
Abstract
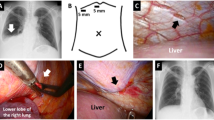
A 74-year-old woman with reduced kidney and cardiac function and a history of coronary artery bypass surgery involving the gastroepiploic artery to the right coronary artery and posterior descending artery #4 presented with dyspnea on exertion. Shortly after the induction of peritoneal dialysis (PD), an increase in the left pleural effusion was observed, and a diagnosis of left pleuroperitoneal communication was made by puncture drainage. The pleuroperitoneal communication hole was not detected under thoracoscopic observation; however, a 10 mm-sized hole in the pericardium was found, confirming leakage of ICG-loaded peritoneal dialysate fluid (PDF). CT peritoneography using PDF mixed with iodine contrast medium revealed that the gastroepiploic artery-to-right coronary artery pathway was defective on the abdominal side. We concluded that the left pleuroperitoneal communication was caused by a two-stage fistulous pathway between the abdominal and pleural cavities through the pericardial cavity after coronary artery bypass graft surgery. Although closure of the diaphragmatic hole around the gastroepiploic artery graft should have been performed to restart PD, the patient did not wish to undergo further invasive procedures. Identification of the fistulous pathway is extremely important for prompt diagnosis and treatment of pleuroperitoneal communication.




Similar content being viewed by others


References
Li PKT, Chow KM, Van de Luijtgaarden MWM, et al. Changes in the worldwide epidemiology of PD. Nat Rev Nephrol. 2017;13(2):90–103.
Chow KM, Szeto CC, Li PKT. Management options for hydrothorax complicating PD. Semin Dial. 2003;16(5):389–94.
Nomoto Y, Suga T, Nakajima K, et al. Acute hydrothorax in continuous ambulatory PD–a collaborative study of 161 centers. Am J Nephrol. 1989;9(5):363–7.
Matsuoka N, Yamaguchi M, Asai A, et al. The effectiveness and safety of computed tomographic peritoneography and video-assisted thoracic surgery for hydrothorax in PD patients: a retrospective cohort study in Japan. PLoS One. 2020;15(9): e0238602.
Shishido T, Ryuzaki M, Takimoto C, et al. A case of recurrent hydrothorax complicating continuous ambulatory peritoneal dialysis after video-assisted thoracoscopic surgery. J Jpn Soc Dial Ther. 2010;43(10):873–9.
Gil C, Ramos SR, Antonia AM. Scintigraphy of the intraperitoneal cavity using technitium 99m: a diagnostic technique for diaphragmatic leaks in peritoneal dialysis regarding two cases. Nephrologia. 2009;29:263–5.
Kawakita N, Takizawa H, Kajiura K, Tangoku A. Indocyanine green fluorescence intraoperative imaging for hepatic hydrothorax with a small diaphragmatic defect. Semin Thorac Cardiovasc Surg. 2016;28(2):606–8.
Manabe T, Ono K, Oka S, Kawamura Y, Osaki T. A case of pleuroperitoneal communication in which establishing a laparoscopic pneumoperitoneum was useful for the detection of a fistula. Surg Case Rep. 2021;7(1):64.
Borzych D, Ley S, Schaefer F, et al. Dialysate leakage into pericardium in an infant on long-term PD. Pediatr Nephrol. 2008;23(2):335–8.
Teoh CW, Nadel H, Armstrong K, Harris KC, White CT. Peritoneal-pericardial communication in an adolescent on PD. Pediatr Nephrol. 2016;31(1):153–6.
Hou CH, Tsai TJ, Hsu KL. Peritoneopericardial communication after pericardiocentesis in a patient on continuous ambulatory PD with dialysis pericarditis. Nephron. 1994;68(1):125–7.
Näther S, Anger H, Koall W, et al. Peritoneal leak and chronic pericardial effusion in a CAPD patient. Nephrol Dial Transplant. 1996;11(6):1155–8.
Ungureanu C, Laruelle C, Pieters D, et al. Compression of the right ventricle by the liver through a diaphragmatic hernia after right gastroepiploic artery coronary bypass grafting. Acta Cardiol. 2013;68(6):647–9.
Takiuchi H, Totsugawa T, Tamaki T, Kuinose M, Yoshitaka H, Tsusima Y. Intrapericardial diaphragmatic hernia after coronary artery bypass grafting using the right gastroepiploic artery graft: report of a case. Ann Thorac Cardiovasc Surg. 2011;17(6):624–7.
Verhofste MA, Tam SK. Diaphragmatic hernia after right gastroepiploic artery coronary artery bypass grafting. Ann Thorac Surg. 1995;60(2):458–9.
Pasic M, Carrel T, Von Segesser L, Turina M. Postoperative diaphragmatic hernia after use of the right gastroepiploic artery for coronary artery bypass grafting. J Thorac Cardiovasc Surg. 1994;108(1):189–91.
Ansari M, Eucher P, De Canniere L. Strangulated giant transdiaphragmatic hernia: a rare complication of coronary artery bypass grafting with the right gastroepiploic artery. J Thorac Cardiovasc Surg. 2002;123(2):358–9.
Acknowledgements
We would like to thank Editage (www.editage.jp) for English language editing.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Ethical approval
All procedures involving human participants performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from an individual participant included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Nakamura, E., Sofue, T., Higashitani, M. et al. A case of a peritoneal dialysis patient with left pleuroperitoneal communication caused by a pericardial defect after coronary artery bypass surgery. CEN Case Rep (2024). https://doi.org/10.1007/s13730-024-00867-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s13730-024-00867-1