
Abstract
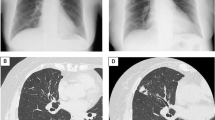
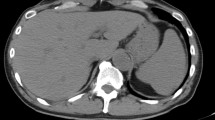
Glomerulonephritis in tuberculosis may be a direct manifestation of renal infection or a result of immune-complex deposition complicating extra-renal infection, such as in pulmonary tuberculosis. A 17-year-old adolescent boy from Somalia was found to have pulmonary tuberculosis during routine health screening performed on entering Malta, with computed tomography of the chest showing scarring and calcification of the left upper lobe, left lower lobe consolidation, and a small left-sided pleural effusion. Five days after starting anti-tuberculous therapy, he developed lower limb and sacral oedema: urinary albumin: creatinine ratio was > 400 µg albumin/mg creatinine, and 24-h urinary protein showed nephrotic-range proteinuria of 4.963 g/day. In view of worsening lower limb, sacral and periorbital oedema and ascites, he was started on oral prednisolone, omeprazole and penicillin V prophylaxis. As heavy proteinuria persisted, a renal biopsy was performed after 8 days of prednisolone treatment, which confirmed the presence of mesangiocapillary glomerulonephritis (MCGN), with electron microscopy showing effacement of the podocytes, with hypercellularity and subendothelial immune deposits, confirming an immune-mediated pathophysiology. Ziehl–Neelsen staining did not reveal acid-fast organisms. The patient received a total of 3 weeks of oral prednisolone with subsequent tailing doses, 2 months of pyrazinamide and ethambutol and 6 months of rifampicin and isoniazid with complete resolution of his clinical and radiological signs, though heavy proteinuria persisted, so he was commenced on oral enalapril. This case highlights the potential association of MCGN with tuberculosis in adolescence. Timely recognition and treatment can prevent progression to chronic kidney disease.



Similar content being viewed by others

References
Sun L, Yuan Q, Feng J, Yao L, Fan Q, Ma J, et al. Be alert to tuberculosis-mediated glomerulonephritis: a retrospective study. Eur J Clin Microbiol Infect Dis. 2012;31:775–9.
Waikhom R, Sarkar D, Bennikal M, Pandey R. Rapidly progressive glomerulonephritis in tuberculosis. Saudi J Kidney Dis Transpl. 2014;25:872–5.
Zhao N, Sun JY, Xu HP, Sun FY. Early diagnosis of tuberculosis-associated IgA nephropathy with ESAT-6. Tohoku J Exp Med. 2017;241:271–9.
Li S, Siyuan T, Jiangmin F, Hailong W, Li Y, Jianfei M, et al. Analysis of the association between Mycobacterium tuberculosis infection and Immunoglobulin A nephropathy by early secreted antigenic target 6 detection in renal biopsies: a prospective study. Postgrad Med. 2017;129:307–11.
Filho RB, Cordeiro AP, de Almeida FT, Shaletich C, Costa RS, Roselino AMF. Rare association of cutaneous vasculitis, IgA nephropathy and antiphospholipid antibody syndrome with tuberculous lymphadenitis. Clinics. 2012;67:1497.
Khaira A, Rathi OP, Mahajan S, Sharma A, Dinda AK, Tiwari SC. Lupus vulgaris with tubercular lymphadenitis and IgA nephropathy. Clin Exp Nephrol. 2008;12:79–81.
Solak Y, Gaipov A, Anil M, Atalay H, Ozbek O, Turkmen K, et al. Glomerulonephritis associated with tuberculosis: a case report and literature review. Kaohsiung J Med Sci. 2013;29:337–42.
Mercadal L, Hulot J, Isnard-Bagnis C, Baumelou A, Beaufils HDG. Favourable outcome of IgA nephropathy on antituberculous treatment. Minerva Urol e Nefrol. 2006;58:355–7.
Kanodia KV, Vanikar AV, Patel RD, Suthar KS, Trivedi HL. Crescentic Glomerulonephritis Associated with Pulmonary Tuberculosis. J Clin Diagn Res. 2016. https://doi.org/10.7860/JCDR/2016/14191.6970.
Oxland JO, Ensor J, Freercks R. Tuberculosis and pauci-immune crescentic glomerulonephritis. BMJ Case Rep. 2018. https://doi.org/10.1136/bcr-2017-221948.
Villar I, Hernandez E, Cozzi J, Paletta C, Mathurin S. Immune complex glomerulonephritis associated with pulmonary tuberculosis. Medicina (B Aires). 1994;54:237–40.
Pecchini F, Bufano G, Ghiringhelli P. Membranoproliferative glomerulonephritis secondary to tuberculosis. Clin Nephrol. 1997;47:63–4.
Ram R, Sandeep P, Sridhar VSN, Rukumangadha N, Sivakumar V. Membranoproliferative glomerulonephritis and Pott’s disease. Clin Kidney. 2014;7:391–3. https://doi.org/10.1093/ckj/sfu051.
Woo Yang C. Membranous glomerulonephritis associated with pancreatic tuberculosis. Korean J Med. 2008;74(5):546–50.
Ghosh B, Pande A, Ghosh A, Banerjee A, Saha S. Membranous glomerulonephritis and tuberculous peritonitis: a rare association. J Infect Dev Ctries. 2011;5:550–2.
Shang M-H, Zhu N, Hao J, Wang L, He Z-Y, Yang M, et al. Membranous nephropathy associated with tuberculosis. Chin Med J (Engl). 2016;129:622–3.
Rodriguez-Garcia JL, Fraile G, Mampaso F, Teruel JL. Pulmonary tuberculosis associated with membranous nephropathy [Internet]. Nephron. 1990;55:218–9.
Smith KD, Alpers CE. Pathogenic mechanisms in membranoproliferative glomerulonephritis. Curr Opin Nephrol Hypertens. 2005;14:396–403.
Wang Y, Tao Y. Tuberculosis-associated IgA nephropathy. J Int Med Res. 2018;46:2549–57.
De Vriese AS, Robbrecht DL, Vanholder RC, Vogelaers DP, Lameire NH. Rifampicin-associated acute renal failure: pathophysiologic, immunologic, and clinical features. Am J Kidney Dis. 1998;31:108–15.
Kohler LJ, Gohara AF, Hamilton RW, Reeves RS. Crescentic fibrillary glomerulonephritis associated with intermittent rifampin therapy for pulmonary tuberculosis. Clin Nephrol. 1994;42:263–5.
Murray AN, Cassidy MJ, Templecamp C. Rapidly progressive glomerulonephritis associated with rifampicin therapy for pulmonary tuberculosis. Nephron. 1987;46:373–6.
Yong JLC, Killingsworth MC. Diffuse glomerulonephritis associated with rifampicin treatment for tuberculosis. Pathology. 2002;34:295–7.
Hirsch DJ, Bia FJ, Kashgarian M, Bia MJ. Rapidly progressive glomerulonephritis during antituberculous therapy. Am J Nephrol. 1983;3:7–10.
Ogata H, Kubo M, Tamaki K, Hirakata H, Okuda S, Fujishima M. Crescentic glomerulonephritis due to rifampin treatment in a patient with pulmonary atypical mycobacteriosis. Nephron. 1998;78:319–22.
Alchi B, Jayne D. Membranoproliferative glomerulonephritis. Pediatr Nephrol. 2010;25:1409–18.
Maher J, Kelly P, Hughes P, Clancy L. Skin anergy and tuberculosis. Respir Med. 1992;86:481–4.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared no competing interest.
Ethical standards
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent was obtained from the index patient referred to in this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Torpiano, P., Holwill, S. & Pace, D. Mesangiocapillary glomerulonephritis complicating pulmonary tuberculosis. CEN Case Rep 11, 17–21 (2022). https://doi.org/10.1007/s13730-021-00626-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13730-021-00626-6