
Abstract
Introduction
This study aimed to determine the efficacy and safety of pars plana vitrectomy (PPV) as treatment for patients with primary symptomatic vitreous floaters.
Methods
We searched 12 databases for studies performing PPV for primary symptomatic vitreous floaters with at least 3 months follow-up. Two authors reviewed the studies and extracted data. Our main outcome of interest was patient satisfaction/reduction of symptoms/quality of life, but other measures of efficacy and safety were also extracted. Where possible, meta-analyses were performed to provide summary estimates.
Results
We identified 18 eligible studies, which included 2077 eyes of 1789 patients. Studies reported that at least 90% of the patients were satisfied or had relief of symptoms. Best corrected visual acuity improved − 0.08 logMAR (95% CI − 0.10 to − 0.06 logMAR, P < 0.0001). Contrast sensitivity improved − 2.26% (95% CI − 3.26 to − 1.26%, P < 0.0001). After surgery, cataract occurred in 31.7% (95% CI 21.7–42.7%), retinal tears/breaks in 2.92% (95% CI 1.38–4.97%), vitreous hemorrhage in 1.97% (95% CI 0.83–3.54%), macular edema in 1.70% (95% CI 0.84–2.83%), retinal detachment in 1.54% (95% CI 0.62–2.82%), glaucoma in 1.04% (95% CI 0.53–1.73%), and endophthalmitis in 0.18% (95% CI 0.02–0.45%).
Conclusions
Postoperative patient satisfaction is high after PPV for primary symptomatic vitreous floaters. However, the patient should be carefully counselled as what to expect from the treatment and understand the risks associated with PPV.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Vitreous opacities are a common phenomenon which affects 76% of the general population, although persisting bothersome vitreous opacities are much rarer. Pars plana vitrectomy can alleviate the symptoms. |
An overview of expected surgical outcomes with pars plana vitrectomy may allow better guidance of patients considering this as a treatment. |
What was learned from the study? |
More than 90% of the patients were satisfied. On average, visual acuity and contrast sensitivity improved significantly. |
After surgery, cataract can be expected to occur in approximately 1 in 3; retinal tears/breaks, vitreous hemorrhage, and macular edema are seen in 2–3%; retinal detachment and glaucoma in 1–1.5%; and endophthalmitis in 0.1–0.2%. |
Introduction
Vitreous opacities are a common visual complaint affecting 76% of the general population [1]. It often occurs as primary vitreous floaters or posterior vitreous detachment (PVD). Primary vitreous floaters are defined as those arising from structures endogenous to the vitreous and they are often a consequence of PVD, myopic vitreopathy, and age-related degenerative changes in the vitreous, which are in contrast to secondary floaters, e.g., hemorrhage, inflammation, or asteroid bodies [2]. These vitreous floaters can have acute presentation such as that seen after PVD or more insidious, e.g., degenerative changes, inflammation, or asteroid hyalosis. After onset of PVD, most individuals become asymptomatic within few months. Asteroid hyalosis, although relatively prevalent (3% of individuals above 80 years of age), also rarely leads to persisting symptoms and visual discomfort which necessitate treatment [3, 4].
Persisting symptomatic vitreous floaters lead to an impairment of quality of life (QOL). Kim et al. used questionnaires and found that severity of floater symptoms correlated with level of depression, perceived stress, and state and trait anxiety [5]. The impact of floaters on QOL was comparable to that of age-related macular degeneration and diabetic retinopathy, and upon investigation patients were willing to accept a 7% risk of blindness to eliminate floater symptoms [6].
Pars plana vitrectomy (PPV) is a surgical solution to cases with persisting symptomatic vitreous floaters [7]. In a survey among vitreoretinal surgeons, Cohen et al. reported that the decision of PPV was influenced by whether the surgeon previously had performed PPV for symptomatic floaters, the risks associated with PPV, the fear of unreasonable patient expectations, and the possibility of ridicule within the local retina community [8]. These challenges can be better dealt with if we have clear knowledge of what to expect in terms of efficacy and safety of PPV for symptomatic floaters.
Therefore, the aim of this systematic review with meta-analyses is to outline the evidence on the efficacy and safety of PPV for primary symptomatic floaters.
Methods
Study Design
This systematic review was designed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [9]. We followed the recommendations of the Cochrane Handbook [10]. No institutional review board approval is required for systematic reviews according to Danish law. This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments.
Eligibility Criteria
We deemed study populations eligible if they included adult (18+ years of age) human patients with primary symptomatic floater symptoms for at least 3 months and if these cases underwent PPV. We did not restrict eligibility of studies based on lens status (i.e., phakic or pseudophakic), type of vitrectomy (i.e., complete, incomplete, or core), gauge, cutting speed, additional internal limiting membrane (ILM) peeling, or whether a combined phacovitrectomy had been performed.
We used predefined outcomes of efficacy and safety. Efficacy was measured as patient satisfaction/reduction of symptoms/QOL, best corrected visual acuity (BCVA), contrast sensitivity, any method of evaluation using quantitative ultrasonography, dynamic light scattering, optical coherence tomography, or scanning laser ophthalmoscopy. Safety measures were incident ocular hypertension (OHT), hypotony, vitreous hemorrhage, retinal tears/breaks, retinal detachment, endophthalmitis, glaucoma, macular edema, and cataract. Without further restrictions, we included studies of eligible populations with outcome measures of at least 3 months after surgery. We included relevant abstracts of studies with original data not disseminated as full papers elsewhere, but not studies without original data or case reports. We did not restrict studies on the basis of geography or journal, but only considered studies written in English.
Information Sources and Search Strategy
We searched the literature databases the Cochrane Central, PubMed/MEDLINE, EMBASE, Web of Science Core Collection, BIOSIS Previews, Current Contents Connect, Data Citation Index, Derwent Innovations Index, KCI-Korean Journal Database, Russian Science Citation Index, SciELO Citation Index, and ClinicalTrials.gov. Literature searches were performed using search phrases specifically tailored the individual databases by a trained individual (YS). All database searches were conducted on September 26, 2021. Details of database searches are available as electronic Supplementary Material 1.
Study Selection, Data Collection, and Risk of Bias Within Study Assessment
Two authors (DDD and SFK) examined titles and abstracts from the literature search to remove any obviously irrelevant records and duplicates. The same authors then independently examined the full text of all the remaining records for potential eligibility and reviewed reference lists from these studies for any additional potentially relevant studies. Consensus was then attempted between the two authors, and cases of disagreement were discussed with a third author (YS) to reach a final decision.
Data regarding study design, characteristics, methods, and results were extracted from all eligible studies using extraction forms. Studies were assessed using the Newcastle–Ottawa Assessment Scale for Cohort Studies, which is the recommended assessment tool for cohort studies [11]. The data extraction and the risk of bias within each study were performed independently by two authors (DDD and SFK). Consensus was then attempted between the two authors, and cases of disagreement was discussed with a third author (YS) to reach a final decision.
Outcome Measures, Data Analysis, and Synthesis
The primary outcome of interest was patient satisfaction. We anticipated that this outcome would be difficult to assess in a quantitative analysis, as it is often defined and measured with different methods. Secondary outcomes of interest were other aspects of efficacy (measured as BCVA, contrast sensitivity, and any method of evaluation using quantitative ultrasonography, dynamic light scattering, optical coherence tomography, or scanning laser ophthalmoscopy) and safety (measured as OHT, hypotony, vitreous hemorrhage, retinal tears/breaks, retinal detachment, endophthalmitis, glaucoma, macular edema, and cataract). All outcomes were extracted for short-term and long-term results defined as the results reported at follow-up closest to 3 months and at follow-up closest to 1 year, respectively. However, upon analyzing the results, we realized that data was not disseminated in such a detailed fashion that would allow us to distinguish between short-term and long-term outcomes. Hence, we consider outcomes at follow-up of at least 3 months after surgery.
All eligible studies were reviewed qualitatively in text and tables. Meta-analyses, where possible, were performed using MetaXL 5.3 (EpiGear International, Sunrise Beach, QLD, Australia). We used the random-effects model in our analyses to account for potential heterogeneity across studies. Heterogeneity was assessed using Cochran’s Q and quantified with I2 [12]. Funnel plots were used to evaluate risk of bias across studies [13]. Final results were the pooled estimates of weighted mean differences (continuous outcomes) and prevalence (categorical outcomes). For continuous outcomes, we realized that several studies did not report standard deviation (SD) of outcomes. In these cases, we followed the recommendation by the Cochrane Handbook and estimated the SDs based on averaged data from other studies using similar methods of measurement [10]. Several studies only reported data from before surgery and follow-up after surgery, but not data for change. In such cases, we calculated the mean by simple subtraction and calculated the SD of the change (SDchange) using the following formula:
where SDbaseline and SDfollowup are respectively the SDs from before surgery and follow-up after surgery and C is the correlation coefficient (ranging between − 1 and + 1), which describes how similar the measures were before surgery and follow-up after surgery [10]. It was possible to estimate the correlation coefficients based on data reported in a subset of the eligible studies. For categorical outcomes, caution must be exercised in prevalence meta-analyses because of variance instability, when prevalence reaches the extremes (0% or 100%) because results of individual studies obtain erroneous weights [14]. Prevalence numbers were therefore transformed using the double arcsine method for analysis and then back-transformed for interpretation. For all meta-analyses, sensitivity analyses were performed to evaluate the robustness of the estimates. P values below 0.05 were considered statistically significant. For prevalence estimates of complications, we also used the qualitative descriptors of frequencies as used by the European Medicines Agency: very rare, less than 0.01%; rare, 0.01–0.1%; uncommon, 0.1–1%; common, 1–10%; and very common, greater than 10%.
Results
Study Selection
The literature database search identified 1004 records, of which 575 remained after removing duplicates. From these, obviously irrelevant records were removed, and 48 records were retrieved in full-text for further evaluation. After consensus was reached, 18 studies in total were found eligible for the qualitative and the quantitative review. Figure 1 outlines the details of the study selection process.

PRISMA flow diagram of the study selection process
Study Characteristics and Risk of Bias Within Studies
The 18 eligible studies summarized data on a total of 2077 eyes of 1789 patients with symptomatic vitreous floaters who underwent PPV (Table 1) [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. Of these eyes, 1089 were phakic, 862 were pseudophakic, and the baseline lens status was unclear for the remaining 126 eyes. Six studies were prospective, and 12 were retrospective. Study populations were from North America (n = 11), Europe (n = 5), Asia (n = 1), and South America (n = 1). Mean age of patients ranged between 52 and 69 years, and the gender distribution was overall well balanced between men and women. Study characteristics are summarized in detail in Table 1.
Overall, 1320 eyes underwent limited vitrectomy, where retrolental vitreous was kept intact, possibly protecting against cataract formation. Another 385 eyes received extensive vitrectomy. Finally, no data were available on the type of vitrectomy for the remaining 372 eyes. The gauge size used was 20G (7.9%), 23G (21.7%), 25G (57.5%), 27G (1.2%), or unknown (11.7%). PVD was induced in 27.4%, and not induced in 27.2%; 24.6% had pre-existing PVD, and no information on PVD status was presented for 20.8% of eyes. Further details are summarized in Table 2.
Our evaluation of the risk of bias within studies using the Newcastle–Ottawa Quality Assessment Scale for Cohort Studies found an overall high study quality, although it was a concern that none of the studies included non-operated individuals. The vast majority (n = 15) received an overall quality score of six or above, whereas the remaining three obtained a score of five (n = 2) or four (n = 1). Risk of bias evaluation within studies is summarized in Table 3.
Results of Individual Studies for Patient Satisfaction and Vision-Related QOL
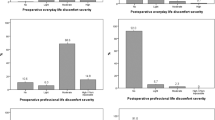
Studies reported on various overlapping aspects of patient satisfaction, resolution of symptoms, and vision-related QOL. Clerici et al. reported that after PPV, 88% reported low level or complete absence of nuisance, and that 94% were overall satisfied or very satisfied with the surgery [15]. De Nie et al. reported that after vitrectomy, 84% were never troubled by floaters and 9% were troubled for less time, and that the patients experienced less difficulties in reading, using computers, watching TV, and driving [16]. Furthermore, the PPV led to 85% of patients being satisfied or very satisfied with the results, and among those who were dissatisfied the majority were those with a complication from the surgery (retinal detachment, refractory cystoid macular edema, glaucoma requiring further surgery, and foveal photoreceptor atrophy) that resulted in significant vision loss [16]. Hahn et al. reported a median overall self-rated impairment index of 44% before surgery, which significantly reduced to 11% at 12 months after PPV [17]. Lam et al. found that core vitrectomy combined with phacoemulsification surgery with intraocular lens (IOL) implantation led to 94% of patients being satisfied or very satisfied with limited number of complications [18]. Mason III et al. reported that after PPV, 92% reported no or extremely mild symptoms, and that 96% were satisfied with the results and 94% claimed the experiences to be a complete success [19]. Mylvaganam et al. found that patients with multifocal or accommodative IOL had a shorter duration of floater onset to PPV than for patients with phakia or patients with monofocal IOL [20]. Navarro et al. investigated outcomes after PPV for symptomatic posterior vitreous detachment that persisted after phacoemulsification and implantation of multifocal IOL [21]. All patients reported improvement of halos, glare, and floaters; no complications were reported, and the authors found a statistically significant improvement on the National Eye Institute Visual Function Questionnaire (NEI-VFQ) with 25 items and specifically on the subsets general vision, near activities, distance activities, mental health, role difficulties, and driving [21]. Rostami et al. (2018) evaluated outcomes after limited PPV using the NEI-VFQ 25-items and estimated a 13.5% QOL improvement [22]. Rostami et al. reported that limited PPV led to a statistically significant increase in NEI-VFQ 39-items [23]. Sebag et al. reported NEI-VFQ 39-items on a subset of their study group and found statistically significant improvements after PPV in the composite score and specifically in the subsets of general vision, near vision, and driving [24]. Sebag et al. found that NEI-VFQ 39-items in patients with symptomatic floaters were statistically significantly lower when compared to age-matched control subjects, and that PPV led to normalization of the NEI-VFQ composite score [25]. Sebag et al. reported that limited PPV led to statistically significant improvement in NEI-VFQ 39-items in the composite score and specifically in the subsets of general vision and near vision [26]. Starr et al. reported that 90% of the patients reported improvements after the PPV [27]. Wa et al. reported that symptoms resolved in 98.5% of eyes after the PPV [28]. Waseem et al. reported that all patients had improvements after PPV in terms of measured activities of daily living [29]. In the European VitreoRetinal Society (EVRS) Floaters study report, Zeydanli et al. reported in a large multicenter study that after the PPV, 92% were satisfied or extremely satisfied, 6% were neutral, and 2% were dissatisfied [32]. Furthermore, discomfort in everyday life, in professional life, and psychological life statistically significantly improved for the vast majority (greater than 95%) of the patients after the surgery [32]. Mylvaganam et al. and Yee et al. did not report patient satisfaction or vision-related QOL data [20, 30, 31].
In summary, across studies we found a consistent trend of patient satisfaction and improvement of the vision-related QOL.
Quantitative Analysis of Secondary Outcomes: Efficacy Beyond Patient Satisfaction and Vision-Related QOL
Change in BCVA after PPV was calculated from data provided in eight studies of 712 eyes. The meta-analysis of change in BCVA led to a summary estimate of logMAR − 0.08 (95% CI − 0.10 to − 0.06, P < 0.0001) (Fig. 2a), i.e., an improvement of vision almost equivalent to a line in the logMAR scale. Heterogeneity statistics (I2 = 0; Cochran’s Q = 1) showed minimal heterogeneity. Funnel plot did not show skewed results and the sensitivity analysis showed robustness (estimate ranged between − 0.07 and − 0.06, all statistically significant) (see electronic Supplementary Material 2). These numbers show a statistically significant improvement of the BCVA after PPV.

Results of the meta-analyses on efficacy and safety aspects of pars plana vitrectomy for symptomatic floaters. a Change in best-corrected visual acuity (BCVA) from before surgery to at least 3 months after surgery as measured in logarithm of the minimum angle of resolution (logMAR). b Change in contrast sensitivity from before surgery to at least 3 months after surgery as measured in Weber index. c Summary estimates of all the prevalence meta-analyses on the prevalence of postoperative complications are listed together with the qualitative descriptors of frequencies as used by the European Medicines Agency
Change in contrast sensitivity after PPV was calculated from data provided in four studies of 407 eyes. The meta-analysis of change in contrast sensitivity led to a summary estimate of − 2.26% on the Weber index (95% CI − 3.26 to − 1.26, P < 0.0001) (Fig. 2b). Heterogeneity statistics (I2 = 0; Cochran’s Q = 0) showed minimal heterogeneity. Funnel plot did not show skewed results and the sensitivity analysis showed robustness (estimate ranged between − 2.34% and − 2.13%, all statistically significant) (see electronic Supplementary Material 3). These numbers show a statistically significant improvement of the contrast sensitivity after PPV.
Sebag et al. was the only study to measure vitreous echodensity with quantitative ultrasonography before and after PPV [26]. The authors reported a 94.1% decrease from 7.37 arbitrary units (AU) to 0.44 AU [26]. No studies reported quantitative efficacy measures for dynamic light scattering, ocular coherence tomography, or scanning laser ophthalmoscopy.
Quantitative Analysis of Secondary Outcomes: Safety
Definitions of postoperative OHT and hypotony were defined differently across studies, hence pooling these heterogeneously defined outcomes would make little sense. Clerici et al. reported one asymptomatic event of OHT (30 mmHg) and one event of hypotony (6 mmHg) [15]. De Nie et al. reported that 25 of 110 cases experienced a postoperative intraocular pressure greater than 25 mmHg, of which eight spontaneously normalized, 16 required pressure-lowering treatment, and one developed glaucoma [16]. Lam et al. experienced that one of 50 cases developed transient hypotony, which required patching one extra day [18]. In Rostami et al., none of the 42 patients experienced either OHT or hypotony [23]. Zeydanli et al. reported that 13 of 581 cases developed OHT, of which four were with transient symptoms and nine developed glaucoma; and that one of 581 cases became chronically hypotonic [32].
Data on cataract after surgery was provided in 16 studies of 954 eyes with a calculated summary prevalence estimate of 31.7% (95% CI 21.7–42.7%). Heterogeneity statistics (I2 = 92; Cochran’s Q = 179) showed substantial heterogeneity, funnel plot did not show skewed results, and the sensitivity analysis showed robustness (estimate ranged between 30.2% and 35.2%) (see electronic Supplementary Material 4).
Data on retinal tears/breaks after surgery was provided in 12 studies of 1660 eyes with a calculated summary prevalence estimate of 2.92% (95% CI 1.38–4.97%). Heterogeneity statistics (I2 = 74; Cochran’s Q = 42) showed substantial heterogeneity, funnel plot did not show skewed results, and the sensitivity analysis showed robustness (estimate ranged between 2.46% and 3.27%) (see Electronic Supplementary Material 5).
Data on vitreous hemorrhage after surgery was provided in 13 studies of 1573 eyes with a calculated summary prevalence estimate of 1.97% (95% CI 0.83–3.54%). Heterogeneity statistics (I2 = 66; Cochran’s Q = 35) showed substantial heterogeneity, funnel plot did not show skewed results, and the sensitivity analysis showed robustness (estimate ranged between 1.22% and 2.22%) (see Electronic Supplementary Material 6).
Data on macular edema after surgery was provided in nine studies of 1313 eyes with a calculated summary prevalence estimate of 1.70% (95% CI 0.84–2.83%). Heterogeneity statistics (I2 = 32; Cochran’s Q = 12) showed moderate heterogeneity, funnel plot did not show skewed results, and the sensitivity analysis showed robustness (estimate ranged between 1.41% and 1.81%) (see Electronic Supplementary Material 7).
Data on retinal detachment after surgery was provided in 14 studies of 1723 eyes with a calculated summary prevalence estimate of 1.54% (95% CI 0.62–2.82%). Heterogeneity statistics (I2 = 62; Cochran’s Q = 32) showed substantial heterogeneity, funnel plot did not show skewed results, and the sensitivity analysis showed robustness (estimate ranged between 1.29% and 1.80%) (see Electronic Supplementary Material 8).
Data on glaucoma after surgery was provided in seven studies of 1148 eyes with a calculated summary prevalence estimate of 1.04% (95% CI 0.53–1.73%). Heterogeneity statistics (I2 = 0; Cochran’s Q = 4) showed minimal heterogeneity, funnel plot did not show skewed results, and the sensitivity analysis showed robustness (estimate ranged between 0.56% and 1.10%) (see Electronic Supplementary Material 9).
Data on endophthalmitis after surgery was provided in 13 studies of 1730 eyes with a calculated summary prevalence estimate of 0.18% (95% CI 0.02–0.45%). Heterogeneity statistics (I2 = 0; Cochran’s Q = 4) showed minimal heterogeneity, funnel plot did not show skewed results, and the sensitivity analysis showed robustness (estimate ranged between 0.13% and 0.19%) (see Electronic Supplementary Material 10).
The overall safety profile with all these calculated summary estimates is summarized in Fig. 2c.
Discussion
In this systematic review with meta-analyses, we present the evidence of the efficacy and safety of PPV for symptomatic primary vitreous floaters, as based on 18 studies including 2077 eyes of 1789 patients. The vast majority of patients were either satisfied or very satisfied after surgery, although up to 8.5% reported some extent of dissatisfaction. Contrast sensitivity improved significantly. Patients had statistically significant but moderate increments in BCVA, which may reflect that the baseline BCVA was high preoperatively and therefore there is only limited measurable improvement because of a ceiling effect. For a balanced patient counseling, safety aspects should also be presented in a balanced manner (Fig. 2c). According to the European Medicines Agency descriptors, cataract is very common and will occur in every third case, depending on the extension of vitrectomy [30, 31] and the use of gas bubble [33]; retinal tears/breaks, vitreous hemorrhage, and macular edema are common at 2–3%; retinal detachment and glaucoma can be considered uncommon at 1–1.5%; and endophthalmitis is rare at approximately 0.1–0.2%.
On the basis of data from the Intelligent Research in Sight Registry, Rubino et al. evaluated the rate of further surgeries 1 year after PPV for vitreous floaters [34]. This study found that surgery other than cataract extraction was performed in 3.7%, and that retinal detachment surgery was performed in 2.6%. These numbers validate to a certain extent the results of our meta-analyses.
Different time intervals from vitrectomy to measurements of postoperative outcomes in the reviewed studies meant that we did not have sufficient data to perform meta-analysis for each outcome at 3 months and 12 months. Even fewer studies provide insight into outcomes after many years. Future studies need to map long-term outcomes more extensively to better counsel patients in what can be expected.
YAG laser vitreolysis is another potential treatment modality, which is an emerging topic with limited published literature available, only two small randomized clinical studies without any PPV comparison groups and short follow-up periods [35, 36]. Future, larger YAG laser vitreolysis studies with a PPV comparison group may allow better comparison across the different treatment modalities.
Limitations of this study should be acknowledged when interpreting the results. First, we can only extrapolate the results of patients with symptomatic floaters. For patients with asymptomatic floaters, treatment should not be encouraged in any circumstances considering the safety profile of the PPV. Second, pooling of results from studies of PPV with difference in gauge size, different PPV quality (extensive, core, and limited), and PPV with or without combined phacoemulsification introduces a certain bias and reduces generalizability of results for a more specific type of surgery or patient group. In particular, limited PPV may provide significantly lower incidence of postoperative cataract formation as demonstrated by Yee et al. [30, 31]. Pooling data from PPV with different gauge size, in particular inclusion of data using the older 20G, may not provide data fully representative of modern surgical practice. Finally, the results of our review are only as good as the studies included. Most studies were retrospective in nature, which introduces selection bias as no-participation bias or loss to follow-up. For example, one can speculate that patients who are lost to follow-up are those more likely to be satisfied and see no reason to turn up for a control, which in turn would lead to a skewed result towards more negative outcomes. Another important design aspect of the included studies is the lack of a non-vitrectomized matched control group that does not allow us to speculate on how the patients would fare without surgery. Also, some studies were only reported as conference abstracts, which made it difficult to assess risk of bias and obtain more detailed data and information regarding study results. Uncertainties from these conference abstracts should also be considered as a limitation.
Conclusion
This systematic review with meta-analyses summarized current evidence of PPV for primary symptomatic vitreous floaters in terms of efficacy and safety. We find that the vast majority of patients are satisfied with the result. There is an improvement of BCVA and contrast sensitivity. Cataract formation is the most common complication in patients with phakia, but is a mild complication with an excellent surgical treatment option with a low risk of postoperative complications. Risks of more serious complications are low but not entirely negligible, which necessitates that the patient should be prepared and aware of the risk profile prior to commencing PPV treatment.
References
Webb BF, Webb JR, Schroeder MC, North CS. Prevalence of vitreous floaters in a community sample of smartphone users. Int J Ophthalmol. 2013;6:402–5.
Coupland SE. The pathologist’s perspective on vitreous opacities. Eye. 2008;22:1318–29.
Møller-Lorentzen TB, Eckmann-Hansen C, Faber C, Larsen M, Subhi Y. Global prevalence of asteroid hyalosis and projection of its future burden: a systematic review and meta-analysis. Acta Ophthalmol. 2020;98:755–62.
Scott DAR, Møller-Lorentzen TB, Faber C, Wied J, Grauslund J, Subhi Y. Spotlight on asteroid hyalosis: a clinical perspective. Clin Ophthalmol. 2021;15:2537–44.
Kim YK, Moon SY, Yim KM, Seong SJ, Hwang JY, Park SP. Psychological distress in patients with symptomatic vitreous floaters. J Ophthalmol. 2017;2017:3191576.
Wagle AM, Lim WY, Yap TP, Neelam K, Au Eong KG. Utility values associated with vitreous floaters. Am J Ophthalmol. 2011;152:60–5.
Ryan EH. Current treatment strategies for symptomatic vitreous opacities. Curr Opin Ophthalmol. 2021;32:198–202.
Cohen MN, Rahimy E, Ho AC, Garg SJ. Management of symptomatic floaters: current attitudes, beliefs, and practices among vitreoretinal surgeons. Ophthalmic Surg Lasers Imaging Retina. 2015;46:859–65.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
Higgins J, Thomas J, Chandler J, et al., editors. Cochrane handbook for systematic reviews of interventions version 6.0 (updated February 2021). Cochrane 2021. www.training.cochrane.org/handbook. Accessed 25 Aug 2021.
Zeng X, Zhang Y, Kwong JS, et al. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic review. J Evid Based Med. 2015;8:2–10.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Barendregt JJ, Doi SA, Lee YY, Norman RE, Vos T. Meta-analysis of prevalence. J Epidemiol Community Health. 2013;67:974–8.
Clerici M, Galli A, Gibin E, et al. Small gauge vitrectomy for symptomatic floaters: safety, efficacy and patient’s satisfaction. Invest Ophthalmol Vis Sci. 2016;57:4480.
de Nie KF, Crama N, Tilanus MAD, Klevering BJ, Boon CJF. Pars plana vitrectomy for disturbing primary vitreous floaters: clinical outcome and patient satisfaction. Graefes Arch Clin Exp Ophthalmol. 2013;251:1373–82.
Hahn U, Krummenauer F, Ludwig K. 23G pars plana vitrectomy for vitreal floaters: prospective assessment of subjective self-reported visual impairment and surgery-related risks during the course of treatment. Graefes Arch Clin Exp Ophthalmol. 2018;256:1089–99.
Lam DS, Leung HY, Liu S, Radke N, Yuan Y, Lee VY. Two-port pars plana anterior and central core vitrectomy (Lam floaterectomy) in combination with phacoemulsification and intraocular lens implantation under topical anesthesia for patients with cataract and significant floaters: results of the first 50 consecutive cases. Asia Pac J Ophthalmol (Phila). 2017;6:33–6.
Mason JO III, Neimkin MG, Mason JO IV, et al. Safety, efficacy, and quality of life following sutureless vitrectomy for symptomatic vitreous floaters. Retina. 2014;34:1055–61.
Mylvaganam H, Osher JM, Lai MM. Vitrectomy for symptomatic vitreous floaters: characteristics of intraocular lens status and patient selection, a retrospective observational study. Invest Ophthalmol Vis Sci. 2017;58:2807.
Navarro RM, Machado LM, Maia O Jr, et al. Small-gauge pars plana vitrectomy for the management of symptomatic posterior vitreous detachment after phacoemulsification and multifocal intraocular lens implantation: a pilot study from the Pan–American collaborative retina study group. J Ophthalmol. 2015;2015:156910.
Rostami B, Nguyen-Cuu J, Brown G, Brown M, Sadun AA, Sebag J. Cost-effectiveness of limited vitrectomy for vision degrading vitreopathy. Invest Ophthalmol Vis Sci. 2018;59:5217.
Rostami B, Nguyen-Cuu G, Brown G, Brown M, Sadun AA, Sebag J. Cost-effectiveness of limited vitrectomy for vision-degrading myodesopsia. Am J Ophthalmol. 2019;204:1–6.
Sebag J, Yee KM, Wa CA, Huang LC, Sadun AA. Vitrectomy for floaters: prospective efficacy analyses and retrospective safety profile. Retina. 2014;34:1062–8.
Sebag J, Yee KMP, Huang LC, Wa C, Sadun AA. Vitrectomy for floaters: prospective efficacy analysis and retrospective safety profile. Trans Am Ophthalmol Soc. 2013;111:16.
Sebag J, Yee KMP, Nguyen JH, Nguyen-Cuu J. Long-term safety and efficacy of limited vitrectomy for vision degrading vitreopathy resulting from vitreous floaters. Ophthalmol Retina. 2018;2:881–7.
Starr M, Chod R, Akduman L. Analyzing the safety and efficacy of pars plana vitrectomy for symptomatic vitreous floaters. Invest Ophthalmol Vis Sci. 2015;56:5099.
Wa C, Yee K, Huang L, Sadun A, Sebag J. Long-term safety of vitrectomy for patients with floaters. Invest Ophthalmol Vis Sci. 2013;54:2142.
Waseem T, DaBreo E, Jiang D, Clawson R, Wagner A, Kapoor K. Pars plana vitrectomy for symptomatic vitreous floaters: another look. Invest Ophthalmol Vis Sci. 2019;60:5784.
Yee KM, Wa CA, Nguyen JH, et al. Reducing post-vitrectomy cataracts. Invest Ophthalmol Vis Sci. 2014;55:2205.
Yee KMP, Tan S, Lesnik Oberstein SY, et al. Incidence of cataract surgery after vitrectomy for vitreous opacities. Ophthalmol Retina. 2016;1:154–7.
Zeydanli EO, Parolini B, Ozdek S, et al. Management of vitreous floaters: an international survey the European VitreoRetinal Society Floaters study report. Eye (Lond). 2020;34:825–34.
Thompson JT. The role of patient age and intraocular gas use in cataract progression after vitrectomy for macular holes and epiretinal membranes. Am J Ophthalmol. 2004;137:250–7.
Rubino SM, Parke DW 3rd, Lum F. Return to the operating room after vitrectomy for vitreous opacities: intelligent research in sight registry analysis. Ophthalmol Retina. 2021;5(1):4–8. https://doi.org/10.1016/j.oret.2020.07.015.
Ludwig GD, Gemelli H, Nunes GM, Serracarbassa PD, Zanotele M. Efficacy and safety of Nd:YAG laser vitreolysis for symptomatic vitreous floaters: a randomized controlled trial. Eur J Ophthalmol. 2021;31:909–14.
Shah CP, Heier JS. YAG laser vitreolysis vs Sham YAG vitreolysis for symptomatic vitreous floaters: a randomized clinical trial. JAMA Ophthalmol. 2017;135:918–23.
Acknowledgements
Funding
No funding or sponsorship was received for this study or publication of this article.
Author Contributions
All authors contributed to the study conception and design. Study selection, data extraction, and data analysis were performed by David Damgaard Dysager, Sigve Flægstad Koren, and Yousif Subhi. The draft of the manuscript was written by David Damgaard Dysager and Sigve Flægstad Koren, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Disclosures
David Damgaard Dysager, Sigve Flægstad Koren, Jakob Grauslund, Jimmi Wied, and Yousif Subhi declare that they have no competing interests.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors. This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Dysager, D.D., Koren, S.F., Grauslund, J. et al. Efficacy and Safety of Pars Plana Vitrectomy for Primary Symptomatic Floaters: A Systematic Review with Meta-Analyses. Ophthalmol Ther 11, 2225–2242 (2022). https://doi.org/10.1007/s40123-022-00578-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-022-00578-9