
Abstract
Background
Population preferences for care at the end of life can inform palliative care policy and direction. Research investigating preferences for care at the end of life has focused predominantly on the context of advanced cancer, with relatively little attention to other life-limiting illnesses that are common causes of death.
Objectives
We aimed to investigate preferences for the care of older people at the end of life in three different disease contexts. The purpose was to understand if population preferences for care in the last 3 weeks of life would differ for patients dying from cancer, heart failure or dementia.
Methods
Three discrete choice experiments were conducted in Australia with a general population sample using similar methods but different end-of-life disease contexts. Some attributes were common across the three experiments and others differed to accommodate the specific disease context. Each survey was completed by a different panel sample aged ≥45 years (cancer, n = 1548; dementia, n = 1549; heart failure, n = 1003). Analysis was by separate mixed logit models.
Results
The most important attributes across all three surveys were costs to the patient and family, patient symptoms and informal carer stress. The probability of choosing an alternative was lowest (0.18–0.29) when any one of these attributes was at the least favourable level, holding other attributes constant across alternatives. The cancer survey explored symptoms more specifically and found patient anxiety with a higher relative importance score than the symptom attribute of pain. Dementia was the only context where most respondents preferred to not have a medical intervention to prolong life; the probability of choosing an alternative with a feeding tube was 0.40 (95% confidence interval 0.36–0.43).
Conclusions
This study suggests a need for affordable services that focus on improving patient and carer well-being irrespective of the location of care, and this message is consistent across different disease contexts, including cancer, heart failure and dementia. It also suggests some different considerations in the context of people dying from dementia where medical intervention to prolong life was less desirable.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Community preferences for the care of older people at the end of life are similar across different disease contexts, with some differences in the dementia context where there is lower tolerance for measures to prolong life and higher tolerance for care and death in hospital. |
The most important aspects of care are patient comfort, approaches to reduce carer stress and cost, which are more important than place of care and place of death. |
Most palliative care services were designed around the needs of patients with cancer, and while there are similarities in preferences across disease contexts, the differences identified suggest a more nuanced disease-specific approach may improve well-being. |
1 Introduction
Palliative care policies in most high-income countries aim to support patient preferences for the care they receive toward the end of life, including the place of death, with the focus on providing most care outside of the acute hospital setting [1]. The policies referred to research findings that most people prefer to receive most care at home and to die at home [1]; consequently, the number of home deaths has become a quality measure for palliative care services [2]. Investigations of the extent to which care at the end of life matches patient preferences have focused on preference for place of death and found that for many patients, the preferred place of death was not known to the health service provider (either not discussed or not recorded) [3,4,5].
There is some evidence of differences across diseases in the type and location of care received at the end of life. Relative to people dying from cancer, those dying from a non-cancer, life-limiting illness are less likely to receive specialist palliative care (either in the community or as an inpatient) and are likely to receive it for a shorter period [6,7,8]. Patients receiving specialist palliative care programmes were also found to use fewer acute care services and to be more likely to die at home or in a nursing home [9, 10]. The extent to which these different patterns of care align with patient or community preferences in different disease contexts is unknown.
The research on preferences for place of care and death finds substantial heterogeneity in preferences among patients and informal carers [11]. Many studies among the general population do not use questions that include contextual information [11], which would allow respondents to understand the trade-offs when choosing place of care. Although qualitative research has found that the preferences of patients and carers for place of care and place of death were not necessarily clear or stable and were conditional on various aspects of the patient’s condition and the caregiver’s coping [12].
Discrete choice experiments (DCEs) allow for the measurement of the trade-offs people make between the different features described in hypothetical end-of-life care scenarios and thus capture more of the contextual factors that influence such preferences. DCEs have been used in end-of-life studies, with many focused on preferences for life extension over a relatively limited number of other aspects of end-of-life care. Generally, these studies (among different populations) have found pain control to be prioritised over other attributes, with quality of life, cost of care and length of life also highly ranked [13]. These other aspects of care were found to be more important than place of care and place of death among both bereaved carers [14] and a general population sample [15].
While DCEs provide a useful method for investigating the trade-offs people are willing to make regarding care at the end of life, most of the DCE research has focused on the context of advanced cancer [13]. However, little is known about preferences for care at the end of life in other disease contexts where the symptoms, patterns of functional decline and potential for use of life-extending therapies may be different. The purpose of this study was to investigate community preferences for the care of older people at the end of life in different disease contexts. The study focuses on care in the latter stages of a life-limiting illness, including the use of life-sustaining measures and the preferred location of care over the last 3 weeks of life, as well as the preferred location of death. We used DCE methods and contrasted preferences in three different disease contexts.
2 Methods
Three DCEs using similar methods but different end-of-life disease contexts were conducted in Australia to ascertain preferences for the care of an older person over the last 3 weeks of life. The three end-of-life disease contexts were advanced cancer, heart failure and dementia, which represent the most common causes of death among older Australians [16]. The dementia experiment used two patient contexts, where the patient lived at home or in a nursing home, while the cancer and heart failure experiments each used a single patient context where the patient lived at home. The last 3 weeks of life were used to capture the preferences and trade-offs people might make in the period near to death when in most cases the patient would be expected to have significant decline in functional capacity and extremely high need for supportive care. Different choices and trade-offs are likely to be required over longer periods before death.
Data were collected through separate online surveys conducted over separate 3- to 4-week periods in November–December 2019 (cancer), March–April 2020 (dementia) and October 2021 (heart failure). The first experiment (cancer) was reported previously [15]. Participants indicated consent by proceeding with the survey after reading the information page.
2.1 Sample
Each experiment recruited a separate general population sample aged ≥45 years through three online survey panel providers. This age group was selected because of the focus of the study on older people and because it was likely to include large numbers of people with chronic conditions, as well as those most likely to be informal carers and surrogate decision makers [17]. We used general population samples as they are widely used in health economics studies, including health preference surveys where they are seen as providing preferences that are more representative of those of the community than patient and carer samples. This is particularly the case in the context of care at the end of life where recruitment for such a challenging survey when the patient is approaching death is extremely difficult. Furthermore, patient preferences for place of care and place of death are specific to the individual context and have been found to change as disease progresses [12, 18, 19], suggesting that other factors become more important as the individual context changes. This makes single point-in-time patient preferences a less useful basis for health care policy (although essential for individual decision making at that time).
The sample completing the cancer survey (n = 1548) was recruited in 2019 through Toluna Australia, the sample completing the dementia survey (n = 1549) was recruited through Toluna and Dynata in 2020, and the sample completing the heart failure survey (n = 1003) was recruited through Pureprofile and Dynata in 2021. Recruitment used quotas to ensure each sample represented the Australian population aged ≥45 years in terms of age group and sex. All three surveys were administered using the SurveyEngine online platform so that the survey appearance was consistent across the three surveys.
2.2 Survey
Each survey included background information and sociodemographic questions in addition to the DCE section. The surveys included an initial explanation of the purpose of the study and information about different types and locations of end-of-life care, as well as a description of the DCE questions and how to answer them (including an example). In each survey, there was also information about how to access additional explanatory information about each attribute using pop-ups. Questions about demographic characteristics and prior experience of the death of someone close were included to describe the sample and to examine if preferences differed by experience.
2.2.1 Discrete Choice Experiments (DCE) Section
The DCE questions of each survey focused on the last 3 weeks of life for a person with advanced disease, either cancer, dementia, or heart failure. Each choice set asked which of two hypothetical completed end-of-life trajectories the respondent considered to be better. The DCE section of each survey began with a vignette describing a patient’s condition over the last 3 weeks of life for a person aged 85 years. For the dementia survey, this was in two parts; one part described a person with dementia living at home (vignette 1), while the other part was a person with dementia living in a residential aged care facility or nursing home (vignette 2). Respondents were asked to think about this person when they answered the questions that followed. Each respondent was shown 11 choice sets (cancer) or 12 choice sets (dementia and heart failure); the 12 dementia choice sets included 6 for each vignette. Each choice set included two completed care trajectories for the hypothetical person described in the vignette. For each choice set, the respondent was asked “Which care option do you think is better?”.
The attributes and levels covered the location of care throughout the last 3 weeks of life, the location of death, disease symptoms experienced by the patient, the use of life-extending therapies and the types of supportive care available, as well as the impact on informal carers and the cost to the patient and family. Each survey was developed using the process described previously [15], with initial attributes developed from previous research [18, 20,21,22] and a workshop conducted with the research team, including palliative care clinicians and consumer representatives with experience in supporting a close family member at the end of life. The survey was then further developed through feedback from pilot studies and a meeting in which consumer representatives completed the online survey and provided feedback during and after completion.
The final list of attributes and levels for each survey is given in Table 1. There were five attributes with identical levels across the three surveys, while the others varied to accommodate the disease-specific context, including disease symptoms, medical intervention, place of care and place of death (see Table 1).
2.3 DCE Design
A separate design was constructed for each of the three surveys using similar methods. As each survey had between 10 and 12 attributes, each design was constructed to ensure that only 6 or 7 attributes varied between the alternatives in each choice set, and this was indicated with coloured highlighting in the choice set presentation [23,24,25]. In addition to reducing the cognitive burden, this avoids the respondent basing the choice on only one attribute as there will always be some choice sets where an attribute is the same across alternatives, forcing respondents to base their choice on other attributes.
A separate generator-developed design [26] was constructed for each survey and for each vignette in the dementia survey. In each case, the initial (starting) design was an orthogonal main effects plan, with ‘place of care’ and ‘place of death’ combined into one location attribute. To get the choice sets, different generators were then added in turn to the initial design. Some of the entries in each generator were 0 to ensure that only 6 or 7 attributes varied between options in each choice set. A detailed description of the approach used is provided by Kenny et al. [15]. The heart failure design required one further constraint to ensure that ‘place of death’ level 4 (intensive care) was aligned with ‘intervention’ levels 3 or 4 (which involved treatment in intensive care). The resulting designs were divided into versions such that there was one choice set from each generator in each version. Thus, the cancer survey design had 352 choice sets divided into 32 versions of 11, the dementia design had 384 choice sets divided into 32 versions of 12 (6 from each vignette), and the heart failure design had 288 choice sets divided into 24 versions of 12. Participants were randomly assigned to versions and the order in which each participant saw the choice sets within each version was also randomised. For the dementia survey, the order in which participants were shown vignettes 1 and 2 (each followed by 6 related choice sets) was randomised prior to the randomisation of order of the choice sets within each set of 6. Example choice sets are shown in the Online Resource (Figs. S1–S4).
2.4 Analysis
Separate analyses were conducted for each survey and the two dementia survey vignette components, using the same analysis method. We used this approach because the differences in some of the attributes were such that it was not possible to analyse the three surveys in a single model. The mixed logit model [27] was used for each analysis, estimated by maximum simulated likelihood in R [28] using the logitr package [29]. The simulation used 2000 Sobol draws, which are recommended when the number of random parameters is large [30]. Attribute levels were dummy coded, with level 1 (Table 1) used as the reference level for each attribute in all models. The estimates from the mixed logit models were used to estimate the relative attribute importance and predicted probabilities. The relative attribute importance scores were estimated using a profile-based normalisation [31] that estimates the proportion of total utility in a model that is represented by an attribute. The 95% confidence interval (CIs) were based on standard errors estimated in R using the delta method [32] implemented in the msm package [33]. The predicted probabilities were estimated as the probability of choosing an alternative when the attribute is set to the specified level in that alternative and to the reference level in the other alternative, holding all other attributes equal across the alternatives. The logitr post-estimation predict command was used to estimate the predicted probabilities and 95% CIs. This command incorporates heterogeneity by simulating draws from the population estimates of the mixed logit model [29].
We also conducted additional analyses to investigate the impact of prior experience with death and end-of-life care on preferences. We used separate mixed logit models, and in each model included attribute interactions with two indicator variables: (1) experience with the death of a close person due to life-limiting illness; and (2) experience of having helped with the care of someone who died from a life-limiting illness.
3 Results
The online survey completion rates ranged from 55 to 68%. The three samples were similar to the Australian population aged ≥45 years on most characteristics (see Table 2). All three samples included fewer people aged ≥85 years (1% instead of 5%), with overrepresentation of those aged 75–84 years due to the oldest quota segment being set at ≥75 years. The majority had previous experience of someone close dying from a chronic disease (72–74%) and about one-third had previously provided care for someone at the end of life (30–33%).
3.1 Relative Attribute Importance
The most important attributes across all three surveys were costs, patient symptoms and informal carer stress (see Fig. 1). In relation to symptoms, the cancer survey also included an attribute about patient anxiety, which had a higher relative importance score than the symptom attribute of pain. The cost to the patient and family was given the highest importance in all surveys, representing between 21 and 25% of total utility in each model, while the attributes indicating how the patient and the informal carer were feeling each represented between 13 and 19%.

Relative attribute importance for each disease context. Symptoms were pain for cancer, agitation for dementia and breathlessness for heart failure. CI confidence interval
3.2 Predicted Probability of Choosing an Alternative
The impact of each attribute level on the probability of choosing a care alternative and the 95% CI is shown in Fig. 2. The dashed line at 0.5 indicates indifference between alternatives, and probabilities <0.5 indicate a preference to not have an alternative with this attribute level (Fig. 2). This figure shows similar patterns across the different disease contexts for most attributes, with the lowest probability of choosing an alternative associated with a cost of $4000 to the patient and family for care over the last 3 weeks of life (probability of choosing 0.18–0.23). The worst levels of patient symptoms and carer stress were also associated with an extremely low probability of choosing an alternative with this attribute level (probability of 0.22–0.27 for patient symptoms, and probability of 0.19–0.29 for carer stress) (see Fig. 2). The model coefficients for these attributes were significantly different from zero (p < 0.001) [see Online Resource Table S1] and the 95% CIs for the predicted probabilities did not include 0.5 (indifference between alternatives).

Predicted probability1 of choosing an alternative at each attribute level for the different disease contexts. Symptoms were pain for cancer, agitation for dementia, and breathlessness for heart failure. A probability of 0.5 indicates indifference between alternatives with and without this attribute level. 1Probability of choosing when the attribute is at the level specified and all other attributes are at the reference level. NH nursing home (treated as home for dementia patients living in a nursing home), ICU intensive care unit
There were some important differences across the different disease contexts. There was either indifference to having most medical interventions to prolong life or a small preference to have these for cancer and heart disease patients. However, for dementia, there was a preference to not have alternatives, including a ‘feeding tube (through the abdomen)’ to prolong life (probability 0.40, 95% CI 0.36–0.43 for both vignettes) (see Fig. 2). There was a small significant preference to have antibiotics across all contexts except for dementia Vignette 2 (living in a nursing home). There was no significant preference related to using a drip for fluids in the context of cancer or dementia and no significant preference related to interventions requiring admission to intensive care in the heart failure context.
There was also a difference in preferences related to alertness where there was a preference for alternatives where the patient was not sleepy during the day in the cancer context (probability 0.43, 95% CI 0.41–0.45), but a preference for the patient to be sleeping most of the time in the dementia context (probability 0.61, 95% CI 0.58–0.63 for both vignettes). The wording of this attribute did differ between the two disease contexts where the reference level was ‘awake and able to interact’ in the cancer context and ‘awake intermittently but confused’ in the dementia context, which was in keeping with the most likely scenario at the advanced stage of these diseases (see Table 1).
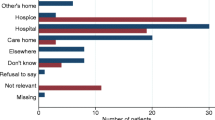
The preferences related to the location of care and of death showed that most people preferred alternatives where most of the last 3 weeks was not spent in hospital in the cancer (probability 0.44, 95% CI 0.42–0.47) and heart failure (probability 0.45, 95% CI 0.42–0.48) contexts, but that there was no significant preference related to this attribute level in the dementia context (probability 0.49, 95% CI 0.46–0.56 Vignette 1, and 95% CI 0.44–0.54 Vignette 2). There was also a slight preference for alternatives that did not include death in hospital in the cancer (probability 0.46, 95% CI 0.43–0.49) and heart failure (probability 0.41, 95% CI 0.38–0.44) contexts, although this was not the case in the dementia context. There was also a preference to not die in the intensive care unit in the heart failure context (probability 0.39, 95% CI 0.36–0.42) (see Fig. 2). Across all disease contexts, there was no significant difference in preferences between dying in a palliative care unit or dying at home (or the nursing home when that is where the person with dementia lived).
3.3 Preference Heterogeneity
There was substantial heterogeneity across all disease contexts for some attribute levels, which is illustrated in Fig. 3; this shows the mean coefficient and interquartile range for the random parameters from each mixed logit model (where the line at 0 indicates indifference between alternatives with or without the attribute level). Some of the attribute levels having the largest impact on preferences (cost of $4000, the most severe level of symptoms, and the carer stressed all of the time) showed substantial heterogeneity but the differences were in strength of preference rather than the direction. The feeding tube intervention in the dementia context showed heterogeneity where some respondents preferred this, although the majority preferred not to have this (Fig. 3). Place of death also showed heterogeneity for all disease contexts where some people preferred death in a palliative care unit or in hospital rather than at home, while some preferred death at home (Fig. 3). In the dementia context Vignette 1 (living at home), death in a nursing home also showed heterogeneity, where some people preferred this to death at home while others preferred death at home (Fig. 3).

Distribution of coefficients1 from the mixed logit models (mean and interquartile range). 1Based on 10,000 draws from the normal distribution of the random parameters. NH nursing home, ICU intensive care unit
Analysis of the impact of prior experience with death or end-of-life caregiving found only a small number of attributes where preferences differed between those with and without prior experience of death from life-limiting illness or of helping to care for someone at the end of life. The predicted probabilities for attributes where at least one level differed by experience are shown in Fig. 4, and the models from which the predictions were estimated are shown in the Online Resource Tables S2a and S2b. Across all disease contexts, those who reported having helped with the care of a friend or relative at the end of life were less concerned about a cost of $4000 than those without this experience (see Fig. 4). This difference was in terms of the size of this effect but did not change its direction (predicted probabilities 0.16–0.20 for those without experience of death and 0.23–0.28 for those who had helped with care). The proportions of former carers reporting an annual household income of $100,000 or more was higher among carers than non-carers for the heart failure survey but not for the cancer and dementia surveys (heart failure 35% vs. 25%, p = 0.003; cancer 25% vs. 21%, p = 0.063; dementia 27% vs. 26%, p = 0.602, Fisher’s exact test). No other significant interactions were identified across all disease contexts. There were some additional small differences in preferences by experience that were specific to one or two disease contexts. These are shown in Fig. 4 and are outlined in detail in the Online Resource.

Predicted probability1 of choosing an alternative: experience with death and end-of-life caregiving interactions. 1Probability of choosing when the attribute is at the level specified and all other attributes are at the reference level. Symptoms were pain for cancer, agitation for dementia, and breathlessness for heart failure. A probability of 0.5 indicates indifference between alternatives with and without this attribute level. Exp1 no experience with life-limiting illness, Exp2 someone close died from life-limiting illness, Exp3 helped care for someone at the end of life, NH nursing home (treated as home for dementia patients living in a nursing home), ICU intensive care unit
4 Discussion
This study examined the preferences of middle aged and older Australians for care in the last 3 weeks of life across three different disease contexts and found similar preferences for most attributes. In particular, the most important attributes across all contexts were the cost to the patient and family, symptoms experienced by the patient, and stress experienced by the informal carer. Interpretation of the importance of cost is not straightforward; rather than indicating a willingness to pay or value for care, this could be an indication that respondents felt families should not be asked to meet these costs through out-of-pocket payments. We did identify some key differences in the dementia context where respondents preferred not to use the most extreme medical intervention (a feeding tube), preferred the patient to be sleeping most of the time, and were not concerned about the patient spending most of the last 3 weeks of life in hospital or dying in hospital. In the cancer and heart failure contexts, there was a preference to not spend most of the time in hospital and to not die in hospital, although these effects were small relative to other aspects of care. There was also a preference to not die in intensive care in the heart failure context. There was considerable preference heterogeneity and most of this was not explained by participant experience with death or with care at the end of life.
The results suggest that the most important aspects of care, irrespective of the illness, are patient comfort, carer coping, and costs to the patient and family, which is consistent with the findings of other DCE studies where pain control, quality of life and the costs of care to the patient were found to be highly ranked attributes [13]. However, our finding is more nuanced for dementia patients (relative to the cancer and heart failure contexts) in terms of lower tolerance for medical intervention to prolong life, higher tolerance of care and death in hospital, and a preference to not have the patient awake in the final weeks. Most of the evidence on preferences for care at the end of life is in the context of advanced cancer or does not specify a disease context [11, 13, 34], and this study adds information on preferences in the context of heart failure and dementia where preferences are relatively underresearched.
The high importance given to costs to the patient and family when there was a cost of $4000 is consistent with the expectation of access to health care at no or low cost in Australia. There is little published information about patient out-of-pocket costs for care at the end of life in Australia. However, while most people have access to free inpatient care in the public sector, there can be costs for care at home, including co-payments for subsidised medicines and medical services, costs for equipment and costs for respite or additional support for the carer beyond what is available through the publicly funded services.
Our finding of a preference to die at home rather than the acute hospital setting for heart failure patients is to some extent consistent with studies among patients with advanced heart failure where most preferred to remain at home [19, 35]. In contrast, our study found no significant difference between home and a palliative care unit. For dementia patients, we found that most respondents preferred to not use a feeding tube to prolong life in the last 3 weeks (irrespective of place of residence) but that some participants had different views on this issue. This is consistent with a previous general population study finding that just over half of respondents would not insert a feeding tube at the end stages of neurological disease where the patient did not have decision-making capacity, but that some respondents preferred this if the patient did not resist and some regardless of patient resistance [36]. Two recent reviews found insufficient evidence to support the benefits of enteral feeding in people with advanced dementia in terms of either quantity or quality of life [37, 38]. Consistent with our findings, qualitative research among people with dementia or their carers found relatively little emphasis on place of death [39,40,41]. Some qualitative studies reported that people with dementia (even at an early stage) had difficulty thinking about the future and what their preferences might be near death [39, 40].
End-of-life care is difficult to research as patients and carers in this phase of illness are dealing with a range of complex physical and psychosocial issues. Not surprisingly, they are often lacking the time, energy, or inclination to participate in research. The limitations of our study are those that generally apply to this approach. There were fewer respondents in the oldest age group than in the Australian population; however, our sample matched the population on several other characteristics. The use of a community sample could be seen as a poor proxy as they may not understand the situation they are evaluating. We chose an older age group to survey, and, as expected, many had experienced the illness and death of someone close. It is possible that preferences may have been different in a younger sample, although there were relatively few differences between those with and without experience of someone close dying of a life-limiting illness or of providing care in our older sample; the differences identified were small and mostly related to the size rather than the direction of the effect. Although culture and ethnicity can be important factors in preferences at the end of life, we were not able to examine this issue in the current study. The three surveys were conducted at different timepoints and among different samples. It is possible that the coronavirus disease 2019 (COVID-19) pandemic, which was ongoing during data collection for the dementia and heart failure surveys, may have influenced preferences. However, the consistency of the main results across the three surveys suggests that this was minimal. We worked with consumers to design the attributes and choice sets to ensure that these were realistic and comprehensible. We avoided the need for respondents to assess probabilities by presenting completed trajectories for patients rather than asking what they would choose for themselves in similar circumstances. While these stated preferences can be a good guide to policy, they should not be taken as indicative of an individual’s choices should they be in those circumstances.
It is important to note that our results do not replace the need for clinicians to elicit individual patient preferences repeatedly throughout the care trajectory to ensure that care at the end of life is patient-centred. Rather, the implications of our findings are about what can be done to make dying easier wherever that happens, so that the preferences of patients and their families might be accommodated at each stage of the process.
5 Conclusion
Most countries face the challenge of providing health care services to support increasing numbers of older people dying from a life-limiting illness. This study suggests a need for affordable services that focus on improving patient and carer wellbeing irrespective of the location of care, and this message is consistent across different disease contexts, including cancer, heart failure and dementia. It also suggests some different considerations in the context of people dying from dementia where medical intervention to prolong life was less desirable. This is important information when declining cognitive functioning makes it difficult to ensure care meets a patient’s preference. Overall, the similarity of preferences across different diseases suggests that greater access to palliative care services could meet community preferences for care at the end of life.
References
Robinson J, Gott M, Gardiner C, Ingleton C. The ‘problematisation’ of palliative care in hospital: an exploratory review of international palliative care policy in five countries. BMC Palliat Care. 2016;15:64.
Hoare S, Antunes B, Kelly MP, Barclay S. End-of-life care quality measures: Beyond place of death. BMJ Support Palliat Care. 2022. https://doi.org/10.1136/spcare-2022-003841.
Ali M, Capel M, Jones G, Gazi T. The importance of identifying preferred place of death. BMJ Support Palliat Care. 2019;9(1):84–91.
De Roo ML, Miccinesi G, Onwuteaka-Philipsen BD, et al. Actual and preferred place of death of home-dwelling patients in four european countries: Making sense of quality indicators. PLoS One. 2014;9: e93762.
Hunt KJ, Shlomo N, Addington-Hall J. End-of-life care and achieving preferences for place of death in england: results of a population-based survey using the voices-sf questionnaire. Palliat Med. 2014;28:412–21.
Quinn KL, Wegier P, Stukel TA, et al. Comparison of palliative care delivery in the last year of life between adults with terminal noncancer illness or cancer. JAMA Netw Open. 2021;4: e210677.
Qureshi D, Tanuseputro P, Perez R, Seow H. Place of care trajectories in the last two weeks of life: a population-based cohort study of ontario decedents. J Palliat Med. 2018;21:1588–95.
Rosenwax L, Spilsbury K, McNamara BA, Semmens JB. A retrospective population based cohort study of access to specialist palliative care in the last year of life: Who is still missing out a decade on? BMC Palliat Care. 2016;15:46.
Quinn KL, Stukel T, Stall NM, et al. Association between palliative care and healthcare outcomes among adults with terminal non-cancer illness: population based matched cohort study. BMJ. 2020;370: m2257.
Seow H, Dhaliwal G, Fassbender K, et al. The effect of community-based specialist palliative care teams on place of care. J Palliat Med. 2016;19:16–21.
Gomes B, Calanzani N, Gysels M, Hall S, Higginson I. Heterogeneity and changes in preferences for dying at home: a systematic review. BMC Palliat Care. 2013;12:7.
Gerber K, Hayes B, Bryant C. “It all depends!”: a qualitative study of preferences for place of care and place of death in terminally ill patients and their family caregivers. Palliat Med. 2019;33:802–11.
Xia Q, Kularatna M, Virdun C, et al. Preferences for palliative and end-of-life care: a systematic review of discrete choice experiments. Value Health. 2023;26(12):1795–809.
Sepulveda JMG, Baid D, Johnson FR, Finkelstein EA. What is a good death? A choice experiment on care indicators for patients at end of life. J Pain Symptom Manage. 2022;63:457–67.
Kenny P, Street DJ, Hall J, Agar M, Phillips J. Valuing end-of-life care for older people with advanced cancer: Is dying at home important? Patient. 2021;14:803–13.
Australian Institute of Health and Welfare. Deaths in australia. Available at: https://www.aihw.gov.au/reports/life-expectancy-death/deaths-in-australia/contents/about. Accessed 20 Jul 2023.
Australian Bureau of Statistics. Disability, Ageing and Aarers, Australia: Summary of findings. Available at: https://www.abs.gov.au/statistics/health/disability/disability-ageing-and-carers-australia-summary-findings/. Accessed 22 Jan 2024.
Agar M, Currow DC, Shelby-James TM, et al. Preference for place of care and place of death in palliative care: Are these different questions? Palliat Med. 2008;22:787–95.
Malhotra C, Bundoc FG, Sim D, Jaufeerally FR, Finkelstein EA. Instability in preference for place of death among patients with symptoms of advanced heart failure. J Am Med Direct Assoc. 2021;22:e29–34.
Hall J, Kenny P, Hossain I, Street DJ, Knox SA. Providing informal care in terminal illness: an analysis of preferences for support using a discrete choice experiment. Med Decis Making. 2014;34:731–45.
Virdun C, Luckett T, Davidson PM, Phillips J. Dying in the hospital setting: a systematic review of quantitative studies identifying the elements of end-of-life care that patients and their families rank as being most important. Palliat Med. 2015;29:774–96.
Zapart S, Kenny P, Hall J, Servis B, Wiley S. Home-based palliative care in sydney, Australia: the carer’s perspective on the provision of informal care. Health Soc Care Community. 2007;15:97–107.
Jonker MF, Donkers B, de Bekker-Grob E, Stolk EA. Attribute level overlap (and color coding) can reduce task complexity, improve choice consistency, and decrease the dropout rate in discrete choice experiments. Health Econ. 2019;28:350–63.
Mulhern B, Norman R, Shah K, et al. How should discrete choice experiments with duration choice sets be presented for the valuation of health states? Med Decis Making. 2018;38:306–18.
Norman R, Viney R, Aaronson NK, et al. Using a discrete choice experiment to value the QLU-C10D: Feasibility and sensitivity to presentation format. Qual Life Res. 2016;25:637–49.
Street D, Burgess L. The construction of stated choice experiments. Hoboken: John Wiley & Sons Inc.; 2007.
Train K. Discrete choice methods with simulation. New York: Cambridge University Press; 2003.
R Core Team (2015). R: A language and environment for statistical computing. R Foundation for Statistical Computing. Available at: http://www.R-project.org/
Helveston JP. Logitr: Fast estimation of multinomial and mixed logit models with preference space and willingness-to-pay space utility parameterizations. J Stat Softw. 2023;105:1–37.
Czajkowski M, Budziński W. Simulation error in maximum likelihood estimation of discrete choice models. J Choice Modell. 2019;31:73–85.
Gonzalez JM. A guide to measuring and interpreting attribute importance. Patient. 2019;12:287–95.
Oehlert GW. A note on the delta method. Am Stat. 1992;46:27–9.
Jackson C. Multi-state modelling with r: The msm package. CRAN. Available at: https://CRAN.R-project.org/package=msm
Woodman C, Baillie J, Sivell S. The preferences and perspectives of family caregivers towards place of care for their relatives at the end-of-life. A systematic review and thematic synthesis of the qualitative evidence. BMJ Support Palliat Care. 2016;6:418–29.
Kitakata H, Kohno T, Kohsaka S, et al. Preferences on advance care planning and end-of-life care in patients hospitalized for heart failure. ESC Heart Failure. 2021;8:5102–11.
Clarke G, Fistein E, Holland A, et al. Preferences for care towards the end of life when decision-making capacity may be impaired: a large scale cross-sectional survey of public attitudes in Great Britain and the United States. PLoS One. 2017;12: e0172104.
Davies N, Barrado-Martín Y, Vickerstaff V, et al. Enteral tube feeding for people with severe dementia. Cochrane Database Syst Rev. 2021;8: CD013503.
Lee YF, Hsu TW, Liang CS, et al. The efficacy and safety of tube feeding in advanced dementia patients: a systemic review and meta-analysis study. J Am Med Dir Assoc. 2021;22:357–63.
Bamford C, Lee R, McLellan E, et al. What enables good end of life care for people with dementia? A multi-method qualitative study with key stakeholders. BMC Geriatr. 2018;18:302.
Dening KH, Jones L, Sampson EL. Preferences for end-of-life care: a nominal group study of people with dementia and their family carers. Palliat Med. 2013;27:409–17.
Mulqueen K, Coffey A. Preferences of residents with dementia for end of life care. Nurs Older People. 2017;29:26–30.
Acknowledgements
The authors thank Imelda Gilmore, Meg Brassil, Bev Noble and Noelene Trotter who, as consumers, provided invaluable advice and assistance with the DCE survey development, drawing on their personal experience as end-of-life family carers.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was supported by a National Health and Medical Research Council project grant (ID 1159202).
Conflicts of Interest
Patricia Kenny, Deborah J. Street, Jane Hall, Meera R. Agar, and Jane Phillips have no conflicts of interest to declare.
Availability of Data and Material
Data are not publicly available due to current ethics approval. The authors will consider requests for data access and may submit an ethics amendment application if appropriate.
Ethics Approval
This study was approved by the University of Technology Sydney Human Research Ethics Committee (UTS HREC REF NO. ETH19-3313).
Authors’ Contributions
All authors contributed to the conception and design of the work, obtaining funding and interpretation of the results. Deborah Street devised the designed experiment for each DCE and Patricia Kenny analysed the data and drafted the manuscript. All authors contributed to critical revision of the manuscript and approved the final version.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Kenny, P., Street, D.J., Hall, J. et al. Community Preferences for the Care of Older People at the End of Life: How Important is the Disease Context?. Patient 17, 407–419 (2024). https://doi.org/10.1007/s40271-024-00675-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-024-00675-w