
Abstract
Eplontersen (Wainua™) is a ligand-conjugated antisense oligonucleotide directed to TTR, which is being developed by Ionis Pharmaceuticals and AstraZeneca for the treatment of TTR-mediated amyloidosis (ATTR). Eplontersen, which is targeted to the liver by a ligand containing three N-acetyl galactosamine residues, binds to wild-type and variant TTR mRNA, thus reducing the levels of circulating TTR protein and amyloid deposition. Subcutaneous eplontersen reduced serum TTR levels, inhibited neuropathy progression and improved health-related quality of life in patients with polyneuropathy of hereditary ATTR (ATTRv-PN; v for variant) in a phase III trial. Based on these results, eplontersen was approved in the USA for the treatment of ATTRv-PN on 21 December 2023 and is currently undergoing regulatory review for a similar indication in the EU, the UK, Switzerland and Canada. Eplontersen is also undergoing phase III development for ATTR cardiomyopathy. This article summarizes the milestones in the development of eplontersen leading to this first approval for ATTRv-PN.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Digital Features for this AdisInsight Report can be found at https://doi.org/10.6084/m9.figshare.25155782. |
A ligand-conjugated antisense oligonucleotide being developed by Ionis Pharmaceuticals and AstraZeneca for the treatment of ATTR |
Received its first approval on 21 December 2023 in the USA |
Approved for use in adults with ATTRv-PN |
1 Introduction
Eplontersen (Wainua™), a ligand-conjugated antisense oligonucleotide that inhibits the production of human transthyretin (TTR) protein, is being developed by Ionis Pharmaceuticals and AstraZeneca for the treatment of TTR-mediated amyloidosis (ATTR) [1]. TTR protein can misfold and form amyloid in organs such as the nerves, leading to polyneuropathy, and the heart, leading to cardiomyopathy [2]. This misfolding can be due to age-related processes, such as in the case of wild-type ATTR, which typically manifests as a restrictive cardiomyopathy. It can also be due to variations in the TTR gene, leading to hereditary ATTR (ATTRv; v for variant), which can manifest as polyneuropathy, cardiomyopathy or a mixed phenotype of both [2].
Eplontersen is an antisense oligonucleotide that binds to and causes the degradation of both wild-type and variant TTR mRNA, thus inhibiting the production of TTR and subsequent amyloid deposition [3]. It has a similar design and identical nucleobase sequence to inotersen, an antisense oligonucleotide that has been previously approved for polyneuropathy of ATTRv (ATTRv-PN) [4]; however, eplontersen has unique chemistry and is conjugated to a ligand containing three N-acetyl galactosamine (GalNAc) residues to target the drug to hepatocytes, the primary source of TTR in the body [3]. This results in a less frequent and lower dosage of eplontersen needed for efficacy [5] and is expected to lead to an improved safety profile compared with inotersen [3].

Eplontersen is the first approved drug for ATTRv-PN that can be self-administered by patients via an auto-injector [1].
Eplontersen received its first approval on 21 December 2023 in the USA for the treatment of adults with ATTRv-PN [1, 6]. The recommended dosage of eplontersen is 45 mg via subcutaneous (SC) injection once monthly, which may be administered by the patient or a caregiver [6]. As TTR serves as a carrier to transport vitamin A in the body [2], decreased serum TTR levels with eplontersen treatment leads to reduced serum vitamin A levels; patients receiving eplontersen should supplement with the recommended daily allowance of vitamin A [6]. As serum vitamin A concentrations do not indicate the total level of vitamin A in the body, supplementation with a higher dose of vitamin A than the recommended daily allowance should not be used in an attempt to achieve normal serum vitamin A levels. Patients who develop ocular symptoms that suggest vitamin A deficiency, such as night blindness or dry eyes, should be referred to an ophthalmologist [6].
Eplontersen is currently undergoing regulatory review for ATTRv-PN in the EU, the UK, Switzerland and Canada, and is in phase III development for TTR-mediated amyloid cardiomyopathy (ATTR-CM) in multiple countries worldwide.
1.1 Company Agreements
In December 2021, Ionis Pharmaceuticals entered a collaboration agreement with AstraZeneca to develop and commercialise eplontersen globally for the treatment of ATTR [7]. Ionis Pharmaceuticals will continue to lead pivotal phase 3 clinical trials, including manufacturing and supplying eplontersen for ongoing clinical trials, as well as process qualifications. AstraZeneca will have responsibility for commercial supply. Both companies will share responsibility for medical affairs and commercial activities in the USA, while AstraZeneca will have an exclusive licence for the development of eplontersen outside of the USA. The original collaboration agreement excluded certain countries in Latin America [7]; however, in July 2023, it was expanded to include exclusive rights for AstraZeneca to commercialise eplontersen in Latin America [8]. The agreement includes territory-specific development, and commercial and medical affairs cost-sharing provisions [9].
Eplontersen was previously being developed by Akcea Therapeutics, which had acquired the rights from Ionis Pharmaceuticals [10]; Akcea Therapeutics has now been acquired by Ionis Pharmaceuticals [11].
Ionis Pharmaceuticals holds patents covering eplontersen in the USA and EU, which have a 20-year term to 2034 [12].
2 Scientific Summary
2.1 Pharmacodynamics
In human hepatocyte cell culture, eplontersen dose-dependently inhibited the expression of wild-type TTR mRNA, with ≈ 50-fold greater potency than inotersen [3]. In transgenic mice expressing the Ile84Ser variant of the human TTR gene, three once-weekly doses of eplontersen dose-dependently reduced hepatic levels of human TTR mRNA; the maximum reduction of human TTR mRNA was 85% at the highest dose (6 mg/kg/week). Decreases in hepatic expression of human TTR mRNA correlated with reductions in plasma human TTR protein, with eplontersen being 15-fold more potent than inotersen in reducing human TTR protein. After a single dose of eplontersen in transgenic mice, eplontersen preferentially distributed to hepatocytes compared with nonparenchymal cells [3].
In patients with ATTRv-PN who received eplontersen once every 4 weeks, serum TTR levels were decreased from baseline at the first assessment at week 5 [5]. At weeks 35 and 65, the adjusted mean reductions in serum TTR concentrations were 81% and 82% from baseline [5]. Decreases in serum TTR were similar across subgroups including those based on Val30Met variant status, body weight, sex, age and race [6]. At week 37, the mean steady state serum level of vitamin A was also reduced by 71% from baseline [6].
No clinically significant QTc interval prolongation was observed after administration of an eplontersen dose 2.7 times the recommended dose [6].
2.2 Pharmacokinetics
Eplontersen exposure (peak plasma concentration and area under the concentration-time-curve) is slightly greater than dose proportional after a single SC dose ranging 45–120 mg [3, 6]. There is no accumulation of eplontersen after repeated doses once every 4 weeks [3]. Peak plasma concentrations of eplontersen are reached ≈ 2 h after a SC dose [6]. Eplontersen is primarily distributed to the liver and kidney cortex. It is > 98% plasma protein bound in vitro and has an apparent central and peripheral volume of distribution of 12 and 11,100 L, respectively [6].
Eplontersen is metabolised into short oligonucleotide fragments by endo- and exonucleases in the liver [6]. It is not a substrate or inhibitor of transporters, nor an inhibitor or inducer of cytochrome P450 enzymes, and does not interact with highly plasma protein bound drugs. Less than 1% of the administered dose of eplontersen is excreted in the urine as unchanged drug in the first 24 h [6]. The terminal elimination half-life is ≈ 3 weeks [6, 13].
There are no clinically meaningful differences in the pharmacological properties of eplontersen in patients based on age, body weight, sex, race, Val30Met variant status, mild-to-moderately impaired kidney function (estimated glomerular filtration rate ≥ 30 to < 90 mL/min) or mildly impaired liver function [total bilirubin ≤ 1 × upper limit of normal (ULN) and aspartate aminotransferase (AST) > 1 × ULN, or total bilirubin > 1.0–1.5 × ULN and any AST] [6]. Eplontersen has not been studied in patients with severely impaired kidney function, kidney failure, moderate-to-severely impaired liver function or previous liver transplant [6].
Features and properties of eplontersen
Alternative names | AKCEA-TTR-LRx; eplontersen sodium; ION-682884; ION-TTR-LRx; IONIS-TTR-LRx; Wainua™ |
Class | Amides; amino sugars; antisense oligonucleotides; drug conjugates |
Mechanism of action | Gene silencing; prealbumin expression inhibitors |
Route of administration | Subcutaneous injection |
Pharmacodynamics | Degradation of wild-type and variant TTR mRNA leading to reduced TTR levels and amyloid deposition; mean reductions in serum TTR of > 80% from baseline at weeks 35–65 of treatment |
Pharmacokinetics | Exposure is slightly greater than dose proportional; Tmax is ≈ 2 h; > 98% plasma protein bound; Vc is 12 L; Vp is 11,100 L; metabolised into short oligonucleotide fragments; low potential for drug-drug interactions; < 1% excreted as unchanged drug within 24 h; t1/2 is ≈ 3 weeks |
Most frequent adverse events | Vitamin A decreased, vomiting, proteinuria, injection site reactions, blurred vision, cataracts |
ATC codes | |
WHO ATC code | N07X-X21 (eplontersen) |
EphMRA ATC code | N7X (all other CNS drugs) |
2.3 Therapeutic Trials
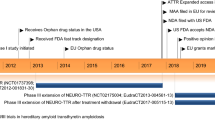
Eplontersen administered subcutaneously every 4 weeks significantly inhibited progression of neuropathy and improved health-related quality of life in patients with ATTRv-PN in the phase III NEURO-TTRansform trial (NCT04136184) [5]. At week 66, the adjusted mean change from baseline (CfB) in modified Neuropathy Impairment Score + 7 (mNIS+7) composite score was 0.3 with eplontersen (n = 144) compared with 25.1 with historical placebo (n = 60) [between-group difference (BGD) − 24.8, 95% CI − 31.0 to − 18.6; p < 0.001; co-primary endpoint]. The adjusted mean CfB in Norfolk Quality of Life Questionnaire–Diabetic Neuropathy (Norfolk QoL-DN) total score was − 5.5 with eplontersen and 14.2 with historical placebo at week 66 (BGD − 19.7, 95% CI − 25.6 to − 13.8; p < 0.001; co-primary endpoint) [5]. In an interim analysis at week 35, on which the US approval for this indication was based [1, 6], the adjusted mean CfB in mNIS+7 composite score was 0.2 with eplontersen and 9.2 with historical placebo (BGD − 9.0, 95% CI − 13.5 to − 4.5; p < 0.001); the adjusted mean CfB in Norfolk QoL-DN total score were − 3.1 and 8.7 in the respective groups (BGD − 11.8, 95% CI − 16.8 to − 6.8; p < 0.001) [5].
NEURO-TTRansform was a multinational, open-label trial that enrolled adult patients with Coutinho stage 1 or 2 (ambulatory without or with assistance, respectively) ATTRv-PN, a Neuropathy Impairment Score of 10–130 (score range 0–244, with higher scores indicating poorer function), and a documented TTR gene variant [5]. Patients were randomized 6:1 to receive eplontersen or inotersen (reference group; n = 24). The trial utilised an historical placebo group from NEURO-TTR [5], the randomized, double-blind, phase III trial in ATTRv-PN on which the approval of inotersen was based [4, 14]. The NEURO-TTR trial had similar eligibility criteria and endpoints to NEURO-TTRansform [5]. Patients in NEURO-TTRansform received SC eplontersen 45 mg every 4 weeks until week 81. Those in the inotersen reference group received SC inotersen 300 mg once weekly up to week 34; these patients then received eplontersen every 4 weeks from weeks 37 to 81 [5].
Key clinical trials of eplontersen
Drug(s) | Sponsor (Collaborator) | Indication | Phase | Status | Location(s) | Identifier |
|---|---|---|---|---|---|---|
Eplontersen, inotersen | Ionis Pharmaceuticals | ATTRv-PN | III | Completed | Multinational | NEURO-TTRansform; NCT04136184; EudraCT2019-001698-10 |
Eplontersen | Ionis Pharmaceuticals | ATTRv-PN | III | Recruiting | Multinational | NCT05071300; EudraCT2021-001427-40 |
Eplontersen | Ionis Pharmaceuticals | ATTR-CM | III | Active, no longer recruiting | Multinational | CARDIO-TTRansform; NCT04136171; EudraCT2019-002835-27 |
Eplontersen | Ionis Pharmaceuticals (AstraZeneca) | ATTR-CM | III | Recruiting | Multinational | NCT05667493; EudraCT2022-000826-74 |
Eplontersen | AstraZeneca | ATTR-CM | III | Recruiting | China | EPIC-ATTR; NCT06194825 |
Eplontersen | Brigham and Women's Hospital | ATTR-CM | II | Not yet recruiting | USA | NCT04843020 |
Eplontersen | Ionis Pharmaceuticals | ATTRv | I/II | Completed | Canada | NCT03728634 |
2.4 Adverse Events
The most common (observed in ≥ 5% of patients) adverse reactions with eplontersen in NEURO-TTRansform were decreased vitamin A levels (including vitamin A deficiency; in 15% of patients), vomiting (9%), proteinuria (8%), injection site reactions (7%), blurred vision (6%) and cataracts (6%) [6]. Three (2%) serious adverse reactions of atrioventricular block, including one case of a complete block, occurred in eplontersen recipients [6]. To week 85, three deaths were reported in the eplontersen group; all deaths were considered to be potentially related to ATTRv and none were considered related to the study drug [5].
Thrombocytopaenia is an adverse event of special interest with eplontersen [5]. In NEURO-TTRansform, three (2%) patients with eplontersen experienced thrombocytopaenia compared with one (2%) patient with historical placebo; all thrombocytopaenia events in eplontersen recipients were mild in severity and did not require dose interruption. There were no incidences of glomerulonephritis in eplontersen recipients. Patients in NEURO-TTRansform were required to supplement with the recommended daily allowance of vitamin A (≈ 3000 IU) [5]. All eplontersen recipients had normal vitamin A levels at baseline and 95% developed low vitamin A levels during treatment [6]. Ocular events potentially related to vitamin A deficiency were reported in 17% of patients with eplontersen and 15% of patients with historical placebo; no patient experienced an ocular event that was assessed to be consistent with vitamin A deficiency by an ophthalmologist [5].
The incidence of anti-drug antibodies (ADAs) in NEURO-TTRansform was 37% among patients receiving eplontersen (mean duration of treatment 63 weeks) [6]. The presence of ADAs did not affect the exposure, pharmacodynamics, safety or efficacy of eplontersen in these patients, although trough drug concentrations were increased [6].
2.5 Ongoing Clinical Trials
The open-label extension study of NEURO-TTRansform (NCT05071300) is currently ongoing. In addition, several studies evaluating eplontersen in ATTR-CM are ongoing. The multinational, randomized, double-blind, placebo-controlled phase III CARDIO-TTRansform trial (NCT04136171) will assess the efficacy of SC eplontersen every 4 weeks compared with placebo in patients receiving background standard of care therapy (which may include tafamidis) [15]. The trial enrolled adults with ATTR-CM (either wild-type or hereditary) and New York Heart Association class I–III symptoms, and has a treatment period of 140 weeks [16]. The longer-term safety and tolerability of eplontersen will be evaluated in the 36-month open-label extension of this trial (NCT05667493). Furthermore, the randomized phase III EPIC-ATTR trial (NCT06194825) is currently enrolling patients in China, while a single-centre, open-label phase II trial (NCT04843020) is planned in patients in the USA who have completed 24 months in an inotersen study.
3 Current Status
Eplontersen received its first approval on 21 December 2023 for ATTRv-PN in the USA [1].
Change history
28 March 2024
A Correction to this paper has been published: https://doi.org/10.1007/s40265-024-02024-5
References
Ionis Pharmaceuticals Inc. WAINUA™ (eplontersen) granted regulatory approval in the U.S. for the treatment of adults with polyneuropathy of hereditary transthyretin-mediated amyloidosis [media release]. 21 Dec 2023. http://www.ionispharma.com/.
Ioannou A, Fontana M, Gillmore JD. RNA targeting and gene editing strategies for transthyretin amyloidosis. BioDrugs. 2023;37(2):127–42.
Viney NJ, Guo S, Tai LJ, et al. Ligand conjugated antisense oligonucleotide for the treatment of transthyretin amyloidosis: preclinical and phase 1 data. ESC Heart Fail. 2021;8(1):652–61.
Keam SJ. Inotersen: first global approval. Drugs. 2018;78(13):1371–6.
Coelho T, Marques W Jr, Dasgupta NR, et al. Eplontersen for hereditary transthyretin amyloidosis with polyneuropathy. JAMA. 2023;330(15):1448–58.
AstraZeneca Pharmaceuticals LP. WAINUA™ (eplontersen) injection, for subcutaneous use. 2023. https://www.accessdata.fda.gov/. Accessed 09 Feb 2024.
Ionis Pharmaceuticals Inc. Ionis and AstraZeneca to develop and commercialize eplontersen [media release]. 06 Dec 2021. http://www.ionispharma.com/.
Ionis Pharmaceuticals Inc. Ionis expands eplontersen agreement with AstraZeneca to include exclusive rights in Latin America [media release]. 28 Jul 2023. http://www.ionispharma.com/.
Ionis Pharmaceuticals Inc. Ionis and AstraZeneca close deal to develop and commercialize eplontersen [media release]. 28 Dec 2021. http://www.ionispharma.com/.
Ionis Pharmaceuticals Inc. Ionis and Akcea partner to commercialize inotersen for hATTR [media release]. 15 Mar 2018. http://www.ionispharma.com/.
Ionis Pharmaceuticals Inc. Ionis Pharmaceuticals completes acquisition of Akcea Therapeutics [media release]. 12 Oct 2020. http://www.ionispharma.com/.
Ionis Pharmaceuticals Inc. Form 10-K to the United States Securities and Exchange Commission. 2021. https://www.sec.gov/. Accessed 09 Feb 2024.
Diep JK, Yu RZ, Viney NJ, et al. Population pharmacokinetic/pharmacodynamic modelling of eplontersen, an antisense oligonucleotide in development for transthyretin amyloidosis. Br J Clin Pharmacol. 2022;88(12):5389–98.
Benson MD, Waddington-Cruz M, Berk JL, et al. Inotersen treatment for patients with hereditary transthyretin amyloidosis. N Engl J Med. 2018;379(1):22–31.
Falk RH, Gertz MA, Benson MD, et al. Rationale and design of a phase 3 study to evaluate the efficacy and safety of ION-682884 in patients with transthyretin-mediated amyloid cardiomyopathy (ATTR-CM) [abstract]. Blood. 2019;134(Suppl 1):5764.
US National Institutes of Health. ClinicalTrials.gov identifier NCT04136171. 2024. https://www.clinicaltrials.gov/. Accessed 09 Feb 2024.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The preparation of this review was not supported by any external funding.
Authorship and Conflict of interest
During the peer review process the manufacturer of the agent under review was offered an opportunity to comment on the article. Changes resulting from any comments received were made by the authors on the basis of scientific completeness and accuracy. Tina Nie is a salaried employee of Adis International Ltd/Springer Nature, and declares no relevant conflicts of interest. All authors contributed to this article and are responsible for its content.
Ethics approval, Consent to participate, Consent to publish, Availability of data and material, Code availability
Not applicable.
Additional information
This profile has been extracted and modified from the AdisInsight database. AdisInsight tracks drug development worldwide through the entire development process, from discovery, through pre-clinical and clinical studies to market launch and beyond.
The original online version of this article was revised due to retrospective open access order.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Nie, T. Eplontersen: First Approval. Drugs 84, 473–478 (2024). https://doi.org/10.1007/s40265-024-02008-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40265-024-02008-5