
Abstract
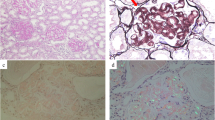
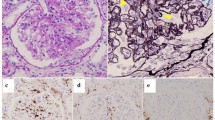
Fibrillary glomerulonephritis (FGN), a rare disease is pathologically characterized by glomerular fibril accumulation ranging from 12 to 24 nm in diameter with negative Congo red staining. Recently, the identification of DnaJ homolog subfamily B member 9 (DNAJB9) as a highly sensitive and specific marker for FGN has revolutionized diagnosis of this disease. However, few recent studies have reported DNAJB9-negative glomerulonephritis with fibrillar deposits. As such, it remains unclear whether DNAJB9-negative cases can be considered equivalent to FGN. Here, we report the case of a 70-year-old woman who developed renal impairment and nephrotic-range proteinuria. Renal biopsy and pathological examination revealed focal glomerulonephritis with fibrocellular crescents. Immunofluorescence microscopy showed IgA-dominant deposition of polytypic IgG in the glomerulus. Electron microscopy revealed hump-like subepithelial electron dense deposits with fibrils of 15–25 nm in diameter. These findings were consistent with FGN; thus, Congo red and direct fast scarlet (DFS) staining, and immunohistochemistry for DNAJB9 were performed. In addition to negative Congo red/DFS/DNAJB9 staining, laser microdissection (LMD) and liquid chromatography-tandem mass spectrometry (LC–MS/MS) resulted negative for DNAJB9, which is a highly sensitive and specific marker for FGN. The patient’s renal function further declined, prompting administration of rituximab weekly for 2 weeks, similar to the treatment for FGN. This is a unique case of IgA-dominant glomerulonephritis with DNAJB9-negative fibrillar polytypic immunoglobulin deposits in the subepithelium, unlike previous DNAJB9-negative cases. Thus, DNAJB9-negative cases diagnosed based on accurate electron microscopic evaluation must be gathered, and LMD and LC–MS/MS must be used to analyze the organized fibrillar deposits to reveal the disease entity.





Similar content being viewed by others

Data availability
The data generated and/or analyzed during the current case report are available from the corresponding author on reasonable request.
References
Andeen NK, et al. Fibrillary glomerulonephritis clinicopathologic features and atypical casese from a multi-institutional cohort. Clin J Am Soc Nephrol. 2019;14:1741–50.
Rosenstock JL, et al. Fibrillary and immunotactoid glomerulonephritis: disintc entities with different clinical and pathologic features. Kidney Int. 2003;63:1450–61.
Javaugue V, et al. Long-term kidney disease outcomes in fibrillary glomerulonephritis: a case series of 27 patients. Am J Kidney Dis. 2013;62:679–90.
Nasr SH, et al. DNAJB9 is a specific immunohistochemical marker for fibrillary glomerulonephritis. Kidney Int Rep. 2018;3:56–64.
Dasari S, et al. DnaJ heat shock protein family B member 9 is a novel biomarker for fibrillary GN. J Am Soc Nephrol. 2018;29:51–6.
Andeen NK, et al. DnaJ homolog subfamily B member 9 is a putative autoantigen in fibrillary GN. J Am Soc Nephrol. 2018;29:231–9.
Nasr SH, et al. Heavy chain fibrillary glomerulonephritis: a case report. Am J Kidney Dis. 2019;74:276–80.
Alexander MP, et al. Congophilic fibrillary glomerulonephritis: a case series. Am J Kidney Dis. 2018;72:325–36.
Kudose S, et al. Diagnostic approach to glomerulonephritis with fibrillar IgG deposits and light chain restriction. Kidney Int Rep. 2021;6:936–45.
Nasr SH, et al. Fibrillary glomerulonephritis: a report of 66 cases from a single institution. Clin J Am Soc Nephrol. 2011;6:775–84.
Said SM, et al. Characteristics of patients with coexisting DNAJB9-associated fibrillary glomerulonephritis and IgA nephropathy. Clin Kidney J. 2021;14:1681–90.
Acknowledgements
We are grateful to Yuriko Sawa, Norihiko Suzuki, Ryoko Sakamoto, and Naoko Asano for their excellent technical assistance. We would like to thank Editage (www.editage.com) for the English language editing.
Funding
The authors declare no relevant financial support.
Author information
Authors and Affiliations
Contributions
RM and KM were responsible for the manuscript, interpretation of data, and writing of this paper. The patient was attended by SF. SS, KN, KT, and SM participated in composing the manuscript and providing advice for the concept. All the authors were involved in drafting, reviewing, and approving the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All the authors have declared no competing interest.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the Institutional and National Research Committee at which the studies were conducted with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent for publication
Written informed consent for the publication of this report was obtained from the patient.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Muto, R., Maeda, K., Fukui, S. et al. IgA-dominant glomerulonephritis with DNAJB9-negative fibrillar polytypic immunoglobulin deposits in the subepithelium. CEN Case Rep 12, 323–328 (2023). https://doi.org/10.1007/s13730-022-00759-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13730-022-00759-2