
Abstract
Introduction
Treatment adherence is a critical success factor in the disease-modifying therapy (DMT) of multiple sclerosis (MS). The REBISTART study prospectively evaluated adherence in patients using components of a patient support program (PSP).
Methods
The 12-month non-interventional multicenter study examined the real-world adherence to subcutaneously (sc) injected interferon beta-1a (Rebif®). Patient-assessed adherence was measured by a visual analog scale (VAS) and the Morisky Medication Adherence Scale (MMAS). Objective adherence data were obtained by readouts from the RebiSmart® injection device.
Results
Of 333 patients, 70.9% used the nursing service as the core component of the PSP. Self-assessed VAS-based adherence was stable over time at 94.0–96.3%. Similarly, MMAS score (maximum 4) was 3.8–3.9 at all visits, also reflecting high self-assessed adherence. In 269 patients using the RebiSmart® injection device, mean readout-based objective adherence was similarly high (93.0–98.4% throughout visits). At last available visit, VAS-based adherence was independent of participation in the PSP nursing service (93.1% with participation versus 91.7% without it).
Adherence was also independent of injection method or disease-related measures, including fatigue, depression, cognition, and quality of life. The most frequent reason for the premature discontinuations (38.7% of patients) was “change of treatment” (10.0%).
Discussion
We suggest that subgroups that may specifically benefit from PSP include patients who live alone, use multiple comedications, and are affected by cognitive impairment, depression, and/or fatigue. Further studies should investigate the potential usefulness of PSPs in these populations.
Conclusions
Very high adherence rates independent of the PSP nursing service over 1 year of treatment indicate that IFN beta-1a sc is an easy-to-use and well-tolerated disease-modifying drug.
Trial Registration Number
Vfa.de: No. 892. https://www.vfa.de/de/arzneimittel-forschung/datenbanken-zu-arzneimitteln/nisdb/nis-details/_892.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
Treatment adherence is a critical success factor in the management of multiple sclerosis (MS). |
The REBISTART study evaluated whether a patient support program and its modules increase the treatment adherence of patients with MS who newly started or restarted subcutaneous treatment with interferon beta-1a over a period of 12 month. |
What was learned from the study? |
Objective adherence (RebiSmart® ID readout) and self-assessed adherence were high and stable over time. |
Adherence was independent of participation in the nursing service of the patient support program, the injection method, or disease-related parameters. |
Self-assessed adherence is a surprisingly accurate tool to gauge adherence in patients with MS. |
Further studies should investigate the usefulness of patient support programs in subgroups that are expected to experience a specific benefit. |
Introduction
Adherence to prescribed drug therapy is a critical prerequisite in the management of chronic diseases [1, 2]. Poor adherence negatively affects outcomes and health benefits of pharmacological treatments [3]. Adherence is influenced by dosing regimen, route and mode of application, side effects, and perceived effectiveness [4]. Patient psychological situation [5] and cognitive capacity also play important roles [6].
In patients with multiple sclerosis (MS), previous studies have shown that non-adherence to disease-modifying treatments (DMTs) and premature discontinuation remain relevant issues [7]. Patient support programs can markedly reduce early treatment discontinuation and foster persistence and adherence to a prescribed regimen [8, 9].
Subcutaneously administered interferon beta-1a (IFN beta-1a sc; Rebif®) is a DMT licensed for patients with relapsing multiple sclerosis (RMS) and individuals with a clinically isolated demyelinating syndrome (CIS) at high risk of developing clinically definitive MS (CDMS) [10]. A significant inverse correlation between adherence and subsequent risk of MS relapse on treatment was previously reported for interferon IFN beta-1a [11].
Patients treated with IFN beta-1a sc are routinely offered participation in the product-specific patient support program (PSP). This voluntary, free-of-charge program includes several modules, e.g., nursing service, coaching, online information, patient academy, and patient journal. Each module can be used without time limits, either as a stand-alone option or as component of a complete package. The nursing service is the core of the PSP. Specifically trained and certified MS nurses support the patients as permanently accessible contacts, in person and via telephone. They provide injection training at the start of therapy, and individualized long-term treatment assistance to patients in their domestic environment. The coaching module may be used on its own or in combination with the nursing service. Coaches are medically trained professionals, who discuss issues of living with MS via telephone. The online module MSdialog serves to more effectively engage patients with MS and their healthcare providers with treatment adherence information. MSdialog also allows people with MS to engage in the management of their disease by asking them to complete periodic health report questionnaires based on short forms of published instruments and standard scales, such as the Multiple Sclerosis Quality of Life Inventory (MSQLI) and the Multiple Sclerosis International Quality of Life (MusiQoL) questionnaires.
Over a period of 12 months, the study REBISTART evaluated whether this PSP and more specifically which of its modules increase the treatment adherence of patients with MS who start or restart treatment with IFN beta-1a sc.
Methods
REBISTART was a non-interventional multicenter clinical study performed at 54 neurological study centers (neurological specialty practices and hospital departments or outpatient clinics) in Germany. It was conducted in accordance with the Declaration of Helsinki, Good Clinical Practice (as far as applicable in the non-interventional setting), Good Epidemiological Practice, and Good Pharmacoepidemiology Practice. The study protocol was approved by relevant institutional review boards and independent ethics committees, in line with national and/or international regulations. All patients provided their written informed consent before inclusion into the study.
Eligibility criteria were as follows: adults with a diagnosis of CIS (clinically isolated syndrome) at high risk of developing clinically definitive MS (CDMS), or relapsing multiple sclerosis (RRMS) according to McDonald criteria of 2010 [12]. Participants could be treatment-naïve or previously treated with any DMT licensed for MS with the exception of IFN beta-1a sc itself. Further prerequisites for inclusion were mild to moderate disability (Expanded Disability Status Scale [EDSS] score ≤ 3.5) at baseline, and time since MS diagnosis ≤ 5 years.
Patients could start treatment with a starter pack containing 12 prefilled syringes for titration of interferon during the first month of treatment: six syringes with 8.8 µg of active ingredient for the first 2 weeks, and six syringes with 22 µg each for weeks 3 and 4.
Participants were observed for a period of up to 12 months. Study data were documented at baseline, i.e., start of treatment with IFN beta-1a sc (visit 1) and at 1 month (visit 2), 3 months (visit 3), 6 months (visit 4), and 12 months (visit 5) thereafter. In patients with premature treatment discontinuation, a final documentation according to the specifications of visit 5 was mandatory.
Data analysis was based on the safety analysis set, comprising all patients who entered the study and received at least one injection of IFN beta-1a sc within the study timeframe.
Study Objectives
The primary target parameter was patient-assessed adherence to treatment with IFN beta-1a sc as a function of participation in the nursing service as the core module of the PSP during 12 months of observation. The patients rated their adherence (during the time since the last visit) on a visual analog scale (VAS) ranging from 0 (lowest adherence) to 100 (highest adherence) and on the 4-item Morisky Medication Adherence Scale (MMAS; 4 = maximum adherence).
Secondary target parameters included the comparison of subjective self-assessed (VAS) adherence versus objective adherence based on the readouts from the electronic injection device RebiSmart®; correlation between VAS data and disease-associated measures which may have a potential impact on, or correlate with, adherence including the participation in coaching as the core module of the PSP; type of injection device used (prefilled syringe, Rebiject II®, RebiDose®, RebiSmart®); fatigue (Fatigue Scale for Motor and Cognitive Functions [FSMC]); depression (Beck Depression Inventory-Fast Screen [BDI-FS]); disease-related quality of life (Multiple Sclerosis International Quality of Life questionnaire [MusiQoL]); and medication possession ratio (MPR; defined as the ratio of the number of days formally covered by a prescription by the actual number of days passed until the next prescription).
Data Retrieval
Patient answers to questionnaires and their VAS scores were transferred into the electronic data capture system. Socio-demographic data, MS history, results of EDSS and magnetic resonance imaging (MRI) examinations (if performed), health-economic and socioeconomic data, data on IFN beta-1a sc therapy, and injection device were extracted from the patient’s medical records and documented in an electronic case report form (CRF). The MPR was calculated from number of prescribed packages multiplied by the package size converted to time on therapy. Occurrence of adverse events was assessed by the physicians on the basis of patient reports, medical records, and physical examinations, as applicable.
Statistical Analyses
Data were first analyzed by descriptive statistics. Categorical variables were represented by frequency distribution. Student’s t test was used to probe for statistical significant differences between participants and non-participants in the PSP nursing service and/or PSP coaching.
Correlations between the VAS score and adherence-related parameters were analyzed by Pearson product-moment correlation assuming normal distributions, and Spearman rank correlation. Statistical tests were exploratory at a 5.0% significance level. All values are given as means ± standard deviation (SD) if not otherwise specified.
Results
Patient Characteristics
A total of 341 patients were enrolled. The safety analysis set comprised 333 patients at a median age of 33 years (range 18–70); the majority was female (74.8%).
The most prevalent MS disease type was RRMS (79.0%) followed by CIS (18.9%) (Table 1). MS disease duration ranged between 0 and 10 years at baseline. The mean duration of MS at baseline was 0.4 ± 1.0 years, indicating a population that was treated early in the course of MS. The majority (92.8%) of the patients had not previously received any DMT, and 82.9% had received no other MS-related drugs (e.g., symptomatic treatments).
MS Disease Activity
The mean number of relapses within the last 12 months prior to baseline (i.e., the annualized relapse rate) was 1.2 ± 0.5. Overall, the patients experienced between 0 and 5 relapses within this period. The percentage of patients with a relapse during the 12 months before study was 88.0% (293 of 333 patients).
Relapses were documented in 3.9% of patients (n = 13) after baseline. A total of 2.7% (n = 9) were hospitalized with a relapse, 5 at visit 4 (month 6), and 4 at visit 5 (month 12).
The mean EDSS at baseline was 1.2 ± 0.7. The mean change of disability (EDSS) between baseline and visit 5 was 0.1 ± 0.8 in 172 patients with data available at both visits.
In patients with available MRI data at baseline and visit 5 (n = 59), there was no substantial change in the number of contrast-enhancing lesions (mean 0.9 ± 4.0) at visit 5 versus at baseline (1.3 ± 3.1), and T2 hyperintense lesions (3.9 ± 5.2 versus 4.1 ± 6.4).
Approximately half of patients already showed at least minimal signs of general and cognitive fatigue in the FSMC, and depressive symptoms in the BDI-FS questionnaires (Table 1).
The proportion of patients who were incapacitated for work during the last 12 months prior to baseline was 33.9% (n = 113). During the treatment period, incapacitation for work was documented in 9.8% (n = 25) at visit 4 (month 6) and in 7.8% (n = 22) at visit 5 (month 12).
Safety
A total of 51 patients (15.3%) experienced 90 adverse drug reactions (ADRs) during the study period. Nine ADRs in 6 patients (1.8%) were assessed by the physicians as serious adverse drug reactions. The most frequent ADRs were classified in the system organ class “general disorders and administration site conditions” (8.1%). Among these injection site reactions were observed in 11 patients (3.3%), erythema at an injection site (2.4%) followed by flu-like symptoms (2.1%).
Drug Administration and Use
The reasons for choosing a specific injection device were “patient’s choice after being presented with various injectors” in 201 patients (60.4%); in 92 patients (27.6%) the choice was based on the recommendation by the MS nurse, in 71 patients (21.3%) on the physician’s recommendation, and in 53 patients (15.9%) on the prescription. RebiSmart® was the most frequently chosen injection device [82.7% (n = 82.7) at visit 1 through 79.1% at visit 5]. Most patients initiated their therapy with the starter pack (88.3%, n = 294). The total mean treatment duration on study was 10.7 ± 3.5 months. Premature discontinuation of study was documented in 132 of 341 patients (38.7%). Reasons were available only for 78 patients with documented early discontinuation whereby multiple entries were possible. The most frequent reason was “change of treatment” (43.6%, 34 patients), others included pregnancy or patient wish (34.6%, 27 patients), followed by “adverse drug reactions” (20.5%, n = 16), and “lack of efficacy” (14.1%, n = 11).
Self-Assessed Adherence
Self-assessed therapy adherence was high (mean VAS score ≥ 91) at all visits, regardless of the injection device used (Table 2). The mean total score of the 4-item MMAS was 3.9 ± 0.5 at visit 2 and did not change substantially during study (Table 3).
Positive correlations (coefficient range 0.35–0.5) between the VAS score and the MMAS were observed at all post-baseline visits (p < 0.0001, at each visit) (Table 3). No correlations between the VAS score and any of the following factors were found at any of the applicable visits: fatigue (FSMC), depression (BDI-FS), or quality of life (MusiQoL).
The most frequent reason for missing injections over all visits and all devices was forgetfulness, with increasing incidence between visit 2 (3.2%, n = 10) and visit 5 (13.5%, n = 38). A conscious decision against injection was another reason for not injecting IFN beta-1a sc at the end of the observational period (visit 5, 4.6%, n = 13).
Objective Adherence
In patients using the RebiSmart® ID, the objective mean adherence was greater than 97.0% at visit 2 (98.4%; n = 258), visit 3 (97.7%; n = 241), and visit 4 (98.2%; n = 212) and greater than 90% at visit 5 (93.0%; n = 223) (Table 4).
The mean cumulative adherence was 95.8 ± 10.6% (n = 269). In most patients (90.7% of 269 patients, n = 244), cumulative adherence was in the range of 85–105%. There were 25 patients (9.3%) with a cumulative adherence below 85%.
Positive correlations (coefficient range 0.36–0.40) between self-assessed adherence based on the VAS score in patients using the RebiSmart® ID and objective adherence (data readouts from RebiSmart® ID) were observed at all post-baseline visits (p < 0.0001 at each visit).
Effects of PSP Nursing Service on Adherence
Participation in the PSP remained fairly constant from baseline (77.5%) to visit 5 (69.9%) (Table 5). The nursing service was the most frequently used module of the PSP (70.9% at baseline to 61.0% at visit 5), followed by MSdialog (43.8% at baseline to 36.5% at visit 5), and RebiSTAR coach (16.8% at baseline to 6.7% at visit 5). However, data on participation in components of the PSP were missing for 22.5% of patients at baseline to 30.1% at visit 5.
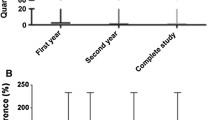
As the primary target parameter, the mean VAS-based adherence to IFN beta-1a sc in patients who exclusively participated in the PSP nursing service at the respective visit was largely stable at a high level during the observation period, ranging from 93.6% at visit 2 to 96.3% at visit 5 (Table 2).
At the last available visit, the mean VAS-based adherence in the patients who used the PSP nursing service (between all or some of the visits) was similar to the adherence in patients who never participated in the PSP nursing service: 93.1% versus 91.7% (Table 6). The mean VAS-based adherence score was 83.8 ± 17.0 (n = 4) in patients who participated only in the PSP coaching, 92.4 ± 10.1 (n = 16) in patients who continuously participated in the PSP nursing service and coaching, and 92.1 ± 14.0 (n = 80) in patients who never participated in the PSP nursing service or coaching.
Discussion
The participants of this non-interventional study were predominantly female and represented a typical population with early MS: at baseline, the majority had only minimal disability and a short disease duration. More than 90% of study participants were treatment-naïve. However, the great majority had experienced at least one relapse in the year before study initiation, which may explain the high rate of work-incapacitated individuals.
We observed high levels of self-assessed adherence to IFN beta-1a sc over the entire first year of treatment that were obviously not affected by first signs of general and cognitive fatigue, and depressive symptoms in approximately 50% of the patients before the start of therapy.
The highly significant correlations of self-assessed adherence based on the VAS and the MMAS results and those between self-assessed adherence based on the VAS and the objective adherence based on the RebiSmart® ID readouts support the validity of the VAS for assessment of adherence. The fact that VAS-assessed adherence was not influenced by disease-associated factors such as fatigue, depression, cognition, or quality of life may have been confounded by the fact that this study included patients early in the disease course with a low burden of symptoms. The high self-assessed adherence levels were similar for all injection devices and confirmed by the MPR and the high rate of objective adherence based on data readouts from the RebiSmart® ID. This type of injector was used by the great majority of the patients throughout the study. The proportion of patients using the RebiSmart® ID was higher than observed in longitudinal prescription data from healthcare system databases [13].
Adherence Compared to Observations in Other Studies with IFNb-1a
The objective cumulative adherence rate over 12 months derived from RebiSmart® ID readouts was comparable to those found in previous long-term observational studies in patients with relapsing MS and treated with IFN beta-1a sc using the RebiSmart® ID [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28].
In a retrospective study performed in Great Britain and Ireland with 225 patients, the mean adherence (doses used per doses prescribed) over the course of 24 months was 95.0% [26]. Another retrospective study from Spain reported an overall adherence rate of 92.6% over 35 months [22]. The patients in the first study were also offered patient support services, whereas a support program was not provided in the Spanish study. However, long-term support is typically offered to patients with MS who are prescribed a DMT.
Adherence Compared to Observations with Other Disease-Modifying Therapies
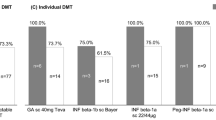
Although comparing adherence among different drugs is generally limited by the diverging routes and schedules of application, self-assessed and objective adherence to IFN beta-1a sc of greater than 90% after 12 months appears to compare favorably with other DMTs. For dimethyl fumarate, a medication possession rate of at least 80% was reported and in 63% of patients over 12 months of therapy [29]. A compliance rate of 81% at 6 months and 60% at 24 months of treatment was reported with teriflunomide in a real-world setting [30]. In other observational studies, proportions of patients with no missed doses were 66% for glatiramer acetate and 85% for IFN beta-1a applied once a week intramuscularly [31]. These data are consistent with findings of studies reviewed by Menzin et al. [32] indicating treatment adherence for injectable DMTs in the range of 49–88%.
Compared to these results, adherence appears to be numerically higher in the REBISTART study. This observation may relate to practical advantages of the RebiSmart® injection device, the route of application, and/or tolerability issues with oral disease-modifying drugs.
While healthcare data collected in clinical routine settings revealed high adherence rates for IFN beta-1a sc similar to our own results [33], previous research still has shown that patients with MS benefit from support programs in terms of higher adherence and persistence with DMTs [34, 35]. In the present study, self-assessed adherence reported at the last available visit of a patient was numerically higher in the group of patients who participated in the PSP nursing service and/or in the PSP coaching. This was consistent with the observation that patients with a higher number of contacts with the PSP nurse tended to have a higher mean VAS score at most visits.
The absence of adherence-enhancing effects of the nursing service as the core module of the PSP is probably due to a ceiling effect of the very high overall adherence in the study population. Favorable tolerability and the easy-to-use injection device probably supported the exceedingly high adherence regardless of the participation in the very well accepted PSP. There was no indication of a withdrawal bias, i.e., that patients with low adherence preferentially left the study. From a general point of view, the high overall adherence may also be related to the background effects of the well-developed support and self-organization landscape for patients with MS in Germany. However, adherence-enhancing effects of PSPs may also occur later during treatment, i.e., after more than 1 year of treatment when “needle weariness/fatigue” sets in.
Limitations
Limitations of this study include the observational, non-comparative design, the lack of a control group, and the inherent potential of biases in patient-reported outcomes, e.g., a tendency to report a supposedly favored behavior. Safety data recorded in non-interventional studies may be skewed by reporting biases which are common in routine practice.
The mere occurrence of a doctor’s visit may temporarily increase the treatment adherence of patients on chronic treatments. Therefore we adapted the number of visits to the schedule of visits most commonly used in routine clinical practice during the first year of treatment with disease-modifying MS treatments.
Subgroups that may specifically benefit from PSP include patients with MS who live alone, use multiple comedications, and suffer from cognitive impairment, depression, and/or fatigue. However, the overall adherence rates were too high to allow for a meaningful subgroup analysis. Further studies should investigate the potential usefulness of PSPs in these populations.
Conclusion
In this non-interventional, multicenter study that included patients with early MS, self-assessed adherence to IFN beta-1a sc was generally very high. The VAS has been proven to be a reliable tool to measure adherence. The favorable adherence even in patients without participation in a PSP reveals that interferon beta-1a sc remains a highly accepted and well-tolerated medication in the era of therapies with oral application and/or prolonged dosage intervals.
Although limited by the non-comparative, observational design of the study, the results support evidence of previous research showing that PSPs in MS are well accepted by patients, potentially supporting effective long-term therapy.
The results of REBISTART supports the decision to maintain the opportunity of participating in the PSP for patients starting treatment with IFN beta-1 sc in the forthcoming years.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–97.
Sabaté E. Adherence to long-term therapies. Evidence for action. World Health Organization; 2003. http://apps.who.int/medicinedocs/pdf/s4883e/s4883e.pdf.
Kern S, Reichmann H, Ziemssen T. Therapieadhärenz in der neurologischen Praxis. Beispiel: Multiple Sklerose [Adherence to neurologic treatment. Lessons from multiple sclerosis]. Nervenarzt. 2008;79:877–90.
Erbay Ö, Usta Yeşilbalkan Ö, Yüceyar N. Factors affecting the adherence to disease-modifying therapy in patients with multiple sclerosis. J Neurosci Nurs. 2018;50:291–7.
Higuera L, Carlin CS, Anderson S. Adherence to disease-modifying therapies for multiple sclerosis. J Manag Care Spec Pharm. 2016;22:1394–401.
Moghadasi AN, Pourmand S, Sharifian M, et al. Behavioral neurology of multiple sclerosis and autoimmune encephalopathies. Neurol Clin. 2016;34:17–31.
Rice DR, Kaplan TB, Hotan GC, et al. Electronic pill bottles to monitor and promote medication adherence for people with multiple sclerosis: a randomized, virtual clinical trial. J Neurol Sci. 2021;428:117612.
Nicholas JA, Edwards NC, Edwards RA, Dellarole A, Grosso M, Phillips AL. Real-world adherence to, and persistence with, once- and twice-daily oral disease-modifying drugs in patients with multiple sclerosis: a systematic review and meta-analysis. BMC Neurol. 2020;20:281.
Rieckmann P, Ziemssen T, Penner IK, et al. Adherence to subcutaneous interferon beta-1a in multiple sclerosis patients receiving periodic feedback on drug use by discussion of readouts of their RebiSmart® injector: results of the prospective cohort study REBIFLECT. Adv Ther. 2022;39:2749–60.
European Medicines Agency. Rebif® (interferon beta-1a sc) summary of product characteristics; 2020.
Moccia M, Palladino R, Russo C, et al. How many injections did you miss last month? A simple question to predict interferon β-1a adherence in multiple sclerosis. Expert Opin Drug Deliv. 2015;12:1829–35.
Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. 2011;69:292–302.
IQVIA Longitudinal Prescription Data (LRx), 09/2021; Merck Serono, data on file.
Rieckmann P, Schwab M, Pöhlau D, et al. Adherence to subcutaneous IFN β-1a in multiple sclerosis: final analysis of the non-interventional study READOUTsmart using the dosing log and readout function of RebiSmart®. Adv Ther. 2019;36:175–86.
Vališ M, Šarláková J, Halúsková S, et al. An observational study demonstrating the adherence and ease of use of the injector device, RebiSmart®. Expert Opin Drug Deliv. 2020;17:719–24.
Sauri-Suárez S, Quiñones-Aguilar S, Contreras-Marín A, et al. Adherence to self-administering interferon-β1a using RebiSmart® device in Mexican patients with relapsing multiple sclerosis. PLoS ONE. 2020;15:e0230959.
Deftereos SN, Koutlas E, Koutsouraki E, et al. Seasonal adherence to, and effectiveness of, subcutaneous interferon β-1a administered by RebiSmart® in patients with relapsing multiple sclerosis: results of the 1-year, observational GEPAT-SMART study. BMC Neurol. 2018;18:186.
Pedersen ED, Stenager E, Vadgaard JL, et al. Adherence to subcutaneous interferon beta-1a treatment using an electronic injection device: a prospective open-label Scandinavian noninterventional study (the ScanSmart study). Patient Prefer Adher. 2018;12:569–75.
Zecca C, Disanto G, Mühl S, et al. Subjective patient-reported versus objective adherence to subcutaneous interferon β-1a in multiple sclerosis using RebiSmart®: the CORE study. BMC Neurol. 2017;17:171.
Ghezzi A, Bianchi A, Baroncini D, et al. A multicenter, observational, prospective study of self- and parent-reported quality of life in adolescent multiple sclerosis patients self-administering interferon-β1a using RebiSmart™-the FUTURE study. Neurol Sci. 2017;38:1999–2005.
Krol M, de Voer G, Osowski U. Patient adherence to subcutaneous IFN beta-1a injections using the RebiSmart® injection device: a retrospective real-world study among Dutch and German patients with multiple sclerosis. Patient Prefer Adher. 2017;11:1189–96.
Fernández O, Arroyo R, Martínez-Yélamos S, et al. Long-term adherence to IFN beta-1a treatment when using RebiSmart® device in patients with relapsing-remitting multiple sclerosis. PLoS ONE. 2016;11:e0160313.
Paolicelli D, Cocco E, Di Lecce V, et al. Exploratory analysis of predictors of patient adherence to subcutaneous interferon beta-1a in multiple sclerosis: TRACER study. Expert Opin Drug Deliv. 2016;13:799–805.
Lugaresi A, De Robertis F, Clerico M, et al. Long-term adherence of patients with relapsing-remitting multiple sclerosis to subcutaneous self-injections of interferon β-1a using an electronic device: the RIVER study. Expert Opin Drug Deliv. 2016;13:931–5.
Bayas A, Ouallet JC, Kallmann B, et al. Adherence to, and effectiveness of, subcutaneous interferon β-1a administered by RebiSmart® in patients with relapsing multiple sclerosis: results of the 1-year, observational SMART study. Expert Opin Drug Deliv. 2015;12:1239–50.
Willis H, Webster J, Larkin AM, et al. An observational, retrospective, UK and Ireland audit of patient adherence to subcutaneous interferon beta-1a injections using the RebiSmart® injection device. Patient Prefer Adher. 2014;8:843–51.
Lugaresi A, Florio C, Brescia-Morra V, et al. Patient adherence to and tolerability of self-administered interferon β-1a using an electronic autoinjection device: a multicentre, open-label, phase IV study. BMC Neurol. 2012;12:7.
D’Arcy C, Thomas D, Stoneman D, et al. Patient assessment of an electronic device for subcutaneous self-injection of interferon β-1a for multiple sclerosis: an observational study in the UK and Ireland. Patient Prefer Adher. 2012;6:55–61.
Thompson MT, Virginia D, Nick B, et al. Adherence and discontinuation rates in patients on Tecfidera™ (dimethyl fumarate): long-term Canadian experience from the Biogen ONE™ support program. Mult Scler Relat Disord. 2022;67:104080.
Vermersch P, Suchet L, Colamarino R, Laurendeau C, Detournay B. An analysis of first-line disease-modifying therapies in patients with relapsing-remitting multiple sclerosis using the French nationwide health claims database from 2014–2017. Mult Scler Relat Disord. 2020;46:10252.
Devonshire V, Lapierre Y, Macdonell R, et al. The Global Adherence Project (GAP): a multicenter observational study on adherence to disease-modifying therapies in patients with relapsing-remitting multiple sclerosis. Eur J Neurol. 2011;18:69–77.
Menzin J, Caon C, Nichols C, White LA, Friedman M, Pill MW. Narrative review of the literature on adherence to disease-modifying therapies among patients with multiple sclerosis. J Manag Care Pharm. 2013;19(1 Suppl A):S24-40.
Moccia M, Loperto I, Lanzillo R, et al. Persistence, adherence, healthcare resource utilisation and costs for interferon beta in multiple sclerosis: a population-based study in the Campania region (southern Italy). BMC Health Serv Res. 2020;20:797.
Tan H, Cai Q, Agarwal S, et al. Impact of adherence to disease-modifying therapies on clinical and economic outcomes among patients with multiple sclerosis. Adv Ther. 2011;28:51–61.
Roche J, McCarry Y, Mellors K. Enhanced patient support services improve patient persistence with multiple sclerosis treatment. Patient Prefer Adher. 2014;8:805–11.
Acknowledgements
The authors thank all involved patients for their willingness to participate and the consent to use their health-related data in this study.
Medical Writing/Editorial Assistance
Medical writing assistance and editorial support was provided by Markus Fischer, PhD (Fischer BioMedical Wissenschaftskommunikation, Homburg/Saar, Germany) and funded by Merck Healthcare. Data management and statistical analysis was performed by Ecron Acunova GmbH, Konstanz, Germany and funded by Merck Healthcare.
Authorship
No tables, figures, images, or other material infringing the copyright of another publisher or individual are included in the manuscript. All coauthors are aware of the submission to this journal and agree to allow the corresponding author to serve as the primary correspondent with the editorial office and to review and sign off on the final proofs for publication. The authors whose names appear on the submission have contributed sufficiently to the manuscript (concept and planning of the work described; acquisition, analysis and interpretation of the data; drafting and/or critical revision of the manuscript; and approved the final submitted version of the manuscript) and, therefore, share collective responsibility and accountability for the manuscript. No deserving authors have been omitted from the authorship list. All persons who made substantial contributions to the manuscript but who do not fulfil the authorship criteria are listed with their specific contributions in the Acknowledgements section of the manuscript, and all persons named in the Acknowledgements section have given written permission to be named in the manuscript.
Funding
This research including the publication and rapid service fee was financially supported by Merck Healthcare Germany, Weiterstadt, Germany, (CrossRef Funder ID: https://doi.org/10.13039/100009945). The company did not fund any of the medications used during the study period.
Author information
Authors and Affiliations
Contributions
All authors were involved in developing the concept and design of the study, analysis and interpretation of the data, drafting of the paper and revising it critically for intellectual content. All authors read and approved the final version of manuscript to be published and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Conflict of Interest
Matthias Schwab has served on advisory boards for, and received funding for travel or speaker honoraria from Actelion-Janssen, Almirall, Bayer, Biogen, Bristol Myers Squibb, Celgene, Sanofi-Genzyme, Merck Healthcare, Novartis, Roche, and Teva, and received research support from Novartis and Bayer. Andrew Chan has served on advisory boards for, and received funding for travel or speaker honoraria from Actelion-Janssen, Almirall, Bayer, Biogen, Bristol Myers Squibb, Celgene, Sanofi-Genzyme, Merck Healthcare, Novartis, Roche, and Teva, all for hospital research funds; and research support from Biogen, Genzyme and UCB. Anna-Katharina Eser has no disclosures to declare. Boris-Alexander Kallmann has received honoraria for serving on advisory boards and as speaker from Merck Healthcare, Biogen, Genzyme, Teva, Roche, Novartis, Genesis Pharma, BMS, Janssen, Celgene, Biologix. Dieter Pöhlau has received speaking fees, travel support and financial support for research projects from Allmirall, Bayer, Biogen-Idec, Merck Healthcare, Octapharm, Novartis, Roche, Sanofi-Aventis and Teva. Joachim Richter is an employee of Merck Healthcare Germany, Weiterstadt, Germany. Torsten Wagner is an employee of Merck Healthcare Germany, Weiterstadt, Germany. Christoph Grothe has received speaking honoraria, travel compensations and fees for serving on advisory boards from Biogen, Merck Healthcare, Novartis, Sanofi, Roche, Boehringer Ingelheim, Teva as well as research grants from Novartis and Merck Healthcare.
Ethical Approval
Ethical approval was received from the Ethics Committee of the Faculty of Medicine of the Ruhr University Bochum, 44789 Bochum on 17 January 2013. In accordance with the legal provisions in Germany (§ 67 subsection 6 of the German Medicinal Products Act), the competent authority, i.e., the German Federal Institute for Drugs and Medical Devices, confirmed that this approval covered all study centers. The German Association of Statutory Health Insurance Physicians and the German Federal Associations of Health Insurance Funds were notified. The provided information included the places, time, monitoring plan, and aim of the non-interventional study, the names of the participating physicians, again covering all study sites. This study was performed in accordance with the Helsinki Declaration of 1964, and its later amendments. All patients provided informed consent (part of the ethic approval) to participate in the study.
Permissions
Permission for use of the Morisky Medication Adherence Scale was obtained from Morisky Medication Adherence Research, LLC.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Schwab, M., Chan, A., Eser, AK. et al. REBISTART: Adherence of Patients with Multiple Sclerosis to Treatment with Subcutaneous Interferon Beta in the Context of a Patient Support Program. Neurol Ther 13, 641–653 (2024). https://doi.org/10.1007/s40120-024-00593-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-024-00593-x