
Abstract
Introduction
Processing of emotional stimuli is altered in patients with depression. The present feasibility study investigated the features of emotional information recognition in people with depressive disorders and how these differ from individuals without depression to determine whether response times could potentially be used as a diagnostic marker to identify individuals at high risk of depression and as an indicator of antidepressant medication response.
Methods
The study recruited 32 individuals, 16 with single or recurrent depressive episodes and 16 control subjects without depression. Patients with depression received 8 weeks of antidepressant therapy. The severity of depressive symptoms at baseline and their changes on prescribed therapy were assessed using the Montgomery-Åsberg Depression Rating Scale (MADRS). The processing of emotional information was assessed using the computerized Penn Emotion Recognition Task (ER-40).
Results
The two groups were well matched in terms of age and gender. There was no difference between the groups in their ability to correctly recognize happy or sad emotional facial expressions, but the average time patients with depression took to recognize a happy face was significantly longer than controls. In addition, they were more likely to misinterpret facial expressions as non-emotional. In patients with depression, the mean MADRS total score decreased from 26.3 ± 4.4 at baseline to 11.1 ± 8.9 at 8 weeks, a reduction of 57.8%. The proportion of responders with greater than 50% reduction in their baseline MADRS total score was 64.3%. Antidepressive treatment was associated with a reduction in the mean time required for recognition of a happy face (P < 0.05).
Conclusions
Patients with depression are slower to identify positive emotions but have a similar time to recognition of negative emotions as patients without depression. The greater time required for recognition of happiness distinguished the patients with depression from control subjects, and was also the only parameter that showed an improvement with antidepressant therapy, suggesting a specific relationship of this parameter with the depressive state.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
This study examined the processing of emotional information in patients with depression and non-depressed control patients. |
Both groups correctly recognized positive and negative emotional facial expressions, but patients with depression took longer to recognize a happy face than controls did. |
Antidepressive treatment was associated with a reduction in the mean time required for recognition of a happy face. |
Studies are ongoing to determine whether changes in emotion recognition times may be used as a marker of treatment response in patients with depression. |
Digital Features
This article is published with digital features, including a summary slide, to facilitate understanding of the article. To view digital features for this article go to https://doi.org/10.6084/m9.figshare.12990791.
Introduction
Interest in cognitive impairment as a core feature of depressive disorders has increased over the last decade [1,2,3]. This relevance can be primarily explained by the conceptual view of depression as a disturbance of “affective cognition”, a term that describes the interaction between cognitive functions and emotions, including the processing of emotionally significant information in contexts that require cognitive appraisal to produce an appropriate response [4]. When affective cognition is disturbed there is distortion in the perception, processing, and synthesis of affective information, hampering interactions of a person with their surroundings [5].
The characteristics of affective cognition, including those found in depressive disorders, are studied using methods that identify the so-called hot cognitive processes. Despite some controversy over their theoretical significance [6], the division of cognitive functions into hot (emotional-affective) and cold (cognitive-deliberative) processes can be of practical value to assess methods of experimental study, rather than specific cognitive phenomena.
It is believed that tasks in which the stimuli are emotionally neutral and in which the test outcome is motivationally irrelevant evaluate the so-called cold cognitive functions. In contrast, hot cognitive functions are evaluated by the direct or indirect reactions of trial subjects to the presented emotionally significant stimuli (e.g., images or words). It should be noted that almost any cold test can be changed into a hot test by introducing some kind of motivational influence (reinforcement) [7].
Research is ongoing to determine the optimal experimental model for identifying cognitive impairments in depressive disorders, and both cold and hot research methods are being evaluated. Knowledge of the relative severity and reproducibility of the settings in which the cognitive tests are conducted will be important to allow identification of abnormalities characteristic or even specific for depressive disorders. These may then be used to identify diagnostic markers [8], as well as to determine goals and predictors for psychological and pharmacological treatment methods [9, 10].
Moreover, the mismatch of cognitive–emotional interactions in patients during depressive episodes and periods of remission, and compared with immediate relatives, can be a diagnostically relevant predisposing factor allowing the identification of persons at high risk of developing depression [11].
Numerous studies have reported that depression and depressed mood are associated with distortions of the processes of attention and perception when studied using hot methods. For example, studies using the emotional Stroop test have shown that patients with depression pay more attention to the negative content of words than to neutral or positive, while non-depressed individuals pay more attention to the positive content [12]. It has also been shown that patients with depression have difficulties recognizing positive facial expressions [13, 14], whereas their ability to detect negative faces is comparable to subjects without depression; people in general tend to recognize sad faces faster than joyful ones, among many neutral faces [14]. Impaired emotional cognition in depression may therefore be associated with a decrease or distortion in the processes of recognition of positive information rather than an increased susceptibility to negative information [15]. This has led to speculation that people with depression have difficulties distinguishing joyful faces, but no differences in the recognition of negative emotions compared to non-depressed subjects.
The present feasibility study was conducted to investigate the features of recognition of emotional information and, in particular, mimic expressions, by patients with depressive disorders with the aim of identifying features that could potentially be used as diagnostic indicators or markers of antidepressant treatment response.
Methods
This prospective, observational study recruited patients aged 18–60 years of both sexes, who were receiving outpatient, semi-inpatient, or inpatient treatment for single or recurrent depressive episodes without psychotic symptoms (defined by ICD-10 criteria), and had a score of at least 15 points on the Montgomery-Åsberg Depression Rating Scale (MADRS) [16].
A control group of subjects without depressive disorders was also recruited. The control group comprised volunteers recruited from the staff and students of Sechenov University, who were examined by a psychiatrist to rule out a diagnosis of depression, who were comparable to the patients with depression in age and gender, and who agreed to participate in the study. The absence of depression was confirmed both clinically during the interview and using the MADRS (less than 7 points). The study was conducted according to the criteria set by the declaration of Helsinki and was approved by the local ethics committee of the V.P. Serbsky National Medical Research Center of Psychiatry and Narcology, Moscow, Russia. Each subject provided signed, informed consent before participating in the study.
Exclusion criteria were the presence of psychotic symptoms and signs of bipolar affective disorder, as well as schizophrenia spectrum disorders; the presence of mental and behavioral disorders associated with the use of psychoactive substances; the presence of acute or exacerbated chronic neurological and somatic diseases; the state of disability; and women who were pregnant or lactating.
Patients were examined at baseline and after 8 weeks of antidepressant therapy and underwent clinical and psychopathological evaluation, assessment using psychometric scales, as well as psychodiagnostics. All patients took antidepressants at medium therapeutic doses, including amitriptyline, clomipramine, venlafaxine, mirtazapine, paroxetine, vortioxetine, and agomelatine, which were prescribed by their attending physicians in accordance with existing treatment standards for the treatment of depressive disorder. A variety of classes of antidepressants allowed us to evaluate the actual class-specific antidepressant effect as a whole, and not the effect of any particular drug or class of antidepressants. Patients receiving adjunctive psychopharmacy (e.g., atypical antipsychotics, normothymics) were not enrolled to avoid bias related to the action of such drugs. Some patients received short courses (3–4 days) of benzodiazepines at the initiation of treatment, but they were prescribed after initial study examination and discontinued at least 3–4 weeks before the second examination and emotion recognition testing.
The severity of depressive symptoms at baseline and their changes on prescribed therapy were assessed using the MADRS [16]. Treatment responders were those with a greater than 50% reduction in their baseline MADRS total score and treatment remitters were those with a score greater than 7 according to MADRS.
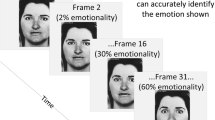
The processing of emotional information was assessed using the Penn Emotion Recognition Task (ER-40) from the Pennsylvania Computerized Neuropsychological Test Battery (PennCNP) [17]. This computerized test presents study participants with alternate images of 40 faces expressing happiness, sadness, anger, fear, and no emotion (eight images of each emotion of low and high intensity, four of which are represented by male and four by female faces). Subjects use the computer mouse to select on the monitor screen the most appropriate word to describe the emotion depicted in the image. Test results recorded include the number of correct and false positive answers, as well as the recognition time for emotional facial expressions. The length of time between baseline and follow-up was 8 weeks. The individuals were unaware of the correct and incorrect answers from the ER-40. Thus, as a result of the lack of direct feedback, the learning effect was minimized and the reliability of the study after a course of antidepressants was increased.
Statistical processing of the data was conducted using Microsoft Excel and MedCalc software. For variables with a normal distribution, one-way analysis of variance (ANOVA) was used to assess differences between independent groups, and for variables that did not follow a normal distribution the Mann–Whitney U test was used. Demographic characteristics such as gender and marital status were compared with the chi-squared test. Significant differences between dependent groups with a normal distribution were tested using the repeated measures ANOVA, while in groups without a normal distribution the Wilcoxon signed-rank test was used. Bonferroni correction for multiple comparisons was applied. The difference was considered statistically significant if the probability of random differences between the values was less than 5% (P < 0.05).
Results
The study recruited 32 individuals, 16 with depressive disorders and 16 healthy individuals who comprised the control group (Table 1). The control group was comparable in age and gender with the study group. The mean age of participants in the study and control groups was 37.9 ± 12.5 and 37.3 ± 11.7 years, respectively (p = 0.64). In both groups, the majority of participants were women (87.5% in the study group, and 81.3% among controls, difference not significant p = 0.87). There were no significant differences between the groups in terms of years of education (p = 0.73). Unmarried status was higher among patients with depression (56.3%) compared with control subjects (18.7%) (p = 0.046).
Among the patients with depression, more than half (10, 62.5%) were experiencing their first depressive episode, while 6 (37.5%) had recurrent depression. None of the patients had received therapy for past depressive episodes. The severity of the depressive symptoms was predominantly moderate: 14 patients had moderate depression and two had severe (the MADRS scores of the last two were, however, close to moderate at 35 and 37, respectively). The mean baseline MADRS total score was 26.3 ± 4.4 (moderate severity depression).
Analysis of emotional information processing revealed that patients with depression correctly recognized emotional facial expressions, with the same number of correct answers (around 80%) as subjects in the control group (Table 2). The average time that patients with depression spent on the recognition of emotions was greater compared with subjects in the control group, although this difference did not reach statistical significance.
There was no difference between groups in their ability to recognize emotions on female and male faces, nor in their ability to recognize low- and high-emotional intensity. In both groups, women’s faces and higher intensity expressions of emotion were recognized somewhat faster.
Correct emotion recognition was highest for happiness in both depressed and control subjects (at least 95% correct answers) and lowest for the recognition of anger (55–56% of correct answers). The rates of correct recognition of fear, sadness, and absence of emotion were 77–79%, 84–85%, and 80–86%, respectively, with no statistical differences between groups.
False positive recognition of anger was low in both groups (no more than 1.3% on average). In addition, rates of correct recognition of emotions were lowest for anger (Table 2). The data indicate that almost half of the face images expressing anger were either not recognized as emotional or mistakenly interpreted as fear or sadness in both groups.
Some differences between patients with depression and control individuals were also revealed. Although it did not reach statistical significance, patients with depression were more likely to misinterpret facial expressions as non-emotional. At the same time, patients with depression made significantly fewer mistakes in the recognition of sad facial expressions (P = 0.024). In cases of false positive recognition of sadness, patients with depression took on average significantly more time to make a decision than control subjects.
An important difference between the groups was noted in the time to emotion recognition, with patients with depression taking significantly more time on average to recognize a happy face even though their ability to correctly recognize happy faces was comparable to the control group.
During the course of the antidepressant therapy, two patients were lost to follow-up. In most of the remaining 14 patients, a significant reduction in severity of depressive symptoms was achieved at the end of the 8-week therapy. The mean MADRS total score decreased from 26.3 ± 4.4 at baseline to 11.1 ± 8.9 at 8 weeks, a reduction of 57.8%. The proportion of responders with greater than 50% reduction in their baseline MADRS total score was 64.3% (nine patients). Seven of these responders were also remitters (50% of follow-up depression group).
Despite the positive changes in depressive symptoms in most patients, the only parameter related to the processing of emotional information for which there was a statistically significant change from baseline was the mean recognition time for happy faces (P = 0.0028 with Bonferroni correction). By the end of the study, the mean recognition time for happy faces in patients with depression had approached the mean value in the control group. Changes in time of reaction to happy faces are shown in Table 3. It should be noted that improvement of happy face recognition was not associated with an overall improvement of cold cognition and reduction of lassitude. This was evident as there was no improvement in time of recognition to sad and no emotion faces (p = 0.16 and P = 0.86 with Bonferroni correction, respectively).
Interestingly, there was no statistically significant difference in mean change of reaction time between responders and non-responders (658 vs. 503 s, p = 0.387).
Parameters such as the number and time to false positive recognition of sadness were not sensitive to antidepressant treatment.
Discussion
From an evolutionary and adaptive perspective, mimic expressions of basic emotions are typical social signals that are automatically recognized and modify interpersonal behavior [18]. The ability to accurately recognize emotions is an important component of human ontogenesis that is formed in early childhood. Even a severe depressive state, in the absence of psychotic symptoms or impaired consciousness and intelligence, does not lead to the loss of this basic cognitive function.
In the present study, no differences were found between patients with depression and subjects without depression in either the total number of correctly recognized emotional and non-emotional faces or the number of low expressed emotions that are harder to recognize. These findings are consistent with the results of Douglas and Porter [19] that also revealed no statistically significant differences in the recognition of anger, happiness, sadness, or fear between patients with severe depression and control subjects.
It is of interest that compared with patients with depression, control individuals were significantly more likely to make mistakes in the recognition of sad faces. This finding suggests that the negativity bias (greater attention paid to negative emotions than to positive) that is often attributed to patients with depression is also observed in people without depression [20].
The only parameter improved during treatment was the response time to happy faces. However, this improvement was reported by both responders and non-responders. Two explanations can be put forward to explain this result. First, the finding could have been obtained as a result of the small sample size and the associated statistical error. Second, changing the reaction time to happy faces could be linked to some action of antidepressant therapy, which is necessary but not sufficient to achieve a response to therapy.
Study Limitations
The current study has several limitations including its small sample size and lack of a placebo group. Most of the patients included in the study were women, which reflects the fact that women are more likely to experience depression than men [21] and women with depression are generally more likely than men to turn to the psychiatric service for help [22, 23]. There was also a predominance of married persons in the depression group. The results of the study may therefore have limitations for extension to a general population. It is also possible that learning by repeating the same recognition tests may bias the contribution of antidepressant treatment, although this was not apparent in the present study. Consequently, further studies in a large cohort of patients are now warranted to assess how soon after treatment initiation changes in recognition times are observed, whether they are related to the response to therapy or reflect the patient's reaction to an antidepressant necessary but not sufficient to respond to therapy, and whether the reaction time can be used as a predictor of response to therapy.
Conclusions
The current study confirms that patients with depression are slower to identify positive emotions, but have a similar time to recognition of negative emotions as patients without depression. The greater time required for recognition of happiness distinguished the patients with depression from control subjects, and was also the only parameter that showed a positive improvement with antidepressant therapy, suggesting a specific relationship of this parameter with the depressive state. These findings may have important implications for the treatment of depression. For example, if time to recognition of positive emotions is related to the clinical effectiveness of treatment, this could be used as a potential predictor of therapeutic response as well as to tailor treatment to individual patients.
References
Krasnov VN, et al. Interrelations of cognitive and emotional disorders in depression. Doctor Ru. 2013;5(83):1–6 (Article in Russian).
Rock PL, Roiser JP, Riedel WJ, Blackwell AD. Cognitive impairment in depression: a systematic review and meta-analysis. Psychol Med. 2014;44(10):2029–40.
Shmukler AB. Cognitive impairment in the structure of the depressive syndrome. Soc Clin Psychiatr. 2016;26(1):72–6 (Article in Russian).
Elliott R, et al. Affective cognition and its disruption in mood disorders. Neuropsychopharmacology. 2011;36(1):153–82.
Balashova MV, et al. Peculiarities of processing emotional information in patients with depressive disorders. Zh Nevrol Psikhiatr Im S S Korsakova. 2018;118(8):11–7 (Article in Russian).
Gladwin TE, Figner B. “Hot” cognition and dual systems: introduction, criticisms, and ways forward. In: Wilhelms EA, Reyna VF, editors. Neuroeconomics, judgment, and decision making. New York: Psychological Press; 2014. p. 157–80.
Roiser JP, Sahakian BJ. Hot and cold cognition in depression. CNS Spectr. 2013;18(03):139–49.
Clark L, et al. Neurocognitive mechanisms in depression: implications for treatment. Annu Rev Neurosci. 2009;32:57–74.
Roiser JP, et al. Cognitive mechanisms of treatment in depression. Neuropsychopharmacology. 2012;37(1):117–36.
Bortolato B, Miskowiak KW, Kohler CA, et al. Cognitive remission: a novel objective for the treatment of major depression? BMC Med. 2016;14:19.
Hasler G, Drevets WC, Manji HK, Charney DS. Discovering endophenotypes for major depression. Neuropsychopharmacology. 2004;29(10):1765–81.
Epp AM, Dobson KS, Dozois DJ, Frewen PA. A systematic meta-analysis of the Stroop task in depression. Clin Psychol Rev. 2012;32(4):316–28.
Mikhailova ES, Tsutsulkovskaya MY, Oleichik IV. Neurophysiological mechanisms of impaired recognition of emotions in endogenous depression. Zh Nevrol Psikhiatr Im S S Korsakova. 2000;1:38–43.
Suslow T, Junghanns K, Arolt V. Detection of facial expressions of emotions in depression. Percept Mot Skills. 2001;92(3 Pt 1):857–68.
Gotlib IH, Joormann J. Cognition and depression: current status and future directions. Annu Rev Clin Psychol. 2010;6:285–312.
Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382–9.
Gur RC, Sara R, Hagendoorn M, et al. A method for obtaining 3-dimensional facial expressions and its standardization for use in neurocognitive studies. J Neurosci Methods. 2002;115(2):137–43.
Bourke C, Douglas K, Porter R. Processing of facial emotion expression in major depression: a review. Aust NZ J Psychiatry. 2010;44:681–96.
Douglas KM, Porter RJ. Recognition of disgusted facial expressions in severe depression. Br J Psychiatry. 2010;197(2):156–7.
Vaish A, Grossmann T, Woodward A. Not all emotions are created equal: the negativity bias in social-emotional development. Psychol Bull. 2008;134(3):383–403.
Girgus JS, Yang K, Ferri CV. The gender difference in depression: are elderly women at greater risk for depression than elderly men? Geriatrics. 2017;2:35.
Wang PS, Lane M, Olfson M, Pincus HA, Wells KB, Kessler RC. Twelve-month use of mental health services in the United States: results from the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):629–40.
Smith KL, Moinedding R, Dunn JR, Lu H, Cairney J, Glazier RH. Gender differences in mental health service utilization among respondents reporting depression in a natinal health survey. Health (NY). 2013;5(10):1561–71.
Acknowledgements
The authors thank all the participants of the study.
Funding
This study and the journal’s rapid service fee was funded by Servier.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Medical Writing and Editorial Assistance
Writing assistance was provided by Jenny Grice, a freelance medical editor, and funded by Servier.
Disclosures
Roman Vitalievich Akhapkin, Beatrisa Albertovna Volel, Rodion Mikhailovich Shishorin, Dmitry Vladimirovich Ustyuzhanin and Dmitry Sergeevich Petelin have nothing to disclose.
Compliance with Ethics Guidelines
The study was conducted according to the criteria set by the declaration of Helsinki and was approved by the local ethics committee of the V.P. Serbsky National Medical Research Center of Psychiatry and Narcology, Moscow, Russia. Each subject provided signed, informed consent before participating in the study.
Data Availability
The datasets generated and/or analyzed for this study are available in the PennCNP repository: https://penncnp.med.upenn.edu/penncnp.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Akhapkin, R.V., Volel, B.A., Shishorin, R.M. et al. Recognition of Facial Emotion Expressions in Patients with Depressive Disorders: A Prospective, Observational Study. Neurol Ther 10, 225–234 (2021). https://doi.org/10.1007/s40120-021-00231-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-021-00231-w