
Abstract
Introduction
The study aimed to evaluate multi-symptom relief of dry eye manifestations with the use of propylene glycol-hydroxypropyl-guar (PG-HPG) nanoemulsion lubricant eye drops, among subjects with dry eye disease (DED).
Methods
This was a post-marketing, prospective, single-arm study conducted in the USA. Subjects aged ≥ 18 years, with tear breakup time (TBUT) ≤ 10 s for both eyes, dry eye questionnaire-5 (DEQ-5) “watery eyes” symptom score 1–4, symptoms of burning/stinging, sore and tired eyes as determined by impact of dry eye on everyday living—symptom bother (IDEEL-SB) questionnaire, and IDEEL-SB score 16–65 were included. Subjects were required to complete IDEEL-SB and DEQ-5 at days 0, 14 ± 2, and 28 ± 2, and self-administer one drop of PG-HPG four times daily for 28 ± 2 days. Primary endpoints were change from baseline at day 28 in symptoms of sore, stinging/burning, and tired eyes on IDEEL-SB; and symptom of watery eyes on DEQ-5. Other endpoints evaluated were corneal staining and TBUT at baseline and day 28 ± 2; symptom relief (5-point Likert scale) at day 28 ± 2, and safety.
Results
Of 119 subjects enrolled, 95 completed the study (mean ± SD age 61.2 ± 13.0 years; female 69.5%). Mean IDEEL-SB scores reduced significantly from baseline at day 28 for symptoms of aching/sore eyes (change from baseline − 1.0 ± 1.1), burning/stinging eyes (change from baseline − 1.1 ± 0.9), and tired eyes (change from baseline − 1.1 ± 1.0) (all p < 0.0001). Mean DEQ-5 score for watery eye symptoms significantly reduced from baseline at day 28 (change from baseline − 0.9 ± 1.0, p < 0.0001). Corneal staining at day 28 was comparable to baseline. TBUT improved from baseline to day 28. On a Likert scale, more than 50% of subjects reported relief from symptoms of sore, stinging, and burning eyes. Three (3.1%) subjects reported treatment-emergent adverse events (non-ocular).
Conclusions
PG-HPG nanoemulsion lubricant eye drops significantly improved multiple dry eye symptoms in subjects with DED over 28 days, with no new safety concerns.
Trial Registration
ClinicalTrials.gov Identifier, NCT05056155.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? | |
Propylene glycol-hydroxypropyl-guar (PG-HPG) nanoemulsion lubricant eye drops are indicated for the temporary relief of burning and irritation due to dryness of the eye. | |
There is a need to assess the effects of these eye drops in relieving multiple symptoms of dry eye comprehensively in the real world. | |
This study aimed to evaluate multi-symptom relief (sore, watery, stinging, burning, and tired eyes) of dry eyes with the use of PG-HPG nanoemulsion lubricant eye drops among subjects with dry eye disease (DED). | |
What was learned from the study? | |
PG-HPG nanoemulsion lubricant eye drops significantly improved symptoms of aching/sore, burning/stinging, and tired eyes, as evaluated by IDEEL-SB scores at day 28 in subjects with DED; the improvement in symptoms was also clinically meaningful. | |
The eye drops significantly improved the symptom of watery eyes, as evaluated by DEQ-5 scores, at day 28. | |
PG-HPG nanoemulsion lubricant eye drops provided multi-symptom relief in subjects with DED, as early as day 14, with no new safety concerns. |
Introduction
Dry eye disease (DED) is a multifactorial ocular surface disease characterized by a loss of tear film homeostasis and accompanied by symptoms such as eye discomfort and visual disturbances [1,2,3] that may impair quality of life of patients with dry eye [4, 5]. DED is a common condition that has impacted at least 344 million people worldwide, and at least 30 million people in the USA alone [1, 3]. The prevalence of DED ranges widely from 5% to 50% with or without symptoms, and up to 75% based on signs alone [3, 6]. Further, the prevalence increases with age (18–34 years vs ≥ 75 years, 2.7% vs 18.6%), and is higher among women than men (8.8% vs 4.5%) in the USA [7]. The estimated prevalence is also high among visual display terminal users (e.g., computers and smartphones users; 9.5–87.5%) [8].
DED is etiologically classified as aqueous deficient dry eye (ADDE), evaporative dry eye (EDE), and mixed DED [3, 9]. ADDE occurs as a result of a decrease in tear production by the lacrimal gland [3]. EDE is more common and occurs as a result of conditions that affect the eyelid (e.g., meibomian gland dysfunction and blink abnormalities) or ocular surface (e.g., mucin deficiency and contact lens wear) that result in abnormal lipid secretion, tear film instability, and excessive evaporation of tears [3, 10]. As DED progresses, it adapts the characteristics of both ADDE and EDE simultaneously, known as mixed DED [3, 10].
The mainstay of DED treatment is the use of artificial tear drops or lubricant eye drops [9]. Most of the artificial tear drops are formulated to supplement either the lipid or aqueous layer of the tear film in dry eye [11]. As DED progresses, both ADDE and EDE overlap and become clinically prominent [10]; this necessitates supplementing both aqueous and lipid layers of the tear film [12]. Propylene glycol-hydroxypropyl-guar (PG-HPG) nanoemulsion lubricant eye drop is formulated to replenish and restore both lipid and aqueous layers of the tear film [13, 14]. PG-HPG nanoemulsion lubricant eye drops have been evaluated in several preclinical [15, 16] and clinical [17,18,19,20] studies, and have been found to be safe and effective in terms of alleviating the signs and symptoms of DED.
Further, clinical studies demonstrated that PG-HPG nanoemulsion lubricant eye drop was well tolerated and effective in relieving dry eye symptoms, reducing ocular discomfort, and providing soothing sensation in patients with DED, regardless of the subtype (EDE, ADDE, and mixed DED) [17, 18]. The drops also enhance tear film stability, and improve lipid layer thickness/grade in subjects with suboptimal lipid layer thickness in DED [19,20,21]. Moreover, PG-HPG nanoemulsion eye drops provide prophylactic benefits against adverse environmental conditions in subjects with DED, by preserving tear film quality and reducing ocular discomfort [21]. The PG-HPG nanoemulsion eye drops are indicated for the temporary relief of burning and irritation due to dryness of the eye, and for the temporary relief of discomfort due to minor irritations of the eye or exposure to wind or sun [22]; and are intended for use in subjects with DED.
As a result of the multifactorial nature of the disease, the management of DED is complicated [9]. It depends on the severity of symptoms as well as signs; and the treatment plan may involve one or more interventions based on the etiology and symptoms [9]. Further, managing multiple symptoms of DED can be challenging because of the complex nature of the disease and wide variation in symptoms [23]. The DED symptoms encompass a broad range of patient-reported experiences (other than discomfort and visual disturbances), such as dryness, stinging, burning, itching, blurry vision, tired eyes, and redness that negatively impact patient’s quality of life [3, 24, 25]. A treatment approach that targets multiple symptoms of DED and provides multi-symptom relief to patients is crucial. Furthermore, symptoms of DED are a common trigger for subjects to pursue eye care, and consequently have emerged as crucial outcome measures for clinicians and investigators in clinical studies to assess the impact of DED treatments. Previous studies have reported the efficacy of PG-HPG nanoemulsion lubricant eye drops in relieving overall dry eye symptoms [17,18,19,20]; however, to date, no study has assessed the effects of these eye drops in relieving multiple symptoms of dry eye comprehensively. We hypothesized that, as evident in the previous clinical efficacy studies [17,18,19,20], the use of PG-HPG nanoemulsion lubricant eye drops might be effective in providing relief from multiple symptoms of dry eyes in real-world clinical settings. Hence, this post-marketing clinical study aimed to evaluate multi-symptom (sore, watery, stinging, burning, and tired eyes) relief with the use of PG-HPG nanoemulsion lubricant eye drops among subjects with DED.
Methods
Study Design
This was a post-marketing, prospective, interventional, single-arm study conducted to evaluate multi-symptom relief with the use of PG-HPG nanoemulsion lubricant eye drops, over 28 days, in subjects with DED at four clinical sites in the USA from November 2021 to March 2022 (NCT05056155).
Eligibility Criteria
This study included subjects aged ≥ 18 years who had tear breakup time (TBUT) ≤ 10 s for both eyes; dry eye questionnaire-5 (DEQ-5) “watery eyes” symptom score 1–4; impact of dry eye on everyday living—symptom bother (IDEEL-SB) questionnaire score of 16–65; and the symptoms of burning, stinging, sore, and tired eyes as determined by the IDEEL-SB questionnaire. Some of subjects were non-treatment naïve. Subjects were required to be willing to discontinue the use of their habitual artificial tear supplements for the duration of the study. Subjects using cyclosporine/other topical dry eye prescriptive medications were required to be on a stable dosing regimen for at least 60 days before enrollment.
Subjects were excluded from the study if they had current punctal plugs/occlusion; or had clinically significant corneal scarring, corneal degeneration, and/or dystrophy, blepharitis in either eye, or meibomian gland disease as determined by the investigator. Subjects who used contact lenses within 1 week before screening or who were unwilling to avoid contact lens use during the study were excluded. Subjects using any systemic medications known to cause dry eye within the 1 month before screening were also excluded.
Study Visits and Treatment
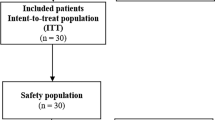
Subjects participated in the study for approximately 28 days. The screening/baseline visit (in-clinic) on day 0 was followed by a phone call on day 14 ± 2 and a follow-up visit (in-clinic) on day 28 ± 2 (Fig. 1). On day 0, subjects were assessed for eligibility, and eligible subjects received the first dose of PG-HPG nanoemulsion lubricant eye drops (SYSTANE™ Complete, Alcon Laboratories, Inc., Fort Worth, TX, USA; 1 mL drop [0.6%]). Subjects were required to self-administer one drop for four times daily for 28 ± 2 days.

Study design and patient disposition. HPG, hydroxypropyl guar; PG, propylene glycol
On day 0, subjects were asked to complete electronic patient questionnaires (IDEEL-SB and DEQ-5) on their own electronic device (smartphone or tablet). Subjects were also asked to complete electronic patient questionnaires at day 14 ± 2 (IDEEL-SB and DEQ-5) and at day 28 ± 2 (IDEEL-SB, DEQ-5, and Likert questionnaire). In addition, subjects were instructed to document their eye drop dosing information on a daily basis in an electronic diary.
Study Endpoints
Primary endpoint was the change from baseline at day 28 in symptoms of sore, stinging/burning, and tired eyes assessed using IDEEL-SB questionnaire, and symptom of watery eyes assessed using DEQ-5. Other endpoints were frequency and bothersomeness of symptoms on IDEEL-SB, frequency and intensity of symptoms on DEQ-5, corneal staining, osmolarity, binocular best-corrected visual acuity (BCVA; logMAR), and TBUT evaluated at baseline and day 28 ± 2; and symptom relief evaluated using Likert questionnaire on day 28 ± 2.
Safety endpoints included adverse events that were reported throughout the study period. Subjects were monitored for any untoward changes in their health or changes in any parameters including the administered questionnaires. Any untoward changes in a parameter or questionnaire were considered as clinically significant and reported as an AE. Further, any clinically significant worsening of baseline conditions or new conditions detected in subjects after instillation of the study eye drops were reported as AEs.
Biomicroscopic findings, ocular signs for each eye (such as aqueous flare and aqueous cells), were assessed by slit lamp biomicroscopy at baseline and day 28 ± 2.
Study Measures/Assessments
Data on subjects’ demographic characteristics and medical history were collected at baseline. The IDEEL-SB module consists of 20 questions that assess general dry eye symptoms experienced/reported by subjects over the last 2 weeks. Question 1 (dry eye symptom frequency) is scored on a 5-point Likert-scale (0 = none of the time, 1 = a little of the time, 2 = some of the time, 3 = most of the time, and 4 = all of the time). Questions 2–20 (symptom bothersomeness) are scored on a 5-point Likert-scale (0 = I did not have this symptom/not applicable, 1 = not at all bothered, 2 = slightly bothered, 3 = moderately bothered, and 4 = very much bothered). The overall IDEEL-SB score is calculated as the mean value of the non-missing item scores for questions 1–20 multiplied by 25. The scores for individual symptom ranges from 0 to 4, with lower scores indicating less bothersomeness. The overall resultant calculated score ranges from 0 to 100, where higher scores indicate greater symptom bother [26, 27].
The DEQ-5 consists of five questions that assess the subject-reported symptoms of eye discomfort, eye dryness, and watery eyes during a typical day in the past month. The symptoms are scored on a scale of 0 to 4 (frequency: 0 = never, 1 = rarely, 2 = sometimes, 3 = frequently, and 4 = constantly) or 0 to 5 (intensity: 0 = never have it, 1 = not at all intense, and 5 = very intense). The scores range from 0 to 22 [28].
Corneal fluorescence staining was evaluated for five corneal regions (central, superior, inferior, temporal, and nasal). Each of the five corneal regions were graded using the National Eye Institute (NEI) grading scale of 0–3 (0 = normal, negative slit lamp findings; 1 = mild, superficial stippling; 2 = moderate, punctate staining including superficial abrasion of the cornea; 3 = severe, abrasion or corneal erosion, deep corneal abrasion, or recurrent erosion) [29].
Tear stability was measured as TBUT using sodium fluorescein (NaFl) strip technique; and the average of three measurements was calculated. Osmolarity was assessed using the Tearlab osmolarity system.
Further, the symptom relief was assessed using a Likert questionnaire containing five questions (5-point scale: strongly agree, agree, neither agree nor disagree, disagree, strongly disagree). The BCVA (logarithm of the minimum angle of resolution, logMAR) was also evaluated.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and Council for International Organizations of Medical Sciences (CIOMS) International Ethical Guidelines, International Council for Harmonization (ICH) GCP guidelines. The study protocol and informed consent form were reviewed and approved by the Institutional Review Board (IRB), Advarra IRB (Columbia, MD) before study commencement; and written informed consent was obtained from each subject before enrollment in the study.
Statistical Analysis
Statistical analyses were performed using SAS® software v9.4 (SAS Institute Inc., Cary, NC). Categorical variables were summarized as counts and percentages; continuous variables were summarized as means and standard deviations (SDs).
Endpoints were analyzed for both per-protocol and safety analysis sets of subjects. The safety analysis set included subjects who received at least one dose of eye drops; and the per-protocol (PP) analysis set was a subset of the safety analysis set and only included subjects who met eligibility criteria and completed the study. Here we report the primary and other endpoint results for the per-protocol set, and safety results for the safety analysis set.
Primary endpoints: The changes in symptom scores from baseline at day 28 (for each of the four symptoms) were analyzed using paired t tests (corroborated with Wilcoxon signed-rank test). To control the testing of multiple endpoints, the Holm method was implemented with an initial α level of 0.0125 (0.05/4) to assess superiority. The p value comparisons of 0.0125, 0.0167, 0.025, and 0.05 for the four endpoints were based on the initial α of 0.05. All other endpoints were each summarized descriptively. No inferential testing was carried out.
Sample Size
Sample size was based on a prior clinical study [30] that evaluated the symptom bother module of the IDEEL questionnaire in subjects with evaporative DED. As a result of the lack of validation and relevant data on clinically meaningful difference for individual items of the IDEEL-SB questionnaire and DEQ-5, a sample size of 78 was calculated on the basis of 87% power (slightly higher power than the standard 80%) and a one-sided α of 0.01.
Results
A total of 119 subjects were enrolled in this study, of whom 23 were excluded because of screen failure, technical reasons, ongoing treatment with prohibited medication, or other reasons. Thus, overall, 96 subjects were included in the safety analysis set, and 95 subjects in the PP analysis set (one subject in the safety analysis set discontinued because of an adverse event) (Fig. 1).
Demographics and Clinical Characteristics
The mean ± SD age of subjects in the PP analysis set was 61.2 ± 13.0 years; the majority were female (69.5%), of white race (94.7%), and not of Hispanic or Latino ethnicity (95.8%) (Table 1). Additional information, such as medical history and treatment compliance of the subjects, is detailed in Table 1.
The IDEEL-SB scores (mean ± SD) of the subjects at baseline were 2.4 ± 0.7 for aching or sore eyes; 2.7 ± 0.6 for burning or stinging eyes, and 2.8 ± 0.6 for tired eyes. At baseline, the overall mean ± SD DEQ-5 score was 13.8 ± 2.6 and the mean ± SD DEQ-5 watery eyes symptom score was 2.1 ± 0.8.
Primary Endpoints: Changes in Aching/Sore, Burning/Stinging, Tired Eyes Symptom Scores on IDEEL-SB and Watery Eyes Symptom Scores on DEQ-5, from Baseline at Day 28
The IDEEL-SB scores reduced significantly from baseline at day 28 for aching or sore eyes (mean ± SD, 1.4 ± 0.9; change from baseline − 1.0 ± 1.1), burning or stinging eyes, (mean ± SD, 1.6 ± 0.9; change from baseline − 1.1 ± 0.9), and tired eyes (mean ± SD, 1.7 ± 0.9; change from baseline − 1.1 ± 1.0) (all p < 0.0001) (Fig. 2).

Changes in IDEEL-SB scores for dry eye symptoms from baseline at day 14 and day 28. Error bars represent standard deviation. *p < 0.0001 for mean changes in IDEEL-SB scores from baseline at day 14 and day 28. A paired t test was used on the mean changes from baseline at day 14 and day 28; corroborated with Wilcoxon signed-rank test. IDEEL-SB, Impact of dry eye on everyday living—symptom bother
Furthermore, the DEQ-5 score for symptom of watery eyes was decreased significantly from baseline at day 28 (mean ± SD, 1.3 ± 1.0; change from baseline − 0.9 ± 1.0) (p < 0.0001) (Fig. 3).

Change in DEQ-5 scores for watery eyes symptom from baseline at day 14 and day 28. Error bars represent standard deviation. *p < 0.0001 for mean changes in DEQ-5 scores (watery eyes) from baseline at day 14 and day 28. A paired t test was used on the mean changes from baseline at day 14 and day 28; corroborated with Wilcoxon signed-rank test. DEQ-5, 5-item dry eye questionnaire
Other Endpoints
Changes in Aching/Sore, Burning/Stinging, Tired Eyes Symptom Scores on IDEEL-SB and Watery Eyes Symptom Scores on DEQ-5, from Baseline at Day 14
A significant reduction in IDEEL-SB scores was observed from baseline at day 14 for aching or sore eyes (mean ± SD, 1.6 ± 0.9; change from baseline − 0.8 ± 1.0), burning/stinging eyes (mean ± SD, 1.9 ± 0.9; change from baseline − 0.8 ± 1.0), and tired eyes (mean ± SD, 2.0 ± 0.8; change from baseline − 0.8 ± 0.9) (all p < 0.0001) (Fig. 2).
The DEQ-5 score for symptom of watery eyes was decreased significantly from baseline at day 14 (mean ± SD, 1.6 ± 0.9; change from baseline − 0.6 ± 0.9) (p < 0.0001) (Fig. 3).
IDEEL-SB: Changes in Frequency and Bothersomeness of Symptoms
The percentage of subjects with no symptom of aching or sore eyes or who were “not at all” bothered by the symptom at baseline (4.3%) increased at day 14 (45.2%) and day 28 (57.5%) on IDEEL-SB. Consequently, percentage of subjects who were “very much” or “moderately” bothered by aching or sore eyes at baseline (34.0%) showed a reduction at day 14 (10.7%) and day 28 (8.0%) (Table S1). Similarly, the percentage of subjects with no symptom of burning/stinging eyes or who were “not at all” bothered by the symptom increased from baseline (1.1%) to day 14 (28.6%) and day 28 (44.8%) on IDEEL-SB. Further, the percentage of subjects who had no symptom of tired eyes or were “not at all” bothered by tired eyes increased from baseline (0.0%) to day 14 (21.4%) and day 28 (41.4%); consequently, the percentage of subjects who were “very much” or “moderately” bothered by symptom of tired eyes at baseline (68.1%) reduced at day 14 (20.2%) and day 28 (17.2%) on IDEEL-SB. Similar trends were observed for the frequency of all other symptoms on the IDEEL-SB questionnaire (Table S1).
DEQ-5: Changes in Frequency and Intensity of Symptoms
On DEQ-5, the percentage of subjects reporting symptom of watery eyes as “frequently” or “constantly” at baseline (30.9%) decreased to 13.6% at day 14 and 12.4% at day 28; whereas the percentage of subjects reporting “never” or “rarely” experiencing the watery symptom at baseline (23.4%) increased to 51.9% at day 14 and 65.2% at day 28 (Table S2). Furthermore, similar results were observed for the frequency and intensity of other symptoms (eye discomfort and dryness) on DEQ-5 (Table S2).
Corneal Staining
The majority of the subjects had “normal, negative slit lamp findings” or “mild, superficial stippling” for the five zones assessed at baseline; the results at day 28 were comparable to the baseline data (Table S3).
Osmolarity
Osmolarity was comparable at baseline (OD, 310.6 ± 20.7; OS, 305.5 ± 18.1) and day 28 (OD, 309.3 ± 21.7; OS, 306.5 ± 17.5).
Visual Acuity
Visual acuity (logMAR) was also found to be comparable at baseline (OD, 0.03 ± 0.12; OS, 0.03 ± 0.12) and day 28 (OD, 0.01 ± 0.12; OS, 0.01 ± 0.13) (Table S4).
Tear Breakup Time
TBUT (seconds) increased/improved from baseline (OD, 5.6 ± 2.2; OS, 5.1 ± 2.0) to day 28 (OD, 7.3 ± 3.1; OS, 6.5 ± 2.6) (Table S4).
Dry Eye Symptom Relief Using Likert Questionnaire
For the dry eye symptom relief (Likert questionnaire), more than 50% of subjects reported relief (agreed/strongly agreed) from symptoms of sore eyes (59.8%), stinging eyes (55.2%), and burning eyes (52.9%) at day 28 (Fig. 4) whereas 48.3% and 36.8% of subjects reported relief from symptoms of tired eyes and watery eyes at day 28, respectively.

Subject-reported relief from dry eye symptoms on the 5-point Likert scale at day 28 (n = 87)
Safety
Of the 96 subjects in the safety analysis set, 3 (3.1%) experienced treatment-emergent adverse events (TEAEs) of non-ocular nature: COVID-19 infection (n = 1), herpes zoster (n = 1), and kidney infection (n = 1); none were related to the study treatment. One subject (1.0%) experienced a serious adverse event (SAE, kidney infection; not related to study treatment) (Table S5). There were no deaths reported in the study. No subjects had aqueous flare or aqueous inflammatory cell in slit lamp biomicroscopy at baseline and at day 28 (Table S5).
Discussion
This post-marketing, prospective, interventional, single-arm, multicenter clinical study evaluated the effects of PG-HPG nanoemulsion lubricant eye drops in providing relief from multiple symptoms of dry eye (sore, watery, stinging, burning, and tired eyes) in subjects with DED, over a period of 28 days.
The mean IDEEL-SB scores for symptoms of aching/sore, stinging/burning, and tired eyes significantly reduced from baseline at day 28 (change from baseline − 1.0 ± 1.1, − 1.1 ± 0.9, and − 1.1 ± 1.0 respectively; all p < 0.0001) with PG-HPG nanoemulsion lubricant eye drops. The results suggest that improvements in these symptoms at day 28 were clinically meaningful (at least a 1-point reduction at individual item level from the IDEEL-SB questionnaire). The IDEEL-SB questionnaire has been previously applied to assess symptom improvement in subjects with EDE by Wesley et al. [30]. Further, a 12-point shift in the IDEEL-SB module score is considered as clinically important difference that relates to a self-report of global change in dry eye condition after the treatment [27]. On the basis of this, in the study conducted, an item-level change of 1 in IDEEL-SB was considered to be a clinically meaningful difference. Additionally, significant improvements in aching/sore eyes, stinging/burning eyes, and tired eyes symptoms on the IDEEL-SB were also observed as early as day 14 (all p < 0.0001), demonstrating quick improvement in dry eye symptoms. Further, improvements were observed for all other symptoms assessed in the IDEEL-SB in the present study.
DEQ-5 score for symptom of watery eyes improved significantly from baseline at day 14 and day 28 (both p < 0.0001). Similarly, DEQ-5 scores for other symptoms (eye dryness and discomfort) also significantly improved from baseline at day 14 and day 28 (all p < 0.0001). Thus, our findings indicate that PG-HPG nanoemulsion lubricant eye drops can provide dry eye symptom relief in subjects with DED and are consistent with those reported in previous studies using other instruments (e.g., ocular surface disease index [OSDI], ocular discomfort visual analogue scale [VAS]) [18,19,20]; however, heterogeneity in methods and symptom assessment tools may limit the direct comparison of the present study results with previous studies. A prospective study by Craig et al. demonstrated that instillation of PG-HPG nanoemulsion lubricant eye drops QID, over 6 months, significantly reduced OSDI, DEQ-5, and symptom assessment in dry eye (SANDE) dry eye symptomology scores from day 30 onwards (all p < 0.001), with reduction in the scores being sustained for up to 180 days (all p ≤ 0.01) [19]. Similarly, a phase IV study evaluating the safety and efficacy of PG-HPG nanoemulsion (one drop BID for 28 days) reported improvement in ocular discomfort VAS score (at day 14) [18]. Further, a 1-month observational study showed clinically and statistically significant improvement in dry eye symptoms on VAS (dryness score; p = 0.045) and OSDI (average score; p = 0.03) from baseline at 1 month with the daily use of PG-HPG nanoemulsion lubricant eye drops (QID) [20].
Furthermore, along with the improvement of dry eye symptoms observed in this study, the percentage of subjects who experienced no symptoms or who were “not at all” bothered by symptoms on IDEEL-SB also increased from baseline at day 14 and day 28 (e.g., aching/sore, stinging/burning, tired). These results emphasize the reduction in dry eye symptoms (both frequency and bothersomeness) with the use of PG-HPG nanoemulsion lubricant eye drops. In line with the IDEEL-SB and DEQ-5 results, on the Likert scale more than 50% of subjects agreed/strongly agreed about experiencing relief from symptoms of sore, stinging, and burning eyes. Relief from symptoms of tired and watery eyes was experienced by a slightly lower proportion of subjects (less than 50%). These results depict the relief of symptoms of dry eye with the use of the eye drop in subjects with DED over 28 days.
The improvement in dry eye symptoms as observed in this clinical study may be attributed to the unique formulation of PG-HPG nanoemulsion lubricant eye drop that contains PG as demulcent, nanodroplets of an anionic phospholipid/mineral oil complex, and a high concentration of HPG. The nano size of the droplets provides benefits of better ocular surface coverage of phospholipids to replenish tear film lipid layer. Further, the HPG forms in situ HPG/borate gel complex upon instillation of eye drops that prolongs the ocular retention of demulcent, enhances tear film stability, and protects the ocular surface, thereby reducing the symptoms of DED [13, 15]. Further, the anionic phospholipids present in the eye drop can be beneficial for the proper structuring of the polar lipid layer and help in maintaining tear film stability by acting as an effective interface between outer non-polar lipid and inner aqueous layers of tear film [15, 18]. In our study, the TBUT increased at day 28, thus depicting an improvement in tear film stability after the use of the eye drop, which could be a reason for relief from dry eye symptoms in subjects with DED. The improvement in TBUT is consistent with previous research on PG-HPG nanoemulsion lubricant eye drops [18].
In this study, no new safety concerns were observed with the use of the eye drops, and the safety results were consistent with the known safety profile of the eye drop [22].
To the best of our knowledge this is the first type of study of PG-HPG nanoemulsion lubricant eye drops showing clinically meaningful improvement in multiple symptoms of dry eye in subjects with DED across the USA.
The limitations of the study are its single-arm nature which limits the comparison of the study eye drops to other standards of treatment and restricts the inference of results to effectiveness of only the study eye drops. However, a comparison of the PG-HPG nanoemulsion lubricant eye drop with existing market products was not performed because of the unique combination of HPG and nanotechnology in this formulation. The study considered a 1-point change in the IDEEL-SB score as a clinically meaningful difference. There is limited literature on validated criteria which provides clinically significant difference in the individual scores of patient-reported outcomes or quality of life. In addition, recall or response bias associated with subject-reported assessments could have influenced the outcomes reported in the study. Finally, there were a limited number of clinical sites in the study which may not be representative of the broader, more diverse populations.
This study evaluated the multi-symptom relief with PG-HPG nanoemulsion lubricant eye drops in subjects with DED for 28 days. The head-to-head comparison between PG-HPG nanoemulsion lubricant eye drop and an existing lubricating eye drop, and the effectiveness of PG-HPG nanoemulsion lubricant eye drop over long-term use (more than 28 days) can be considered for future studies.
Conclusion
The findings of the present real-world clinical study demonstrated that the PG-HPG nanoemulsion lubricant eye drop significantly and quickly improved multiple dry eye symptoms in subjects with DED, over a period of 28 days. No new safety concerns were identified in the study.
References
Dry eye redefined: TFOS DEWS II report; 2017; 1-6. https://www.tfosdewsreport.org. Accessed 18 Feb 2022.
Pucker AD, Ng SM, Nichols JJ. Over the counter (OTC) artificial tear drops for dry eye syndrome. Cochrane Database Syst Rev. 2016;2(2):CD009729.
Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II report executive summary. Ocul Surf. 2017;15(4):802–12.
Friedman NJ. Impact of dry eye disease and treatment on quality of life. Curr Opin Ophthalmol. 2010;21:310–6.
Uchino M, Schaumberg DA. Dry eye disease: impact on quality of life and vision. Curr Ophthalmol Rep. 2013;1:51–7.
Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15:334–65.
Farrand KF, Fridman M, Stillman IÖ, Schaumberg DA. Prevalence of diagnosed dry eye disease in the united states among adults aged 18 years and older. Am J Ophthalmol. 2017;182:90–8.
Courtin R, Pereira B, Naughton G, et al. Prevalence of dry eye disease in visual display terminal workers: a systematic review and meta-analysis. BMJ Open. 2016;6:6–13.
Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15:575–628.
Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017:276–83.
Srinivasan S, Manoj V. A decade of effective dry eye disease management with systane ultra (polyethylene glycol/propylene glycol with hydroxypropyl guar) lubricant eye drops. Clin Ophthalmol. 2021;15:2421–35.
Agarwal P, Craig JP, Rupenthal ID. Formulation considerations for the management of dry eye disease. Pharmaceutics. 2021;13:1–19.
Ramamoorthy P. White paper: an overview of the current consensus, clinical impact and management of dry eye. 2018. p. 6. https://alconscience.com/wp-content/uploads/2019/01/1811A23-US-SYS-18-E-2312_Dry-Eye-White-Paper_LR.pdf. Accessed 18 Feb 2022.
Yeh TN, Ketelson HA. White paper: Evolution of Systane artificial tears. 2020. https://us.alconscience.com/sites/g/files/rbvwei1736/files/pdf/Evolution-of-Systane®-Artificial-Tears-US-SYD-2000005.pdf. Accessed 18 Feb 2022.
Rangarajan R, Ketelson H. Preclinical evaluation of a new hydroxypropyl-guar phospholipid nanoemulsion-based artificial tear formulation in models of corneal epithelium. J Ocul Pharmacol Ther. 2019;35:32–7.
Rangarajan R, Ketelson H, Do R, et al. Characterization of a new phospholipid containing nanoemulsion lubricant eye drop for dry eye. Invest Ophthalmol Vis Sci. 2019;60:303–303.
Silverstein S, Yeu E, Tauber J, et al. Symptom relief following a single dose of propylene glycol-hydroxypropyl guar nanoemulsion in patients with dry eye disease: a phase IV, multicenter trial. Clin Ophthalmol. 2020;14:3167–77.
Yeu E, Silverstein S, Guillon M, et al. Efficacy and safety of phospholipid nanoemulsion-based ocular lubricant for the management of various subtypes of dry eye disease: a phase IV, multicenter trial. Clin Ophthalmol. 2020;14:2561–70.
Craig JP, Muntz A, Wang MTM, et al. Developing evidence-based guidance for the treatment of dry eye disease with artificial tear supplements: a six-month multicentre, double-masked randomised controlled trial. Ocul Surf. 2021;20:62–9.
Weisenberger K, Fogt N, Swingle FJ. Comparison of nanoemulsion and non-emollient artificial tears on tear lipid layer thickness and symptoms. J Optom. 2020;14:20–7.
Muntz A, Marasini S, Wang MTM, Craig JP. Prophylactic action of lipid and non-lipid tear supplements in adverse environmental conditions: a randomised crossover trial. Ocul Surf. 2020;18:920–5.
Systane Complete drug facts (nih.gov). https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=2df0de02-a3e2-471a-9e10-040c3fba75fe&type=display. Accessed 18 Feb 2022.
Aragona P, Giannaccare G, Mencucci R, Rubino P, Cantera E, Rolando M. Modern approach to the treatment of dry eye, a complex multifactorial disease: a P.I.C.A.S.S.O. board review. Br J Ophthalmol. 2021;105(4):446–53.
Golden MI, Meyer JJ, Patel BC. Dry eye syndrome. Treasure Island (FL): StatPearls; 2023.
Barabino S, Benitez-Del-Castillo JM, Fuchsluger T, et al. Dry eye disease treatment: the role of tear substitutes, their future, and an updated classification. Eur Rev Med Pharmacol Sci. 2020;24(17):8642–52.
Abetz L, Rajagopalan K, Mertzanis P, Begley C, Barnes R, Chalmers R. Development and validation of the impact of dry eye on everyday life (IDEEL) questionnaire, a patient-reported outcomes (PRO) measure for the assessment of the burden of dry eye on patients. Health Qual Life Outcomes. 2011;9:111. https://doi.org/10.1186/1477-7525-9-111.
Fairchild CJ, Chalmers RL, Begley CG. Clinically important difference in dry eye: change in IDEEL-symptom bother. Optom Vis Sci. 2008;85:29–34.
Chalmers RL, Begley CG, Caffery B. Validation of the 5-item dry eye questionnaire (DEQ-5): discrimination across self-assessed severity and aqueous tear deficient dry eye diagnoses. Contact Lens Anterior Eye. 2010;33:55–60.
Lemp CMA. Report of the National Eye Institute/Industry Workshop on Clinical Trials in Dry Eyes. Eye Contact Lens. 1995;21. https://pubmed.ncbi.nlm.nih.gov/8565190/. Accessed 18 Feb 2022.
Wesley G, Bickle K, Downing J, et al. Comparison of two thermal pulsation systems in the treatment of meibomian gland dysfunction: a randomized, multicenter study. Optom Vis Sci. 2022;99:323–32.
Acknowledgements
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contribution
Study concept, design, analysis and interpretation were performed by Deborah Awisi-Gyau. Data acquisition was performed by Katherine Bickle, Jason R. Miller and Joseph Tauber. The manuscript was critically reviewed for important intellectual content by all authors. All authors read and approved the final manuscript. All authors agree to be accountable for the accuracy and integrity of the work.
Funding
This study and the journal’s Rapid Service fee was funded by Alcon.
Medical Writing and Editorial Assistance
Writing, editorial, and formatting assistance was provided by Aru Singh, PhD, Sonali Dalwadi, PhD, and Sudha Korwar, PhD, from Indegene Pvt. Ltd. which was contracted and funded by Alcon. Alcon was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations. We acknowledge Dr. Jeffry Lane for participating as an independent clinical investigator in the study.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to varying rights of individuals and contractual rights of parties involved; Alcon does not make a practice of sharing datasets.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and Council for International Organizations of Medical Sciences (CIOMS) International Ethical Guidelines, International Council for Harmonization (ICH) GCP guidelines. The study protocol and informed consent form were reviewed and approved by the Institutional Review Board (IRB), Advarra IRB (Columbia, MD) before study commencement; and written informed consent was obtained from each subject before enrollment in the study.
Conflict of Interest
Katherine Bickle is independent clinical investigator conducting research for Alcon and Johnson and Johnson. Jason R. Miller and Joseph Tauber are independent clinical investigators conducting research for Alcon. Deborah Awisi-Gyau is employee of Alcon.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Bickle, K., Miller, J.R., Tauber, J. et al. Multi-symptom Relief with Propylene Glycol-Hydroxypropyl-Guar Nanoemulsion Lubricant Eye Drops in Subjects with Dry Eye Disease: A Post-Marketing Prospective Study. Ophthalmol Ther 13, 481–494 (2024). https://doi.org/10.1007/s40123-023-00853-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-023-00853-3