
Abstract
Background and Objective
Recombinant zoster vaccine (RZV) is approved in adults for the prevention of herpes zoster. The effect of RZV in moderating the severity of breakthrough cases of herpes zoster has been noted but not explicitly quantified before. In this study, a meta-analysis was undertaken to estimate differential utility losses between unvaccinated (Placebo) and vaccinated (RZV) subjects in breakthrough cases of herpes zoster from three RZV clinical trials.
Methods
Differential utility losses between the two groups were estimated in units of quality-adjusted life-years (QALYs), leveraging aggregate patient data from the ZOE-50 (NCT01165177), ZOE-70 (NCT01165229), and ZOE-HSCT (NCT01610414) clinical trials. Differential utility losses and the ratio of mean utility losses were analyzed using random-effects and fixed-effects meta-regression models.
Results
The mean QALY loss differences between the unvaccinated (Placebo) and vaccinated (RZV) groups were 0.008, 0.004, and 0.011 in the ZOE-50, ZOE-70, and ZOE-HSCT studies, respectively, yielding an overall estimated difference of 0.007 (95% confidence interval 0.002–0.012) QALYs. Quality-adjusted life-year loss in the vaccinated group was estimated to be 35.5% of the value in the placebo group. A sensitivity analysis estimated an overall difference of 0.005 (95% confidence interval 0.001–0.009) QALYs, corresponding to 48.6% of the QALY loss value in the placebo group.
Conclusions
Recombinant zoster vaccine is effective in alleviating disease severity in breakthrough cases of herpes zoster. The results may be useful in distinguishing QALY losses between vaccinated and unvaccinated cohorts in health economics studies, particularly cost-effectiveness analyses.
Plain Language Summary
Herpes zoster, also known as shingles, may cause painful rashes and persistent pain for months or even years after the initial episode. Recombinant zoster vaccine is approved for the prevention of shingles. Pivotal recombinant zoster vaccine clinical trials have reported data about the impact of shingles episodes on daily activities and overall health-related quality of life. In this work, we combined data from three recombinant zoster vaccine clinical trials and compared the loss in quality of life—measured in quality-adjusted life-years—incurred by vaccinated and unvaccinated subjects who experienced a shingles episode. We found that vaccinated patients experienced lower quality-adjusted life-year losses when they developed shingles compared with unvaccinated patients. Our results may be useful in assessing quality-adjusted life-year losses between vaccinated and unvaccinated cohorts in future herpes zoster vaccination health economics analyses.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Quality-of-life data from three recombinant zoster vaccine clinical trials were analyzed and the quality-adjusted life-years lost by vaccinated and unvaccinated patients who experienced a shingles episode were compared. |
In addition to preventing herpes zoster, vaccinated patients experienced lower quality-adjusted life-year losses when they developed herpes zoster compared with unvaccinated patients. |
These results may be useful in assessing quality-adjusted life-year losses in vaccinated and unvaccinated patients in future health economics analyses. |
1 Introduction
Herpes zoster, also known as shingles, results from a reactivation of latent varicella-zoster virus (VZV) infection. Herpes zoster often manifests as a painful vesicular rash within a dermatome. Most herpes zoster cases are accompanied by uncomplicated skin lesions and pain, which usually disappear within 2–4 weeks of rash onset. However, up to 30% of patients with herpes zoster develop postherpetic neuralgia, a type of persistent neuropathic pain with a duration of several weeks to months (or even years) after rash onset, which is difficult to treat [1,2,3]. Patients’ quality of life (QoL) during an episode of herpes zoster with or without postherpetic neuralgia may be significantly reduced as a consequence of enduring pain and discomfort affecting their activities of daily living at the physical, emotional, and social levels, in turn undermining their physical and mental health [4,5,6,7].
Approximately one in three people are expected to develop herpes zoster during their lifetime due to VZV reactivation. The risk of herpes zoster increases with advancing age, owing to an age-related decline in cell-mediated immunity against VZV [8]. For individuals living to the age of 85 years, the lifetime risk of shingles increases from one in three to one in two [9, 10].
The main treatment options available for herpes zoster and its complications include analgesics and antiviral agents; despite some efficacy recorded in clinical trials, these treatments have been shown to be suboptimal in clinical practice [10]. Herpes zoster is a vaccine-preventable disease, and the first herpes zoster vaccine, which contained live attenuated VZV (zoster vaccine live, ZVL; Zostavax; Merck Sharp & Dohme Co, Kenilworth, NJ, USA) [11], was licensed in the USA [12] and Europe in 2006 [13].
Adjuvanted recombinant zoster vaccine (RZV; Shingrix; GSK; Rixensart; Belgium) represents a more recent prophylactic vaccination option against herpes zoster. Recombinant zoster vaccine is a two-dose (non-live) recombinant subunit vaccine, combining VZV glycoprotein E with the AS01B adjuvant system. AS01B is an adjuvant system containing 3-O-desacyl-4′-monophosphoryl lipid A, QS-21 (Quillaja saponaria Molina, fraction 21, licensed by GSK from Antigenics LLC, a wholly owned subsidiary of Agenus Inc., a Delaware, USA corporation) and liposome (50 mg of 3-O-desacyl-4′-monophosphoryl lipid A and 50 µg of QS-21).
Clinical trials evaluating the efficacy, safety, immunogenicity, and impact on health-related QoL of RZV were recently reviewed [14]. Efficacy was assessed in two multinational, phase III randomized, observer-blinded, placebo-controlled clinical trials, which were conducted concurrently at the same study sites using the same methods, albeit in two different immunocompetent adult populations: the ZOE-50 study (NCT01165177) recruited 15,411 patients (7698 vaccinated; 7713 placebo) aged 50 years and older [15], whereas the ZOE-70 study (NCT01165229) recruited 13,900 patients (6950 vaccinated; 6950 placebo) aged 70 years and older [16]. A third clinical trial, ZOE-HSCT (NCT01610414), examined the efficacy of RZV in 1846 adults (922 vaccinated; 924 placebo) aged 18 years and older recovering from an autologous hematopoietic stem-cell transplant [17].
The aforementioned trials also collected data on the herpes zoster burden of illness and interference with activities of daily living assessed by the Zoster Brief Pain Inventory instrument [18], as well as the herpes zoster impact on health-related QoL, assessed with the aid of the EuroQol 5-Dimension utility index [19] and the SF-36 health survey [20]. Comparisons between the vaccinated and unvaccinated arms suggested that RZV mitigates the severity of pain in breakthrough cases of herpes zoster, limiting QoL losses [21, 22]. No quantitative outcomes on the exact QoL losses by breakthrough episode of the disease were shown. It is the purpose of this work to estimate differential utility (QoL) losses between unvaccinated (Placebo) and vaccinated subjects in breakthrough cases of herpes zoster from readily available QoL outcomes of RZV clinical trials.
2 Methods
2.1 Study Selection
ZOE-50 (NCT01165177) [15], ZOE-70 (NCT01165229) [16], and ZOE-HSCT (NCT01610414) [17] were included in the present analysis based on herpes zoster case detection defined as the primary endpoint of data collection in the trial (with availability of vaccine efficacy outcomes) and additional availability of health-related QoL results. The selection was validated by recently published medical literature reviews [14, 23], as well as a non-systematic database search for herpes zoster and RZV-related (code GSK1437173A) clinical trials within ClinicalTrials.gov, the results of which are summarized as Electronic Supplementary Material (ESM), including a modified PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [24] flowchart (Fig. S-1 of the ESM) for registry searches further corroborating the selection of NCT01165177, NCT01165229, and NCT01610414 into the present analysis.
2.2 Data Sources
To estimate differential utility losses between unvaccinated and vaccinated subjects per breakthrough episode of herpes zoster, published aggregate patient data (APD) were employed to analyze the ZOE-50 [15], ZOE-70 [16], and ZOE-HSCT [17] clinical trial QoL outcomes. A subset of the relevant datasets has been reported previously [21, 22].
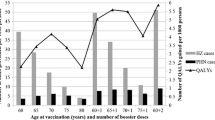
Quality-of-life aggregate patient data retrieved by trial were: (a) annual baseline utility scores from day 0 (vaccination) to 38 (13) months post-vaccination in ZOE-50/70 (ZOE-HSCT) for the vaccinated (RZV) and unvaccinated (Placebo) groups and (b) weekly utility scores for confirmed breakthrough herpes zoster cases from day 0 (herpes zoster case onset) to 4 weeks follow-up for the vaccinated (RZV) and unvaccinated (Placebo) groups. Weekly utility scores were adjusted for response shift bias [25], ensuring that no average weekly utility score exceeded the average baseline utility score for the respective group and study. The complete dataset is provided as Appendix A of the ESM.
2.3 Tools and Implementation
The statistical analysis package metafor [26], written in R [27], was deployed to synthesize individual trial outcomes into an aggregate differential quality-adjusted life-year (QALY)-loss metric. For each study, i, a two-group comparison using continuous (quantitative) data was employed, as outlined in Table 1. Differential utility losses per breakthrough episode of herpes zoster between Group 1 (Placebo) and Group 2 (RZV) were estimated in units of QALYs.
The ratio of means (ROM), mean difference, and standardized mean difference (SMD) were estimated as outcome measures. A SMD with heteroscedastic population variances between the two groups was also calculated as a sensitivity analysis on SMD.
The ratio of means (log-transformed) was defined as:
Mean difference was defined as:
Standardized mean difference was defined as:
with \({\text{SDP}}_{i}\) denoting the pooled standard deviation (SD) between the two groups:
Standardized mean difference with heteroscedastic population variances between the two groups was defined in a similar way to SMD, with \({{\text{SDP}}}_{{\text{i}}}\) denoting the square root of the average variance between the two groups:
Detailed formulas for estimating M and SD for each group are documented in Appendix B of the ESM.
2.4 Meta-analysis
The meta-analysis was performed within a random-effects (RE) model and a fixed-effects (FE) model for comparison [28]. Some methodological differences between the two are noted below, in the context of interpreting results.
In the FE model, the true effect/outcome θ[i] from each study i with sampling variance v[i] is related to the observed effect/outcome y[i] as y[i] = θ[i] + ε[i], where epsilon denotes the sampling error. An average (weighted) effect/outcome for all studies can be estimated from: θw = sum(w[i] × θ[i])/sum(w[i]), where w[i] denotes the weight of each study, estimated as the inverse of the study variance: w[i] = 1/v[i].
In the RE model, the true effect/outcome of study i, θ[i], is assumed to be distributed (usually normally) as θ[i] ~ N(µ, τ2), where μ denotes the true effect/outcome in the population and τ2 the variance of the true/effect outcome in the population, sometimes referred to as the amount of heterogeneity in the true effects/outcomes. The observed effect/outcome y[i] is given by: y[i] = µ + u[i] + ε[i], where u[i] ~ N(0, τ2) and ε[i] ~ N(0, v[i]).
The RE model estimates µ, τ2. The average effect/outcome for all studies is computed as: θw = sum(w[i] × θ[i])/sum(w[i]), with w[i] = 1/(τ2 + v[i]).
The default estimator applied to the RE model was the restricted maximum likelihood (REML) one [29]. Simulation studies have indicated that REML estimation tends to provide approximately unbiased estimates of the degree of heterogeneity [30].
The maximum likelihood and Paule–Mandel estimators [31, 32] were employed for the sensitivity analysis. The Paule–Mandel estimator has been considered optimal in several investigations [33, 34]. Heterogeneity was explored by reporting τ2, I2 (total heterogeneity over total variability), H2 (total variability over sampling variability), and Cochran’s Q statistic [35].
3 Results
Making use of the formulas outlined in Appendix B of the ESM, differential QALY losses between Group 1 (Placebo) and Group 2 (RZV), as well as QALY loss ratios between the two groups, are shown in Table 2. The mean QALY loss differences between the unvaccinated (Placebo) and vaccinated (RZV) groups were 0.008, 0.004, and 0.011 in the ZOE-50, ZOE-70, and ZOE-HSCT studies, respectively.
Aggregate outcome measures taking into account study weights estimated by the RE model (with the REML, ML, and Paule-Mandel estimators) as well as the FE model are summarized in Table 3. The overall estimated difference between the unvaccinated (Placebo) and vaccinated (RZV) groups was 0.007 (95% confidence interval [CI] 0.002–0.012) QALYs. Quality-adjusted life-year loss in the vaccinated group was estimated to be 35.5% of the value in the placebo group. Further details can be found in Appendix C of the ESM.
The forest plot of MD (ROM) corresponding to the RE model with the REML estimator is shown in Figs. 1 and 2. The analysis revealed low (4.88%) to moderate (37.19%) across-study heterogeneity as reflected in the I2 index, depending on model selection (ML vs REML, see Table C-1 of the ESM). Note that the p value (0.24574) in Cochran’s Q test was higher than the value of 0.1 usually employed as the threshold of study homogeneity in meta-analyses, something to be expected given the small number of studies employed [36]. Detailed summary statistics by model type for MD (ROM) are shown in Table C-1 (C-2) of the ESM.

Forest plot of mean differences indicating study weights, mean effects, and mean effect 95% confidence intervals (CIs) with the random-effects (RE) [restricted maximum likelihood estimator] model. QALY quality-adjusted life-year

Forest plot of the log transformed ratio of means indicating study weights, mean effects, and mean effect 95% confidence intervals (CIs) with the random-effects (RE) [restricted maximum likelihood estimator] model. QALY quality-adjusted life-year
3.1 Sensitivity Analysis
A sensitivity analysis was performed using common baseline utility values for the two groups, determined as the simple mean of their pooled average values. Making use of the formulas outlined in Appendix B, differential QALY losses between Group 1 (Placebo) and Group 2 (RZV), as well as QALY-loss ratios between the two groups, are shown in Table 4. The mean QALY loss differences between the unvaccinated (Placebo) and vaccinated (RZV) groups were 0.006, 0.002, and 0.008 in the ZOE-50, ZOE-70, and ZOE-HSCT studies, respectively.
Aggregate outcome measures taking into account study weights estimated by the RE model (with the REML, ML, and Paule-Mandel estimators) as well as the FE model are summarized in Table 5. The overall estimated difference between the unvaccinated (Placebo) and vaccinated (RZV) groups was 0.005 (95% CI 0.001–0.009) QALYs. Quality-adjusted life-year loss in the vaccinated group was estimated to be 48.6% of the value in the placebo group. The forest plot of MD (ROM) corresponding to the RE model with the REML estimator is shown in Figs. 3 and 4. Summary statistics by model type for MD (ROM) are shown in Table C-3 (C-4) in the ESM.

Supplementary analysis using common baseline utility values for the two groups: forest plot of mean differences indicating study weights, mean effects, and mean effect 95% confidence intervals (CIs) with the random-effects (RE) [restricted maximum likelihood estimator] model. QALY quality-adjusted life-year

Supplementary analysis using common baseline utility values for the two groups: forest plot of the log-transformed ratio of means indicating study weights, mean effects, and mean effect 95% confidence intervals (CIs) with the random-effects (RE) [restricted maximum likelihood estimator] model. QALY quality-adjusted life-year
4 Discussion
The present analysis was conducted using aggregate patient QoL data sourced from three pivotal RZV clinical trials. The results indicate a mean difference in QALY losses between unvaccinated (Placebo) and vaccinated (RZV) subjects of 0.007 QALYs for each breakthrough case of herpes zoster, amounting to QALY losses in the vaccinated group equal to 35.5% of those in the placebo. A sensitivity analysis performed with common baseline utility values for the two groups yielded slightly more conservative results: the mean difference in QALY losses for the two groups was estimated to be 0.005 QALYs, and the (logarithmic) ratio of means between the two groups indicated that the QALY losses in the vaccinated group were 48.6% of those in the placebo group.
To place these results into perspective, QALYs can be recast into quality-adjusted life-days, indicating that over 2.5 (1.8 for the sensitivity analysis) quality-adjusted life-days would be gained per vaccinated subject and episode of breakthrough herpes zoster infection. The results indicate that, in addition to preventing herpes zoster, vaccination with RZV reduces the impact of herpes zoster on QALY losses. Because the analysis was limited to the first 4 weeks post breakthrough herpes zoster case detection, the mean QALY loss difference estimated in the present study poses a conservative limit on the differential QALY losses in breakthrough cases of herpes zoster between unvaccinated and vaccinated individuals, i.e., the actual QoL gains for vaccinated subjects, taking into account the sub-acute and chronic pain herpes zoster phases [37], may in fact be higher.
A limitation of the analysis lies in the use of aggregate patient data. Meta-analyses based on individual patient data may offer advantages over meta-analyses conducted using APD. Nevertheless, APD meta-analyses are utilized by the US Preventive Services Task Force, the Cochrane Collaboration, and many professional societies, in support of clinical practice guidelines [38]. The use of APD in meta-analyses frequently produces results equivalent to those of meta-analyses based on individual patient data and should always be explored first [39].
Practical applications of the present work can be foreseen in health economics and outcomes research. The cost benefits of vaccination interventions against herpes zoster have been reviewed extensively [40,41,42,43,44] and QALY losses have been identified as significant sources of outcome variability in cost-effectiveness analyses. While differentiation of QALY losses per episode of herpes zoster between vaccinated and unvaccinated cohorts has been performed for ZVL [45], based on primary pain and QoL outcomes reported elsewhere [1, 11, 46], the equivalent analysis for RZV was until now missing.
5 Conclusions
Recombinant zoster vaccine has been shown to reduce QoL losses in breakthrough cases of herpes zoster. This result should influence the way new cost-effectiveness analyses of herpes zoster vaccination with RZV are designed, by differentiating between QoL losses in vaccinated and unvaccinated cohorts accordingly.
References
Oster G, Harding G, Dukes E, Edelsberg J, Cleary PD. Pain, medication use, and health-related quality of life in older persons with postherpetic neuralgia: results from a population-based survey. J Pain. 2005;6(6):356–63. https://doi.org/10.1016/j.jpain.2005.01.359.
Lukas K, Edte A, Bertrand I. The impact of herpes zoster and post-herpetic neuralgia on quality of life: patient-reported outcomes in six European countries. J Public Health. 2012;20(4):441–51. https://doi.org/10.1007/s10389-011-0481-8.
Pickering G, Marcoux M, Chapiro S, David L, Rat P, Michel M, et al. An algorithm for neuropathic pain management in older people. Drugs Aging. 2016;33(8):575–83. https://doi.org/10.1007/s40266-016-0389-7.
Katz J, Cooper EM, Walther RR, Sweeney EW, Dworkin RH. Acute pain in herpes zoster and its impact on health-related quality of life. Clin Infect Dis. 2004;39(3):342–8. https://doi.org/10.1086/421942.
Drolet M, Brisson M, Schmader KE, Levin MJ, Johnson R, Oxman MN, et al. The impact of herpes zoster and postherpetic neuralgia on health-related quality of life: a prospective study. Can Med Assoc J. 2010;182(16):1731–6. https://doi.org/10.1503/cmaj.091711.
Johnson RW, Bouhassira D, Kassianos G, Leplège A, Schmader KE, Weinke T. The impact of herpes zoster and post-herpetic neuralgia on quality-of-life. BMC Med. 2010;8(1):37. https://doi.org/10.1186/1741-7015-8-37.
Van Oorschot D, McGirr A, Goulet P, Koochaki P, Pratiwadi R, Shah S, et al. A Cross-sectional concept elicitation study to understand the impact of herpes zoster on patients’ health-related quality of life. Infect Dis Ther. 2022;11(1):501–16. https://doi.org/10.1007/s40121-021-00581-w.
Gershon AA, Gershon MD. Pathogenesis and current approaches to control of varicella-zoster virus infections. Clin Microbiol Rev. 2013;26(4):728–43. https://doi.org/10.1128/CMR.00052-13.
Yoshikawa TT, Schmader K. Herpes zoster in older adults. Clin Infect Dis. 2001;32(10):1481–6. https://doi.org/10.1086/320169.
Gater A, Abetz-Webb L, Carroll S, Mannan A, Serpell M, Johnson R. Burden of herpes zoster in the UK: findings from the Zoster Quality Of Life (ZQOL) study. BMC Infect Dis. 2014;14:402. https://doi.org/10.1186/1471-2334-14-402.
Oxman MN, Levin MJ, Johnson GR, Schmader KE, Straus SE, Gelb LD, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005;352(22):2271–84. https://doi.org/10.1056/NEJMoa051016.
Centers for Disease Control and Prevention (CDC). Prevention of herpes zoster. Recommendations of the Advisory Committee on Immunization Practices (ACIP) 2008. https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5705a1.htm. Accessed 1 Aug 2023.
European Medicines Agency (EMA). Zostavax. 2022. https://www.ema.europa.eu/en/medicines/human/EPAR/zostavax#overview-section. Accessed 1 Aug 2023.
Mwakingwe-Omari A, Lecrenier N, Naficy A, Curran D, Posiuniene I. Recombinant zoster vaccine in immunocompetent and immunocompromised adults: a review of clinical studies. Hum Vaccin Immunother. 2023;19(3):2278362. https://doi.org/10.1080/21645515.2023.2278362.
Lal H, Cunningham AL, Godeaux O, Chlibek R, Díez-Domingo J, Hwang S-J, et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med. 2015;372(22):2087–96. https://doi.org/10.1056/NEJMoa1501184.
Cunningham AL, Lal H, Kovac M, Chlibek R, Hwang S-J, Díez-Domingo J, et al. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older. N Engl J Med. 2016;375(11):1019–32. https://doi.org/10.1056/NEJMoa1603800.
Bastidas A, de la Serna J, El Idrissi M, Oostvogels L, Quittet P, López-Jiménez J, et al. Effect of recombinant zoster vaccine on incidence of herpes zoster after autologous stem cell transplantation: a randomized clinical trial. JAMA. 2019;322(2):123–33. https://doi.org/10.1001/jama.2019.9053.
Coplan PM, Schmader K, Nikas A, Chan IS, Choo P, Levin MJ, et al. Development of a measure of the burden of pain due to herpes zoster and postherpetic neuralgia for prevention trials: adaptation of the brief pain inventory. J Pain. 2004;5(6):344–56. https://doi.org/10.1016/j.jpain.2004.06.001.
Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337–43. https://doi.org/10.3109/07853890109002087.
Ware JE Jr. SF-36 health survey update. Spine. 2000;25(24):3130–9. https://doi.org/10.1097/00007632-200012150-00008.
Curran D, Oostvogels L, Heineman T, Matthews S, McElhaney J, McNeil S, et al. Quality of life impact of an adjuvanted recombinant zoster vaccine in adults aged 50 years and older. J Gerontol A. 2019;74(8):1231–8. https://doi.org/10.1093/gerona/gly150.
Curran D, Matthews S, Rowley SD, Young JH, Bastidas A, Anagnostopoulos A, et al. Recombinant zoster vaccine significantly reduces the impact on quality of life caused by herpes zoster in adult autologous hematopoietic stem cell transplant recipients: a randomized placebo-controlled trial (ZOE-HSCT). Biol Blood Marrow Transplant. 2019;25(12):2474–81. https://doi.org/10.1016/j.bbmt.2019.07.036.
de Oliveira GJ, Gagliardi AM, Andriolo BN, Torloni MR, Andriolo RB, Puga M, et al. Vaccines for preventing herpes zoster in older adults. Cochrane Database Syst Rev. 2023;10(10):CD008858. https://doi.org/10.1002/14651858.CD008858.pub5.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372: n160. https://doi.org/10.1136/bmj.n160.
Rapkin BD, Schwartz CE. Advancing quality-of-life research by deepening our understanding of response shift: a unifying theory of appraisal. Qual Life Res. 2019;28(10):2623–30. https://doi.org/10.1007/s11136-019-02248-z.
Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1–48. https://doi.org/10.18637/jss.v036.i03.
R Core Team. The R Project for statistical computing. 2022. https://www.r-project.org/. Accessed 16 Mar 2023.
Cooper H, Hedges LV, Valentine JC, editors. The handbook of research synthesis and meta-analysis. 2nd ed. New York: Russell Sage Foundation; 2009.
Raudenbush SW. Analyzing effect sizes: random-effects models. In: Cooper H, Hedges LV, Valentine JC, editors. The handbook of research synthesis and meta-analysis. 2nd ed. New York: Russell Sage Foundation; 2009. p. 295–315.
Veroniki AA, Jackson D, Viechtbauer W, Bender R, Bowden J, Knapp G, et al. Methods to estimate the between-study variance and its uncertainty in meta-analysis. Res Synth Methods. 2016;7(1):55–79. https://doi.org/10.1002/jrsm.1164.
Harville DA. Maximum likelihood approaches to variance component estimation and to related problems. J Am Stat Assoc. 1977;72(358):320–38. https://doi.org/10.1080/01621459.1977.10480998.
Paule RC, Mandel J. Consensus values and weighting factors. J Res Natl Bur Stand (1977). 1982;87(5):377–85. https://doi.org/10.6028/jres.087.022.
Kacker R. Combining information from interlaboratory evaluations using a random effects model. Metrologia. 2004;41(3):132. https://doi.org/10.1088/0026-1394/41/3/004.
Rukhin AL, Biggerstaff BJ, Vangel MG. Restricted maximum likelihood estimation of a common mean and the Mandel–Paule algorithm. J Stat Plan Inference. 2000;83(2):319–30. https://doi.org/10.1016/S0378-3758(99)00098-1.
Langan D, Higgins JPT, Jackson D, Bowden J, Veroniki AA, Kontopantelis E, et al. A comparison of heterogeneity variance estimators in simulated random-effects meta-analyses. Res Synth Methods. 2019;10(1):83–98. https://doi.org/10.1002/jrsm.1316.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557. https://doi.org/10.1136/bmj.327.7414.557.
Desmond RA, Weiss HL, Arani RB, Soong SJ, Wood MJ, Fiddian PA, et al. Clinical applications for change-point analysis of herpes zoster pain. J Pain Symptom Manag. 2002;23(6):510–6. https://doi.org/10.1016/s0885-3924(02)00393-7.
Lyman GH, Kuderer NM. The strengths and limitations of meta-analyses based on aggregate data. BMC Med Res Methodol. 2005;5(1):14. https://doi.org/10.1186/1471-2288-5-14.
Tudur Smith C, Marcucci M, Nolan SJ, Iorio A, Sudell M, Riley R, et al. Individual participant data meta-analyses compared with meta-analyses based on aggregate data. Cochrane Database Syst Rev. 2016;9(9):MR000007. https://doi.org/10.1002/14651858.MR000007.pub3.
Kawai K, Preaud E, Baron-Papillon F, Largeron N, Acosta CJ. Cost-effectiveness of vaccination against herpes zoster and postherpetic neuralgia: a critical review. Vaccine. 2014;32(15):1645–53. https://doi.org/10.1016/j.vaccine.2014.01.058.
Leidner AJ, Murthy N, Chesson HW, Biggerstaff M, Stoecker C, Harris AM, et al. Cost-effectiveness of adult vaccinations: a systematic review. Vaccine. 2019;37(2):226–34. https://doi.org/10.1016/j.vaccine.2018.11.056.
Chiyaka ET, Nghiem VT, Zhang L, Deshpande A, Mullen PD, Le P. Cost-effectiveness of herpes zoster vaccination: a systematic review. Pharmacoeconomics. 2019;37(2):169–200. https://doi.org/10.1007/s40273-018-0735-1.
Meredith NR, Armstrong EP. Cost-effectiveness of herpes zoster vaccines in the US: a systematic review. Prev Med Rep. 2022;29:101923. https://doi.org/10.1016/j.pmedr.2022.101923.
Giannelos N, Ng C, Curran D. Cost-effectiveness of the recombinant zoster vaccine (RZV) against herpes zoster: an updated critical review. Hum Vaccin Immunother. 2023;19(1):2168952. https://doi.org/10.1080/21645515.2023.2168952.
Pellissier JM, Brisson M, Levin MJ. Evaluation of the cost-effectiveness in the United States of a vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. Vaccine. 2007;25(49):8326–37. https://doi.org/10.1016/j.vaccine.2007.09.066.
Schmader KE, Johnson GR, Saddier P, Ciarleglio M, Wang WW, Zhang JH, et al. Effect of a zoster vaccine on herpes zoster-related interference with functional status and health-related quality-of-life measures in older adults. J Am Geriatr Soc. 2010;58(9):1634–41. https://doi.org/10.1111/j.1532-5415.2010.03021.x.
Acknowledgments
The authors thank Business & Decision Life Sciences Medical Communication Service Center for editorial assistance and manuscript coordination, on behalf of GSK.
Author information
Authors and Affiliations
Contributions
All authors were involved in the design of the study, collected or generated the data, analyzed and/or interpreted the data, and participated in the development of this manuscript and in its critical review, providing substantial intellectual contributions. All authors had full access to the data and gave approval of the final manuscript before submission. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The work described was carried out in accordance with ICMJE recommendations for the conduct, reporting, editing, and publishing of scholarly work in medical journals. The corresponding author had the final responsibility to submit the manuscript for publication.
Corresponding author
Ethics declarations
Funding
GlaxoSmithKline Biologicals SA funded this study (GSK study identifier: VEO-000509) and was involved in all stages of the study conduct, including analysis of the data. GlaxoSmithKline Biologicals SA also took charge of all costs associated with the development and publication of this manuscript.
Conflict of interest
Nikolaos Giannelos, Bernard Francq, and Desmond Curran are employed by and hold shares in GSK. The authors declare no other financial and non-financial relationships and activities.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary information.
Code availability
Not applicable.
Trademarks
Shingrix is a trademark owned by or licensed to GSK. Zostavax is a trademark of Merck Sharp & Dohme Corp. AS01 is a trademark owned by or licensed to GSK.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Giannelos, N., Francq, B. & Curran, D. Differential Utility Losses in Herpes Zoster Cases Between Vaccinated and Unvaccinated Subjects: A Meta-analysis of Three Clinical Trials. Clin Drug Investig 44, 293–301 (2024). https://doi.org/10.1007/s40261-024-01355-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-024-01355-1