
Abstract
Intraocular pressure (IOP) reduction by medications, laser, or surgery remains the mainstay of treatment in glaucoma. However, the role of complementary and alternative medicine (CAM) in glaucoma has received great interest from both patients and ophthalmologists. Previous evidence suggests that diet, a major domain of CAM, can influence an individual’s IOP level. Furthermore, certain dietary components have been linked to the incidence and progression of glaucoma. In this review, we aim to provide a summary of the current evidence regarding the role of obesity, certain dietary components, and dietary supplements in glaucoma.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Glaucoma is a major cause of irreversible blindness worldwide. Globally, it is estimated that 5.7 million people are visually impaired as a result of glaucoma [1]. Increased intraocular pressure (IOP) is the most significant risk factor in glaucoma [2]; however, recent research on the pathogenesis of glaucoma suggests that non-IOP-dependent mechanisms also play a role. Vascular dysregulation [3], oxidative stress [4], autoimmunity [5], and excitotoxicity [6] are all mechanisms that can explain why glaucomatous optic neuropathy may occur despite normal IOP.
IOP reduction is currently the mainstay of glaucoma treatment. It has been shown that IOP reduction significantly delays glaucoma progression by means of optic disc damage and visual field loss [7]. This is usually achieved by anti-glaucoma medications, laser therapy, or surgical intervention. Recently, a considerable amount of glaucoma research has been directed towards therapeutic approaches targeting non-IOP-dependent mechanisms. The effect of novel therapeutic agents [8,9,10] and complementary medications [11,12,13] targeting such pathways is a subject of attention.
The use of complementary and alternative medicine (CAM), targeting both IOP-dependent and non-IOP-dependent mechanisms, in glaucoma has received interest from some ophthalmologists [14] and glaucoma patients [15]. A report from Canada showed that one in every nine patients with glaucoma uses CAM in the treatment of his condition [16]. This encompasses a wide range of CAM categories, e.g. herbs, dietary interventions, exercise, and body-based practices.
A major domain of CAM in glaucoma is the utilization of dietary interventions. A considerable amount of research suggests that an individual’s diet may have an effect on IOP [17], the incidence of glaucoma [18], and progression of the disease [19]. Furthermore, glaucoma patients commonly inquire about what to eat and drink in order to help in the treatment of their disease, and whether or not their dietary habits will affect the progression of their condition. Although it seems simple, an answer to such question is yet to be determined by ongoing research in this arena.
The objective of this review was to provide a summary of the current evidence regarding the effect of obesity and diet on IOP, incidence, and progression of glaucoma. The review outlines three major elements pertinent to diet: obesity and energy intake, individual dietary components, and dietary supplements.
Methods
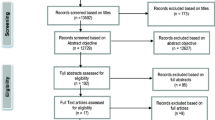
A literature review using the advanced search builder on PubMed was made in December 2017. The following search technique was implemented; “glaucoma” or “IOP” along with all of the following keywords: diet, nutrition, obesity, body mass index, alcohol, coffee, caffeine, tea, Ginkgo biloba extract, fruits, vegetables, chocolate, saffron, dietary supplements, and antioxidants. Search results were evaluated for relevance to our current review. Additional studies were added by manually reviewing bibliographies of articles obtained during the initial search. Results were limited to studies written in English, and published during the period from 1966 to 2017. In order to maintain clinical relevance, the main focus was on epidemiological and clinical studies conducted on human subjects.
This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Obesity and Energy Intake
Body mass index (BMI), a major anthropometric indicator of obesity, has been linked to elevated IOP in many cross-sectional [20,21,22] and longitudinal [23,24,25] studies on healthy subjects. The exact pathophysiology of elevated IOP in obesity remains unclear. Possible mechanisms that can explain such association include: obesity-related oxidative stress [26] leading to trabecular meshwork malfunctioning [27], increased orbital fat impeding aqueous outflow [28], and dysregulation of retrobulbar blood flow [29].
Interestingly, epidemiological studies looking at the relationship between BMI and primary open-angle glaucoma (POAG) have yielded inconsistent results [30,31,32,33,34,35]. The Gangnam Eye Study [30] found a positive association between BMI and the incidence of POAG, while others reported a negative association [33,34,35]. Furthermore, after adjustment for possible confounding variables, some studies did not find any association [31, 32]. A possible explanation of such difference is the presence of a racial variation between the studied populations.
Although BMI is a commonly used indicator of obesity, it has some limitations. A major drawback is that it does not differentiate between fat and muscle, such that it does not reflect the actual amount of fat tissue. In an attempt to overcome this, some studies have looked into the influence of other obesity markers on IOP [20, 36, 37]. The Korea National Health and Nutrition Examination Survey [36] found a positive linear relationship between different obesity markers (i.e. waist circumference, total body fat mass, and fat percentage) and IOP. Other reports have also found similar results on variable markers [20, 37].
In addition to obesity, other components of metabolic syndrome (MetS) have also been linked to elevated IOP and glaucoma. In a retrospective review of 12,747 subjects, Wygnanski-Jaffe et al. [38] found that MetS was more prevalent in subjects with high IOP. Moreover, other reports have found that the IOP rises linearly as the number of MetS components increases [39]. Newman-Casey et al. [40] looked at the association between POAG development and various components of MetS in a large cohort of patients. They found that those with diabetes mellitus (DM) or hypertension (HTN), alone or combined, had an increased risk of developing POAG. On the other hand, hyperlipidemia was found to decrease the risk of POAG, and reduce the effect of DM and HTN if it occurs with any of them.
Individual Dietary Components
Alcohol
It has been shown that alcohol lowers IOP following acute ingestion in both glaucoma patients and healthy subjects [41, 42]. The exact mechanism leading to such finding is poorly understood; however, it is thought to be secondary to variable physiological changes such as a hyperosmotic effect exerted by alcohol, reduction of net water movement into the eye through vasopressin suppression [43], and inhibition of secretory cells in the ciliary processes [44]. Moreover, alcohol was shown to increase blood flow to the optic nerve head, a mechanism that is thought to offer a protective effect against the development of POAG [45].
With this in mind, various epidemiological studies were conducted to investigate the relation between alcohol consumption and glaucoma. Contrary to what is expected, the majority of those studies did not report any association [33, 46,47,48]. On the other hand, data from the Framingham Eye Study [49] suggests that there is a positive association between high alcohol consumption and glaucoma. Finally, a subset of case-control studies conducted on small numbers of patients found that alcohol consumption offers a protective effect against the development of POAG [50] and ocular HTN [51].
Coffee
Coffee is a rich source of caffeine, a biologically active compound that exerts numerous physiological effects on the human body. A transient elevation in IOP has been noted following caffeine ingestion in patients with different types of glaucoma [52,53,54] and, to a lesser extent, in healthy individuals [17, 55]. Furthermore, the Blue Mountains Eye Study [56] found a higher mean IOP among POAG patients that reported regular caffeine consumption. Caffeine acts as a phosphodiesterase inhibitor which leads to an increase in intracellular cyclic adenosine monophosphate dehydrogenase, thereby stimulating aqueous humor production [57, 58].
Although elevated IOP is a well-established risk factor in POAG, studies looking into the connection between caffeine consumption and the incidence of POAG did not establish any association [59, 60]. However, Pasquale et al. [61] reported a positive association between caffeine consumption and the likelihood of developing pseudoexfoliative glaucoma in a large cohort of patients. Such association is assumed to be secondary to a caffeine-induced elevation in homocysteine levels [62, 63], which is thought to be a trigger stimulating the formation of basement membrane material [64].
Tea
The nutritional value of tea is derived from its major constituents (i.e. polyphenols, caffeine, and minerals) [65]. Flavonoids, a major polyphenol in tea, are thought to play a role in glaucoma [13, 66] owing to their various physiological actions that are proposed to affect non-IOP-dependent mechanisms. Studies have shown that flavonoids demonstrate their protective effect by reducing oxidative stress [67] and improving blood flow [68].
The available evidence on the relation between tea consumption, outside the context of caffeine intake, and the incidence of glaucoma is scarce. Wu et al. [60] recently published a cross-sectional report from the National Health and Nutrition Examination Survey in the USA on the association between glaucoma and commonly consumed beverages. Their results have demonstrated that participants consuming at least one cup of hot tea daily are less likely to have glaucoma compared to their non-consuming counterparts.
Ginkgo biloba Extract
Ginkgo biloba extract (GBE) has been tested in the treatment of various medical conditions [69], including glaucoma [70, 71]. GBE exhibits a myriad of pharmacological properties making it relevant to the pathogenesis of glaucoma. The current evidence suggests that GBE increases ocular blood flow [72], improves retinal ganglion cell survival [73], and protects against oxidative stress [74].
Based on the fact that reduced ocular blood flow is thought to be a major player in the pathogenesis of normal tension glaucoma (NTG) [75], multiple studies have looked into the effect of GBE on patients with NTG. Park JW, et al. [76] proved that GBE intake improves retinal blood flow in the peri-papillary region among patients with NTG. Moreover, multiple reports agree that GBE improves visual function [77, 78], and slows the progression of visual field damage [19] in NTG. Conversely, a clinical trial from China found no effect on newly diagnosed patients with mild visual field loss [79].
Fruits and Vegetables
Being rich in antioxidants, it is speculated that a diet rich in fruits and vegetables can decrease the risk of developing glaucoma. However, the nutrient composition of different fruits and vegetables varies, making it difficult to link the presumed protective effect to a single source. Nonetheless, multiple cross-sectional studies were conducted using food frequency questionnaires in an attempt to link certain fruits and vegetables to glaucoma. Coleman et al. [80] found a decreased glaucoma risk in women who consumed fruits and vegetables rich in vitamin A and carotenes, namely collard greens, kale, carrots, and peaches. Another study by Giaconi et al. [18] also concluded that there is a decreased likelihood of glaucoma among women that reported a greater intake of fruits and vegetables rich in vitamins A and C, and carotenes.
Moreover, nitric oxide (NO) is thought to be a major contributor to vascular dysregulation in patients with POAG [81]. Therefore, it is hypothesized that high consumption of dietary nitrates might have a protective effect against the development of POAG. In a prospective cohort, Kang et al. [82] found that a diet rich in nitrates and green leafy vegetables was associated with a lower risk of developing POAG.
Chocolate
Dark chocolate is a rich dietary source of polyphenol compounds, specifically flavonoids [83]. Acute consumption of dark chocolate has been shown to reverse vascular endothelial dysfunction by decreasing oxidative stress and increasing the bioavailability of NO [84]. Therefore, it is proven beneficial in patients with certain cardiovascular diseases such as HTN [85] and peripheral artery disease [86].
In glaucoma, the only trial looking into the effect of dark chocolate was published by Terai et al. [87]. Their study showed that acute consumption of dark chocolate increased retinal vessel diameter in healthy subjects, but not in glaucoma patients. A possible explanation of such finding is a compromised ability of the vascular endothelium to produce NO in patients with glaucoma. In spite of that, further research is still required to properly outline the role of dark chocolate in glaucoma.
Saffron
The only published study on the relation between IOP and saffron comes from Iran, the world’s largest saffron exporter. Jabbarpoor Bonyadi et al. [88] studied the effect of a daily oral saffron capsule on IOP in patients with POAG. After a period of 3 weeks, a statistically significant decline in IOP was noted among the study group. They suggested that this hypotensive action is secondary to the antioxidative effect of saffron [89] on dysfunctional trabecular meshwork. However, due to limited experimental data, the exact mechanism remains unclear.
Table 1 summarizes key findings from all the cited studies providing evidence regarding the effect of individual dietary components on IOP and glaucoma.
Dietary Supplements
The benefit of dietary supplements is well-established in the management of patients with age-related macular degeneration [90, 91]; however, in glaucoma, we still lack supporting evidence. A considerable amount of research suggests that levels of oxidative markers are altered in the plasma [92,93,94,95,96,97] and aqueous [98, 99] of patients with POAG [95, 99], as well as different types of glaucoma [92,93,94]. Therefore, it is hypothesized that the use of dietary supplements rich in antioxidants might play a role in glaucoma.
Wang et al. [100] looked at the relation between the prevalence of glaucoma and the use of dietary supplements containing antioxidant vitamins (i.e. A, C, and E) among participants of the National Health and Nutrition Examination Survey. They also obtained measurements of serum vitamin levels to correlate them with the intake of supplements. No relation was found between reported glaucoma and supplemental use, or serum levels, of vitamins A and E. On the other hand, the supplemental intake of vitamin C was linked to a decreased chance of glaucoma; however, this did not correlate with serum vitamin C levels.
To date, the only prospective randomized clinical trial evaluating the possible effect of antioxidant supplements in glaucoma was published by Garcia-Medina et al. [101]. They studied the effect of the Age-Related Eye Disease Study (AREDS) formula on a small sample of patients with mild to moderate POAG. After 2 years of follow up, there was no difference in outcome between the studied groups.
Moreover, the possible role of long-chain polyunsaturated fatty acids has also been explored in the literature. A fatty acid imbalance between omega-3 and omega-6 is believed to contribute to the pathogenesis of POAG [102]. Furthermore, epidemiological studies assessing the dietary consumption of fatty acids have suggested that an imbalance in the omega-3-to-omega-6 ratio might be associated with an increased risk of developing glaucoma [103, 104]. However, in the trial conducted by Garcia-medina et al. [101], the addition of omega-3 supplements to one of the arms in the study did not yield any benefit to POAG patients.
Conclusion
The current level of evidence suggests that an individual’s diet might have an impact on IOP, incidence, and progression of glaucoma. Given that the majority of results are drawn from observational studies, well-designed, randomized, controlled, clinical trials are required to reinforce the current body of evidence.
A sound dietary advice to glaucoma patients would be to maintain a normal weight, avoid excessive coffee consumption, and increase the intake of fruits and vegetables. However, patients should be advised that nutritional management may complement, but would not substitute conventional glaucoma treatment.
References
Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–8.
Coleman AL, Miglior S. Risk factors for glaucoma onset and progression. Surv Ophthalmol. 2008;53(Suppl 1):S3–10.
Flammer J, Haefliger IO, Orgül S, Resink T. Vascular dysregulation: a principal risk factor for glaucomatous damage? J Glaucoma. 1999;8(3):212–9.
Izzotti A, Bagnis A, Saccà SC. The role of oxidative stress in glaucoma. Mutat Res. 2006;612(2):105–14.
Rieck J. The pathogenesis of glaucoma in the interplay with the immune system. Invest Ophthalmol Vis Sci. 2013;54(3):2393–409.
Casson RJ. Possible role of excitotoxicity in the pathogenesis of glaucoma. Clin Experiment Ophthalmol. 2006;34(1):54–63.
Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120(10):1268–79.
Osborne NN. Recent clinical findings with memantine should not mean that the idea of neuroprotection in glaucoma is abandoned. Acta Ophthalmol. 2009;87(4):450–4.
Klöcker N, Kermer P, Weishaupt JH, Labes M, Ankerhold R, Bähr M. Brain-derived neurotrophic factor-mediated neuroprotection of adult rat retinal ganglion cells in vivo does not exclusively depend on phosphatidyl-inositol-3′-kinase/protein kinase B signaling. J Neurosci. 2000;20(18):6962–7.
Yamamoto R, Yoneda S, Hara H. Neuroprotective effects of beta-secretase inhibitors against rat retinal ganglion cell death. Neurosci Lett. 2004;370(1):61–4.
Kojima S, Sugiyama T, Kojima M, Azuma I, Ito S. Effect of the consumption of ethanol on the microcirculation of the human optic nerve head in the acute phase. Jpn J Ophthalmol. 2000;44(3):318–9.
Jia LY, Sun L, Fan DS, Lam DS, Pang CP, Yam GH. Effect of topical Ginkgo biloba extract on steroid-induced changes in the trabecular meshwork and intraocular pressure. Arch Ophthalmol. 2008;126(12):1700–6.
Patel S, Mathan JJ, Vaghefi E, Braakhuis AJ. The effect of flavonoids on visual function in patients with glaucoma or ocular hypertension: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2015;253(11):1841–50.
Bower TN, Muhsen S, Overbury O, Birt C, Kasner O. Canadian ophthalmologists’ opinions concerning complementary and alternative medicine (CAM) use in glaucoma. J Glaucoma. 2014;23(7):430–4.
Rhee DJ, Spaeth GL, Myers JS, et al. Prevalence of the use of complementary and alternative medicine for glaucoma. Ophthalmology. 2002;109(3):438–43.
Wan MJ, Daniel S, Kassam F, et al. Survey of complementary and alternative medicine use in glaucoma patients. J Glaucoma. 2012;21(2):79–82.
Ajayi OB, Ukwade MT. Caffeine and intraocular pressure in a Nigerian population. J Glaucoma. 2001;10(1):25–31.
Giaconi JA, Yu F, Stone KL, et al. The association of consumption of fruits/vegetables with decreased risk of glaucoma among older African-American women in the study of osteoporotic fractures. Am J Ophthalmol. 2012;154(4):635–44.
Lee J, Sohn SW, Kee C. Effect of Ginkgo biloba extract on visual field progression in normal tension glaucoma. J Glaucoma. 2013;22(9):780–4.
Kim HT, Kim JM, Kim JH, et al. Relationships between anthropometric measurements and intraocular pressure: the Korea National Health and Nutrition Examination Survey. Am J Ophthalmol. 2017;173:23–33.
Lin CP, Lin YS, Wu SC, Ko YS. Age- and gender-specific association between intraocular pressure and metabolic variables in a Taiwanese population. Eur J Intern Med. 2012;23(1):76–82.
Cohen E, Kramer M, Shochat T, Goldberg E, Garty M, Krause I. Relationship between body mass index and intraocular pressure in men and women: a population-based study. J Glaucoma. 2016;25(5):e509–13.
Yoshida M, Ishikawa M, Karita K, et al. Association of blood pressure and body mass index with intraocular pressure in middle-aged and older Japanese residents: a cross-sectional and longitudinal study. Acta Med Okayama. 2014;68(1):27–34.
Wang YX, Xu L, Zhang XH, You QS, Zhao L, Jonas JB. Five-year change in intraocular pressure associated with changes in arterial blood pressure and body mass index. The Beijing eye study. PLoS One. 2013;8(10):e77180.
Nakano T, Tatemichi M, Miura Y, Sugita M, Kitahara K. Long-term physiologic changes of intraocular pressure: a 10-year longitudinal analysis in young and middle-aged Japanese men. Ophthalmology. 2005;112(4):609–16.
Marseglia L, Manti S, D’Angelo G, et al. Oxidative stress in obesity: a critical component in human diseases. Int J Mol Sci. 2014;16(1):378–400.
Caballero M, Liton PB, Epstein DL, Gonzalez P. Proteasome inhibition by chronic oxidative stress in human trabecular meshwork cells. Biochem Biophys Res Commun. 2003;308(2):346–52.
Stojanov O, Stokić E, Sveljo O, Naumović N. The influence of retrobulbar adipose tissue volume upon intraocular pressure in obesity. Vojnosanit Pregl. 2013;70(5):469–76.
Çekiç B, Toslak İE, Doğan B, Çakır T, Erol MK, Bülbüller N. Effects of obesity on retrobulbar flow hemodynamics: color Doppler ultrasound evaluation. Arq Bras Oftalmol. 2017;80(3):143–7.
Kim YK, Choi HJ, Jeoung JW, Park KH, Kim DM. Five-year incidence of primary open-angle glaucoma and rate of progression in health center-based Korean population: the Gangnam Eye Study. PLoS One. 2014;9(12):e114058.
Le A, Mukesh BN, Mccarty CA, Taylor HR. Risk factors associated with the incidence of open-angle glaucoma: the visual impairment project. Invest Ophthalmol Vis Sci. 2003;44(9):3783–9.
Jiang X, Varma R, Wu S, et al. Baseline risk factors that predict the development of open-angle glaucoma in a population: the Los Angeles Latino Eye Study. Ophthalmology. 2012;119(11):2245–53.
Ramdas WD, Wolfs RC, Hofman A, De Jong PT, Vingerling JR, Jansoniusg NM. Lifestyle and risk of developing open-angle glaucoma: the Rotterdam study. Arch Ophthalmol. 2011;129(6):767–72.
Pasquale LR, Willett WC, Rosner BA, Kang JH. Anthropometric measures and their relation to incident primary open-angle glaucoma. Ophthalmology. 2010;117(8):1521–9.
Leske MC, Connell AM, Wu SY, Hyman LG, Schachat AP. Risk factors for open-angle glaucoma. The Barbados Eye Study. Arch Ophthalmol. 1995;113(7):918–24.
Jang HD, Kim DH, Han K, et al. Relationship between Intraocular pressure and parameters of obesity in Korean Adults: the 2008–2010 Korea National Health and Nutrition Examination Survey. Curr Eye Res. 2015;40(10):1008–17.
Zhao D, Kim MH, Pastor-Barriuso R, et al. A longitudinal study of association between adiposity markers and intraocular pressure: the Kangbuk Samsung Health Study. PLoS One. 2016;11(1):e0146057.
Wygnanski-Jaffe T, Bieran I, Tekes-Manova D, Morad Y, Ashkenazi I, Mezer E. Metabolic syndrome: a risk factor for high intraocular pressure in the Israeli population. Int J Ophthalmol. 2015;8(2):403–6.
Oh SW, Lee S, Park C, Kim DJ. Elevated intraocular pressure is associated with insulin resistance and metabolic syndrome. Diabetes Metab Res Rev. 2005;21(5):434–40.
Newman-casey PA, Talwar N, Nan B, Musch DC, Stein JD. The relationship between components of metabolic syndrome and open-angle glaucoma. Ophthalmology. 2011;118(7):1318–26.
Giurlani BP, Obie LG, Petersen CG, Presley DD. Alcohol and open angle glaucoma–influence on detection, IOP, BP/IOP ratios. J Am Opt Assoc. 1978;49(4):409–16.
Buckingham T, Young R. The rise and fall of intra-ocular pressure: the influence of physiological factors. Ophthalmic Physiol Opt. 1986;6(1):95–9.
Houle RE, Grant WM. Alcohol, vasopressin, and intraocular pressure. Invest Ophthalmol. 1967;6(2):145–54.
Leydhecker W, Krieglstein GK, Uhlich E. Experimental investigations on the mode of action of alcoholic liquor on the intra-ocular pressure (author’s transl). Klin Monbl Augenheilkd. 1978;173(1):75–9.
Kojima S, Sugiyama T, Kojima M, Azuma I, Ito S. Effect of the consumption of ethanol on the microcirculation of the human optic nerve head in the acute phase. Jpn J Ophthalmol. 2000;44(3):318–9.
Klein BE, Klein R, Ritter LL. Relationship of drinking alcohol and smoking to prevalence of open-angle glaucoma. The Beaver Dam Eye Study. Ophthalmology. 1993;100(11):1609–13.
Kang JH, Willett WC, Rosner BA, Hankinson SE, Pasquale LR. Prospective study of alcohol consumption and the risk of primary open-angle glaucoma. Ophthalmic Epidemiol. 2007;14(3):141–7.
Xu L, You QS, Jonas JB. Prevalence of alcohol consumption and risk of ocular diseases in a general population: the Beijing Eye Study. Ophthalmology. 2009;116(10):1872–9.
Kahn HA, Milton RC. Alternative definitions of open-angle glaucoma. Effect on prevalence and associations in the Framingham eye study. Arch Ophthalmol. 1980;98(12):2172–7.
Fan BJ, Leung YF, Wang N, et al. Genetic and environmental risk factors for primary open-angle glaucoma. Chin Med J. 2004;117(5):706–10.
Seddon JM, Schwartz B, Flowerdew G. Case-control study of ocular hypertension. Arch Ophthalmol. 1983;101(6):891–4.
Jiwani AZ, Rhee DJ, Brauner SC, et al. Effects of caffeinated coffee consumption on intraocular pressure, ocular perfusion pressure, and ocular pulse amplitude: a randomized controlled trial. Eye (Lond). 2012;26(8):1122–30.
Avisar R, Avisar E, Weinberger D. Effect of coffee consumption on intraocular pressure. Ann Pharmacother. 2002;36(6):992–5.
Higginbotham EJ, Kilimanjaro HA, Wilensky JT, Batenhorst RL, Hermann D. The effect of caffeine on intraocular pressure in glaucoma patients. Ophthalmology. 1989;96(5):624–6.
Li M, Wang M, Guo W, Wang J, Sun X. The effect of caffeine on intraocular pressure: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2011;249(3):435–42.
Chandrasekaran S, Rochtchina E, Mitchell P. Effects of caffeine on intraocular pressure: the Blue Mountains Eye Study. J Glaucoma. 2005;14(6):504–7.
Kurata K, Fujimoto H, Tsukuda R, Suzuki T, Ando T, Tokuriki M. Aqueous humor dynamics in beagle dogs with caffeine-induced ocular hypertension. J Vet Med Sci. 1998;60(6):737–9.
Kurata K, Maeda M, Nishida E, et al. Relationship between caffeine-induced ocular hypertension and ultrastructure changes of non-pigmented ciliary epithelial cells in rats. J Toxicol Sci. 1997;22(5):447–54.
Kang JH, Willett WC, Rosner BA, Hankinson SE, Pasquale LR. Caffeine consumption and the risk of primary open-angle glaucoma: a prospective cohort study. Invest Ophthalmol Vis Sci. 2008;49(5):1924–31.
Wu CM, Wu AM, Tseng VL, Yu F, Coleman AL. Frequency of a diagnosis of glaucoma in individuals who consume coffee, tea and/or soft drinks. Br J Ophthalmol. 2017. https://doi.org/10.1136/bjophthalmol-2017-310924.
Pasquale LR, Wiggs JL, Willett WC, Kang JH. The relationship between caffeine and coffee consumption and exfoliation glaucoma or glaucoma suspect: a prospective study in two cohorts. Invest Ophthalmol Vis Sci. 2012;53(10):6427–33.
Grubben MJ, Boers GH, Blom HJ, et al. Unfiltered coffee increases plasma homocysteine concentrations in healthy volunteers: a randomized trial. Am J Clin Nutr. 2000;71(2):480–4.
Urgert R, van Vliet T, Zock PL, Katan MB. Heavy coffee consumption and plasma homocysteine: a randomized controlled trial in healthy volunteers. Am J Clin Nutr. 2000;72(5):1107–10.
Bleich S, Roedl J, Von ahsen N, et al. Elevated homocysteine levels in aqueous humor of patients with pseudoexfoliation glaucoma. Am J Ophthalmol. 2004;138(1):162–4.
Wierzejska R. Tea and health—a review of the current state of knowledge. Przegl Epidemiol. 2014;68(3):501–6 (595-9).
Milea D, Aung T. Flavonoids and glaucoma: revisiting therapies from the past. Graefes Arch Clin Exp Ophthalmol. 2015;253(11):1839–40.
Maher P, Hanneken A. Flavonoids protect retinal ganglion cells from oxidative stress-induced death. Invest Ophthalmol Vis Sci. 2005;46(12):4796–803.
Grassi D, Mulder TP, Draijer R, Desideri G, Molhuizen HO, Ferri C. Black tea consumption dose-dependently improves flow-mediated dilation in healthy males. J Hypertens. 2009;27(4):774–81.
Nash KM, Shah ZA. Current Perspectives on the beneficial role of Ginkgo biloba in neurological and cerebrovascular disorders. Integr Med Insights. 2015;10:1–9.
Cybulska-Heinrich AK, Mozaffarieh M, Flammer J. Ginkgo biloba: an adjuvant therapy for progressive normal and high tension glaucoma. Mol Vis. 2012;18:390–402.
Kang JM, Lin S. Ginkgo biloba and its potential role in glaucoma. Curr Opin Ophthalmol. 2017. https://doi.org/10.1097/ICU.0000000000000459.
Chung HS, Harris A, Kristinsson JK, Ciulla TA, Kagemann C, Ritch R. Ginkgo biloba extract increases ocular blood flow velocity. J Ocul Pharmacol Ther. 1999;15(3):233–40.
Hirooka K, Tokuda M, Miyamoto O, Itano T, Baba T, Shiraga F. The Ginkgo biloba extract (EGb 761) provides a neuroprotective effect on retinal ganglion cells in a rat model of chronic glaucoma. Curr Eye Res. 2004;28(3):153–7.
Eckert A, Keil U, Scherping I, Hauptmann S, Müller WE. Stabilization of mitochondrial membrane potential and improvement of neuronal energy metabolism by Ginkgo biloba extract EGb 761. Ann N Y Acad Sci. 2005;1056:474–85.
Fan N, Wang P, Tang L, Liu X. Ocular blood flow and normal tension glaucoma. Biomed Res Int. 2015;2015:308505.
Park JW, Kwon HJ, Chung WS, Kim CY, Seong GJ. Short-term effects of Ginkgo biloba extract on peripapillary retinal blood flow in normal tension glaucoma. Korean J Ophthalmol. 2011;25(5):323–8.
Shim SH, Kim JM, Choi CY, Kim CY, Park KH. Ginkgo biloba extract and bilberry anthocyanins improve visual function in patients with normal tension glaucoma. J Med Food. 2012;15(9):818–23.
Quaranta L, Bettelli S, Uva MG, Semeraro F, Turano R, Gandolfo E. Effect of Ginkgo biloba extract on preexisting visual field damage in normal tension glaucoma. Ophthalmology. 2003;110(2):359–62.
Guo X, Kong X, Huang R, et al. Effect of Ginkgo biloba on visual field and contrast sensitivity in Chinese patients with normal tension glaucoma: a randomized, crossover clinical trial. Invest Ophthalmol Vis Sci. 2014;55(1):110–6.
Coleman AL, Stone KL, Kodjebacheva G, et al. Glaucoma risk and the consumption of fruits and vegetables among older women in the study of osteoporotic fractures. Am J Ophthalmol. 2008;145(6):1081–9.
Emam WA, Zidan HE, Abdulhalim BE, Dabour SA, Ghali MA, Kamal AT. Endothelial nitric oxide synthase polymorphisms and susceptibility to high-tension primary open-angle glaucoma in an Egyptian cohort. Mol Vis. 2014;20:804–11.
Kang JH, Willett WC, Rosner BA, Buys E, Wiggs JL, Pasquale LR. Association of dietary nitrate intake with primary open-angle glaucoma: a prospective analysis from the nurses’ health study and health professionals follow-up study. JAMA Ophthalmol. 2016;134(3):294–303.
Kerimi A, Williamson G. The cardiovascular benefits of dark chocolate. Vascul Pharmacol. 2015;71:11–5.
Heiss C, Kleinbongard P, Dejam A, et al. Acute consumption of flavanol-rich cocoa and the reversal of endothelial dysfunction in smokers. J Am Coll Cardiol. 2005;46(7):1276–83.
Desch S, Kobler D, Schmidt J, et al. Low vs. higher-dose dark chocolate and blood pressure in cardiovascular high-risk patients. Am J Hypertens. 2010;23(6):694–700.
Loffredo L, Perri L, Catasca E, et al. Dark chocolate acutely improves walking autonomy in patients with peripheral artery disease. J Am Heart Assoc. 2014;3(4):e001072. https://doi.org/10.1161/JAHA.114.001072.
Terai N, Gedenk A, Spoerl E, Pillunat LE, Stodtmeister R. The short-term effect of flavonoid-rich dark chocolate on retinal vessel diameter in glaucoma patients and age-matched controls. Acta Ophthalmol. 2014;92(5):e341–5.
Jabbarpoor Bonyadi MH, Yazdani S, Saadat S. The ocular hypotensive effect of saffron extract in primary open angle glaucoma: a pilot study. BMC Compl Altern Med. 2014;14:399.
Maccarone R, Di Marco S, Bisti S. Saffron supplement maintains morphology and function after exposure to damaging light in mammalian retina. Invest Ophthalmol Vis Sci. 2008;49(3):1254–61.
Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001; 119(10):1417–36.
Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA. 2013; 309(19):2005–15.
Abu-Amero KK, Azad TA, Mousa A, Osman EA, Sultan T, Al-Obeidan SA. Total antioxidant level is correlated with intra-ocular pressure in patients with primary angle closure glaucoma. BMC Res Notes. 2014;7:163.
Demirdögen BC, Ceylan OM, Işikoğlu S, Mumcuoğlu T, Erel O. Evaluation of oxidative stress and paraoxonase phenotypes in pseudoexfoliation syndrome and pseudoexfoliation glaucoma. Clin Lab. 2014;60(1):79–86.
Dursun F, Vural Ozec A, Aydin H, et al. Total oxidative stress, paraoxonase and arylesterase levels at patients with pseudoexfoliation syndrome and pseudoexfoliative glaucoma. Int J Ophthalmol. 2015;8(5):985–90.
Abu-Amero KK, Kondkar AA, Mousa A, Osman EA, Al-Obeidan SA. Decreased total antioxidants in patients with primary open angle glaucoma. Curr Eye Res. 2013;38(9):959–64.
Mousa A, Kondkar AA, Al-obeidan SA, et al. Association of total antioxidants level with glaucoma type and severity. Saudi Med J. 2015;36(6):671–7.
Abu-Amero KK, Kondkar AA, Mousa A, Osman EA, Al-Obeidan SA. Decreased total antioxidants status in the plasma of patients with pseudoexfoliation glaucoma. Mol Vis. 2011;17:2769–75.
Beyazyıldız E, Cankaya AB, Beyazyıldız O, et al. Disturbed oxidant/antioxidant balance in aqueous humour of patients with exfoliation syndrome. Jpn J Ophthalmol. 2014;58(4):353–8.
Ergan E, Ozturk F, Beyazyildiz E, et al. Oxidant/antioxidant balance in the aqueous humor of patients with glaucoma. Int J Ophthalmol. 2016;9(2):249–52.
Wang SY, Singh K, Lin SC. Glaucoma and vitamins A, C, and E supplement intake and serum levels in a population-based sample of the United States. Eye (Lond). 2013;27(4):487–94.
Garcia-Medina JJ, Garcia-Medina M, Garrido-Fernandez P, et al. A two-year follow-up of oral antioxidant supplementation in primary open-angle glaucoma: an open-label, randomized, controlled trial. Acta Ophthalmol. 2015;93(6):546–54.
Ren H, Magulike N, Ghebremeskel K, Crawford M. Primary open-angle glaucoma patients have reduced levels of blood docosahexaenoic and eicosapentaenoic acids. Prostaglandins Leukot Essent Fatty Acids. 2006;74(3):157–63.
de Arcelus MP, Toledo E, Martínez-González MÁ, Sayón-Orea C, Gea A, Moreno-Montañés J. Omega 3:6 ratio intake and incidence of glaucoma: the SUN cohort. Clin Nutr. 2014;33(6):1041–5.
Kang JH, Pasquale LR, Willett WC, et al. Dietary fat consumption and primary open-angle glaucoma. Am J Clin Nutr. 2004;79(5):755–64.
Acknowledgements
Funding
No funding or sponsorship was received for this study or publication of this article. The article processing charges were funded by the authors.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Disclosures
A. M. Al Owaifeer and A. A. Al Taisan have nothing to disclose.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Data Availability
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article, go to https://doi.org/10.6084/m9.figshare.5809545.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Al Owaifeer, A.M., Al Taisan, A.A. The Role of Diet in Glaucoma: A Review of the Current Evidence. Ophthalmol Ther 7, 19–31 (2018). https://doi.org/10.1007/s40123-018-0120-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-018-0120-3