
Abstract
Background and Objective
Intravesical instillation of glycosaminoglycans is a promising option for the treatment of chronic cystitis, as it supports the regeneration of the damaged urothelial layer. We investigated the efficacy of short-term intravesical chondroitin sulphate treatment (six courses of instillation) in patients with chronic radiotherapy- or chemotherapy-associated cystitis.
Methods
This prospective, observational study included patients with chronic radiotherapy- or chemotherapy-associated cystitis, who received six once-weekly intravesical instillations of 0.2 % chondroitin sulphate 40 mL. Every week, patients recorded their symptoms and their benefits and tolerance of treatment, using a self-completed questionnaire.
Results
The study included 16 patients (mean age 68.5 years; 50 % male). During the study, a reduction in all evaluated parameters was observed. After one dose of chondroitin sulphate, symptom improvement was observed in 38 % of patients, and after the second dose, an additional 31 % of patients showed improvement. At week 6, 80 % of patients had either improved or were symptom free, and significant improvements in urinary urgency (p = 0.0082), pollakisuria (p = 0.0022), urge frequency (p = 0.0033) and lower abdominal pain (p = 0.0449) were observed. Haematuria, present in 9 of the 16 patients at baseline, was completely resolved in all cases after 6 weeks. The majority of patients (93 %) evaluated the tolerance of chondroitin sulphate as ‘good’ or ‘very good’. No treatment-related adverse events were reported.
Conclusion
Intravesical administration of chondroitin sulphate was effective for the treatment of radiotherapy- or chemotherapy-associated cystitis. Even short-term treatment appears to be effective in reducing symptoms and improving the quality of life of patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Intravesically applied chondroitin sulphate was a safe and well-tolerated therapeutic option for the treatment of radiotherapy- or chemotherapy-associated cystitis. |
Even brief treatment with intravesically applied chondroitin sulphate produced rapid symptom improvement in the majority of patients. |
This benefit of glycosaminoglycan replacement therapy positively influences the acceptance of oncological therapies. |
1 Introduction
Nonbacterial cystitis is a common adverse event of radiotherapy and chemotherapy in patients with pelvic tumours. In radiotherapy-associated cystitis, a differentiation is made between the acute and late forms of the disease. Acute toxicity phenomena normally occur 2–3 weeks after the start of radiation to pelvic organs. The symptoms generally resolve spontaneously; however, they lead to a significant decrease in the quality of life [1] and thus affect the acceptance of oncological therapy. The late form of radiogenic cystitis is associated with chronic changes of the bladder wall, which start 6 months after radiotherapy. These alterations lead to vascular and muscle changes and increase the susceptibility to mucosal ulceration and haemorrhage [2]. Approximately 85 % of patients with prostate cancer receiving external radiotherapy (74 Gy) and 24 % of patients with cervical carcinoma receiving brachytherapy develop acute radiogenic cystitis [2, 3]. Recurrent haematuria, a severe symptom of cystitis, which requires surgical intervention, occurs in approximately 8 % of patients 3–6 months following radiation of the bladder [4] and is even more frequent in the interval of 3 months to 5 years. Cystitis is a common chemotherapy-associated complication following intravesical adjuvant therapy for urothelial malignancy. It occurs in up to 21 % of mitomycin C–treated patients and in up to 27 % of bacillus Calmette–Guérin (BCG)–treated patients [5].
Nonbacterial cystitis following radiotherapy and topical chemotherapy presents significant problems for those affected and for health care professionals because of the often unsuccessful long-term treatment [6]. Clinically, the primary symptoms of cystitis are irritative urination and pain, which can significantly reduce quality of life and can possibly affect ongoing oncological therapy [7]. Recurrent haematuria further complicates the situation.
To date, there are no consistent treatment recommendations for the treatment of radiotherapy- and chemotherapy-associated cystitis [8], and in everyday clinical and outpatient practice in Germany, patients with radiotherapy- or chemotherapy-associated cystitis represent an underserved patient group [8]. Given the lack of a causal approach to cystitis, treatment is limited to symptomatic therapy with anticholinergics, analgesics and antibiotics [8]. Furthermore, bladder instillations with chondroitin sulphate have been shown to support the regeneration of the damaged urothelium in patients with interstitial cystitis [9].
While the clinical efficacy of chondroitin sulphate in patients with interstitial cystitis has been investigated thoroughly [9–11], few studies have investigated the efficacy of this treatment in patients with radiotherapy- and chemotherapy-associated cystitis [1, 13]. However, as the pathophysiology of interstitial cystitis is similar to that of radiotherapy- and chemotherapy-associated cystitis, it is likely that instillation therapy with chondroitin sulphate can also be effective in these patients [12, 13]. As such, the objective of this study was to investigate the efficacy and tolerability of short-term treatment with intravesical chondroitin sulphate (Gepan® instill; G. Pohl-Boskamp GmbH & Co. KG, Hohenlockstedt, Germany) in patients with symptomatic radiotherapy- and chemotherapy-associated cystitis.
2 Methods
2.1 Study Design
This observational, prospective study enrolled patients aged ≥18 years with symptomatic radiogenic- or chemotherapy-associated cystitis from July 2011 until June 2012. Patients were enrolled by the participating urologists if they matched the inclusion and exclusion criteria and were willing to take part in the study. Male and female patients aged ≥18 years with a diagnosis of symptomatic chronic radiogenic- or chemotherapy-associated cystitis were eligible for the study. As this study was purely observational, the diagnosis was mainly obtained from the attending urologists’ patient records. No additional invasive examinations were carried out. Patients were excluded from the study if (1) they had a contraindication for Gepan® instill; (2) they were receiving concomitant therapy with another glycosaminoglycan (GAG) replacement treatment or another instillation therapy; (3) they were participating in another clinical study; (4) they were receiving antibiotics for an acute urinary tract infection; (5) they were receiving other medications to treat their bladder symptoms after study inclusion; or (vi) they were pregnant (breastfeeding was not a specific exclusion criterion).
The study was conducted according to the ethical principles of the Declaration of Helsinki, and the study protocol was reviewed and approved by the ethics committee of the University of Leipzig (Ethik-Kommission an der Medizinischen Fakultät der Universität Leipzig), Leipzig, Germany. Written informed consent was obtained from all patients prior to participation in the study.
2.2 Treatment
A total of six instillations of 0.2 % chondroitin sulphate 40 mL (Gepan® instill) were administered weekly. The first instillation was given after baseline characteristics and demographics were collected at visit 1. The treatment was applied (in accordance with the instructions for use) by a trained nurse under the supervision of the attending urologist, or by the attending urologist. The bladder was transurethrally catheterized with a single-use catheter. After the bladder was completely emptied, the entire volume of the solution was instilled in the bladder. Patients were advised to retain the instillation for at least 30 min.
2.3 Outcomes
Patients were assessed at baseline before initiation of 0.2 % chondroitin sulphate treatment and at each weekly study visit until the end of treatment (visit 6). As the study design was purely observational, the main objective was to investigate the effectiveness and tolerability of the instillation treatment. Data collected at baseline included the patient characteristics and demographics, including age, gender, type of cancer, duration of radiotherapy or chemotherapy, cystoscopy findings (if available), previous medications, concomitant medications, current symptoms and duration of symptoms.
At each study visit, the following cystitis symptoms were assessed in each patient, using a self-completed questionnaire: daytime and night-time urinary frequency (patients reported their average number of micturitions during the daytime and night-time, and the micturition count was documented), urinary urgency, pollakisuria, urge frequency, dysuria, lower abdominal pain and haematuria. With the exception of urinary frequency, symptoms were assessed by the patient, using a numerical rating scale (NRS). This 11-item NRS ranged from 0 (symptom free) to 10 (maximal imaginable symptom intensity). Clinical improvement was defined as a reduction in the NRS score of ≥1 point.
Patients were asked to provide their viewpoints on the efficacy and tolerability of 0.2 % chondroitin sulphate treatment at every study visit. Patients self-assessed the severity of their symptoms as ‘symptom free’, ‘improved’, ‘unchanged’ or ‘worsened’. Moreover, at each study visit, they were asked whether any abnormalities had occurred during or after the instillation procedure (this was an open question to encourage the patients to report anything out of the normal). The patients’ urologists also provided their viewpoints on the efficacy and tolerability of 0.2 % chondroitin sulphate treatment. The urologists were asked whether any adverse events had occurred and, if so, were asked to document details of these events throughout the study period.
2.4 Statistical Analyses
Because this was an observational study, no sample size calculation was performed. Quantitative data are presented as means, medians and ranges. Qualitative data are presented as absolute numbers and percentages.
Missing data were excluded from the statistical analysis. All available patient data were consulted to assess tolerability. Statistical calculations were generated using Microsoft Excel (2003) and PRISM (version 4.0, GraphPad). Calculation of significance levels was performed using the Wilcoxon matched-pairs rank test. A p value of <0.05 was defined as being significant.
3 Results
3.1 Patient Disposition and Baseline Characteristics
A total of 16 patients (mean age 68.5 years; 50 % male) were included in the study. Baseline patient demographic and clinical characteristics are listed in Table 1. The mean time between the start of radiotherapy or chemotherapy and the onset of instillation therapy was 2.8 years (minimum 0.4 years; maximum 21 years). For one patient, the period between the start of chemotherapy and the start of instillation therapy was only 5 months. The time period for all other patients between the start of radiotherapy or chemotherapy and the start of instillation therapy was ≥1 year. The majority of patients (n = 12; 75 %) had received at least one treatment for cystitis before enrolment, primarily antibiotics and/or anticholinergics. One patient had received another instillation therapy, and three patients had received analgesics (Table 1). The most common cystitis symptoms experienced by patients at baseline were urinary urgency, pollakisuria and pain (Table 1).
3.2 Effectiveness
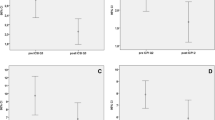
Overall, a rapid reduction of ≥1 point on the NRS in all cystitis symptoms was observed after treatment with 0.2 % chondroitin sulphate, independently of the underlying disease (Fig. 1). After one dose of 0.2 % chondroitin sulphate, clinical improvement was observed in 6 of 16 patients (38 %) (Fig. 2). In an additional 31 % of patients, there was relief of symptoms after the second administration of treatment. At the end of treatment, 80 % of patients either had improved symptoms or were symptom free (Fig. 2). At week 6, the cystitis symptoms of urinary urgency (p = 0.0082), pollakisuria (p = 0.0022), urge frequency (p = 0.0033) and lower abdominal pain (p = 0.0449) were significantly improved from baseline. Furthermore, haematuria, which was present in 9 of the 16 patients at baseline, was completely resolved in all cases after 6 weeks. At week 6, the median micturition frequency was decreased from nine to seven micturitions during the day, and from four to two micturitions during the night.

Changes from baseline in the degree of discomfort of cystitis clinical symptoms (measured using a numerical rating scale [NRS], ranging from 0 [symptom free] to 10 [maximum symptom intensity]) during intravesical treatment with 0.2 % chondroitin sulphate (n = 15)

Proportions of patients with cystitis who were symptom free, had improved disease symptoms, had unchanged disease symptoms and had worsened disease symptoms after intravesical treatment with 0.2 % chondroitin sulphate at each study visit (visits 2–4: n = 16; visits 5 and 6: n = 15)
3.3 Tolerability
Most patients who were included in this study (93 %) evaluated the tolerability of intravesical chondroitin sulphate as ‘good’ or ‘very good’. This rating was congruent with the evaluation by the attending urologists, who assessed the tolerability as ‘good’ or ‘very good’ in 93 % of the cases. There were no adverse events related to the treatment with 0.2 % chondroitin sulphate during the study visits. One male patient terminated the instillation therapy after the third instillation because of catheter intolerance after the operation. This patient completed study visits 1–4 but was not available for visits 5 and 6.
4 Discussion
This investigator-initiated, observational, prospective study investigated the influence of 0.2 % chondroitin sulphate instillations on the symptoms of radiotherapy- or chemotherapy-associated cystitis in 16 patients over a brief observation period. The decisive rationale for this study was to provide a therapeutic option, which, in contrast to other symptom-oriented forms of cystitis treatment, influences the mechanism of development of chronic inflammation and thus represents a causal-oriented therapeutic approach. The results of this study showed that chondroitin sulphate provides rapid improvements in the symptoms of radiotherapy- or chemotherapy-associated cystitis.
To explain why bladder instillations of chondroitin sulphate are beneficial for the treatment of cystitis, it is important to understand the pathophysiology of radiotherapy- and chemotherapy-associated cystitis. Radiotherapy and chemotherapy can damage the GAG layer of the bladder, which leads to a loss of urothelial barrier function [14, 15]. The GAG layer consists of negatively charged sulphated polysaccharides, which are coupled to a negatively charged anchor protein [16]. When the integrity of the GAG layer and urothelial cells is disrupted, the permeability for aggressive components in the urine (potassium ions, proteases, calcium crystals, etc.) is increased. This can increase the stimulation of suburothelial pain fibres. In addition, these generated signals are amplified within the suburothelial networks [17], which explains the clinical symptoms of pain, pollakisuria and urinary urgency seen with cystitis. Finally, damage to the GAG layer can lead to development of a chronic transmural inflammatory process and promotion of bacterial adhesion, causing patients to have recurrent urinary tract infections [18]. The late stage of radiotherapy-associated cystitis is characterized by an alteration of the bladder wall, with angiopathy and interstitial fibrosis (Fig. 3). The consecutive decrease in bladder compliance and anatomical capacity can ultimately lead to a complete loss of bladder function, and sometimes the only possible therapeutic option remaining is a cystectomy. Therefore, a crucial aspect for the success of GAG replacement therapy is a urothelium that can still be regenerated and is treated before ulceration and wall fibrosis occur.

Progressive forms of radiogenic cystitis. Histological image of the bladder wall, trabeculae = 200 μm, Leipzig University Hospital Institute of Pathology. a Preserved urothelium with mild lymphoplasmacellular inflammation in the subepithelial region, smooth muscles unremarkable (haematoxylin and eosin stain). b Significantly flattened urothelium, only a few cell layers preserved (arrow) with moderate lymphoplasmacellular inflammation and proliferation of capillaries in the lamina propria (haematoxylin and eosin stain). c Nearly completely denuded epithelium with erosive, chronic granulating inflammation with interstitial collagen fibre proliferation and capillary vascular proliferates in the mucosal layer and dissemination of the changes to the superficial muscularis layer (Elastica–van Gieson stain). d Significantly flattened mucosal layer with superficially erosive chronic granulating inflammation and reactive capillary proliferates, as well as moderate lymphoplasmacellular infiltrates (haematoxylin and eosin stain)
An available treatment that addresses the cause of chronic cystitis is intravesical instillation of substances that replace the GAG layer—a regimen that was successfully introduced in the 1990s. While this treatment regimen can now be regarded as established in the therapy of interstitial cystitis, it is rarely used in radiotherapy- and chemotherapy-associated cystitis. Of the different substances that are used in GAG replacement therapy, chondroitin sulphate is particularly suitable. Chondroitin sulphate is the GAG, which is located mainly on the luminal side of the urothelium and contributes to maintaining transepithelial resistance [19]. Data from animal studies show that instillation of chondroitin sulphate leads to restoration of the permeability barrier [20]; thus, in the suburothelium, the number of inflammatory cells decreases [12]. Furthermore, for intravesical chondroitin sulphate, it has been proven that the GAG molecules selectively attach apically to damaged areas of mucosa and do not penetrate into deeper layers of the bladder wall [21]. As a result, reductions in clinical symptoms, particularly episodes of urinary urgency, bladder pain and pollakisuria, have been observed with chondroitin sulphate treatment in patients with interstitial cystitis, overactive bladder, radiogenic cystitis and recurrent urinary tract infections with corresponding GAG layer defects [13], and in female patients with overactive bladder [22].
To our knowledge, only one other study has specifically investigated the use of 0.2 % chondroitin sulphate in patients with radiotherapy- and chemotherapy-associated cystitis [1]. In that pilot study, Hazewinkel and colleagues showed that prophylactic intravesical administration of 0.2 % chondroitin sulphate reduced the symptoms of acute radiotherapy- and chemotherapy-associated cystitis. Patients treated with chondroitin sulphate experienced significantly fewer urinary urgency symptoms than those in the control group.
Although the current study and the pilot study reported by Hazewinkel et al. [1] both showed the positive effect of intravesical treatment with 0.2 % chondroitin sulphate, the two studies cannot be compared, as they investigated different indications. While Hazewinkel et al. investigated the potential effect of 0.2 % chondroitin sulphate in preventing radiotherapy- and chemotherapy-associated cystitis, the objective of the current study was investigation of the treatment effect in patients with existing chronic radiotherapy- and chemotherapy-associated cystitis.
As we were able to confirm in this study, an instillation of 0.2 % chondroitin sulphate is an effective therapeutic option for improving parameters that influence quality of life in patients with radiotherapy- and chemotherapy-associated cystitis. Considering the available data from the current study, as well as that of Hazewinkel et al. [1], treatment with 0.2 % chondroitin sulphate seems to be useful in prevention and treatment of radiotherapy- and chemotherapy-associated cystitis. In one recent study of intensity-modulated radiation therapy (IMRT) in prostate carcinoma, the 10‐year risk of grade >2 toxicities of the urinary tract was 17 % [23]. The extent to which patients can benefit from GAG replacement therapy is not yet clear and cannot be definitively assessed using the data available. Experience from clinical practice indicates that GAG replacement therapy is used relatively late. Considering the mechanism of action of GAG replacement, the best possible benefit would involve promoting early use in order to avoid urothelial destruction and fibrosis of the bladder wall.
This work was intended to investigate whether brief treatment with intravesical therapies triggers a therapeutic effect in these indications. Since a significant improvement in symptoms was observed for most symptoms, even after only five applications of chondroitin sulphate, brief installations over short periods of time on a weekly basis appear to be useful.
In the current study, there were two patients with unaltered symptom intensity and one patient with even worsened symptoms. It is not clear whether additional instillations might have improved their symptoms. GAG replacement therapy can be of limited effectiveness in patients with very progressive disease. Additionally, high-degree urge incontinence, highly limited bladder capacity or advanced bladder wall alteration may limit the therapeutic benefit.
Cystoscopy was performed in 69 % of the patients prior to the start of the study. We consider it mandatory to collect cystoscopic baseline findings to record the extent of the urothelial damage, even if the benefit cannot be proven in this work. The cystoscopic findings, and particularly the histopathological assessment, make it possible to optimize the duration of treatment and the instillation intervals, depending on the degree of urothelial damage. In addition, in the event of a clinically unsatisfactory treatment, a cystoscopic assessment of disease progression may be of help. Since most patients have to undergo cystoscopy anyway because of concurrent oncological issues, assessing the composition of the mucosa via a resection biopsy represents only a minimal additional burden for the patient.
The limitations of this study were its short duration and the lack of a control group. The observation time period of 5 weeks in the current investigation represents only a short period in the care of patients with chemotherapy-associated and radiogenic cystitis. No follow-up was performed after the final instillation, so the duration of effects could not be evaluated. Although this observational study did not include a control group, it still demonstrated measurable improvements in a realistic therapeutic setting for the two different chronic diseases studied. Moreover, this study shows that chondroitin sulphate is a possible therapeutic option for patients with multiple prior therapies, as it is well tolerated and provides subjective improvements in patient wellbeing, with the majority of patients reporting symptomatic improvement.
We recommend that future studies of intravesical chondroitin sulphate in radiotherapy- and chemotherapy-induced cystitis should include long-term follow-up to evaluate the duration of the therapeutic effect. Furthermore, the use of a standardized questionnaire would facilitate comparison of the results from different studies.
5 Conclusion
If one summarizes the results of the study, the following lessons can be learned:
-
Brief application of chondroitin sulphate instillations (six weekly instillations) leads to a significant improvement in symptoms of chronic radiotherapy- or chemotherapy-associated cystitis, which positively influences the oncological therapeutic concept.
-
Supportive instillation of chondroitin sulphate for mucosal regeneration should be performed in the case of persistent cystitis following radiation or topical chemotherapy.
References
Hazewinkel MH, Stalpers LJ, Dijkgraaf MG, Roovers JP. Prophylactic vesical instillations with 0.2 % chondroitin sulfate may reduce symptoms of acute radiation cystitis in patients undergoing radiotherapy for gynecological malignancies. Int Urogynecol J. 2011;22(6):725–30.
Dearnaley DP, Hall E, Lawrence D, Huddart RA, Eeles R, Nutting CM, Gadd J, Warrington A, Bidmead M, Horwich A. Phase III pilot study of dose escalation using conformal radiotherapy in prostate cancer: PSA control and side effects. Br J Cancer. 2005;92(3):488–98.
Shakespeare TP, Lim KH, Lee KM, Back MF, Mukherjee R, Lu JD. Phase II study of the American Brachytherapy Society guidelines for the use of high-dose rate brachytherapy in the treatment of cervical carcinoma: is 45–50.4 Gy radiochemotherapy plus 31.8 Gy in six fractions high-dose rate brachytherapy tolerable? Int J Gynecol Cancer. 2006;16(1):277–82.
Martínez-Rodríguez R, Areal Calama J, Buisan Rueda O, González Satue C, Sanchez Macias J, Arzoz Fabregas M, Gago Ramos J, Bayona Arenas S, Ibarz Servio L, Saladié Roig JM. Practical treatment approach of radiation induced cystitis. Actas Urol Esp. 2010;34(7):603–9 (in Spanish).
Shelley MD, Wilt TJ, Court J, Coles B, Kynaston H, Mason MD. Intravesical bacillus Calmette-Guerin is superior to mitomycin C in reducing tumour recurrence in high-risk superficial bladder cancer: a meta-analysis of randomized trials. BJU Int. 2004;93(4):485–90.
Smit SG, Heyns CF. Management of radiation cystitis. Nat Rev Urol. 2010;7(4):206–14.
Berkey FJ. Managing the adverse effects of radiation therapy. Am Fam Physician. 2010;82(4):381–8 (394).
Thompson A, Adamson A, Bahl A, Borwell J, Dodds D, Heath C, Huddart R, McMenemin R, Patel P, Peters J, et al. Guidelines for the diagnosis, prevention and management of chemical- and radiation-induced cystitis. J Clin Urol. 2014;7(1):25–35.
Madersbacher H, van Ophoven A, van Kerrebroeck PE. GAG layer replenishment therapy for chronic forms of cystitis with intravesical glycosaminoglycans—a review. Neurourol Urodyn. 2013;32(1):9–18.
Jocham D, Froehlich G, Sandig F, Ziegler A. The care situation of patients with interstitial cystitis in Germany: results of a survey of 270 patients. Urologe A. 2013;52(5):691–702 (in German).
Neuhaus J, Schwalenberg T. Intravesical treatments of bladder pain syndrome/interstitial cystitis. Nat Rev Urol. 2012;9(12):707–20.
Engles CD, Hauser PJ, Abdullah SN, Culkin DJ, Hurst RE. Intravesical chondroitin sulfate inhibits recruitment of inflammatory cells in an acute acid damage “leaky bladder” model of cystitis. Urology. 2012;79(2):483 (e413–487).
Nordling J, van Ophoven A. Intravesical glycosaminoglycan replenishment with chondroitin sulphate in chronic forms of cystitis: a multi-national, multi-centre, prospective observational clinical trial. Arzneimittelforschung. 2008;58(7):328–35.
Damiano R, Cicione A. The role of sodium hyaluronate and sodium chondroitin sulphate in the management of bladder disease. Ther Adv Urol. 2011;3(5):223–32.
Hauser PJ, Dozmorov MG, Bane BL, Slobodov G, Culkin DJ, Hurst RE. Abnormal expression of differentiation related proteins and proteoglycan core proteins in the urothelium of patients with interstitial cystitis. J Urol. 2008;179(2):764–9.
Parsons CL. The role of a leaky epithelium and potassium in the generation of bladder symptoms in interstitial cystitis/overactive bladder, urethral syndrome, prostatitis and gynaecological chronic pelvic pain. BJU Int. 2011;107(3):370–5.
Neuhaus J, Heinrich M, Schlichting N, Oberbach A, Fitzl G, Schwalenberg T, Horn LC, Stolzenburg JU. Structure and function of suburothelial myofibroblasts in the human urinary bladder under normal and pathological conditions (in German). Urologe A. 2007;46(9):1197–202.
Parsons CL, Mulholland SG, Anwar H. Antibacterial activity of bladder surface mucin duplicated by exogenous glycosaminoglycan (heparin). Infect Immun. 1979;24(2):552–7.
Janssen DA, van Wijk XM, Jansen KC, van Kuppevelt TH, Heesakkers JP, Schalken JA. The distribution and function of chondroitin sulfate and other sulfated glycosaminoglycans in the human bladder and their contribution to the protective bladder barrier. J Urol. 2013;189(1):336–42.
Hauser PJ, Buethe DA, Califano J, Sofinowski TM, Culkin DJ, Hurst RE. Restoring barrier function to acid damaged bladder by intravesical chondroitin sulfate. J Urol. 2009;182(5):2477–82.
Kyker KD, Coffman J, Hurst RE. Exogenous glycosaminoglycans coat damaged bladder surfaces in experimentally damaged mouse bladder. BMC Urol. 2005;5:4.
Gauruder-Burmester A, Popken G. Follow-up at 24 months after treatment of overactive bladder with 0.2 % sodium chondroitin sulfate. Aktuelle Urol. 2009;40(6):355–9 (in German).
Alicikus ZA, Yamada Y, Zhang Z, Pei X, Hunt M, Kollmeier M, Cox B, Zelefsky MJ. Ten-year outcomes of high-dose, intensity-modulated radiotherapy for localized prostate cancer. Cancer. 2011;117(7):1429–37.
Author contributions
TS was responsible for the design of the trial and acted as the responsible scientific study expert overseeing the entire trial. All authors were involved in the conception and planning of the study; evaluation of the data; and drafting, revision and approval of the final submitted version of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This investigator-initiated study (sponsor: Universitätsklinik Leipzig AöR, Leipzig, Germany) was supported in the following form by G. Pohl-Boskamp GmbH & Co. KG (Hohenlockstedt, Germany): study medication, and minor financial and administrative support for orderly conduct of the study.
Medical writing assistance was provided by Sheridan Henness, Simone Boniface and Mary Hines of Springer Healthcare Communications, and was funded by G. Pohl-Boskamp GmbH & Co. KG.
Conflicts of interest
TS and FB received financial support from G. Pohl-Boskamp GmbH & Co. KG in the form of expenses for the publication. LH, PT, JS and JN have no conflicts of interest to declare. At no time did G. Pohl-Boskamp GmbH & Co. KG apply undue influence on the data presented here and the conclusions drawn from them.
Ethical approval
This study was performed in accordance with the Declaration of Helsinki 1964 and its amendments. The study protocol, patient information and informed consent form were reviewed and approved by the responsible ethics committee of Leipzig University (Ethik-Kommission an der Medizinischen Fakultät der Universität Leipzig), Leipzig, Germany.
Informed consent
Participation in this study was voluntary. Only patients who were willing and able to provide informed consent were eligible.
Additional information
T. Schwalenberg and F. P. Berger share lead authorship of this manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Schwalenberg, T., Berger, F.P., Horn, L.C. et al. Intravesical Glycosaminoglycan Replacement with Chondroitin Sulphate (Gepan® instill) in Patients with Chronic Radiotherapy- or Chemotherapy-Associated Cystitis. Clin Drug Investig 35, 505–512 (2015). https://doi.org/10.1007/s40261-015-0306-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-015-0306-6