age at assessment (e.g., with these differences decreasing at older ages).
The present systematic review and meta-analysis aimed to determine the effects of preterm birth and LBW on different physical fitness indicators, as well as to examine whether different variables (i.e., gestational age, birthweight, age at assessment) moderate these effects. Of note, although preterm birth and LBW are two interrelated conditions, we aimed to study them separately, which could help to understand the similarities and differences between them.
2 Methods
The present systematic review was registered in PROSPERO (CRD42021231845), and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) [29].
2.1 Study Selection and Search Strategy
Case–control and cohort studies analyzing the association between preterm birth or LBW (or gestational age or birthweight as a continuous variable) with at least one physical fitness-related outcome (i.e., CRF, muscle strength, flexibility, speed, or agility) were included. Studies were excluded if they were solely focused on specific populations such as individuals with overweight, respiratory conditions, or functional disabilities.
Two authors (MDMZ and CMM) independently performed the systematic search for relevant articles in PubMed, Scopus, and PsycINFO from inception up to 7 December 2023. The search included terms in titles and abstracts related to both the populations (i.e., preterm birth and LBW) and the outcomes of interest (i.e., physical fitness components). The search was limited to peer-reviewed articles published in English and Spanish. Additional search filters were not applied. The search strategies are shown as Table S1 in the Online Supplementary Material (OSM). The electronic search was supplemented with a manual review of reference lists from relevant publications and other reviews related to the topic [26,27,28] to locate additional studies.
Citations were first retrieved and preliminarily screened by title and abstract, and duplicates were removed manually. Full-texts of those studies that met the inclusion criteria were assessed. Each author provided a separate list with the studies selected at each stage, as well as with those to be finally included. Potential disagreements were resolved through discussion with two other authors (OMDQ and PLV).
2.2 Data Extraction
Two authors (MDMZ and CMM) independently extracted the relevant information from each study (i.e., participants’ characteristics, outcomes assessed, and main results). Data for quantitative analyses were extracted, when available, as mean and standard deviation (SD). When data were provided as the median and/or using other measures of dispersion (e.g., standard error, range, 95% confidence interval (CI)), the required information was estimated as explained elsewhere [30]. When available, we used the most adjusted model (e.g., adjusting for covariates such as sex, age at assessment, or socioeconomic status) for analyses. We had to contact the authors of 14 studies because the required data were not reported. Of these, the authors of eight studies provided the required information [31,32,33,34,35,36,37,38].
2.3 Study Quality Assessment
Study quality was determined using the Newcastle–Ottawa Scale (NOS) [39], which assesses the risk of bias considering three domains: selection of participants, comparability, and outcomes (Table S2, OSM). Two authors (MDMZ and CMM) independently scored the studies, and disagreements were resolved through discussion with a third author (OMDQ). A 0–10 total score was determined by counting the number of criteria satisfied by each study, which could be classified as having good (≥ 8), fair (7), or poor quality (≤ 6).
2.4 Statistical Analysis
Pooled analyses were performed using a random-effects model (DerSimonian and Laird method) when at least three studies assessed a given outcome. The pooled standardized mean difference (SMD) between groups was computed along with 95% CI, and if the studies reported the same outcome using the same assessment method and measurement units (e.g., VO2max in ml/kg/min, handgrip strength in kg), the absolute mean difference (MD) was computed. When a study assessed a given outcome at several time points, the longest follow-up was used for analyses. In the same line, when two studies shared some of the same participants, the study with the longest follow-up was analyzed. When two studies shared some of the same participants and had the same follow-up, the study with the largest sample size was used for analyses. For an initial general analysis, in those cases in which one study assessed different indicators related to the same outcome, we selected the outcome most commonly assessed (e.g., VO2max over distance in the shuttle run test for the analysis of CRF, or handgrip strength over curl ups or horizontal jump distance for the analysis of muscle strength). However, sub-analyses were performed for the different indicators when possible. As recommended elsewhere, when a study included more than two groups of cases (e.g., extremely preterm and preterm individuals) in comparison with a control group, we halved the number of participants in the control group for each of the comparisons [30]. Sensitivity analyses were conducted by testing significance when removing one study at a time (leave-one-out method) to check if findings were mostly driven by an individual study. Meta-regression analyses were performed using a random effects model (method of moments) to assess the association between birthweight, gestational age, or age at assessment with the magnitude of the differences between groups. Meta-regression analyses were only performed for those outcomes assessed by ten or more studies [30]. Begg’s test was used to determine the presence of publication bias (small-study effects), and the I2 statistic was used to assess heterogeneity across studies. I2 values > 25%, 50%, and 75% were considered indicative of low, moderate, and high heterogeneity, respectively. The level of significance was set at 0.05. All statistical analyses were performed using the statistical software package Comprehensive Meta-analysis 2.0 (Biostat; Englewood, NJ, USA).
3 Results
3.1 Characteristics of the Included Studies
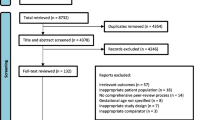
A flowchart of the literature search is shown in Fig. 1. A total of 52 studies (n = 920,603 participants) were eventually included, of which 26 (n = 455,135 participants) assessed the influence of preterm birth and 27 (n = 466,506 participants) were focused on the influence of LBW. In one study [40] all participants had both conditions. Some studies shared part of the same sample [41,42,43], and only the largest one was used for the computation of the total sample size to avoid duplication of participants. The characteristics of the included studies are summarized in Tables S3 and S4 (SM) for preterm and low birthweight participants, respectively.

Flow diagram of the literature search
The studies focused on preterm birth included between 21 and 218,802 participants with an average age ranging from 4.7 to 28 years (weighted average age 17.5 years), whereas those focused on LBW included between 30 and 144,369 participants with an average age ranging between 5 and 34.4 years (weighted average age 17.5 years). Most studies analyzed both male and female participants except for five studies that included solely male participants [23, 33, 34, 44, 45]. Most studies followed a cross-sectional case–control design, except for four cross-sectional cohort studies [33, 34, 46, 47]. Only three studies followed a longitudinal case–control design, in which the last measurement was considered for analyses [48,49,50]. Of the included case–control studies, eight divided the participants in sub-groups according to their gestational age or birthweight (e.g., very low birthweight and extremely low birthweight, extremely preterm and very preterm), whereas 40 of them combined them in one single group (i.e., controls vs. preterm or LBW). Most studies (n = 7) included participants from the USA, followed by Australia (n = 6), Norway (n = 4), and Sweden (n = 4). Most studies were conducted in medium- and high-income countries except for one [44] conducted in Mozambique.
3.2 Quality Assessment
The quality of the included studies was overall good (average score of 8 out of 10, Table S5 (OSM)). Most studies adequately described the representativeness of the sample and justified the sample size (72% and 79%, respectively), although only 41% reported a satisfactory rate of response. All studies described the assessment tool and used a validated tool. Most studies (~ 93%) adjusted for the main demographic variables such as age and sex, and others also adjusted for socioeconomic status, physical activity levels, or body composition, but most of the studies did not adjust for potential confounding variables such as delivery mode or body mass index at the time of assessment. All studies described appropriately the statistical test performed, and 82% employed an independent blind assessment.
3.3 Synthesis
A summary of the pooled results is shown in Table 1.
3.3.1 Cardiorespiratory Fitness (CRF)
Twenty-three studies [24, 37, 38, 40, 45, 49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66] assessed the influence of preterm birth on CRF-related measures such as VO2max, maximal power output (Wmax) on a cycle ergometer, distance covered on an incremental treadmill test, or the 6-min walking test. Of these, 17 studies including 24 group comparisons (n = 89,230 participants, weighted average age at assessment = 19 years) could be meta-analyzed. Pooled analyses revealed a reduced CRF in preterm individuals compared to controls (SMD = −0.38, 95% CI = −0.51 to −0.25, p < 0.001, Fig. S1), with no signs of risk of bias (Begg’s p = 0.185) but with large heterogeneity (I2 = 77.4%). Sensitivity analyses by removing one study at a time confirmed these differences, as well as when replacing the data from the 6-min walking test with data from the shuttle run test in the study by Cheong et al. [55], which analyzed both tests. Sub-analysis of those studies assessing VO2max (11 studies, 15 group comparisons, n = 688 participants) also confirmed significantly lower values in individuals born preterm compared to controls (MD = −3.47 ml/kg/min, 95% CI = −5.04 to −1.89, p < 0.001; equivalent to SMD = −0.45, 95% CI = −0.61 to −0.28, I2 = 34.9%, Begg’s p = 0.444). Five studies could not be meta-analyzed [23, 46, 50, 58, 59], but only one of them did not find differences in CRF between preterm individuals and controls [59].
Seventeen [25, 34,35,36, 40,41,42,43, 47, 60, 67,68,69,70,71,72,73] studies assessed the influence of LBW on CRF-related measures, of which 14 including 18 group comparisons (n = 1758 participants, weighted average age at assessment = 18 years) could be meta-analyzed. Their pooled analysis revealed a reduced CRF in individuals born with LBW compared to controls (SMD = −0.40, 95% CI = −0.64 to −0.17, p = 0.001, Fig. S2 (OSM)), albeit with signs of heterogeneity (I2 = 76.1%). Sensitivity analyses confirmed these differences. All of them analyzed VO2max, and differences corresponded to a MD = −2.81 ml/kg/min (95% CI = −4.45 to −1.17, p = 0.001). Only two studies could not be meta-analyzed [34, 73], but both of them reported a significantly lower CRF among individuals with LBW.
3.3.2 Muscle Strength
Nine studies [24, 38, 46, 50, 58, 59, 74,75,76] assessed different muscle strength indicators such as standing long jump test, vertical jump, or handgrip strength with a dynamometer in preterm individuals. Of these, eight studies including ten group comparisons (n = 2845 participants, weighted average age at assessment = 17 years) could be meta-analyzed. The initial general analysis revealed a reduced muscle strength in preterm individuals compared to controls (SMD = −0.44, 95% CI = −0.79 to −0.08, p = 0.016, Fig. S3 (OSM)), with no signs of publication bias (Begg’s p = 0.059) but large heterogeneity (I2 = 89.1%). Sensitivity analyses revealed a significant or quasi-significant trend (all p ≤ 0.06) when removing each individual study. Sub-analysis of the five studies (n = 1843 participants) that assessed handgrip strength (in kg) confirmed significantly lower values in preterm individuals compared to controls in standardized (SMD = −0.19, 95% CI = −0.33 to −0.06, p = 0.004) and absolute units (MD = −0.64 kg, 95% CI = −1.01 to −0.27, p = 0.001), with no heterogeneity (I2 = 0%) and no signs of publication bias (Begg’s p = 0.226). One study could not be meta-analyzed [50], but found lower scores in extremely preterm participants compared to controls.
Ten studies [33, 35, 44, 47, 48, 69, 73, 77,78,79] including 16 group comparisons (n = 274,100 participants, weighted average age at assessment = 18 years) assessed the influence of LBW on muscle strength, and all of them could be meta-analyzed. A reduced muscle strength was overall observed in individuals with LBW compared to controls (SMD = −0.18, 95% CI = −0.24 to −0.13, p < 0.001, Fig. S4 (OSM)), albeit with signs of heterogeneity (I2 = 86.6%). Sensitivity analyses confirmed these differences. Sub-analysis of the seven studies (n = 145,299 participants) assessing handgrip strength also confirmed significantly lower values in individuals with LBW compared to controls (MD = −1.37 kg, 95% CI = −1.81 to −0.93, p < 0.001; equivalent to SMD = −0.23, 95% CI = −0.29 to −0.16), again with large heterogeneity (I2 = 86.4%) and no signs of publication bias (p = 0.296). Sub-analysis of the four studies (n = 129,112 participants) assessing lower-limb strength indicators such as vertical or horizontal jump tests also revealed significantly lower values in individuals with LBW compared to controls (SMD = −0.23, 95% CI = −0.38 to −0.08, p = 0.002), and the separate analysis of the three studies (n = 596 participants) that assessed vertical jump ability confirmed these differences (MD = −6.66 cm, 95% CI = −10.24 to −3.08, p < 0.001, equivalent to SMD = −0.74, 95% CI = −1.19 to −0.30), in this case with no heterogeneity (I2 = 0%) and no publication bias (p = 0.154).
3.3.3 Flexibility
Only data from two studies [24, 38] were available for the analysis of flexibility in preterm individuals, and therefore this outcome could not be meta-analyzed. However, only one of them found differences in flexibility related to preterm birth, with term individuals showing better scores [24].
Four studies [35, 44, 73, 78] including nine group comparisons (n = 29,779 participants, weighted average age at assessment = 7 years) assessed flexibility in individuals with LBW, all of them using the sit and reach test. Their pooled analysis revealed a reduced flexibility in individuals with LBW compared to controls (MD = −0.83 cm, 95% CI = −1.59 to −0.08, p = 0.031; equivalent to SMD = −0.11, 95% CI = −0.22 to −0.01, Fig. S5 (OSM)), albeit with large heterogeneity (I2 = 70.3%) and signs of publication bias (p = 0.038). Results remained significant in sensitivity analyses.
3.3.4 Agility
Only data from two studies [24, 58] were available for the meta-analysis of agility in preterm individuals, and therefore this outcome could not be analyzed. However, these studies reported that preterm birth is related to a reduced agility, as assessed by the 4 × 10 test.
On the other hand, three studies [35, 44, 78] including seven group comparisons (n = 29,695, weighted average age at assessment = 7 years) assessed agility in individuals with LBW using the 10 × 5 m shuttle test or the 4 × 4 m square test. Their pooled analysis revealed a reduced agility in individuals with LBW compared to controls (SMD = −0.99, 95% CI = −1.91 to −0.07, p = 0.036; Fig. S6 (OSM)), albeit with signs of large heterogeneity (I2 = 99.7%).
3.3.5 Speed
Only data from one [58] and two studies [35, 44] were available for the meta-analysis of speed (assessed by 20-m or 50-m running tests) in preterm and LBW individuals, respectively, and therefore this outcome could not be analyzed. These studies found a reduced speed among preterm individuals compared to controls, but no differences when analyzing LBW.
3.4 Meta-Regressions
Meta-regression analyses could be performed on the influence of preterm birth and LBW on CRF and muscle strength. Analyses revealed a significant or quasi-significant trend towards a greater reduction of CRF in those individuals with a lower gestational age (p = 0.028, Fig. S7 (OSM)) or birthweight (p = 0.058, Fig. S8 (OSM)). Similarly, both a lower gestational age (p = 0.024, Fig. S9 (OSM)) and a lower birthweight (p < 0.001, Fig. S10 (OSM)) were associated with greater reductions in muscle strength. No significant associations were found in any case between the magnitude of the reductions in CRF or muscle strength and age at assessment (all p > 0.05, Figs. S11–S14 (OSM)).
4 Discussion
The present systematic review and meta-analysis [including 52 studies and 920,603 participants with a wide age range (from 4.7 to 34.4 years)] shows that both preterm birth and LBW are associated with a reduced physical fitness, as reflected by a lower CRF and muscle strength. Although the number of studies available precluded drawing strong conclusions on other fitness outcomes, our results also suggest that these conditions might also be associated with reductions in other fitness components, such as flexibility, or agility (which were reduced in individuals with LBW). Of note, a lower gestational age or birthweight seemed to be associated with greater reductions in physical fitness outcomes (at least for CRF and muscle strength, for which meta-regressions could be performed). No consistent associations were found between age at assessment and the magnitude of the reductions (see graphical summary of the results in Fig. 2).

Graphical summary of the study findings
The present findings are of potential clinical relevance due to the importance of physical fitness for both short- and long-term health. For instance, our results show that preterm individuals and those with LBW present a reduced CRF compared to controls (average differences in VO2max of 4.29 and 3.10 ml/kg/min, respectively). A lower CRF during youth is associated with a higher risk of obesity and cardiometabolic diseases in later years [19], and indeed CRF has proven to be a major prognostic factor of mortality in individuals of all ages [22]. Interestingly, each metabolic equivalent reduction in CRF (i.e., 3.5 ml/kg/min, which is approximately the difference observed in the present study) has been associated with a 11.6%, 16.1%, and 14.0% increase in all-cause, cardiovascular, and cancer mortality, respectively [80], which further supports the potential relevance of our findings. Similar findings were observed for muscle strength levels in the present study, which were also reduced in individuals born preterm or with LBW. Low muscle strength levels during childhood are likely to be maintained into adulthood [81, 82], and are associated with a greater cardiometabolic risk later in life [20]. Indeed, muscle strength has been inversely associated with mortality risk in young [83] and adult populations [21]. Therefore, although further research is warranted to confirm the long-term clinical relevance of the observed differences, preventive strategies are needed to counteract the reduction of physical fitness observed in individuals born preterm or with LBW. In this regard, physical exercise might be an effective option, as shown by a recent study that reported increases in VO2max in preterm individuals after 16 weeks of training [84].
The present findings expand on those from previous meta-analyses that provided preliminary evidence of reductions of physical fitness in individuals with LBW or preterm birth. Specifically, Edwards et al. found lower VO2max values (−2.20 ml/kg/min) in preterm individuals compared to their counterparts aged between 5 and 21 years [26]. Poole et al. also reported that participants aged over 18 years with very low birthweight had lower VO2max (−3.35 ml/kg/min) compared with their term-born peers [28]. In addition to confirming these findings, the present work suggests that preterm and LBW individuals might also show reductions in other major fitness outcomes such as muscle strength. This is in line with the meta-analysis by Dodds et al. [27], who reported a positive association between birthweight and muscle strength. Moreover, our results show reductions in other outcomes that to the best of our knowledge had not been previously meta-analyzed such as flexibility. Further research is, however, warranted to confirm whether other physical fitness components (e.g., agility, speed) are also reduced in these populations, as well as the mechanisms involved.
Another major finding of the present study derives from the meta-regression analyses. Similar to what has been reported for the risk of medical conditions [85], in the present study we found a trend toward greater reductions in physical fitness (specifically, CRF and muscle strength) with lower gestational age or birthweight. Confirming these trends, large cohort studies have also reported that birthweight is inversely associated with CRF and muscle strength [33, 34, 46]. Interestingly, our meta-regression analyses also suggest that the reductions in physical fitness associated with preterm birth or LBW seem not to be ameliorated at an older age, which is in line with the few longitudinal studies available on this topic. For instance, Pikel et al. [50] reported reductions in physical fitness components in preterm individuals after the period of childhood, some of which were maintained into early adulthood. Morrison et al. [48] found that individuals with LBW showed a similar change in grip strength from their mid-20s to their mid-30s, leading to consistently low levels in the former. Similarly, another longitudinal study reported that extremely preterm individuals showed a consistently lower physical fitness compared with those born at term through the school age, albeit only if they suffered from bronchopulmonary dysplasia [49]. Thus, preterm individuals not suffering from this condition progressively improved their fitness level through the school age, eventually reaching ‘normal’ values [49]. More research is therefore warranted to confirm these findings.
The present results might be at least partly explained by biological processes during pregnancy, which could be still evident at older ages. For instance, the association between gestational age and CRF might be explained by the late development of the lungs and cardiac chambers during pregnancy, which can lead to interrupted lung growth [86] in very preterm individuals. Dysanapsis might also be present in preterm individuals, that is, normal lung volumes and total cardiac size but smaller cardiac chambers and lung airways, which might impair expiratory airflow limitation [87]. Similarly, the reduction observed for other fitness outcomes such as muscle strength might also be related with essential processes in brain development that occur during the last weeks of gestation [88,89,90]. Moreover, although body composition was not analyzed in the present study, preterm individuals might also have a lower muscle mass and body mass index than their peers born at term [91], which might negatively influence fitness parameters such as muscle strength. It must be noted, nonetheless, that other behavioral or environmental factors such as the lower physical activity levels usually seen in preterm individuals might also be a confounding factor [92]. However, a recent study by our research group found reductions in several fitness components such as CRF, muscle strength, flexibility, and agility among preterm individuals compared to individuals born at term despite performing similar physical activity levels [24]. Thus, whether increasing physical activity levels can counteract the reduced fitness observed in individuals born preterm or with LBW remains to be elucidated.
4.1 Limitations and Strengths
Some limitations of the present study should be acknowledged. The limited number of available studies for some outcomes such as speed or agility hindered performing meta-analyses. Moreover, meta-regression analyses could not be performed for all outcomes, as ten or more studies were required [30]. The required data from some studies could not be obtained despite asking the corresponding authors, which made it impossible to include these studies in quantitative synthesis. In addition, variables such as physical activity, body mass index, delivery mode, or socioeconomic status could potentially confound our findings, as most included studies did not adjust their analyses for these variables. Moreover, the inclusion of individuals with extremely low gestational age or birthweight could overestimate the observed results. Another limitation that should be considered is the fact that in the present review we did not assess the effects of being born small for gestational age, which should be addressed in future research.
On the other hand, the major strengths of this study are having analyzed two highly prevalent conditions such as preterm birth and LBW, which could help in understanding the similarities between them. In this regard, it is worth noting that these conditions are highly interrelated, and many individuals may present both of them concomitantly. Indeed, we observed rather similar estimates for outcomes such as CRF (SMD = −0.38 and −0.40 for preterm and LBW, respectively), although research is warranted to confirm whether there can be differences for other outcomes such as muscle strength. Moreover, the wide variety of fitness-related outcomes included and the inclusion of meta-regression analyses can also be considered strengths of our study. The large sample size, including participants with a wide age range from several cohorts of different countries, can also be considered a strength of the study, although the present findings might not be necessarily applicable to all populations, as only one study came from a low-income country.
5 Conclusions
Both preterm birth and LBW seem to be associated with a reduced physical fitness, as reflected by lower values for outcomes such as CRF and muscle strength in an overall dose–response manner. Of note, the magnitude of these reductions seems overall independent of participants’ age at assessment, which suggests that these conditions are associated with reductions in physical fitness components not only during childhood, but also later in life. However, the magnitude of these reductions was inversely associated with both gestational age and birthweight. These findings might support the implementation of preventive strategies (e.g., fitness monitoring and lifelong exercise training) in these populations.
References
Howson C, Kinney M, Lawn J. Born too soon: the global action report on preterm birth. World Heal Organ. 2012;29:283–7.
Goldenberg RL, Culhane JF. Low birthweight in the United States. Am J Clin Nutr. 2007;85:584–90.
Chawanpaiboon S, Vogel JP, Moller AB, Lumbiganon P, Petzold M, Hogan D, et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Heal. 2019;7:e37-46.
WHO. Global nutrition targets. Low birth weight policy brief. World Heal Organ. 2025;2002(287):270.
Perin J, Mulick A, Yeung D, Villavicencio F, Lopez G, Strong K, et al. Global, regional, and national causes of under-5 mortality in 2000–19: an updated systematic analysis with implications for the sustainable development goals. Lancet Child Adolesc Heal. 2022;6:106–15. https://doi.org/10.1016/S2352-4642(21)00311-4.
Risnes K, Bilsteen J, Brown P, Pulakka A, Andersen A, Opdahl S, et al. Mortality among young adults born preterm and early term in 4 Nordic nations. JAMA Netw Open. 2021;4:1–12.
Crump C, Sundquist J, Winkleby M, Sundquist K. Gestational age at birth and mortality from infancy into mid-adulthood: a national cohort study. Lancet Child Adolesc Hea. 2019;3:408–17. https://doi.org/10.1016/S2352-4642(19)30108-7.
Metgud CS, Naik VA, Mallapur MD. Factors affecting birthweight of a newborn—a community based study in rural Karnataka, India. PLoS ONE. 2012;7: e40040.
Lawn JE, Wilczynska-Ketende K, Cousens SN. Estimating the causes of 4 million neonatal deaths in the year 2000. Int J Epidemiol. 2006;35:706–18.
Nugent JT, Lu Y, Deng Y. Effect measure modification by birth weight on the association between overweight or obesity and hypertension in children and adolescents. JAMA J Am Med Assoc. 2023;7:735–7.
Carr H, Cnattingius S, Granath F, Ludvigsson JF, EdstedtBonamy AK. Preterm birth and risk of heart failure up to early adulthood. J Am Coll Cardiol. 2017;69:2634–42.
De Jong F, Monuteaux MC, Van Elburg RM, Gillman MW, Belfort MB. Systematic review and meta-analysis of preterm birth and later systolic blood pressure. Hypertension. 2012;59:226–34.
Lewandowski AJ, Augustine D, Lamata P, Davis EF, Lazdam M, Francis J, et al. Preterm heart in adult life: cardiovascular magnetic resonance reveals distinct differences in left ventricular mass, geometry, and function. Circulation. 2013;127:197–206.
Lilja L, Bygdell M, Martikainen J, Rosengren A, Ohlsson C, Kindblom JM. Low birth weight as an early-life risk factor for adult stroke among men. J Pediatr. 2021;237:162-167.e4. https://doi.org/10.1016/j.jpeds.2021.06.050.
Crump C, Howell EA, Stroustrup A, McLaughlin MA, Sundquist J, Sundquist K. Association of preterm birth with risk of ischemic heart disease in adulthood. JAMA Pediatr. 2019;173:736–43.
Yang F, Janszky I, Gissler M, Cnattingius S, Roos N, Miao M, Yuan W, et al. Preterm birth, small for gestational age, and large for gestational age and the risk of atrial fibrillation up to middle age. JAMA Pediatr. 2023;177:599.
Kvaavik E, Klepp K, Tell GS, Meyer HE, Batty GD. Physical fitness and physical activity at age 13 years as predictors of cardiovascular disease risk factors at ages 15, 25, 33, and 40 years: extended follow-up of the Oslo youth study. Pediatrics. 2009;123:e80–6.
Mintjens S, Menting MD, Daams JG, Van PMNM, Roseboom TJ. Cardiorespiratory fitness in childhood and adolescence affects future cardiovascular risk factors: a systematic review of longitudinal studies. Sport Med. 2018;48:2577–605.
García-Hermoso A, Ramírez-Vélez R, García-Alonso Y, Alonso-Martínez A, Izquierdo M. Association of cardiorespiratory fitness levels during youth with health risk later in life: a systematic review and meta-analysis. JAMA Pediatr. 2020;174:952–60.
Fraser BJ, Blizzard L, Buscot MJ, Schmidt MD, Dwyer T, Venn AJ, et al. Muscular strength measured across the life-course and the metabolic syndrome. Nutr Metab Cardiovasc Dis. 2022;32:1131–7. https://doi.org/10.1016/j.numecd.2022.01.018.
García-Hermoso A, Cavero-Redondo I, Ramírez-Vélez R, Ruiz JR, Ortega FB, Lee DC, et al. Muscular strength as a predictor of all-cause mortality in an apparently healthy population: a systematic review and meta-analysis of data from approximately 2 million men and women. Arch Phys Med Rehabil. 2018;99:2100-2113.e5.
Kokkinos P, Faselis C, Samuel IBH, Pittaras A, Doumas M, Murphy R, et al. Cardiorespiratory fitness and mortality risk across the spectra of age, race, and sex. J Am Coll Cardiol. 2022;80:598–609.
Svedenkrans J, Kowalski J, Norman M, Bohlin K. Low exercise capacity increases the risk of low cognitive function in healthy young men born preterm: a population-based cohort study. PLoS ONE. 2016;11:1–12.
Martinez-Zamora MD, Valenzuela PL, Díez IE, Martínez-de-Quel Ó. Influence of preterm birth on physical fitness in early childhood. Eur J Sport Sci. 2023;23(11):2129–38. https://doi.org/10.1080/17461391.2023.2207082.
Smith L, Van Asperen P, McKay K, Selvadurai H, Fitzgerald D. Reduced exercise capacity in children born very preterm. Pediatrics. 2008;122:e287–93.
Edwards MO, Kotecha SJ, Lowe J, Watkins WJ, Henderson AJ, Kotecha S. Effect of preterm birth on exercise capacity: a systematic review and meta-analysis. Pediatr Pulmonol. 2015;50:293–301.
Dodds R, Denison HJ, Ntani G, Cooper R, Cooper C, Sayer AA, et al. Birth weight and muscle strength: a systematic review and meta-analysis. J Nutr Heal Aging. 2012;16:609–15.
Poole G, Harris C, Greenough A. Exercise capacity in very low birth weight adults: a systematic review and meta-analysis. Children. 2023;10:1–15.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2020;2021:372.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch V (editors). Cochrane handbook for systematic reviews of interventions version 6.4. Cochrane Database Syst Rev; 2023. Available from https://training.cochrane.org/handbook.
Dziuba E, Drzał-Grabiec J, Truszczyńska-Baszak A, Guzek K, Zajkiewicz K. Balance in children born prematurely currently aged 6–7. Biomed Hum Kinet. 2017;9:181–6.
Odd DE, Lingam R, Emond A, Whitelaw A. Movement outcomes of infants born moderate and late preterm. Acta Paediatr Int J Paediatr. 2013;102:876–82.
Ahlqvist VH, Persson M, Ortega FB, Tynelius P, Magnusson C, Berglind D. Birth weight and grip strength in young Swedish males: a longitudinal matched sibling analysis and across all body mass index ranges. Sci Rep. 2019;9:1–8.
Ahlqvist V, Persson M, Ortega F, Tynelius P, Magnusson C, Berglind D. Birth weight and cardiorespiratory fitness among young men born at term: the role of genetic and environmental factors. J Am Heart Assoc. 2020;9: e014290.
Moura-Dos-Santos M, Wellington-Barros J, Brito-Almeida M, Manhães-de-Castro R, Maia J, Góis LC. Permanent deficits in handgrip strength and running speed performance in low birthweight children. Am J Hum Biol. 2013;25:58–62.
Burns Y, Danks M, O’Callaghan M, Gray P, Cooper D, Poulsen L, et al. Motor coordination difficulties and physical fitness of extremely-low-birthweight children. Dev Med Child Neurol. 2009;51:136–42.
O’Dea CA, Logie K, Wilson AC, Pillow JJ, Murray C, Banton G, et al. Lung abnormalities do not influence aerobic capacity in school children born preterm. Eur J Appl Physiol. 2021;121:489–98. https://doi.org/10.1007/s00421-020-04530-2.
Svien L. Health-related fitness of seven-to-10-year-old children with histories of preterm birth. Pediatr Phys Ther. 2003;15(2):74–83.
Wells GA, Shea B, O’Connel D et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford htm. 1 February 2009; 2009.
Kriemler S, Keller H, Saigal S, Bar-Or O. Aerobic and lung performance in premature children with and without chronic lung disease of prematurity. Clin J Sport Med. 2005;15:349–55.
Clemm H, Røksund O, Thorsen E, Eide G, Markestad T, Halvorsen T. Aerobic capacity and exercise performance in young people born extremely preterm. Pediatrics. 2012;129:e97–105.
Clemm H, Vollsæter M, Røksund O, Markestad T, Halvorsen T. Adolescents who were born extremely preterm demonstrate modest decreases in exercise capacity. Acta Paediatr Int J Paediatr. 2015;104:1174–81.
Clemm H, Vollsæter M, Røksund O, Eide G, Markestad T, Halvorsen T. Exercise capacity after extremely preterm birth: development from adolescence to adulthood. Ann Am Thorac Soc. 2014;11:537–45.
Tchamo M, Santos M, Almeida M, Silva A, Leandro C. Physical fitness and birth weight in young men from Maputo City, Mozambique. Rev Bras Med do Esporte. 2016;22:66–70.
Svedenkrans J, Henckel E, Kowalski J, Norman M, Bohlin K. Long-term impact of preterm birth on exercise capacity in healthy young men: a national population-based cohort study. PLoS ONE. 2013;8(12): e80869.
Van Deutekom AW, Chinapaw MJM, Vrijkotte TGM, Gemke RJBJ. The association of birthweight and infant growth with physical fitness at 8–9 years of age—the ABCD study. Int J Obes. 2015;39:593–600. https://doi.org/10.1038/ijo.2014.204.
de Souza LV, de Meneck F, Parizotto GP, Franco M. Low birthweight and its relation to physical fitness parameters in children: its negative effect on muscle strength and cardiorespiratory endurance. Am J Hum Biol. 2022;34:1–8.
Morrison K, Gunn E, Guay S, Obeid J, Schmidt L, Saigal S. Grip strength is lower in adults born with extremely low birthweight compared to term-born controls. Pediatr Res. 2021;89:996–1003. https://doi.org/10.1038/s41390-020-1012-5.
Praprotnik M, StucinGantar I, Krivec U, Lucovnik M, Rodman Berlot J, Starc G. Physical fitness trajectories from childhood to adolescence in extremely preterm children: a longitudinal cohort study. Pediatr Pulmonol. 2023;58:1904–11.
RobičPikel T, Starc G, Strel J, Kovač M, Babnik J, Golja P. Impact of prematurity on exercise capacity and agility of children and youth aged 8 to 18. Early Hum Dev. 2017;110:39–45.
Lovering AT, Laurie SS, Elliott JE, Beasley KM, Yang X, Gust CE, et al. Normal pulmonary gas exchange efficiency and absence of exercise-induced arterial hypoxemia in adults with bronchopulmonary dysplasia. J Appl Physiol. 2013;115:1050–6.
Vrijlandt E, Gerritsen J, Boezen H, Grevink R, Duiverman E. Lung function and exercise capacity in young adults born prematurely. Am J Respir Crit Care Med. 2006;173:890–6.
Welsh L, Kirkby J, Lum S, Odendaal D, Marlow N, Derrick G, et al. The EPICure study: maximal exercise and physical activity in school children born extremely preterm. Thorax. 2010;65:165–71.
Caskey S, Gough A, Rowan S, Gillespie S, Clarke J, Riley M, et al. Structural and functional lung impairment in adult survivors of bronchopulmonary dysplasia. Ann Am Thorac Soc. 2016;13:1262–70.
Cheong JLY, Haikerwal A, Wark JD, Irving L, Garland SM, Patton GC, et al. Cardiovascular health profile at age 25 years in adults born extremely preterm or extremely low birthweight. Hypertension. 2020;76(6):1838–46.
Narang BJ, Manferdelli G, Kepic K, Sotiridis A, Osredkar D, Bourdillon N, et al. Effects of pre-term birth on the cardio-respiratory responses to hypoxic exercise in children. Life. 2022;12(1):79.
Cousins M, Hart K, Williams EM, Kotecha S. Impaired exercise outcomes with significant bronchodilator responsiveness in children with prematurity-associated obstructive lung disease. Pediatr Pulmonol. 2022;57:2161–71.
Kosiecz A, Chrościńska-Krawczyk M, Taczała J, Zawadka M. Evaluation of physical and cardiorespiratory fitness in 7-year-old prematurely born children—preliminary study. Ann Agric Environ Med. 2021;28:502–8.
Tikanmaki M, Tammelin T, Sipola-Leppänen M, Kaseva N, Matinolli H, Miettola S, et al. Physical fitness in young adults born preterm. Pediatrics. 2016. https://doi.org/10.1542/peds.2015-1289.
Evensen KAI, Steinshamn S, Tjønna AE, Stølen T, Høydal MA, Wisløff U, et al. Effects of preterm birth and fetal growth retardation on cardiovascular risk factors in young adulthood. Early Hum Dev. 2009;85:239–45. https://doi.org/10.1016/j.earlhumdev.2008.10.008.
Weigelt A, Bleck S, Huebner MJ, Rottermann K, Waellisch W, Morhart P, et al. Impact of premature birth on cardiopulmonary function in later life. Eur J Pediatr. 2023;182:3265–74. https://doi.org/10.1007/s00431-023-04952-y.
Tsopanoglou S, Davidson J, Dourado V, Goulart A, Barros M, dos Santos A. Aerobic capacity of preterm children with very low birth weight at school age and its associated factors. Arch Bronconeumol (English Ed). 2020;56:157–62. https://doi.org/10.1016/j.arbr.2019.05.022.
Ruf K, Thomas W, Brunner M, Speer CP, Hebestreit H. Diverging effects of premature birth and bronchopulmonary dysplasia on exercise capacity and physical activity—a case control study. Respir Res. 2019;20:1–9.
McKay L, Goss KN, Haraldsdottir K, Beshish AG, Barton GP, Palta M, et al. Decreased ventricular size and mass mediate the reduced exercise capacity in adolescents and adults born premature. Early Hum Dev. 2021;160: 105426. https://doi.org/10.1016/j.earlhumdev.2021.105426.
Huckstep OJ, Burchert H, Williamson W, Telles F, Tan CMJ, Bertagnolli M, et al. Impaired myocardial reserve underlies reduced exercise capacity and heart rate recovery in preterm-born young adults. Eur Heart J Cardiovasc Imaging. 2021;22:572–80.
Goss KN, Beshish AG, Barton GP, Haraldsdottir K, Levin TS, Tetri LH, et al. Early pulmonary vascular disease in young adults born preterm. Am J Respir Crit Care Med. 2018;198:1549–58.
Baraldi E, Zanconato S, Zorzi C, Santuz P, Benini F, Zaccheilo F. Exercise performance in very low birthweight children at the age of 7–12 years. Eur J Pediatr. 1991;1991:713–6.
Farrell E, Bates M, Pegelow D, Palta M, Eickhoff J, O’Brien M, et al. Pulmonary gas exchange and exercise capacity in adults born preterm. Ann Am Thorac Soc. 2015;12:1130–7.
Haraldsdottir K, Watson A, Pegelow D, Palta M, Tetri L, Levin T, et al. Blunted cardiac output response to exercise in adolescents born preterm. Eur J Appl Physiol. 2020;120:2547–54. https://doi.org/10.1007/s00421-020-04480-9.
Kilbride H, Gelatt M, Sabath R. Pulmonary function and exercise capacity for ELBW survivors in preadolescence: effect of neonatal chronic lung disease. J Pediatr. 2003;143:488–93.
Crispi F, Rodríguez-López M, Bernardino G, Sepúlveda-Martínez Á, Prat-González S, Pajuelo C, et al. Exercise capacity in young adults born small for gestational age. JAMA Cardiol. 2021;6:1308–16.
Yang J, Epton MJ, Harris SL, Horwood J, Kingsford RA, Troughton R, et al. Reduced exercise capacity in adults born at very low birth weight a population-based cohort study. Am J Respir Crit Care Med. 2022;205:88–98.
Rogers M, Fay T, Whitfield M, Tomlinson J, Grunau R. Aerobic capacity, strength, flexibility, and activity level in unimpaired extremely low birthweight (≤800 g) survivors at 17 years of age compared with term-born control subjects. Pediatrics. 2005;116:e58–65.
FitzGerald TL, Cameron KL, Albesher RA, Mentiplay BF, Lee KJ, Clark RA, et al. Strength, motor skills, and physical activity in preschool-aged children born either at less than 30 weeks of gestation or at term. Phys Ther. 2021;101:1–10.
Ito Y, Ito T, Sugiura H, Kidokoro H, Sugiyama Y, Mizusawa J, et al. Physical functions and gait performance in school-aged children born late preterm. Early Hum Dev. 2021;163: 105478. https://doi.org/10.1016/j.earlhumdev.2021.105478.
Bruun E, Pätsi P, Leskinen M, Björkman K, Kulmala P, Tulppo MP, et al. Preterm-born young women have weaker hand grip strength compared to their full-term-born peers. Children. 2023;10:1–13.
Ford GW, Kitchen WH, Doyle LW. Muscular strength at 5 years of children with a birthweight under 1500g. J Paediatr Child Health. 1988;24:295–6.
Cieśla E, Zaręba M, Kozieł S. The level of physical fitness in children aged 6–7 years with low birthweight. Early Hum Dev. 2017;111:23–9.
Pal A, Manna S, Dhara PC. Comparison between the motor function of school-aged children with normal birthweight and children with low birthweight: a cross-sectional study. Turk J Pediatr. 2019;61:374–85.
Imboden MT, Harber MP, Whaley MH, Finch WH, Bishop DL, Kaminsky LA. Cardiorespiratory fitness and mortality in healthy men and women. J Am Coll Cardiol. 2018;72:2283–92.
Fraser BJ, Blizzard L, Buscot MJ, Schmidt MD, Dwyer T, Venn AJ, et al. The association between grip strength measured in childhood, young- and mid-adulthood and prediabetes or type 2 diabetes in mid-adulthood. Sport Med. 2021;51:175–83. https://doi.org/10.1007/s40279-020-01328-2.
Fraser BJ, Blizzard L, Buscot MJ, Schmidt MD, Dwyer T, Venn AJ, et al. Muscular strength across the life course: The tracking and trajectory patterns of muscular strength between childhood and mid-adulthood in an Australian cohort. J Sci Med Sport. 2021;24:696–701. https://doi.org/10.1016/j.jsams.2021.01.011.
Ortega FB, Silventoinen K, Tynelius P, Rasmussen F. Muscular strength in male adolescents and premature death: cohort study of one million participants. BMJ. 2012;345:1–12.
Burchert H, Lapidaire W, Williamson W, McCourt A, Dockerill C, Woodward W, et al. Aerobic exercise training response in preterm-born young adults with elevated blood pressure and stage 1 hypertension: a randomized clinical trial. Am J Respir Crit Care Med. 2023;207:1227–36.
Dag Moster MD, Lie RT, Trond Markestad MD. Long-term medical and social consequences of preterm birth. Surv Anesthesiol. 2009;53:24.
O’Dea CA, Beaven ML, Wilson AC, Smith EF, Maiorana A, Simpson SJ. Preterm birth and exercise capacity: what do we currently know? Front Pediatr. 2023;11:1–7. https://doi.org/10.3389/fped.2023.1222731.
Duke JW, Lewandowski AJ, Abman SH, Lovering AT. Physiological aspects of cardiopulmonary dysanapsis on exercise in adults born preterm. J Physiol. 2021;3:463–82.
Hüppi PS, Warfield S, Kikinis R, Barnes PD, Zientara GP, Jolesz FA, et al. Quantitative magnetic resonance imaging of brain development in premature and mature newborns. Ann Neurol. 1998;43:224–35.
Li SJ, Tsao PN, Tu YK, Hsieh WS, Yao NJ, Wu YT, et al. Cognitive and motor development in preterm children from 6 to 36 months of age: Trajectories, risk factors and predictability. Early Hum Dev. 2022;172: 105634.
Williams J, Lee KJ, Anderson PJ. Prevalence of motor-skill impairment in preterm children who do not develop cerebral palsy: a systematic review. Dev Med Child Neurol. 2010;52:232–7.
Bertini G, Elia S, Dani C. Using ultrasound to examine muscle mass in preterm infants at term-equivalent age. Eur J Pediatr. 2021;180:461–8.
Nevill AM, Holder RL. Modelling handgrip strength in the presence of confounding variables: results from the Allied Dunbar National Fitness Survey. Adv Sport Leis Ergon. 2000;43(10):1547–58.
Acknowledgements
We sincerely thank Dr. Adrián Castillo García for designing the graphical abstract.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Authors’ Contributions
MMZ, OMDQ, and PLV designed the original idea. MMZ and CMM performed the systematic search and extracted the data. MMZ, CMM, and OMDQ performed the quality assessment. PLV performed the statistical analyses. MMZ and PLV drafted the original version of the manuscript. OMDQ and PLV supervised the study. All authors revised the manuscript critically for important intellectual content and approved the final version.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
PLV is supported by a Sara Borrell postdoctoral contract granted by Instituto de Salud Carlos III (CD21/00138).
Availability of Data and Material
Data are available upon request.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Martínez-Zamora, M.D., Martín-Martínez, C., Martínez-de-Quel, Ó. et al. Influence of Preterm Birth and Low Birthweight on Physical Fitness: A Systematic Review, Meta-Analysis, and Meta-Regression. Sports Med 54, 1907–1919 (2024). https://doi.org/10.1007/s40279-024-02026-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-024-02026-z