
Abstract
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are well established as effective adjuncts to lifestyle modification in the treatment of type 2 diabetes (T2D) as monotherapy or in combination with oral glucose-lowering drugs ± insulin. The six subcutaneous GLP-1RA formulations (i.e. twice-daily exenatide, once-daily liraglutide and lixisenatide, and once-weekly dulaglutide, exenatide and semaglutide) currently available in the EU and USA have many similarities, but also some unique features and properties. By stimulating GLP-1 receptors, GLP-1RAs increase insulin secretion and suppress glucagon release in a glucose-dependent manner, thereby improving clinical and patient-reported outcomes related to glycaemic control and weight. They also have been shown to reduce, or at least not increase, the risk of major cardiovascular outcomes. GLP-1RAs are generally well tolerated, with gastrointestinal and injection-site reactions being the most troublesome drug-related adverse events, and are associated with a very low intrinsic risk of hypoglycaemia. Treatment with GLP-1RAs should be customized to meet the clinical needs and personal preferences of the individual.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
GLP-1RAs improve glycaemic control, reduce patient weight and improve patient-reported outcomes when administered as monotherapy or add-on therapy to other glucose-lowering drugs |
GLP-1RAs reduce, or at least not increase, the risk of major cardiovascular events |
GLP-1RAs are generally well tolerated with a very low intrinsic risk of hypoglycaemia |
Once-weekly administration of GLP-1RAs may improve treatment adherence and satisfaction relative to more frequent treatment |
Consider clinical and administration differences between-GLP-1RAs and patient preferences when individualizing treatment |
1 Rationale for Using GLP-1RAs in Type 2 Diabetes
In many patients, the treatment of type 2 diabetes (T2D) requires the use of two or more glucose-lowering drugs [1, 2]. Unless contraindicated or poorly tolerated, metformin is commonly used as first-line therapy, but the addition of glucose-lowering drugs with different mechanisms of action is usually required to provide adequate glycaemic control.
Glucagon-like peptide-1 (GLP-1), an intestinal hormone with properties that include increasing insulin secretion after eating, plays has an important role in glucose homeostasis [3]. The effects of GLP-1 are impaired in patients with T2D, thereby providing the rationale for developing GLP-1 receptor agonists (GLP-1RAs) to treat T2D [3]. These agents have established efficacy in improving glycaemic control in patients with T2D and, unlike insulin and insulin secretagogues (e.g. sulfonylureas and meglitinides), induce weight loss and have a low intrinsic risk of hypoglycaemia [3].
This article reviews the features and properties of the six GLP-1RA formulations, which are administered subcutaneously twice daily [exenatide immediate release (IR)] [4, 5]; once daily (liraglutide [6, 7] and lixisenatide [8, 9]); or once weekly [dulaglutide [10, 11], exenatide extended release (ER) [12,13,14], and semaglutide [15, 16]] that are currently marketed in the EU and the USA. GLP-1RAs that have been voluntarily withdrawn for commercial reasons (e.g. albiglutide), are currently available only in countries outside the EU/USA (e.g. taspoglutide) or are available as and fixed-dose combinations (e.g. insulin degludec/liraglutide and insulin glargine/lixisenatide) are not discussed in this review.
2 Pharmacological Properties of GLP-1RAs
Native GLP-1 has a very short half-life, as it is rapidly degraded by proteases, namely the dipeptidyl peptidase (DPP)-4 enzyme [17,18,19]. To overcome this, GLP-1RAs have been developed that are structurally similar to GLP-1 with regard to their amino-acid sequences, but with modifications that provide stabilization against DPP-4 degradation and/or minimise their renal clearance, thereby increasing their duration of activity (Table 1). Differences in the structure of GLP-1RAs may also determine accessibility to the CNS, which may partly explain differences between GLP-1RAs in weight loss (Table 2). The homology of the GLP-RAs to the structure of human GLP-1 (i.e. the proportion of amino acid sequence similar to native GLP) ranges from ≈ 50% with exenatide and lixisenatide (which are based on the exendin-4 molecule present in Gila monster venom) to 90–97% with lixisenatide, dulaglutide and semaglutide (which are modified from the human GLP-1 active fragment) [Table 1] [4,5,6,7,8,9,10,11,12,13,14,15,16].
GLP-1RAs selectively bind to and activate GLP-1 receptors in the same manner as native GLP-1 [4,5,6,7,8,9,10,11,12,13,14,15,16]. When blood glucose levels are high, activation of the GLP-1 receptors by GLP-1RAs stimulates insulin secretion and lowers inappropriately high glucagon secretion in a glucose-dependent manner, thereby improving glycaemic control. When blood glucose levels are low, GLP-1RAs do not stimulate insulin secretion and do not impair glucagon secretion, which also helps maintain glycaemic control by reducing the risk of hypoglycaemia [17,18,19,20]. Reduced feelings of hunger and lowered energy intake also help patients lose weight.
Individual GLP-1RAs differ with regard to their pharmacological profiles and duration of activity due to several factors, including the rate of absorption, degree of binding to albumin/plasma proteins, degree of protection against metabolic degradation and rate of renal clearance (Table 1) [17,18,19,20]. Based on their duration of activation of the GLP-1 receptor, exenatide IR and lixisenatide are classified as short-acting GLP-1RAs, whereas liraglutide, dulaglutide, exenatide ER and semaglutide are classified as long-acting GLP-1RAs (Table 1). [17,18,19,20]. Unlike long-acting GLP-1RAs, short-acting GLP-1RAs are associated with substantial delays in gastric emptying [19].
The half-life of the GLP-1RAs varies from a few hours to several days, with the long half-lives of dulaglutide and semaglutide allowing administration once weekly (Table 1) [4,5,6,7,8,9,10,11,12,13,14,15,16]. The ER formulation of exenatide also allows once-weekly administration, as the microspheres in the formulation release surface-bound exenatide initially, then gradually release exenatide from the microspheres (Table 1) [12,13,14].
3 Effects of GLP-1RAs on Glycaemic Control and Weight Loss
The efficacy of GLP-1RAs in controlling glycaemia in patients with T2D is well established. This section provides an overview of the results of randomized clinical trials (RCTs) that were pivotal in the approval of exenatide IR] [4, 5], liraglutide [6, 7], lixisenatide [8, 9], [dulaglutide [10, 11], exenatide ER [12,13,14], and semaglutide [15, 16] in the EU and the USA, as well as other relevant data.
3.1 Compared with Placebo, Oral Glucose-Lowering Drugs and Insulin
With regard to reducing glycosylated haemoglobin (HbA1c) from baseline in RCTs in patients with T2D, monotherapy or add-on treatment with GLP-1RAs was significantly more effective than placebo [4,5,6,7,8,9,10,11,12,13,14,15,16]. GLP-1RA monotherapy or add-on treatment was also generally noninferior or more effective in reducing HbA1c than several oral glucose-lowering drugs, including metformin, glimepiride (a sulfonylurea), sitagliptin (a DPP-4 inhibitor), pioglitazone (a thiazolidinedione) and dapagliflozin [a sodium-glucose cotransporter 2 (SGLT2) inhibitor], as well as insulin glargine (long acting) and insulins glulisine and lispro (rapid acting) [4,5,6,7,8,9,10,11,12,13,14,15,16]. The GLP-1RAs were also associated with significant or numerical improvements in other measures of glycaemic control, such as changes from baseline in mean fasting serum/plasma and 2-h post-prandial glucose levels [4,5,6,7,8,9,10,11,12,13,14,15,16].
In keeping with their efficacy in reducing HbA1c levels, GLP-1RAs were also associated with patients achieving their HbA1c targets (i.e. HbA1c ≤ 6.5 or < 7%) [4,5,6,7,8,9,10,11,12,13,14,15,16]. The proportion of patients who achieved their HbA1c target varied depending on the design of the RCT (e.g. trial duration, background and comparator treatment, inclusion/exclusion criteria, GLP-1RA dosage, etc.). For example, where reported in the RCTs in Table 2, the proportions of patients who achieved the HbA1c < 7% target at trial end were: 25–57% with exenatide IR, 35–58% with liraglutide, 25–50% with lixisenatide, 34–71% with dulaglutide, 27–73% with exenatide ER and 55–79% with semaglutide [4,5,6,7,8,9,10,11,12,13,14,15,16]. Overall, in individual RCTs, the proportion of patients achieving this target were generally significantly or numerically higher with GLP-1RA than with placebo (5–39%), and similar or somewhat higher with GLP-1RA than with oral glucose-lowering drugs (e.g. 48–52% with metformin, 30–40% with sitagliptin, 28–36% with glimepiride and 22–55% with thiazolidinediones) and insulin (30–54% with insulins glargine, glulisine or lispro) [4,5,6,7,8,9,10,11,12,13,14,15,16].
Treatment with the GLP-1RAs was associated with weight loss in many RCTs (Table 2), which is an important consideration in the treatment of T2D. In most RCTs, weight decreased from baseline to a greater extent with GLP-1RAs than with placebo when taken as monotherapy or as an add-on to treatment with one or more glucose-lowering drugs [4,5,6,7,8,9,10,11,12,13,14,15,16]. Relative to add-on treatment with other oral glucose-lowering drugs and insulin, decreases from baseline in weight were significantly better with a GLP-1RAs in the following comparisons: liraglutide versus glimepiride, rosiglitazone and insulin glargine; lixisenatide versus insulin glulisine three times daily; dulaglutide versus sitagliptin and insulin glargine; exenatide ER versus sitagliptin, pioglitazone and insulin glargine; and semaglutide versus sitagliptin and insulin glargine (Table 2).
GLP-1RAs were also associated with decreases from baseline in waist circumference [21], according to network meta-analyses of 17 RCTs [21]. Waist circumference decreased to a greater extent with GLP-RAs than with placebo, thiazolidinediones and insulin, and somewhat greater than those with sitagliptin [21].
3.2 Comparisons Between GLP-1RAs
Given the pharmacological differences between individual GLP-1RAs (Table 1), the drugs in this class may have differences in their effectiveness [18,19,20, 22]. However, there are few RCTs that directly compare the relative efficacy of drugs in this class (Table 2). In the available head-to-head comparisons, reductions from baseline in HbA1c were significantly greater: with exenatide IR 10 μg twice daily than with lixisenatide 20 μg/day; with liraglutide 1.8 mg/day than with exenatide IR 10 μg twice daily; with dulaglutide 0.75 or 1.5 mg/week than with exenatide IR 10 μg twice daily; withsemaglutide 0.5 mg/week than with dulaglutide 0.75 mg/week; with semaglutide 1.0 mg/week than with dulaglutide 1.5 mg/week; and with semaglutide 1.0 mg/week than with exenatide ER; there were no significant differences between exenatide ER and liraglutide (Table 2).
Due to their effects in delaying gastric emptying, short-acting GLP-1RAs had greater effects on post-prandial glucose levels than long-acting ones. However, the long-acting GLP-1RAs offer the pharmacological advantage of reducing plasma glucose levels across the 1-day or 1-week administration intervals [18, 20, 22]. In a meta-analysis of RCTs comparing a GLP-1RA with placebo or another GLP-1RA [23], dulaglutide, exenatide, liraglutide and lixisenatide improved HbA1c and fasting plasma glucose levels relative to placebo (semaglutide data were not available at the time of the meta-analysis). Overall, the long-acting GLP-1RAs (once-weekly dulaglutide, liraglutide and exenatide ER) were superior to the short-acting agents (twice-daily exenatide and lixisenatide) with regard to improvements in glycaemic control, whereas no differences were shown in comparisons between either the various short-acting drugs or long-acting drugs [23]. Updated meta-analyses that include data for semaglutide would be of interest given the significantly better efficacy with semaglutide shown in head-to-head RCTs with the two other currently available weekly GLP-1RAs.
When added to oral glucose-lowering treatment, reductions in weight were more than twofold greater (p < 0.0001) with once-weekly semaglutide than with either once-weekly exenatide ER or once-weekly dulaglutide (Table 2). Weight reductions with once-daily liraglutide 1.8 mg were comparable to those with exenatide IR 10 μg twice daily, and significantly greater than those with dulaglutide 1.5 mg/week (Table 2). The clinical data are supported by results in the real-world setting [24]. In a retrospective cohort study in 2465 patients receiving once-weekly exenatide, dulaglutide or albiglutide, the overall mean decrease from baseline in HbA1c at 6 months was 0.5%, with no significant differences between treatment groups [24]. However, weight loss with dulaglutide was significantly better with than with exenatide and albiglutide (2.7 vs 1.4 and 1.6 kg; p = 0.001) [24].
4 Effects of Once-Weekly GLP-1RAs on Patient-Reported Outcomes
Once-weekly GLP-1RAs improved most patient-reported outcomes (PROs) related to T2D treatment relative to baseline, with significant improvements relative to placebo or active comparators also being shown in some RCTs (Table 3) [25,26,27,28,29,30,31,32]. As these RCTs had differences in trial design (e.g. comparators, PRO measures, inclusion criteria and trial duration), results tend to vary between RCTs.
Overall, the currently available data suggest that treatment with a once-weekly GLP-1RA may improve Diabetes Treatment Satisfaction Questionnaire (DTSQ) total, treatment satisfaction and patient perception of the frequency of hyperglycaemia scores to a significantly greater extent than treatment with placebo (Table 3) [25,26,27,28,29,30,31,32], as well, in a few RCTs, some other glucose-lowering drugs (most frequently semaglutide vs sitagliptin or insulin glargine [28,29,30,31,32]) [Table 3]. With a few exceptions, DTSQ patient perception of the frequency of hypoglycaemia and weight-related PRO scores generally did not improve to a significantly greater extent with once-weekly GLP-1RAs than with placebo or glucose-lowering drugs (Table 3). In head-to-head comparisons of GLP-1RAs, improvements in some DTSQ scores were greater with once-weekly dulaglutide or exenatide ER than with exenatide IR [25, 26], and greater with semaglutide than with exenatide ER [31] (Table 3).
General health-related quality-of-life (HR-QoL) was evaluated in several RCTs, with once-weekly GLP-1RAs showing consistent and significant improvements from baseline for most HR-QoL-related PROs, such as EuroQol 5 Dimension, Psychological General Well-Being Index and Short-Form-36 (SF-36) total and/or domain scores [25, 27, 29, 30, 32]. However, with a few exceptions, once-weekly GLP-1RAs did not consistently improve such outcomes to a significantly greater extent than placebo or active comparators [25, 27, 29, 30, 32].
Nevertheless, general HR-QoL-related PROs, as well as T2D-related PROs, may improve in conjunction with significant weight loss, such as that seen with semaglutide [33]. In pooled analyses of PROs in 2808 recipients of semaglutide 0.5 or 1.0 mg/week, patients with a weight loss of ≥ 5 or ≥ 10% had significantly (p < 0.01) greater improvements in SF-36 version 2 physical component summary, general health and physical function scores than those without the corresponding weight-loss response [33]. DTSQ overall treatment satisfaction and perception of hyperglycaemia frequency scores were also significantly (p < 0.01) greater in patients who lost ≥ 5 or ≥ 10% of their weight than those in patients who did not [33].
Adherence to treatment may be better with the once-weekly GLP-1RAs than with the once- or twice-daily options, leading to improvements in clinical outcomes [34]. Over a 6-month period in retrospective studies in the real-world setting, treatment adherence was significantly better with once-weekly exenatide ER than with twice-daily exenatide IR [35, 36] and/or once-daily liraglutide [35,36,37], and treatment adherence and persistence rates were significantly higher, and discontinuation rates were significantly lower, with once-weekly dulaglutide than with once-daily liraglutide and once-weekly exenatide [38].
5 Effects of GLP-1RAs on Major Cardiovascular Outcomes
As patients with T2D have an increased risk of adverse cardiovascular (CV) outcomes, current management of T2D includes the reduction of CV risk factors including, but not limited to, hyperglycaemia [39, 40]. GLP-1RAs, as a class, provide beneficial effects with regards to several CV risk factors by improving glycaemic control and promoting weight loss (Sect. 3), as well as improving factors that are independent of changes in blood glucose [39,40,41,42].
RCTs evaluating major adverse CV events (MACE) with once-daily or -weekly GLP-1RAs in patients with T2D have found the incidence of MACE to be significantly reduced (liraglutide [43], dulaglutide [44] and semaglutide [45]), or at least not increased (lixisenatide [46] and exenatide ER [47]) relative to placebo, with hazard ratios ranging to 0.74–1.02 (Table 4). The primary MACE component appearing to be driving the reduction in MACE was CV death with liraglutide [43], and non-fatal stroke with dulaglutide [44] and semaglutide [45], with no other significant differences in the risk of individual MACE components shown between individual GLP-1RAs and placebo (Table 4). The risk of all-cause death was significantly lower with liraglutide and exenatide ER than with placebo (Table 4).
Between-trial discrepancies may be explained by factors such the heterogeneity across the RCTs, the definitions of composite and individual outcomes, GLP-1RA pharmacokinetics and the degree to which each GLP-1RA may impact modifiable CV risk factors [39,40,41,42, 44]. According to a meta-analysis of RCTs of lixisenatide, liraglutide, exenatide ER and semaglutide investigating CV outcomes, overall these GLP-1RAs significantly reduced the risk of MACE by 10%, CV mortality by 13% and all-cause mortality by 12% relative to placebo [48].
6 Tolerability Profiles of GLP-1RAs
Overall, GLP-1RAs are well tolerated, with gastrointestinal effects being the most common adverse drug reactions (ADRs; Table 5) [19, 49,50,51]. Of note, as the effects of GLP-1RAs are glucose-dependent, they do not have an intrinsic risk of hypoglycaemia. In RCTs, GLP-1RAS were associated with very low rates of major/severe hypoglycaemia when used as monotherapy or in combination with other glucose-lowering drugs [4,5,6,7,8,9,10,11,12,13,14,15,16]. However, when a GLP-1RA is added to an existing regimen, the dosage of insulin or an insulin secretagogue may need to be reduced, in order to decrease the potential for hypoglycaemic episodes [4,5,6,7,8,9,10,11,12,13,14,15,16].
Although many ADRs appear to be class effects, the tolerability profiles of individual GLP-1RAs are affected by differences in their structure and duration of effect with regard to some ADRs, especially with regard to gastrointestinal ADRs and injection-site reactions (Table 5) [19, 49, 50].
In head-to-head RCTs, significant differences in the rates of gastrointestinal ADRs were found only with liraglutide versus exenatide ER [65], and exenatide IR versus dulaglutide 0.75 (but not 1.5) mg/week [53]. A meta-analysis found no significant differences in the rates of nausea and discontinuation for ADRs between exenatide ER and dulaglutide, exenatide IR, liraglutide and lixisenatide as add-ons to metformin [66]. Another meta-analysis found that the once-weekly GLP-1RAs (semaglutide data were not included) had similar risks of diarrhoea, but the risk of nausea was greater with dulaglutide than with exenatide ER [23]. In a head-to-head RCT, the rate of nausea was higher with semaglutide 1.0 mg/week than with dulaglutide 1.5 mg/week (83.2 vs 45.4/100 patient-years), but the rate of all gastrointestinal ADRs was similar (43 vs 44% of patients) [32].
The relative incidences of injection-site reactions with GLP-1RAs are difficult to determine as their frequency and characteristics in RCTs are inconsistently reported and lack statistical analysis [19, 51]. In head-to-head RCTs, exenatide ER recipients had a higher rate of injection-site reactions than exenatide IR recipients [12,13,14] and semaglutide recipients had a lower rate of injection-site reactions than exenatide ER recipients [31]. Rates of injection-site reactions were similar between dulaglutide and liraglutide [67], as well as between dulaglutide and semaglutide [32].
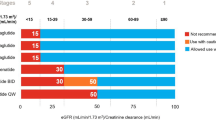
With some exceptions, dosage changes are generally not required in patients with hepatic impairment or mild renal impairment (Table 6). However, due to limited data, the use of GLP-1RAs in patients with more severe renal impairment usually requires caution or is not recommended (Table 6). Dosage changes are not required on the basis of age (limited data in patients aged ≥ 70 or 75 years), but treatment in elderly patients should take into account any age-related renal impairment. The use of GLP-1RAs is not recommended in women who are pregnant or breastfeeding. Precautions should also be taken in patients at risk of acute kidney disease, pancreatitis or thyroid disease (Table 5).
7 Approved Indications of GLP-1RAs
Six GLP-1RA formulations (i.e. twice-daily exenatide IR, once-daily liraglutide and lixisenatide, and once-weekly dulaglutide, exenatide ER and semaglutide) are approved for the treatment of T2D in the EU and/or USA (Table 6) [4,5,6,7,8,9,10,11,12,13,14,15,16]. They are all indicated as an adjunct to diet and exercise to improve glycaemic control in adults with T2D in combination with other glucose-lowering drugs (including insulin) when current treatment + diet/exercise do not provide adequate glycaemic control. Some GLP-1RAs are also indicated as an adjunct to diet and exercise as monotherapy, or as monotherapy when the use of metformin is considered inappropriate due to intolerance or contraindications (Table 6) [4,5,6,7,8,9,10,11,12,13,14,15,16].
All of the GLP-1RAs are injected subcutaneously to the abdomen, thigh or upper arm, with a different injection site being used each time when injecting in the same region [4,5,6,7,8,9,10,11,12,13,14,15,16]. Their use differs with regard to some parameters, such as dosage, administration and dose preparation (Table 6) [4,5,6,7,8,9,10,11,12,13,14,15,16].
8 Current Clinical Position of GLP-1RAs
Current treatment guidelines recommend GLP-1RAs as an option for T2D management, most commonly as add-on therapy in patients not achieving glycaemic targets with lifestyle interventions plus metformin and/or other glucose-lowering drugs [1, 2]. As a class, GLP-1RAs offer some potential advantages over other classes of glucose-lowering drugs. Outcomes related to glycaemic control and weight loss improved to at least, or better, extent with a GLP-1RA than metformin, sulfonylureas, DPP-4 inhibitors, thiazolidinediones, SGLT2 inhibitors and long-and rapid-acting insulins (Sect. 3). The beneficial effects of the GLP-1RAs on glycaemic control, including the low intrinsic risk of hypoglycaemia, and loss of weight are associated with improvements in PROs pertaining to diabetes treatment satisfaction, perception of weight and perceived frequency of hyper- and hypoglycaemia (Sect. 4).
GLP-1RAs, SGLT2 inhibitors, DPP-4 inhibitors and thiazolidinediones are often indicated as add-on options to current therapies at the same step of treatment guidelines [1, 2]. Although both GLP-1RAs and DPP-4 inhibitors are incretin-based therapies, GLP-1RAs have direct intrinsic effects on the incretin system, whereas DPP-4 inhibitors work indirectly to prevent the inactivation of endogenous GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) through competitive inhibitor of the DPP-4 enzyme [72,73,74]. Both drug classes have a low risk of hypoglycaemia and weight gain; however, GLP-1RAs provide better glycaemic control than DPP-4 inhibitors, and promote weight loss instead of being weight neutral. In patients who have a compelling need to lose weight, treatment with a GLP-1RA or an SGLT2 inhibitor (which also promote weight loss), therefore, could be preferred over a DPP-4 inhibitor; if weight is not a concern, oral administration is desired or GLP-1RA treatment is not tolerated, treatment with a DPP-4 inhibitor may sometimes be preferred.
Treatment with a GLP-1RA or an SGLT2 inhibitor with proven CV benefits may also be preferred over other options in patients at risk of atherosclerotic CV events [2]. In RCTs of GLP-1RAs assessing CV outcomes, semaglutide, dulaglutide and liraglutide significantly reduced the risk of MACE by 26%, 13% and 12%, respectively, and exenatide ER and lixisenatide at least did not increase the risk of MACE (Table 4). These are important findings as the treatment of T2D should manage aspects of T2D beyond achieving glycaemic control. Overall, current evidence regarding efficacy in reducing CV events is greatest with liraglutide, followed by semaglutide and then by exenatide ER [2]. Of note, SGLT2 inhibitors have also shown CV benefits relative to placebo and other oral glucose-lowering drugs (i.e. metformin, sulfonylureas, thiazolidinediones and DPP-4 inhibitor) [75], with evidence being moderately stronger for empagliflozin than for canagliflozin [2]. In patients in whom heart failure or chronic kidney disease (CKD) predominates, treatment with an SGLT2 inhibitor with evidence of reducing heart failure and/or CKD is preferable in patients with adequate renal function; a GLP-1RA with proven CV benefits can be added if an SGLT2 inhibitor is not tolerated/contraindicated or if renal function is less than adequate [2].
In patients without established atherosclerotic CV disease or CKD and in whom the cost of glucose-lowering drug treatment is a major issue, the addition of a sulfonylurea or thiazolidinedione to metformin may generally be preferred over the addition of a GLP-1RA, SGLT2 inhibitor or DPP-4 inhibitor, with the addition of a glucose-lowering drug in the newer, and more costly, drug classes being reserved for subsequent treatment lines (consider treatment with the drug with the lowest acquisition cost) [2].
GLP-1RAs must be administered subcutaneously, which is a disadvantage relative to the convenient oral administration of most other classes of glucose-lowering drugs. Clinical outcomes in individuals with T2D are worse in those with low treatment adherence, which can be particularly problematic with injectable glucose-lowering drugs, such as GLP-1RAs and insulin. Concerns about injections (e.g. pain, fear of needles, needle size) and the burden/inconvenience of injections are common barriers to using and continuing injectable glucose-lowering drug treatment [76]. GLP-1RAs that are administered once weekly (i.e. dulaglutide, exenatide ER and semaglutide) may be preferred by some patients over the GLP-1RAs that are administered once or twice daily.
No one GLP-1RA has yet been shown to be clearly better overall than the other GLP-1RAs. However, long-acting GLP-1RAs consistently reduce glucose levels across the 1-day or 1-week dosage interval (Sect. 3), and may offer some clinical benefits in selected patients. In meta-analyses, improvements in glycaemic control with long-acting GLP-1RAs were superior those with the short-acting agents, and both short- and long-acting agents reduced weight. No overall clinically meaningful differences were consistently shown between individual short-acting GLP-1RAs. In contrast, of the long-acting GLP-1RAs, semaglutide was significantly more effective in lowering HbA1c levels and reducing weight than the other once-weekly GLP-1RAs (dulaglutide and exenatide ER; Table 2).
Overall, GLP-1RAs are generally well tolerated (Sect. 5), but the common gastrointestinal ADRs can be troublesome and may lead to treatment discontinuation. Such events are generally transient and decrease in frequency over a period of a few weeks or months. More gradual dosage titration may help reduce their frequency and intensity. Injection-site reactions are also common, but transient, and may occur more frequently in patients with relatively high titres of antibodies to the GLP-1RA. Comparative data from the real-world setting would help clarify the relative effectiveness, tolerability and acceptance of this drug class.
Differences in the pharmacological, effectiveness, tolerability and administration profiles of GLP-1RAs should be considered, together with patient preferences, when these drugs are added to lifestyle modifications ± other glucose-lowering drugs. Patients should be advised on the correct use of the GLP-1RA device, as well as the potential for and management of treatment-related ADRs. When used appropriately, GLP-1RAs are a valuable and effective class of glucose-lowering drugs, especially in patients who have difficulty managing T2D with diet/exercise ± metformin and other glucose-lowering drugs.
Change history
12 September 2019
A Correction to this paper has been published: https://doi.org/10.1007/s40261-019-00852-y
10 February 2020
A Correction to this paper has been published: https://doi.org/10.1007/s40261-020-00892-9
17 August 2019
A Correction to this paper has been published: https://doi.org/10.1007/s40261-019-00839-9
References
International Diabetes Federation. IDF clinical practice recommendations for managing type 2 diabetes in primary care. Brussels: International Diabetes Federation; 2017.
American Diabetes Association. 9. Pharmacological approaches to glycemic treatment: standards of medical care in diabetes—2019. Diabetes Care. 2019;42(Suppl 1):S90–102.
Ahren B. Glucagon-like peptide-1 receptor agonists for type 2 diabetes: a rational drug development. J Diabetes Investig. 2018. https://doi.org/10.1111/jdi.12911.
Byetta (exenatide) solution for injection in prefilled-pen: EU summary of product characteristics. Södertälje: AstraZeneca AB; 2018.
Byetta (exenatide) injection: US prescribing information. Wilmington: AstraZeneca Pharmaceuticals LP; 2018.
Victoza (liraglutide) 6 mg/ml solution for injection in pre-filled pen: EU summary of product characteristics. Bagsværd: Novo Nordisk A/S; 2018.
Victoza (liraglutide) injection, for subcutaneous use: US prescribing information. Plainsboro: Novo Nordisk Inc.; 2018.
Lyxumia (lixisenatide) 10 and 20 micrograms solution for injection: EU summary of product characteristic. Paris: Sanofi-aventis Groupe; 2017.
Adlyxin (lixisenatide) injection, for subcutaneous use: US prescribing information. Bridgewater Sanofi-Aventis U.S. LLC; 2019.
Trulicity (dulaglutide) 0.75 and 1.5 mg solution for injection in pre-filled pen: EU summary of product characteristics. Utrecht: Eli Lilly Nederland B.V.; 2018.
Trulicity (dulaglutide) injection for subcutaneous use: US prescribing information. Indianapolis: Eli Lilly and Company; 2019.
Bydureon 2 mg prolonged-release suspension for injection ([powder and solvent; pre-filled pen and BCise): EU summary of product characteristics. Södertälje (Sweden): AstraZeneca AB; 2019.
Bydureon® (exenatide extended-release) for injectable suspension, for subcutaneous use: US prescribing information. Wilmington (DE): AstraZeneca Pharmaceuticals LP; 2018.
Bydureon® BCise™ (exenatide extended-release) injectable suspension, for subcutaneous use: US prescribing information. Wilmington (DE): AstraZeneca Pharmaceuticals LP; 2019.
Ozempic (semagutide) 0.25, 0.5 and 1 mg solution for injection in pre-filled pen: EU summary of product characteristics. Bagsværd: Novo Nordisk A/S; 2018.
Ozempic (semaglutide) injection 0.5 mg/1 mg: US prescribing information. Plainsboro: Novo Nordisk Inc.; 2017.
Sposito AC, Berwanger O, de Carvalho LSF, et al. GLP-1RAs in type 2 diabetes: mechanisms that underlie cardiovascular effects and overview of cardiovascular outcome data. Cardiovasc Diabetol. 2018;17(1):157. https://doi.org/10.1186/s12933-018-0800-2.
Sharma D, Verma S, Vaidya S, et al. Recent updates on GLP-1 agonists: current advancements and challenges. Biomed Pharmacother. 2018;108:952–62.
Gentilella R, Pechtner V, Corcos A, et al. Glucagon-like peptide-1 receptor agonists in type 2 diabetes treatment: are they all the same? Diabetes Metab Res Rev. 2019;35:e3070. https://doi.org/10.1002/dmrr.3070.
Sfairopoulos D, Liatis S, Tigas S, et al. Clinical pharmacology of glucagon-like peptide-1 receptor agonists. Hormones (Athens). 2018;17(3):333–50.
Sun F, Wu S, Gou S, et al. Effect of GLP-1 receptor agonists on waist circumference among type 2 diabetes patients: a systematic review and network meta-analysis. Endocrine. 2015;48(3):794–803.
Madsbad S. Review of head-to-head comparisons of glucagon-like peptide-1 receptor agonists. Diabetes Obes Metab. 2016;18:317–32.
Hitke ZZ, Zaccardi F, Papamargaritis D, et al. Efficacy and safety of glucagon-like peptide-1 receptor agonists in type 2 diabetes: a systematic review and mixed-treatment comparison analysis. Diabetes Obes Metab. 2017;19(4):524–36.
Unni S, Wittbrodt E, Ma J, et al. Comparative effectiveness of once-weekly glucagon-like peptide-1 receptor agonists with regard to 6-month glycaemic control and weight outcomes in patients with type 2 diabetes. Diabetes Obes Metab. 2018;20(2):468–73.
Yu M, Van Brunt K, Varnado OJ, et al. Patient-reported outcome. Results in patients with type 2 diabetes treated with once-weekly dulaglutide: data from the AWARD phase III clinical trial programme. Diabetes Obes Metab. 2016;18(4):419–24.
Best JH, Boye KS, Rubin RR, et al. Improved treatment satisfaction and weight-related quality of life with exenatide once weekly or twice daily. Diabet Med. 2009;26(7):722–8.
Best JH, Rubin RR, Peyrot M, et al. Weight-related quality of life, health utility, psychological well-being, and satisfaction with exenatide once weekly compared with sitagliptin or pioglitazone after 26 weeks of treatment. Diabetes Care. 2011;34(2):314–9.
Rodbard HW, Lingvay I, Reed J, et al. Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN 5): a randomized, controlled trial. J Clin Endocrinol Metab. 2018;103(6):2291–301.
Ahrén B, Masmiquel L, Kumar H, et al. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): a 56-week, double-blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol. 2017;5(5):341–54.
Aroda VR, Bain SC, Cariou B, et al. Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naive patients with type 2 diabetes (SUSTAIN 4): a randomised, open-label, parallel-group, multicentre, multinational, phase 3a trial. Lancet Diabetes Endocrinol. 2017;5(5):355–66.
Ahmann AJ, Capehorn M, Charpentier G, et al. Efficacy and safety of once-weekly semaglutide versus exenatide ER in subjects with type 2 diabetes (SUSTAIN 3): a 56-week, open-label, randomized clinical trial. Diabetes Care. 2017. https://doi.org/10.2337/dc17-0417.
Pratley R, Aroda V, Lingvay I, et al. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol. 2018;6(4):275–86.
Uusinarkaus K, Rodbard HW, Van Gaal L, et al. Semaglutide-induced weight loss is associated with improved health-related quality of life and treatment satisfaction [abstract no. 1020-P]. Diabetes. 2019;68 (Suppl 1). https://doi.org/10.2337/db19-1020-P.
Giorgino F, Penformis A, Pechtner V, et al. Adherence to antihyperglycemic medications and glucagon-like peptide 1-receptor agonists in type 2 diabetes: clinical consequences and strategies for improvement. Patient Prefer Adherence. 2018;12:707–19.
Nguyen H, Dufour R, Caldwell-Tarr A. Glucagon-like peptide-1 receptor agonist (GLP-1RA) therapy adherence for patients with type 2 diabetes in a Medicare population. Adv Ther. 2017;34(3):658–73.
Johnston SS, Nguyen H, Felber E, et al. Retrospective study of adherence to glucagon-like peptide-1 receptor agonist therapy in patients with type 2 diabetes mellitus in the United States. Adv Ther. 2014;31(11):1119–33.
Qaio Q, Ouwens MJ, Grandy S, et al. Adherence to GLP-1 receptor agonist therapy administered by once-daily or once-weekly injection in patients with type 2 diabetes in Germany. Diabetes Metab Syndr Obes. 2016;9:201–5.
Alatorre C, Fernández Landó L, Yu M, et al. Treatment patterns in patients with type 2 diabetes mellitus treated with glucagon-like peptide-1 receptor agonists: higher adherence and persistence with dulaglutide compared with once-weekly exenatide and liraglutide. Diabetes Obes Metab. 2017;19(7):953–61.
Heile M, Wyne K, Billings LK, et al. Cardiovascular outcomes with once-weekly GLP-1 RAs: clinical and economic implications. J Manag Care Spec Pharm. 2018;24(9-a):S42–52.
Bahtiyar G, Pujais-Kury J, Sacerdote A. Cardiovascular effects of different GLP-1 receptor agonists in patients with type 2 diabetes. Curr Diabetes Rep. 2018;18(10):92. https://doi.org/10.1007/s11892-018-1043-z.
Li Y, Rosenbilt PD. Glucagon-like peptide-1 receptor agonists and cardiovascular risk reduction in type 2 diabetes mellitus: is it a class effect? Curr Cardiol Rep. 2018;20(11):113. https://doi.org/10.1007/s11886-018-1051-2.
Torekov SS. Glucagon-like peptide-1 receptor agonists and cardiovascular disease: from LEADER to EXSCEL. Cardiovasc Res. 2018;114(10):e70–1.
Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311–22.
Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet. 2019;1:1. https://doi.org/10.1016/S0140-6736(19)31149-3.
Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–44.
Pfeffer MA, Claggett B, Diaz R, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med. 2015;373(23):2247–57.
Holman RR, Bethel MA, Mentz RJ, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2017;377(13):1228–39.
Bethel MA, Patel RA, Merrill P, et al. Cardiovascular outcomes with glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes: a meta-analysis. Lancet Diabetes Endocrinol. 2018;6(2):105–13.
Filippatos TD, Panagiotopoulou TV, Elisaf MS. Adverse effects of GLP-1 receptor agonists. Rev Diabet Stud. 2014;11(3–4):202–30.
Handelsman Y, Wyne K, Cannon A, et al. Glycemic efficacy, weight effects, and safety of once-weekly glucagon-like peptide-1 receptor agonists. J Manag Care Spec Pharm. 2018;24(9-a):S14–29.
Romera I, Cebrián-Cuenca A, Álvarez-Guisasola F, et al. A review of practical issues on the use of glucagon-like peptide-1 receptor agonists for the management of type 2 diabetes. Diabetes Ther. 2019;10:5–19.
Sun F, Yu K, Yang Z, et al. Impact of GLP-1 receptors agonists on major gastrointestinal disorders for type 2 diabetes mellitus: a mixed treatment comparison meta-analysis. Exp Diabetes Res. 2012;2012:230624.
Wysham C, Blevins T, Arakaki R, et al. Efficacy and safety of dulaglutide added onto pioglitazone and metformin versus exenatide in type 2 diabetes in a randomized controlled trial (AWARD-1). Diabetes Care. 2014;37(8):2159–67.
Filion KB, Azoulay L, Platt RW, et al. A multicenter observational study of incretin-based drugs and heart failure. N Engl J Med. 2016;374(12):1145–54.
Monami M, Nreu A, Scatena S, et al. Glucagon-like peptide-1 receptor agonists and atrial fibrillation: a systematic review and meta-analysis of randomised controlled trials. J Endocrinol Investig. 2017;40(11):1251–8.
Sun F, Wu S, Guo S, et al. Impact of GLP-1 receptor agonists on blood pressure, heart rate and hypertension among patients with type 2 diabetes: a systematic review and network meta-analysis. Diabetes Res Clin Pract. 2015;110(1):26–37.
Vilsboll T, Bain SC, Leiter LA, et al. Semaglutide, reduction in glycated haemoglobin and the risk of diabetic retinopathy. Diabetes Obes Metab. 2019;20(4):889–97.
Dicembrini I, Nreu B, Scatena A, et al. Microvascular effects of glucagon-like peptide-1 receptor agonists in type 2 diabetes: a meta-analysis of randomized controlled trials. Acta Diabetol. 2017;54(10):933–41.
Pang B, Zhou H, Kuang H. The potential benefits of glucagon-like peptide-1 receptor agonists for diabetic retinopathy. Peptides. 2018;100:123–6.
Sun F, Wu S, Wang J, et al. Effect of glucagon-like peptide-1 receptor agonists on lipid profiles among type 2 diabetes: a systematic review and network meta-analysis. Clin Ther. 2015;37(1):225–41.
Filippatos TD, Elisaf MS. Effects of glucagon-like peptide-1 receptors on renal function. World J Diabetes. 2013;4(5):190–201.
Egan AG, Blind E, Dunder K, et al. Pancreatic safety of incretin-based drugs: FDA and EMA assessment. N Engl J Med. 2014;370(9):794–7.
Alves C, Batel-Marques F, Macedo AF. A meta-analysis of serious adverse events reported with exenatide and liraglutide: acute pancreatitis and cancer. Diabetes Res Clin Pract. 2012;98(2):271–84.
Su B, Sheng H, Zhang M, et al. Risk of bone fractures associated with glucagon-like peptide-1 receptor agonists’ treatment: a meta-analysis of randomized controlled trials. Endocrine. 2015;48(1):107–15.
Buse JB, Nauck M, Forst T, et al. Exenatide once weekly versus liraglutide once daily in patients with type 2 diabetes (DURATION-6): a randomised, open-label study. Lancet. 2013;381(9861):117–24.
Kayaniyil S, Lozano-Ortega G, Bennet HA, et al. A network meta-analysis comparing exenatide once weekly with other GLP-1 receptor agonists for the treatment of type 2 diabetes mellitus. Diabetes Ther. 2016;7(1):27–43.
Dungan KM, Povedano ST, Forst T, et al. Once-weekly dulaglutide versus once-daily liraglutide in metformin-treated patients with type 2 diabetes (AWARD-6): a randomised, open-label, phase 3, non-inferiority trial. Lancet. 2014;384(9951):1349–57.
Xultophy (insulin degludec 100 units/mL + liraglutide 3.6 mg/mL) solution for injection in pre-filled pen: EU summary of product characteristics. Bagsværd: Novo Nordisk A/S; 2018.
Xultophy 110/3.6 (insulin degludec and liraglutide injection), for subcutaneous use: US prescribing information. Plainsboro: Novo Nordisk Inc.; 2019.
Suliqua 100/33 (insulin glargine 100 units/ml +lixisenatide 33 or 50 micrograms/ml) solution for injection in a pre-filled pen: EU summary of product characteristics. Paris: Sanofi-Aventis Groupe; 2017.
Soliqua 100/33 (insulin glargine and lixisenatide injection), for subcutaneous use: US prescribing information. Bridgewater: Sanofi-Aventis U.S. LLC; 2017.
Morales J. The pharmacologic basis for clinical differences among GLP-1 receptor agonists and DPP-4 inhibitors. Postgrad Med. 2011;123(6):189–201.
Madsbad S. Dipeptidyl peptidase-4 (DPP-4) inhibitors are favourable to glucagon-like peptide-1 (GLP-1) agonists: no. Eur J Intern Med. 2012;23(2):132–6.
Brunton S. GLP-1 receptor agonists vs. DDP-4 inhibitors for type 2 diabetes: is one approach more successful or preferable than the other? Int J Clin Pract. 2014;68(5):557–67.
Lee G, Oh SW, Hwang SS, et al. Comparative effectiveness of oral antidiabetic drugs in preventing cardiovascular mortality and morbidity: a network meta-analysis. PLoS One. 2017;12(5):e0177646.
Spain CV, Wright JJ, Hahn RM, et al. Self-reported barriers to adherence and persistence to treatment with injectable medications for type 2 diabetes. Clin Ther. 2016;38(7):1653–64.e1.
Acknowledgements
The author thanks Prof. John Wilding, Obesity & Endocrinology Research, Institute of Ageing & Chronic Disease, University of Liverpool, Liverpool, UK for his assistance in preparing this review.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The preparation of this review was not supported by any external funding.
Conflict of interest
K.A. Lyseng-Williamson is an employee of Adis International/Springer Nature, is responsible for the article content and declares no conflicts of interest.
Additional information
The original version of this article was revised due to a retrospective Open Access request.
Article was updated after its initial online publication, and that the current version is the correct one.
Enhanced material for this Adis Disease Management article (including translations) can be found at https://doi.org/10.6084/m9.figshare.11320370.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, duplication, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
About this article

Cite this article
Lyseng-Williamson, K.A. Glucagon-Like Peptide-1 Receptor Agonists in Type 2 Diabetes: Their Use and Differential Features. Clin Drug Investig 39, 805–819 (2019). https://doi.org/10.1007/s40261-019-00826-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-019-00826-0