
Abstract
Purpose
Ureaplasma urealyticum is a rare pathogen associated with septic arthritis that predominantly affects patients with hypogammaglobulinemia. Bacterial identification of fastidious organisms is challenging because they are undetectable by routine culture testing. To the best of our knowledge, this is the first report of septic arthritis induced by U. urealyticum infection in Japan.
Case description
We describe the case of a 23-year-old Japanese female with secondary hypogammaglobulinemia (serum immunoglobulin level < 500 mg/dL), identified 8 years after treatment with rituximab. The patient presented with persistent fever and polyarthritis that were unresponsive to ceftriaxone and prednisolone. Contrast-enhanced computed tomography and gallium-67 scintigraphy revealed effusion and inflammation in the left sternoclavicular, hip, wrist, knee, and ankle joints. Although Gram staining and bacterial culture of the drainage fluid from the left hip joint were negative, the condition exhibited characteristics of purulent bacterial infection. The patient underwent empirical treatment with doxycycline, and her symptoms promptly resolved. Subsequent 16S ribosomal RNA (rRNA) gene sequencing of the joint fluid confirmed the presence of U. urealyticum, leading to the diagnosis of septic arthritis. Combination therapy with doxycycline and azithromycin yielded a favorable recovery from the inflammatory status and severe arthritic pain.
Conclusion
This case highlights U. urealyticum as a potential causative agent of disseminated septic arthritis, particularly in patients with hypogammaglobulinaemia. The 16S rRNA gene analysis proved beneficial for identifying pathogens in culture-negative specimens, such as synovial fluid, in suspected bacterial infections.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Members of the family Mycoplasmataceae, including Ureaplasma and Mycoplasma species, colonize the human genitourinary tract. Ureaplasma spp. can be isolated from cervical and vaginal secretions, ranging from 31.2 to 72.1% among fertile females and from 72.3 to 80% among pregnant females [1, 2], possibly causing non-gonococcal urethritis, prostatitis, gynecological diseases, and infertility [3, 4]. The diagnosis of Ureaplasma infections without clinical suspicion is challenging because these organisms are untraceable by both Gram staining and bacterial culture [3]. Ureaplasma species may also cause extragenital and disseminated infections in immunocompromised patients, such as those with hypogammaglobulinemia [5], hematologic malignancies [6], and solid organ transplantation [7]. Septic arthritis caused by Ureaplasma spp., although rare, has been documented in patients with hypogammaglobulinemia [5]. Rituximab, an anti-CD20 chimeric monoclonal antibody, is associated with secondary hypogammaglobulinemia [8]. A recent case of U. urealyticum septic arthritis has been reported in a patient who developed hypogammaglobulinemia after rituximab therapy [5]. Although the diagnosis is difficult, 16S ribosomal RNA (rRNA) sequencing is used to detect Ureaplasma species [9]. PCR testing for 16S rRNA is an effective method for identifying pathogens that are undetectable by routine microbiological testing [10, 11]. Nevertheless, 16S rRNA gene analysis is not commonly used in Japan, and its clinical use remains limited. To the best of our knowledge, no case of Ureaplasma septic arthritis has been reported in Japan.
Herein, we present a case of septic arthritis caused by U. urealyticum, successfully diagnosed using 16S rRNA gene sequencing in a patient previously treated with rituximab for nephrotic syndrome.
Case report
A 23-year-old Japanese female was referred to our department for fever and polyarthritis. Approximately 8 years prior to this presentation, the patient had undergone four cycles of rituximab for glucocorticoid-resistant nephrotic syndrome. Two months prior, she had been hospitalized for empyema and underwent surgical debridement; however, the pathological and microbiological etiologies remained unclear. Subsequently, she developed fever and polyarthritis affecting the elbow, shoulder, hip, wrist, and ankle joints. At the previous hospital, ceftriaxone and 30 mg/day of prednisolone were initiated for suspected septic and reactive arthritis; however, her symptoms did not improve, and she became bedridden because of severe joint pain.
Upon admission, she was alert and her vital signs were stable, except for fever. Physical examination revealed severe tenderness of the left wrist, left sternoclavicular joint, left ankle joint, and both hip joints. Laboratory testing demonstrated an elevation in white blood cell count (20,920/µL) and serum C-reactive protein (CRP, 23.36 mg/dL). Serum levels of IgG, IgA, and IgM decreased to 243.3 mg/dL (normal range, 861.0–1747 mg/dL), 20.4 mg/dL (normal range, 93.0–393.0 mg/dL), and < 2.0 mg/dL (normal range, 50.0–269.0 mg/dL), respectively, leading to a diagnosis of hypogammaglobulinemia, for which we promptly initiated immunoglobulin replacement therapy. Both antinuclear and antineutrophil cytoplasmic antibodies tested negative. Immunoglobulin levels were confirmed to be within normal limits before receiving rituximab.
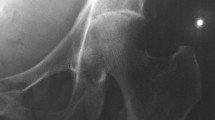
Contrast-enhanced computed tomography (CT) revealed effusions in the left sternoclavicular and bilateral hip joints (Fig. 1A, B). Gallium-67 scintigraphy revealed uptake in the left sternoclavicular, hip, wrist, knee, and ankle joints (Fig. 1C). CT-guided drainage of the left hip joint detected yellowish, cloudy joint fluid, with an increased cell count (60,000/µL) showing a predominance of polynuclear cells (99%) over mononuclear cells (1%). Despite these findings, Gram staining and bacterial culture of the joint fluid did not reveal any pathogens. While, we observed a positive testing result for alpha-defensin lateral flow tests (Synovasure® lateral flow test; Zimmer Biomet, IN, USA) in synovial fluid of both hips.

Radiological findings A, B Contrast-enhanced computed tomography showing effusions in the left sternoclavicular and both hip joints. C Gallium-67 scintigraphy demonstrating uptakes in bilateral wrist, knee, ankle joints, and large joints. D Magnetic resonance imaging of the hips detecting bone marrow edema along with fluid retention bilaterally
Suspecting septic arthritis caused by atypical organisms, treatment with 200 mg doxycycline (DOXY) daily was initiated. Following antibiotic therapy, the joint symptoms and serum C-reactive protein (CRP) levels improved (Fig. 2). Although clinically effective, DOXY therapy was switched to 500 mg/day levofloxacin (LVFX) because of DOXY-induced gastritis, as confirmed using gastroendoscopy. Soon after, the serum CRP level was elevated during LVFX therapy, accompanied by severe joint tenderness, suggesting LVFX resistance. We then switched to oral DOXY therapy. Gastric symptoms recurred, and DOXY was converted to intravenous minocycline.

The clinical course of the patient Serum C-reactive protein levels decreased following DOXY therapy and resurged after switching to LVFX. Combination therapy with DOXY (MINO) and AZM was effective, and the patient was discharged with AZM monotherapy. PSL prednisolone; CRP C-reactive protein; IVIG intravenous immunoglobulin; DOXY doxycycline; MINO minocycline; LVFX levofloxacin; AZM azithromycin
Around that time, we performed an in-house two-step PCR for the 16S rRNA gene to accurately identify the causative organism. DNA was isolated from hip joint fluid using the DNeasy® PowerSoil Pro Kit (QIAGEN). The 16S rRNA gene was amplified with 8UA and 1485B primers (forward primer: 5′-AGAGTTTGATCMTGGCTCAG-3′; reverse primer: 5′-TACGGTTACCTTGTTACGAC-3′). PCR was performed using the following regimen: 98 °C for 3 min followed by 45 cycles at 98 °C for 4 s, 60 °C for 30 s, 72 °C for 1 min, and a final extension at 72 °C for 5 min (ramp rate = 1 °C/s). The second PCR was carried out with 341A and 519B primers (forward primer: 5′-CTACGGGAGGCAGCAGTGGG-3′, and reverse primer: 5′-ATTACCGCGGCKGCTG-3′) under a following amplification process: 96 °C for 1 min, followed by 25 cycles at 96 °C for 10 s, 50 °C for 5 s, 60 °C for 1 min (ramp rate = 1 °C/s). The sequence data of the PCR products were analyzed using the Basic Local Alignment Search Tool (BLAST), and the isolate was identified as U. urealyticum with a 100% concordance rate with the reference strain (GenBank accession number: NR_041710.1).
Under the diagnosis of disseminated arthritis caused by U. urealyticum, we added oral azithromycin (500 mg for 3 days, followed by 250 mg/day) as combination therapy to prevent the emergence of antimicrobial resistance. Magnetic resonance imaging revealed bilateral joint effusions, bone marrow edema in both hip joints (Fig. 1D) and fluid retention in the ankle joints. Thereafter, arthroscopic irrigation and debridement of both hip joints were performed 63 days after admission. During hospitalization, the patient remained bedridden because of severe joint tenderness, even after intravenous fentanyl therapy. Combination therapy with antibiotics and surgical intervention led to an improvement in her fever and polyarthritis. Intravenous minocycline was discontinued and the patient was discharged in good condition on oral azithromycin, with plans to continue antibiotic treatment for several months.
Discussion
Ureaplasma joint infection is a rare entity, predominantly reported in patients with hypogammaglobulinemia [5, 9, 12, 13]. Although patients with Ureaplasma joint infections often present with preceding urogenital infections, there were no prior infectious episodes in this case. Instead, the patient experienced an empyema episode of unknown etiology. Ureaplasma rarely causes respiratory infections [14], and it remains uncertain whether the fastidious pathogen was responsible for the empyema observed in the present case.
Ureaplasma species are difficult to detect using routine assays, and PCR testing is often used to identify these organisms [15]. Although PCR testing for Ureaplasma species is commercially available for urine specimens in Japan, no equivalent commercial tests exist for other types of specimens such as joint fluids. The absence of testing options complicates the diagnosis of joint infections caused by Ureaplasma species. In this case, the alpha-defensin, a synovial fluid biomarker used for diagnosing periprosthetic joint infection, tested positive, having supported our presumptive diagnosis of bacterial infection [16]. Sequencing of the 16 s rRNA gene, which is ubiquitously present in bacteria, is a critical tool for identifying difficult-to-culture organisms [10]. There have been several reports on Ureaplasma detection using 16S rRNA gene analysis [15, 17, 18]. Given that only a limited number of medical facilities can perform the 16 s rRNA gene analysis, it is crucial to collect and preserve specimens from the infection site before initiating empiric therapy.
Ureaplasma species are generally susceptible to antibiotics such as tetracyclines, fluoroquinolones, and macrolides [13]. In a study of 48 clinical isolates of U. urealyticum from the United States, all isolates were susceptible to tetracyclines and macrolides, whereas resistance to LVFX was observed in 5.2% of the cases [19]. In contrast, in China, the resistance rate of U. urealyticum to LVFX ranges between 60 and 82% [2, 4], indicating significant geographical variation in resistance patterns. In our case, the clinical deterioration following the switch from DOXY to LVFX implied the presence of an LVFX-resistant strain. The optimal treatment duration for joint infections caused by Ureaplasma remains unknown. Nevertheless, we considered that an extended treatment period of several months may have been preferable in the present case, as evidenced by the relapse in a patient following a 6-week treatment regimen [13].
Hypogammaglobulinemia can be classified into primary and secondary types. Most secondary hypogammaglobulinemia cases are associated with B cell-targeted therapies, such as rituximab [20]. The incidence of rituximab-associated hypogammaglobulinemia requiring immunoglobulin replacement therapy has been reported to be 6.6% in patients with lymphoma and 14–21% in those with ANCA-associated vasculitis [21]. The median interval between initial rituximab administration and onset of hypogammaglobulinemia was 18 months, and the prevalence of hypogammaglobulinemia reportedly ranged from 13–17% during an observation period of up to 60 months [22]. In the present case, the patient’s immunoglobulin levels were within the normal range before rituximab administration, suggesting a low likelihood of primary hypogammaglobulinemia. However, the onset of hypogammaglobulinemia was not determined because immunoglobulin levels were not monitored after rituximab administration. Severe hypogammaglobulinemia was diagnosed in this patient 8 years after the last rituximab administration. It is advisable to examine immunoglobulin levels after B cell-targeted therapy and administer immunoglobulin replacement therapy as needed [21].
Here, we present a case of U. urealyticum disseminated arthritis in an immunocompromised patient with hypogammaglobulinemia. We highlighted that 16S rRNA gene analysis is a valuable tool for the diagnosis of culture-negative infections.
Data availability
No datasets were generated or analysed during the current study
References
Capoccia R, Greub G, Baud D. Ureaplasma urealyticum, Mycoplasma hominis and adverse pregnancy outcomes. Curr Opin Infect Dis. 2013;26:231–40.
Wang QY, Li RH, Zheng LQ, Shang XH. Prevalence and antimicrobial susceptibility of Ureaplasma urealyticum and Mycoplasma hominis in female outpatients, 2009–2013. J Microbiol Immunol Infect. 2016;49:359–62.
Kokkayil P, Dhawan B. Ureaplasma: current perspectives. Indian J Med Microbiol. 2015;33:205–14.
Yang T, Pan L, Wu N, Wang L, Liu Z, Kong Y, et al. Antimicrobial resistance in clinical Ureaplasma spp. and Mycoplasma hominis and structural mechanisms underlying quinolone resistance. Antimicrob Agents Chemother. 2020;64:e02560.
El Zein S, Garvey T, Amin S, Tande AJ. Native joint polyarticular septic arthritis secondary to disseminated Ureaplasma urealyticum infection in a patient on rituximab therapy with hypogammaglobulinemia: a case report. IDCases. 2023;32: e01744.
Balsat M, Galicier L, Wargnier A, Pereyre S, Itzykson R, Zouakh M, et al. Diagnosis of Ureaplasma urealyticum septic polyarthritis by PCR assay and electrospray ionization mass spectrometry in a patient with acute lymphoblastic leukemia. J Clin Microbiol. 2014;52:3456–8.
Cannon CA, Corcorran MA, Shaw KW, Montenovo M, Sibulesky L, Reyes JD, et al. Hyperammonemia syndrome due to Ureaplasma infection after liver-kidney transplant. Transpl Infect Dis. 2020;22: e13298.
Roberts DM, Jones RB, Smith RM, Alberici F, Kumaratne DS, Burns S, et al. Rituximab-associated hypogammaglobulinemia: incidence, predictors and outcomes in patients with multi-system autoimmune disease. J Autoimmun. 2015;57:60–5.
George MD, Cardenas AM, Birnbaum BK, Gluckman SJ. Ureaplasma septic arthritis in an immunosuppressed patient with juvenile idiopathic arthritis. J Clin Rheumatol. 2015;21:221–4.
Clarridge JE 3rd. Impact of 16S rRNA gene sequence analysis for identification of bacteria on clinical microbiology and infectious diseases. Clin Microbiol Rev. 2004;17:840–62.
Rampini SK, Bloemberg GV, Keller PM, Büchler AC, Dollenmaier G, Speck RF, et al. Broad-range 16S rRNA gene polymerase chain reaction for diagnosis of culture-negative bacterial infections. Clin Infect Dis. 2011;53:1245–51.
MacKenzie CR, Nischik N, Kram R, Krauspe R, Jäger M, Henrich B. Fatal outcome of a disseminated dual infection with drug-resistant Mycoplasma hominis and Ureaplasma parvum originating from a septic arthritis in an immunocompromised patient. Int J Infect Dis. 2010;14:e307–9.
Harold R, Simon GL, Akselrod H, Siegel MO, Roberts A. Ureaplasma septic polyarthritis in a young woman with neuromyelitis optica receiving rituximab. BMJ Case Rep. 2021;14: e237916.
Canouï E, Blanc K, Loubinoux J, Valade S, Hamard C, Lefebvre A, et al. The value of molecular techniques to diagnose Ureaplasma urealyticum and Nocardia farcinica pleuropneumonia in a patient with diffuse large B-cell lymphoma. Int J Infect Dis. 2017;64:93–5.
Suárez-Cuervo C, Nicolás C, Fernández-Suárez J, Morilla A, Fernández J, Caminal-Montero L. Ureaplasma parvum septic arthritis, a clinic challenge. Diagnostics (Basel). 2022;12:2416.
Frangiamore SJ, Gajewski ND, Saleh A, Farias-Kovac M, Barsoum WK, Higuera CA. α-Defensin accuracy to diagnose periprosthetic joint infection-best available test? J Arthroplasty. 2016;31:456–60.
Rouard C, Pereyre S, Abgrall S, Guillet-Caruba C, Diviné P, Bourgeois-Nicolaos N, et al. Early prosthetic joint infection due to Ureaplasma urealyticum: benefit of 16S rRNA gene sequence analysis for diagnosis. J Microbiol Immunol Infect. 2019;52:167–9.
Ball ND, Snape SE. Periprosthetic joint infection with Ureaplasma parvum detected by 16S rRNA PCR. BMJ Case Rep. 2021;14: e239858.
Fernández J, Karau MJ, Cunningham SA, Greenwood-Quaintance KE, Patel R. Antimicrobial susceptibility and clonality of clinical ureaplasma isolates in the United States. Antimicrob Agents Chemother. 2016;60:4793–8.
Otani IM, Lehman HK, Jongco AM, Tsao LR, Azar AE, Tarrant TK, et al. Practical guidance for the diagnosis and management of secondary hypogammaglobulinemia: a work group report of the aaaai primary immunodeficiency and altered immune response committees. J Allergy Clin Immunol. 2022;149:1525–60.
Wijetilleka S, Jayne DR, Mukhtyar C, Ala A, Bright PD, Chinoy H, et al. Recommendations for the management of secondary hypogammaglobulinaemia due to B cell targeted therapies in autoimmune rheumatic diseases. Rheumatology (Oxford). 2019;58:889–96.
Marco H, Smith RM, Jones RB, Guerry MJ, Catapano F, Burns S, et al. The effect of rituximab therapy on immunoglobulin levels in patients with multisystem autoimmune disease. BMC Musculoskelet Disord. 2014;15:178.
Acknowledgements
We would like to thank Editage (www.editage.jp) for English language editing.
Funding
Open Access funding provided by Okayama University.
Author information
Authors and Affiliations
Contributions
KO drafted the manuscript. SF and HH revised it. YO, YS, MK, YS, NU, and KY directly contributed to the patient care. TF and KI were responsible for the microbiological testing. FO supervised the case. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest.
Consent for publication
Written informed consent for publication was obtained from the patient.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Oguni, K., Fukushima, S., Otsuka, Y. et al. Disseminated septic arthritis caused by Ureaplasma urealyticum in an immunocompromised patient with hypogammaglobulinemia after rituximab therapy. Infection (2024). https://doi.org/10.1007/s15010-024-02301-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s15010-024-02301-1