
Abstract
The Monitoring Medicines project (MM), funded by the FP-7 EU framework, was carried out between 2009 and 2013 by a consortium of 11 partners. The objectives were to support and strengthen consumer reporting of adverse drug reactions (ADRs); expand the role and scope of national pharmacovigilance centres concerning medication errors; promote improved use of pharmacovigilance data; and develop methods to complement spontaneous reporting. The work was organised into four themes: patient reporting; medication errors; drug dependence, counterfeit and substandard medicines and clinical risk estimation; and active and targeted spontaneous pharmacovigilance. MM differed from some other major pharmacovigilance initiatives by having participants from developing countries in Asia and Africa and in leaning towards public health and communicable diseases. MM brought together stakeholders including WHO, drug regulators, pharmacovigilance centres, consumers, public health and disease specialists and patient safety networks. Resources and methodologies developed directly by, or with support from, MM include electronic systems/tools for consumer ADR reporting and cohort event monitoring; publication by WHO of handbooks on consumer reporting, medication errors and pharmacovigilance for TB medicines; methodologies for detecting drug dependence and substandard or counterfeit medicines in ADR databases; and a database on HIV treatment risks with a risk assessment tool. MM enabled stakeholders to achieve more than if they had worked alone in pursuit of patient safety.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Monitoring Medicines brought together diverse parties in order to develop methods, tools and guidelines for pharmacovigilance. |
Outputs included handbooks on consumer reporting, medication errors and pharmacovigilance for TB medicines; systems for consumer reporting, cohort event monitoring and managing antiretroviral risks; and methodologies for detecting medication errors, drug dependence and substandard/counterfeit medicines in safety databases. |
Synergies resulted from collaboration between public health bodies and pharmacovigilance units. |
1 Introduction
Spontaneous reporting of suspected adverse drug reactions (ADRs) has long been the cornerstone of pharmacovigilance worldwide for the identification of early signals of problems of safety related to the use of medicines. Spontaneous reporting systems operate at the level of individual pharmaceutical companies and regional and national pharmacovigilance centres. In addition, there are overarching multinational pharmacovigilance databases: Eudravigilance, operated by the European Medicines Agency (EMA) and EU Member States, and WHO’s global individual case safety report (ICSR) database, VigiBase®, managed by the Uppsala Monitoring Centre (UMC).
The Monitoring Medicines project (MM), with the full title “Optimising drug safety monitoring to enhance patient safety and achieve better health outcomes”, was set up in 2009 with a consortium of 11 partners from Africa, Asia and Europe (Table 1). The project was funded by the FP-7 EU framework and was carried out over the period September 2009 to July 2013. Its stated objectives [1] were:
-
1.
Support and strengthen consumer reporting of suspected ADRs.
-
2.
Expand the role and scope of national pharmacovigilance centres to identify, analyse and prevent medication errors.
-
3.
Promote better and broader use of existing pharmacovigilance data for patient safety.
-
4.
Develop additional pharmacovigilance methods to complement data from spontaneous reporting systems.
The work was organised into four main themes.
-
Increasing patient reporting of problems associated with the use of medicines.
-
Collection by national pharmacovigilance centres of reports of medication errors.
-
Improving the use of available pharmacovigilance data for identifying drug dependence, counterfeit and substandard medicines, and for clinical risk estimation.
-
Development of active and targeted spontaneous pharmacovigilance activities.
An integral part of the project would be the dissemination of resulting knowledge and practical implementation of the outputs from the project.
Work was distributed among 14 work packages (WPs) as follows:
WPs 1–4. Review consumer reporting of ADRs; develop mechanisms for facilitating consumer reporting; improve facilities for storing and managing consumer reports; increase the capability of consumer organisations to undertake reporting of ADRs; and encourage the forwarding of consumer reports to the WHO VigiBase®.
WP 5–6. Develop a guideline that would improve the capability of national pharmacovigilance centres to analyse reports of medication errors; increase their ability to identify preventable medication errors; and help minimise their recurrence by changing the behaviour of healthcare providers.
WP 7–8. Develop a method to improve the detection of medicines causing dependence; develop a method to detect reports within spontaneous safety databases that might indicate substandard or counterfeit medicines.
WP 9–13. Review available pharmacovigilance methods that could complement spontaneous ADR reporting; develop a guidance document on active and targeted spontaneous reporting (TSR) methods; and create tools for collecting, processing and storing active surveillance and spontaneous data in a global database. Additional specific objectives were: increase national capability for pharmacovigilance on specified categories of drugs; create an information resource on ADRs to specified drugs with associated mechanisms for improving awareness of these risks for health professionals.
WP 14. Coordinate all project-related activities and provide overall direction; ensure adequate communication within the project and externally, including to the wider public health community; and manage finances and reporting to the European Commission (EC).
2 Project Activities and Results
2.1 Consumer Reporting
2.1.1 Review of Existing Systems
Current practices in countries with established systems for direct patient reporting of suspected adverse reactions and other safety issues associated with medicines were reviewed [2]. A survey using face-to-face or telephone interviews was carried out from June to August 2010, covering patient reporting systems in 11 countries: Europe (5), Asia (2), America (2) and in Australia and New Zealand. In parallel with the survey, an extensive review of the scientific literature was carried out. A committee including representatives of several patient and consumer organisations reviewed the report and subsequently a handbook on how to establish systems for consumer reporting of ADRs and other problems associated with drug safety was drafted.
2.1.2 Development of an Internet-Based ADR Reporting System
An internet-based system for the management of consumer reports was created, with input into the design by pharmacovigilance experts and consumers [3]. This system facilitates submission of ICSRs from patients or healthcare professionals to national pharmacovigilance centres and subsequently to international databases. The system is compatible with the ICH-E2B standard format for electronic data exchange and with the VigiFlow ICSR management system maintained by the UMC. The web-based reporting tool was subsequently implemented on the websites of the Croatian and Turkish regulatory authorities. After positive feedback from these countries, the facility is being introduced in additional countries (e.g., Moldova, Egypt and Venezuela) and is being offered as a free add-on module for all current users of VigiFlow in more than 60 countries. The tool is easily adapted to the local language using the graphical design of the hosting website.
2.1.3 Reporting System Interface Prototype
A prototype interface was developed to facilitate the use of a standard ADR terminology in patient reporting to pharmacovigilance centres. This involved a re-ordering of WHO-ART terms under existing and new System Organ Classes (SOCs) to allow more intuitive searching for terms according to anatomical site; development of electronic graphical representations of SOCs that provide a simple means of searching for relevant ADR terms; and mapping of terms to Lowest Level Terms in MedDRA® (Medical Dictionary for Regulatory Activities) for use in data input.
2.1.4 Workshop and Seminar on Direct Patient Reporting
The consortium organised a workshop in 2012 to discuss direct patient reporting of ADRs and other safety problems associated with medicines. Thirty participants, representing national regulatory agencies and consumer/patient organisations from 11 countries attended the workshop, which also provided a platform for testing and refinement of the internet-based patient reporting tool.
2.2 Medication Errors
2.2.1 Questionnaire on Medication Error Monitoring
A questionnaire-based analysis was carried out to assess the capability of pharmacovigilance centres to detect, analyse and prevent medication errors. The analysis highlighted the need to develop and strengthen tools for detection, analysis and prevention of medication errors [4].
2.2.2 Workshop on Medication Errors
In 2011, a workshop on medication errors in safety databases was attended by ten national pharmacovigilance centres (Morocco, Kenya, Iran, New Zealand, Thailand, Spain, Switzerland, Nigeria, Brazil and Tunisia) and by patient safety organisations from the UK and Canada. The output from the workshop included an improved ICSR form with the addition of fields to optimise medication error detection, a terminology for the most commonly used terms and definitions used by both pharmacovigilance centres and patient safety organisations, and an assessment tool (P method) for assessing the preventability of medication errors [5]. This latter was tested on ICSRs associated with medication errors submitted by the centres. The methodology was subsequently tested further by the participating national pharmacovigilance centres. A manual on the role of pharmacovigilance centres in detecting and preventing medication errors was published by WHO in 2014 [6].
2.2.3 Follow-Up Questionnaire on Medication Error Monitoring
In response to a follow-up questionnaire distributed in August 2014, some of the pharmacovigilance centres represented at the workshop reported subsequent modifications of their processes to improve monitoring of medication errors as part of their routine pharmacovigilance activities. These included modification of definitions or reporting forms; amendment of ADR terminology; utilisation of a standard method to assess preventability of ADRs; educational activities for potential reporters; and collaboration with other parties involved in medication error prevention. Some pharmacovigilance centres reported having identified new signals of preventable patient harm.
2.3 Detection of Drug Dependence and Counterfeit Medicines
2.3.1 Detecting Drug Dependence in Large Spontaneous Reporting Databases
All ADR terms reported alongside the term ‘drug dependence’ were identified within subsets of VigiBase® corresponding to the pharmacological categories of (a) benzodiazepines, (b) opioids and (c) other medicines reported as causing dependence. The ADR Preferred Terms identified using Standardised MedDRA® Queries (SMQs) for drug abuse and drug withdrawal (version 12.1) were classified into (i) terms directly relating to dependence; (ii) terms describing cognitive and mental effects; and (iii) terms describing relevant physical effects. The primary indicators were then defined as co-reporting of either one term from (i) and one from (ii) in the same report; or one term from (i) and one from (iii) in the same report. The approach was validated by application to the dependence-producing potential of pregabalin [15].
2.3.2 Identifying Substandard or Falsified Medicines [7]
Twenty-four Preferred Terms in the MedDRA® terminology (version 12.1) that may represent the results of using inferior quality products were selected. A data mining approach was then developed to identify medicinal products that (i) were associated with a higher than expected number of ICSRs in VigiBase® compared with other brands in the same country containing the same substance; or (ii) represented an excess of reports with the selected terms during 1 year in a specific country; or (iii) were strongly indicative of falsified medicines based on a set of selected Preferred Terms or additional text in the reports.
The algorithm highlighted several thousand such clusters of medicinal products with excess reporting of potential quality issues. The top 30 medicinal products in respect of disproportionality scores and another random sample among the clusters were further investigated by searching data published on the websites of national regulatory authorities or by contacting the national pharmacovigilance centres. In several instances, the clusters identified in the database indicating effects of substandard or falsified medicines were confirmed by the presence of information on batch withdrawals or regulatory confirmation of product quality problems. A survey was also carried out on the extent to which national pharmacovigilance centres submitted ICSRs relating to quality issues to VigiBase® or withheld these.
2.4 Complementing Spontaneous Reporting and Facilitating Clinical Utilisation of Pharmacovigilance Data
2.4.1 Identification of Methods to Complement Spontaneous Reporting
At a meeting of pharmacovigilance experts and specialists in epidemiology, HIV and TB participants proposed cohort event monitoring (CEM) and targeted spontaneous reporting (TSR) as having good potential for use in monitoring the safety of medicines used long-term in populations with specified diseases. CEM involves reporting of all adverse events occurring in a cohort of patients identified as having received treatment with a specified drug (as occurs, for example, in Prescription Event Monitoring in the UK [8] or the Intensive Medicines Monitoring Programme in New Zealand [9]). TSR focuses on capturing ADRs in a well defined group of patients on treatment, based on the premise that patients, whose condition is repeatedly being followed-up at the same health facility during long-term treatment, should be routinely monitored for suspected ADRs [10].
2.4.2 Training on Cohort Event Monitoring and Targeted Spontaneous Reporting
In 2011, training courses were held in Kenya on CEM for anti-malarial medicines and on TSR for HIV treatment programmes; and a course was held on CEM for anti-retroviral therapy (ART) in the Ukraine. Participants from Botswana, Burkina Faso, Ethiopia, Ghana, Kenya, Nigeria, Tanzania and Zimbabwe attended the workshop in Kenya, including delegates both from the national pharmacovigilance centres and from the national HIV/AIDS or malaria programmes. Participants in the workshop held in Ukraine represented the HIV/AIDS and pharmacovigilance programmes from Belarus, Moldova and Ukraine.
2.4.3 Initiatives in Cohort Event Monitoring and Targeted Spontaneous Reporting
Several of the countries that received training through the MM Project are in the process of implementing projects in CEM or in TSR. CEM is currently being used for antimalarials in Ghana, Kenya, and Zimbabwe and for antiretrovirals in Belarus [11], whilst Nigeria and the United Republic of Tanzania have moved on from pilot to a full scaling up of their CEM studies (on antimalarials in Nigeria and Tanzania and antiretrovirals in Tanzania). Uganda implemented a TSR project on tracking renal toxicity in a cohort of HIV patients receiving tenofovir [12]. At the end of the pilot project, the TSR method was recommended by the authorities in Uganda to be rolled out to other parts of the country. Also, in Zimbabwe, TSR was piloted to monitor the safety of anti-retroviral and anti-tuberculosis medicines. Because of the positive experience, the pilot was scaled up to a main phase programme [13].
In general, the results from these efforts are encouraging and there is general enthusiasm and interest in adopting TSR and CEM elsewhere, especially in those countries that are likely to introduce newer anti-TB medicines such as bedaquiline.
2.4.4 Clinical Utilisation of Pharmacovigilance Data: Initiative on Antiretroviral Therapy
The Copenhagen HIV Programme (CHIP) created a website incorporating a database for storage of information on ADRs to ART based on published literature, together with tools for public (patient and healthcare professional) searching and evaluation of the information and for disseminating and testing knowledge about ADRs. Tools for assessing risk of ADRs related to ART were developed and tested. A patient management module for the website incorporates risk assessment tools: physicians enter anonymised data on their patients, calculate risks and plot these to show change in risk over time.
3 Project Outputs
The Monitoring Medicines project was formally completed in July 2013. However, the intention was that the project would stimulate initiatives on the part of national pharmacovigilance centres and patient/consumer organisations and these, as well as the resources and methods developed in the project, should be considered as part of its results. Table 2 summarises the current status of the resources and methodologies developed in the project.
4 Discussion
The Monitoring Medicines project is one of several major pharmacovigilance initiatives that have been established over the last decade. Prior to, and during, this period there had been increasing public concern about the safety of medicines, the process for evaluating and monitoring adverse effects and the measures available to protect the public health. Steps taken by government bodies, particularly in high-income countries, included extensive revisions to pharmacovigilance legislation and regulations, with a focus on a risk management approach to safety and an emphasis on quality aspects of pharmacovigilance. In addition to these regulatory changes, government agencies have been active in establishing projects—either alone, or in collaboration with pharmaceutical companies and other bodies—with the aim of improving the quality of pharmacovigilance and pharmacoepidemiology and of exploring and developing new methodologies in these fields.
Notable among these initiatives have been the PROTECT (Pharmacoepidemiological Research on Outcomes of Therapeutics by a European Consortium) [17] project, ENCePP (European Network of Centres for Pharmacoepidemiology and Pharmacovigilance [18], EU-ADR [19] and SALUS [20] in Europe; and OMOP (Observational Medical Outcomes Partnership) [21], Sentinel [22] and mini-Sentinel [23] in the US.
The focus of the initiatives has varied from purely national (e.g., Sentinel) to regional (e.g., PROTECT) or multi-regional (e.g., MM). Budgets for these initiatives have varied greatly. The EU Commission grant for MM was €2 million and around €3.3 million for SALUS, with a total budget of ca €5 million; €4.5 million for EU-ADR, total cost €5.88 million; and for PROTECT, €20 million, with half of the funding comprising in-kind contributions from the participating EFPIA pharmaceutical companies. The EU government contributions for these have been under the umbrella of the Innovative Medicines Initiative. At the top of the range, the budget for Sentinel in the US is 135 million US dollars.
Like SALUS, EU-ADR, OMOP and PROTECT, MM has involved a partnership between government and commercial organisations, although in the case of MM this did not include pharmaceutical industry involvement. Objectives of the various initiatives overlap to some extent and include the following:
-
Increasing the range of sources for safety information, e.g.,
-
promoting patient/consumer spontaneous or solicited reporting—MM, PROTECT;
-
utilising safety information from within healthcare database systems—SALUS, Sentinel/Mini-Sentinel, PROTECT, EU-ADR, OMOP.
-
-
Enhancing methodology or identifying new methods within pharmacovigilance and pharmacoepidemiology, e.g.,
-
developing signal detection and validation methods—MM, PROTECT, EU-ADR, OMOP, Mini-Sentinel;
-
developing methods for benefit–risk assessment—PROTECT;
-
implementing new or improved methodologies for pharmacovigilance and pharmacoepidemiology—PROTECT, OMOP, MM;
-
devising tools for risk prediction for individual patients—MM.
-
-
Provision of new resources for data or for studies, e.g.,
-
PROTECT: database of established ADRs; EU drug consumption database;
-
EU-ADR: computerised platform for pharmacovigilance;
-
ENCePP: database of research resources, checklist for study protocols;
-
Mini-Sentinel: electronic health record database.
-
-
Improving quality of work carried out, e.g.,
-
education, communication and training—MM, PROTECT;
-
dissemination of project results—PROTECT, OMOP, MM;
-
provision of guidelines for pharmacovigilance or pharmacoepidemiology—ENCePP Study Seal, ENCePP Code of Conduct, MM.
-
As a function of its multi-regional scope, the MM programme differs somewhat from the other projects by the inclusion of participants from developing countries in Asia and Africa and its leaning towards public health and communicable diseases.
The MM project brought together additional stakeholders (consumers, public health specialists, patient safety networks), promoted the better and broader use of global pharmacovigilance data, and investigated additional methods to complement existing pharmacovigilance methodologies. In short, the MM project achievements are a sound response to some of the concerns expressed by the European Commission [24] in 2007: the need for additional resources and methodologies for pharmacovigilance; greater collaboration with international partners; and the need for introduction of consumer reporting of ADRs.
The project set out to exploit the WHO definition of pharmacovigilance [25]. The focus was on the phrase “… and all other drug-related effects” and the interpretation that pharmacovigilance is not only about detecting adverse reactions to medicines, but also about detecting/addressing all other drug-related safety problems. The project thus successfully proposed the use of pharmacovigilance data to detect product quality problems and to unearth inappropriate use of medicines as part of routine pharmacovigilance activities.
The project also attempted to broaden the resource base on patient harm by developing guidance documents and tools for direct patient reporting. The guidance document on setting up patient reporting systems within pharmacovigilance centres [14] was released just ahead of the new EU pharmacovigilance legislation. The publication was translated into both Russian and Spanish and also presented at a seminar at the World Health Assembly, all of which may have contributed to the current positive attitude towards patient reporting. In a recent survey, 44 countries out of 50 accept ADR reporting from the general public [26]. The debate as to whether patients can contribute to our knowledge of risks has clearly tilted in favour of patient involvement and ADR reporting is no longer the prerogative of health professionals and specialists [27, 28].
The 34th meeting in 2006 of the WHO Expert Committee on Drug Dependence (WHO ECDD) made recommendations [29] for a more scientific basis for using pharmacovigilance data to identify dependence-producing medicines. Through the MM project, novel approaches were developed for analysis of drug dependence liability using information captured in the ICSR databases. Early indications suggest that the method can be usefully employed in informing the work of the WHO ECDD, but additional validation would help determine the potential for routine use of this approach in the WHO Programme for International Drug Monitoring.
Substandard, spurious, falsified, falsely-labelled and counterfeit medicinal products (SSFFCs) are a serious threat to patient safety and health systems globally [30]. The effects of SSFFCs are severe; patients can suffer adverse reactions to additives and substitute products on the one hand, or a total lack of therapeutic effect on the other, leading to worsening of the disease and possibly death.
An effective global response to the threat of SSFFCs requires that we first measure the extent of the problem. The MM project demonstrated how pharmacovigilance databases could be exploited to complement the ongoing efforts to generate data on SSFFCs. The WHO Collaborating Centre, the UMC, has developed an algorithm to detect clusters of reports that are suggestive of SSFFCs within the WHO global ICSR database, VigiBase®. This algorithm was successfully tested in a retrospective setting by WHO and UMC in 2012 on specific known adverse events associated with SSFFC medicinal products. A subsequent project evaluated the algorithm and its use under real-life conditions to detect suspected SSFFC reports within national pharmacovigilance data sets. The results demonstrated that some clusters of suspected substandard products from VigiBase® can be verified by national regulatory authorities but that the processes of ICSR management and submission to the global database need to be faster and supporting information needs to be available at the national level for the method to be an effective tool in the global battle against SSFFCs [7].
The MM project also developed a method by which pharmacovigilance centres could detect preventable ADRs associated with medication errors. A ground-breaking guidance document published by WHO on the topic of medication errors and prevention of associated ADRs [6] recognises differences in use of terminologies and classifications between organisations concerned primarily with pharmacovigilance and those involved directly with clinical safety. It highlights the need to find common ground for future work for the prevention of avoidable medicine-related harm.
Since the WHO guidance document on reporting on and learning from medication errors for pharmacovigilance centres (which contains tools developed for the detection and prevention of medication errors) only became publicly available in 2014, it is too early to evaluate its impact. However, some participants in the MM workshop have reported modifications of their processes and expansion of collaborative networks [31].
An important goal for the MM project was to develop and evaluate monitoring methods and tools that would provide meaningful safety information for medicines being introduced and used in Public Health Programmes (PHPs). PHP managers need safety profiles and quantitative risk estimates which cannot be provided by spontaneous reporting systems that were designed primarily to detect new safety signals of rare, serious adverse reactions. Unique datasets were collected in the MM pilot studies documenting the nature and frequency of patient harm from medicines being used in the PHP setting. Results of these studies are currently being published.
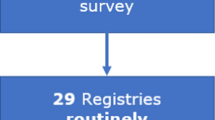
By developing CEM for new medicines through collaboration between pharmacovigilance centres and malaria and HIV/AIDS programmes, there was an enhanced understanding of the advantages of working together for the benefit of patients. Greater awareness of the risks associated with medicines has led to increased spontaneous reporting rates of ICSRs in countries participating in the MM training activities (Fig. 1). Some of the countries have been able to document major contributions from public health programmes in reporting suspected adverse reactions to the national pharmacovigilance programmes [13, 32].

Sum of ICSRs reported to VigiBase® 1 January 2005–30 September 2014 by countries participating in Monitoring Medicines training courses for pharmacovigilance and public health programmes (Belarus, Botswana, Burkina Faso, Ethiopia, Kenya, Moldova, Uganda, Ukraine and Zimbabwe). ICSRs individual case safety reports
Since CEM requires both considerable funding and specialised skills it was important to also propose a method that can be introduced for safety monitoring with only minor modifications to routine management of patients. The TSR pilot project in Uganda was considered to be successful and was later expanded. The WHO programmes for TB and HIV/AIDS, in addition to certain donor organisations, are subsequently promoting the use of this method.
The timing of publication of the TB pharmacovigilance handbook was significant: national TB programmes worldwide were expanding care for multidrug-resistant (MDR-TB) patients; a new drug, bedaquiline, had just received fast-track approval for use in MDR-TB; another new drug, delamanid, was recently authorised for MDR-TB by EMA, and WHO had issued guidance and conditions for the safe introduction of the new drugs and for shorter treatment regimens for MDR-TB patients [33]. The handbook was thus timely in providing practical advice on how pharmacovigilance could be integrated into the TB programmes to monitor risks associated with these relatively unknown and novel treatment approaches.
Pharmacological treatment of patients infected with HIV is complicated, with many alternative treatment regimens and combinations of drugs and the attendant risks of toxicity and development of resistance. A unique support tool intended to be used by clinicians responsible for treatment of HIV/AIDS patients was developed as part of the MM project. In addition to up-to-date information on risks based on the results of randomised clinical trials, a website offers five methods for prediction of the risk of treatment-related toxicity based on individual factors relevant to each patient. At the time of writing, information is not yet available on the uptake and utility of the resource.
In broad terms, by engaging these specialist groups—malaria, TB and HIV/AIDS treatment programmes—the MM project appears to have contributed to a culture of safety within the PHPs, where the previous emphasis has been more on improving access and perhaps less on monitoring the safety and safe use of treatments. Not only do HIV and TB programmes now include pharmacovigilance reporting as a routine, but there is also a clear interest in fostering collaborations with the pharmacovigilance networks and the national pharmacovigilance centres. The project has helped improve communication and collaboration between these systems that have traditionally worked in isolation.
It can be considered that the success of the MM project is related to three aspects: building on ongoing projects and infrastructure (leverage); extending the scope of previous efforts (continuity); and applying the project results to local, every-day use (sustainability). Thus, the project pulled together the partnerships and networks created through other initiatives. Examples include the project on ‘Working with African countries to ensure a pharmaceutical quality response to malaria’ under the EuropeAid framework for poverty-related diseases in developing countries; the WHO EC Partnership project for Strengthening Pharmaceutical Systems and improving access to quality medicines in African, Caribbean and Pacific Islands (ACP) countries; and the WHO project on pharmacovigilance for antiretrovirals supported by the Bill and Melinda Gates Foundation. It developed additional methods for exploring the WHO global ICSR data and it proposed everyday use of these approaches nationally: the SSFFC detection method with uptake by national pharmacovigilance centres and by pharmaceutical procurement agencies to ensure supply chain integrity; a focused pharmacovigilance methodology (TSR) integrated within communicable disease treatment centres; and use of algorithms and decision trees for aiding management of HIV patients, etc.
5 Conclusions
Medicines are critically important health interventions, with 10–60 % of all health expenditure worldwide allocated to pharmaceuticals, and the safe use of those pharmaceuticals is paramount. This project brought together a diverse collection of individuals and organisations in order to develop methods, tools and guidelines that would both generate information on pharmaceuticals and improve the way public health organisations, pharmacovigilance units, healthcare professionals and patients share and respond to that information. The MM Project provided a platform for WHO, disease specialists, regulators, technical organisations and consumers to work together, enabling the stakeholders to achieve much more than if they had worked alone in the pursuit of patient safety: the whole has indeed been greater than the sum of its parts. How the outputs from the MM project will be used and exploited in the coming years remains to be seen but, based on the progress made to date and with support from WHO and other global health initiatives, there are likely to be continuing practical benefits resulting directly or indirectly from the project.
References
Monitoring Medicines: monitoring medicines for the purpose of patient safety [Poster]. World Research and Innovation Congress, Brussels, 5–6 June, 2013.
Van Hunsel F, Härmark L, Pal S, Olsson S, van Groothest K. Experiences with adverse drug reaction reporting from the general public: an 11-country survey. Drug Saf. 2012;35(1):45–60.
Plöen M, Wallberg M, Olsson S. User-driven development of a web-based tool for patient reporting of drug-related harm. Drug Safety. doi:10.1007/s40264-015-0276-x.
Benabdallah G, Benkirane R, Khattabi A, Edwards IR, Bencheikh RS The involvement of pharmacovigilance centres in medication errors detection. A questionnaire-based analysis. Int J Risk Saf Med. 2011;23:17–29.
Benkirane R, Soulaymani-Bencheikh R, Khattabi A et al. Assessment of a new instrument for detecting preventable adverse drug reactions. Drug Safety. doi:10.1007/s40264-014-0257-5.
World Health Organisation. Reporting and learning systems for medication errors: the role of pharmacovigilance centres. Geneva: WHO Press; 2014.
Juhlin K, Karimi G, Andér M, et al. Using VigiBase to identify substandard medicines: detection capacity and key prerequisites. Drug Safety. doi:10.1007/s40264-015-0271-2.
Layton D, Shakir S. Prescription-event monitoring (PEM): the evolution to the new Modified PEM and its support of risk management. In: Andrews EB, Moore N, editors. Mann’s pharmacovigilance. 3rd ed. Chichester: Wiley Blackwell; 2014. p. 359–84.
Harrison-Woolrych M. Prescription-event monitoring in New Zealand. In: Andrews EB, Moore N, editors. Mann’s pharmacovigilance. 3rd ed. Chichester: Wiley Blackwell; 2014. p. 385–402.
Pal SN, Duncombe C, Falzon D, Olsson S. WHO strategy for collecting safety data in public health programmes: complementing spontaneous reporting systems. Drug Saf. 2013;36:75–81.
Setkina S, Dotsenko M, Bondar S et al. Safety and effectiveness of HAART in treatment-naïve HIV patients: preliminary findings of a Cohort Event Monitoring Study in Belarus. Drug Saf. doi:10.1007/s40264-015-0279-7.
Ndagije H, Nambasa V, Namagala E et al. Targeted Spontaneous Reporting of suspected renal toxicity in patients undergoing Highly Active Anti-Retroviral Therapy in two public health facilities in Uganda. Drug Saf. doi:10.1007/s40264-015-0277-9.
Nyambayo P, Gavi S, Mahlangu G et al. Pilot phase of targeted spontaneous reporting of adverse drug reactions due to antiretrovirals and anti-tuberculosis medicines: Zimbabwe experience. Oral communication. First African congress of pharmacovigilance. Actes du Congrès, Rabat; 2013. pp. 42–44. http://www.smpv.ma. Accessed 7 Nov 2014.
World Health Organisation. Safety monitoring of medicinal products: reporting system for the general public. Geneva: WHO Press; 2012.
Caster O, Edwards IR, Norén GN, Lindquist M. Earlier discovery of pregabalin’s dependence potential might have been possible. Eur J Clin Pharmacol. 2011;67(3):319–20.
World Health Organisation. A practical handbook on the pharmacovigilance of medicines used in the treatment of tuberculosis: enhancing the safety of the TB patient. Geneva: WHO Press; 2012.
PROTECT (Pharmacoepidemiological Research on Outcomes of Therapeutics by a European Consortium). http://www.imi-protect.eu. Accessed 12 June 2014.
ENCEPP (European Network of Centres for Pharmacoepidemiology and Pharmacovigilance). http://www.encepp.eu. Accessed 12 June 2014.
EU-ADR. http://euadr-project.org. Accessed 12 June 2014.
SALUS (Scalable, Standard based Interoperability Framework for Sustainable Proactive Post Market Safety Studies). http://www.salusproject.eu. Accessed 17 Aug 2014.
OMOP (Observational Medical Outcomes Partnership). http://omop.org. Accessed 12 June 2014.
FDA Sentinel Initiative. http://www.fda.gov/Safety/FDAsSentinelInitiative/ default.htm. Accessed 12 June 2014.
Mini-Sentinel http://mini-sentinel.org. Accessed 12 June 2014.
European Commission: assessment of the community system of pharmacovigilance—European Commission Public Consultation—presentation of results. European Commission Enterprise and Industry Directorate-General. 2007. http://ec.europa.eu/health/files/pharmacovigilance/docs/2007_02_26/analysis_consultation_responses_en.pdf. Accessed 7 Nov 2014.
World Health Organisation. The importance of pharmacovigilance: safety monitoring of medicinal products, WHO, Geneva. 2002 http://apps.who.int/medicinedocs/en/d/Js4893e/. Accessed 29 Oct 2014.
Margraff F, Bertram D. Adverse drug reaction reporting by patients: an overview of fifty countries. Drug Saf. 2014. doi:10.1007/s40264-014-0162-y.
Härmark L, van Hunsel F, Grundmark B. ADR reporting by general public: lessons learned from the Dutch and Swedish systems. Drug Saf. doi:10.1007/s40264-015-0264-1.
Kenneth Hartigan-Go. Empowering consumers as contributors for health product safety: lessons from the Philippines. Drug Saf. doi:10.1007/s40264-015-0274-z.
WHO Expert Committee on Drug Dependence. World Health Organisation technical report series 942, 34th report. Geneva: WHO Press; 2006.
Institute of Medicine. Countering the problem of falsified and substandard drugs. Washington, DC: The National Academies Press; 2013.
Cousins D, Gerrett D, Richards N, Jadeja MM. Initiatives to identify and mitigate medication errors in England. Drug Saf. doi:10.1007/s40264-015-0270-3.
Abwao E, Sumbi V, Kusu N, Njeri M. Kenya sets record as a leader in ADR reports. Pharmacy and Poisons board newsletter. 2014;2:9–10. http://pharmacyboardkenya.org. Accessed 7 Nov 2014.
World Health Organisation. The use of bedaquiline in the treatment of multidrug-resistant tuberculosis. Interim policy guidance. Geneva: WHO Press. 2013. http://www.who.int/tb/challenges/mdr/bedaquiline/en/. Accessed 30 Oct 2014.
Acknowledgments
The diligent work of Ennita Nilsson and Hanna Lindroos in managing the operations of the Monitoring Medicines project at UMC over different periods is gratefully acknowledged.
Funding and conflict of interest
Shanthi Pal, Sten Olsson and Elliot Brown are employees of organisations that were consortium members in the Monitoring Medicines project that benefited from funding from the European Commission under the FP7 framework.
Theme issue
This article is part of a theme issue co-edited by Shanthi Pal, Sten Olsson and Elliot Brown. No external funding was used to support the publication of this theme issue.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article

Cite this article
Pal, S.N., Olsson, S. & Brown, E.G. The Monitoring Medicines Project: A Multinational Pharmacovigilance and Public Health Project. Drug Saf 38, 319–328 (2015). https://doi.org/10.1007/s40264-015-0283-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-015-0283-y