
Abstract
The experience of itch often poses a burden on patient quality of life and has the capacity to inflict significant suffering. Topical therapies are a mainstay of treatment for many cutaneous and systemic diseases and afford patients the opportunity to manage their conditions without many of the systemic side effects of non-topical therapies. We review a multitude of new topical medications targeting the skin, immune system, and neural receptors. The list includes Janus kinase inhibitors, tyrosine kinase inhibitors, phosphodiesterase inhibitors, transient receptor vanilloid inhibitors, topical cannabinoids, and topical acetaminophen. Many of the topical therapies reviewed show promising data in phase 2–3 clinical trials, but further research is needed to compare therapies head-to-head and test their efficacy on a broader range of conditions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Itch poses a substantial burden on patient quality of life. |
Topical therapies offer the unique ability to treat itch with minimal side effects. |
We review a range of topical therapies targeting the skin, immune, and neural systems, and their effects on itch. |
Many of the novel topical therapies we explored show promising clinical data with regards to reducing itch. |
Further studies are warranted to evaluate the efficacy of these new topicals, spanning a range of conditions. Additionally, head-to-head comparison studies are needed to provide comprehensive insight into their effectiveness. |
Introduction
Itch is an unpleasant sensory phenomenon, and its chronic form has significant psychosocial impacts on patient quality of life. Numerous systemic and cutaneous pathologies produce the sensation of itch, and different mechanisms are implicated [1]. With this, there also exists a plethora of therapeutic targets for drug discovery. Research in pruritus is continually evolving as mechanisms of diseases are uncovered and clarified and as new and creative therapeutics enter the scientific community for investigation. The interplay between advancements in the understanding of disease mechanisms and data on the efficacy of novel drugs yields an expansive framework from which clinical decision-making in the management of pruritus may be derived.
Topical therapies in particular serve as a cornerstone of treatment for many dermatologic conditions as they often lack the systemic side effects that are present with systemic therapies. They are especially implicated as primary treatment modalities for conditions where the mechanism of disease is based in the skin; nevertheless, their role as adjunctive therapy in more systemic diseases is crucial. This review explores novel topical drug therapies that have recently emerged in the past few years and show potential for the treatment of pruritus, most commonly localized pruritus. We review a wide range of therapies, from drugs in preclinical phases of study to medications that have recently been introduced into clinical practice (Table 1).
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Topical Janus Kinase Inhibitors (Brepocitinib, Delgocitinib, Ruxolitinib)
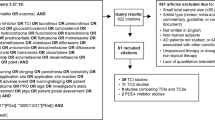
Topical Janus kinase (JAK) inhibitors have emerged as promising therapeutics in the treatment of pruritus owing to their efficacy and favorable safety profiles (Fig. 1). Their mechanism of action is immunomodulatory, involving inhibition of Janus kinases, which leads to disruption of signaling through type 2 cytokine, e.g., interleukin (IL)-4, IL-13, and IL-31, receptors as well as direct effects on cytokine receptors in nerve fibers [2].

Overview of the JAK/STAT pathway’s role in generating action potentials after binding of cytokines and the mechanism of action of topical JAK inhibitors. Detomidine activates skin nociceptor α2-adrenergic receptors, reducing itch signaling (Created with BioRender.com). JAK janus kinase, TRPV1 transient receptor potential vanilloid subfamily V member 1, TRPA1 transient receptor potential ankyrin 1
Ruxolitinib
Topical ruxolitinib is a JAK1 and JAK2 inhibitor that was approved by the US Food and Drug Administration (FDA) in September 2021 for the treatment of atopic dermatitis and has shown efficacy in the treatment of associated atopic itch and other itchy conditions including psoriasis, lichen planus, and cutaneous graft-versus-host disease (GVHD).
Phase III trials showed ruxolitinib to be efficacious in treating atopic itch. The Topical Ruxolitinib Evaluation in Atopic Dermatitis Studies (TRuE-AD) comprise two randomized, double-blind, vehicle-controlled studies with the same design [3]. Both studies looked at individuals 12 years or older with atopic dermatitis for 2 years or more, an IGA score of 2 or 3, and a body surface of 3–20% not including the scalp [3]. Patients were randomized to receive twice daily 0.75% or 1.5% ruxolitinib cream or vehicle cream for the initial 8 weeks of the study [3]. Within the first 12 h of the first application of ruxolitinib cream, there were significant reductions in itch NRS scores compared to vehicle [3]. Additionally at week 8, in patients with baseline itch NRS scores ≥ 4, there were significantly more patients with clinically relevant improvements in scores in TruE-AD1 and TruE-AD2 in those treated with ruxolitinib 0.75% (40.4% and 42.7%, respectively) and ruxolitinib 1.5% (52.2% and 50.7%, respectively) compared to the vehicle (15.4% and 16.3%, respectively) [3]. By the second day, both studies showed a significantly greater proportion of patients achieving ≥ 4-point reductions on NRS in the ruxolitinib 1.5% cohort (TruE-AD1, 11.6%; TruE-AD2, 10.8%) versus the vehicle (TruE-AD1, 2.9%; TruE-AD2, 1.3%) [3].
Ruxolitinib has demonstrated efficacy in reducing disease severity in psoriasis but with no published data on itch [4]. Further study in this area is needed, but it is assumed that it would also work to reduce pruritus. Similarly, ruxolitinib has demonstrated efficacy in treating lichen planus (LP) in a phase 2 study [5]. The study investigated 12 patients with LP; ruxolitinib 1.5% cream was applied twice daily to LP lesions for 8 weeks except for an untreated index lesion that served as a control [5]. The results showed that patient-reported quality of life and symptoms of pruritus were rapidly improved following treatment with ruxolitinib on the Skindex-16 and pruritus NRS, respectively [5]. By week 2, average scores on both scales were decreased by more than half and progressively decreased throughout the duration of the treatment period [5]. At week 4, Skindex-16 and pruritus NRS were reduced from baseline scores of 56.2 and 5.8 to 19.8 and 1.3, respectively [5]. Although the mechanism of itch is unclear in LP, some evidence points to the role of JAK1 and/or JAK2 [5, 6].
Additionally, topical ruxolitinib has been studied in the management of cutaneous GVHD with good efficacy on disease severity [7]. Patients with cutaneous GVHD often complain of pruritus, but the pathophysiology of itch in this condition is not well elucidated and the severity of itch has been reported not to be associated with disease severity [8]. There is a reported association between the reduction of pruritus and a longer failure-free survival in patients with chronic GVHD, pointing to the need for further research in this area [8, 9]. Numerous studies are currently underway to evaluate ruxolitinib’s efficacy in other itchy conditions including prurigo nodularis, lichen sclerosus, and seborrheic dermatitis.
Brepocitinib
Brepocitinib, a small-molecule tyrosine kinase 2 (TYK2)/JAK1 inhibitor is among the novel drugs in this category. A recent phase 2b randomized, double-blind, vehicle-controlled, dose-ranging, and parallel group study evaluated its use in patients with mild to moderate atopic dermatitis [10]. The study utilized the Peak Pruritus Numerical Rating Scale (PP-NRS) in 241 patients; this is a single-item survey designed to inquire about a patient’s worst itch over the preceding 24 h on a scale of 0 (no itch) to 10 (worst itch imaginable) [11]. Across all treatment dosages including brepocitinib 0.1% once daily, 0.3% once or twice daily, 1.0% once or twice daily, and 3.0% once daily, there was a numerically higher proportion of participants with ≥ 4-point reductions in weekly average of the PP-NRS from week 3 to week 6, the end of the study period, compared to vehicle groups (once or twice daily). However, statistically significant differences in ≥ 4-point reductions on the PP-NRS were noted at week 6 in the brepocitinib 1% once daily (45.2%), 3% once daily (50.0%), and 1% twice daily (40.7%) treatment groups compared to vehicles (daily, 18.2%; twice daily, 16.7%) [10].
Delgocitinib
Delgocitinib, a JAK1–3 and TYK2 inhibitor, that has been approved for pediatric and adult atopic dermatitis in Japan is another novel topical that has shown some evidence in alleviating atopic pruritus [12]. A phase 3, randomized, double-blind, vehicle-controlled study and an open-label, long-term extension study evaluated the use of delgocitinib 0.5% ointment applied twice daily for the treatment of patients with moderate to severe AD as determined by a modified eczema area and severity index score ≥ 10, an investigator global assessment (IGA) score of 3 or 4, and a body surface area of 10–30% [13]. This was performed for 4 weeks followed by a continuation period of 24 weeks [13]. The trial evaluated changes in pruritus NRS during the daytime and nighttime and found that in as early as the nighttime of the first day, patients applying the delgocitinib ointment saw a statistically significant reduction in pruritus NRS score compared to the vehicle ointment; this change was maintained over time [13]. Moreover, the mean change in pruritus NRS at week 4 was − 1.6 and the change at week 25 was − 1.3 [13]. Nevertheless, despite these improvements in NRS scores, the level of change is not considered clinically significant [14].
Delgocitinib has also demonstrated efficacy in the management of chronic hand eczema [15]. One phase 2b dose-ranging double-blind randomized clinical trial evaluated 258 adults with mild to severe chronic hand eczema [15]. Patients were randomized to delgocitinib cream 1, 3, 8, or 20 mg/g or a vehicle cream applied twice daily for 16 weeks. Eleven signs and symptoms of chronic hand eczema were evaluated through a Hand Eczema Symptom Diary on an 11-point rating scale [15]. Application of 20 mg/g delgocitinib cream resulted in early and sustained reductions in of both itch and pain [15]. Clinically relevant reductions of ≥ 4 points in itch and pain from baseline were noted by week 16 in 48.4% and 63.6% of patients, respectively, compared to 17.9% and 5.9% of patients treated with vehicle cream [15]. Furthermore, there were statistically significant improvements in all chronic hand eczema signs and symptoms in this treatment group compared to the vehicle cream [15]. Clinician-reported outcomes corroborated this data [15].
Phosphodiesterase 4 Inhibitors (Roflumilast, Difamilast, Lotamilast, LEO 29102)
Phosphodiesterase 4 (PDE4) catalyzes the metabolism of cyclic adenosine 3′,5′-monophosphate (cAMP), resulting in enhanced production of proinflammatory cytokines and chemokines [1]. Elevated cAMP levels, by inhibiting PDE4, may reduce inflammation and itch in various disorders including AD. Topical PDE4 inhibitors include crisaborole, roflumilast, lotamilast, difamilast, and LEO 29102.
Roflumilast
Roflumilast cream was FDA approved for plaque psoriasis in July 2022, as it rapidly and effectively reduced itch severity, providing improvement after 2 weeks with a reduction in worst itch of − 4 on a 10-point scale at week 8 [16, 17]. Furthermore, in two pivotal phase III trials, DERMIS-1 and DERMIS-2, 67.5% and 69.4% of patients treated with roflumilast and with baseline WI-NRS scores ≥ 4 had at least a 4-point reduction in score (WI-NRS Success) compared to 26.8% and 35.6% of patients treated with vehicle cream, respectively [18]. In December 2023, roflumilast 0.3% was approved for the treatment of seborrheic dermatitis. A phase III trial demonstrated that in 8 weeks, 62.8% of patients treated with roflumilast for seborrheic dermatitis experienced WI-NRS Success compared to 40.6% of those treated with vehicle cream; this improvement was noted within 2 days of initial therapy [19]. Roflumilast is also currently being studied for AD. Two phase III trials, INTEGUMENT-1 and INTEGUMENT-2, showed significant reductions in WI-NRS within 1 month in patients with AD treated with 0.15% roflumilast cream; 33.6% and 30.2% of treated patients had significant improvements versus 20.7% and 12.4% in the vehicle group in both studies, respectively, and improvements were noted as early as 1 day after initial application [20].
Difamilast
Difamilast is another topical PDE4 inhibitor approved in Japan in September of 2021 for the management of AD in adults and children greater than the age of 2. Difamilast 0.3%, difamilast 1%, or placebo was administered twice daily for 8 weeks in a phase 2 clinical trial for patients with mild or moderate AD (baseline IGA score of 2 or 3 and a 3-year history of disease) and 10–70 years of age. Regarding pruritus, difamilast 1% improved pruritus visual analog scale (VAS) scores from baseline within the first week (− 36.4% mean change) compared with placebo. Itch improvement was sustained, with a reduction of VAS scores throughout the 8 weeks of the study [21]. Another phase 2 clinical trial looked at Japanese pediatric patients 2–14 years old. This was a randomized, double-blind, placebo-controlled, 4-week study to evaluate the safety and efficacy of difamilast for AD [22]; 73 patients were randomized to treatment with difamilast 0.3%, difamilast 1%, or vehicle ointment twice daily. Patients receiving difamilast showed a consistent improvement in VAS pruritus scores over the trial period; such improvements were evident as early as week 1 where patients treated with difamilast 0.3% and 1% had least square mean changes from baseline of − 18.61 and − 12.83, respectively, compared to 0.34 in patients treated with vehicle [22]. By week 4, changes in least square means were − 18.00, − 17.21, and 8.19 for difamilast 0.3%, difamilast 1%, and vehicle, respectively [22].
Two phase 3 trials similarly highlight the efficacy of difamilast in treating pruritus. One double-blind, vehicle-controlled phase 3 trial looked at difamilast for the treatment of atopic dermatitis in patients aged 2–14 years. Patients received difamilast 0.3%, difamilast 1%, or vehicle ointment twice daily for 4 weeks [23]. Using a pruritus visual rating score, at week 1, patients treated with difamilast 0.3% and difamilast 1% had least square mean changes of − 0.59 and − 0.54, respectively, compared to − 0.14 in the vehicle group; these differences were statistically significant and persisted until week 4 of the study [23]. Another randomized, double-blind, vehicle-controlled phase 3 trial looked at a Japanese cohort of patients aged 15 to 70 years old with atopic dermatitis. Patients were treated with difamilast 1% ointment or vehicle twice daily for 4 weeks [23]. At week 1, there was a significantly greater change of least square mean from baseline in patients treated with difamilast 1% compared to vehicle, and by week 4, the change was − 0.65 in the difamilast 1% cohort compared to − 0.04 in the vehicle group, which was statistically significant [23].
Lotamilast
Lotamilast is another PDE4 inhibitor that has garnered attention. One multicenter, randomized, vehicle-controlled phase 2 clinical trial evaluated patients with AD aged 20 to 64 years with an affected body surface area of 5–30%. Patients received 0.2% lotamilast or vehicle ointment for 4 weeks, and those who continued for the extension phase received 0.2% lotamilast for an additional 8 weeks [24]. Pruritus scores were evaluated using Scoring Atopic Dermatitis C (SCORAD-C), which showed statistically significant improvements after 4 weeks [24]. There was a − 50.0% and − 69.5% mean difference between lotamilast and vehicle in the full analysis set and per protocol set, respectively [14, 24]. A randomized, vehicle-controlled, exploratory trial on Japanese children with AD also found lotamilast to be efficacious in the reduction of pruritus [25]. In this study, 62 patients were treated with lotamilast 0.05%, lotamilast 0.2%, or vehicle ointment twice daily for 2 weeks [25]. Notably, the trial found a greater decrease in pruritus score in those treated with lotamilast 0.2% compared to vehicle (− 37.5% vs. − 6.7%) [25].
LEO 29102
LEO 29102 is a PDE inhibitor selective for the PDE4D isoform that has also been studied in patients with AD [14]. A proof of concept phase 2 trial compared the efficacy of LEO 29102 to pimecrolimus in patients with AD. Patients were treated with LEO 29102 dosages of 0.03 mg/g, 0.1 mg/g, 0.3 mg/g, 1.0 mg/g, and 2.5 mg/g twice daily [14]. Pruritus was evaluated using the descriptors absent, mild, moderate, and severe to describe itch on the trunk and limbs [14]. The study found that patients treated with 0.3 mg/g and 2.5 mg/g of LEO 29102 twice daily had the greatest reductions in pruritus after 4 weeks (28.0% and 23.3%, respectively), although the statistical significance of the results was not reported [14].
Aryl Hydrocarbon Activator (Tapinarof)
Activation of the aryl hydrocarbon receptor (AHR) induces epidermal differentiation and has implications in skin barrier repair [26]. Tapinarof is a topical agent that activates AHR and has been FDA approved in a 1% formulation for the treatment of plaque psoriasis. Two phase III trials on patients with mild to severe plaque psoriasis showed a highly significant difference in patients achieving itch-free status compared to controls in 12 weeks (50% in both trials compared to 32% and 27% in the vehicle groups, respectively) [27]. Tapinarof has also been studied in AD in two phase III trials ADORING 1 and 2. Both trials showed substantial amounts of patients achieving meaningful itch reductions in those treated with tapinarof compared to vehicle by week 8 (ADORING 1, 55.8% vs. 34.2%, respectively; ADORING 2, 52.8% vs. 24.1%, respectively) [28, 29].
TRPV1 Antagonist (Asivatrep)
TRPV1 is strongly implicated in acute itch via histamine inhibition and also plays a role in non-histaminergic pruritus and chronic itch via activation of protease-activated receptors and subsequent neurogenic inflammation [25, 30,31,32].
Asivatrep or PAC-14028 is a selective and potent transient receptor potential vanilloid subfamily V member 1 (TRPV1) antagonist [33]. In a randomized, double-blind, vehicle-controlled phase 2b trial, patients with mild to moderate AD were randomized to receive vehicle cream or asivatrep 0.1%, 0.3%, and 1% applied twice daily for 8 weeks. All asivatrep-treated groups showed decreased mean change in VAS from baseline over the course of the study, although this difference was only statistically significant from baseline at week 8 in the asivatrep 1% group [34]. In a randomized, vehicle-controlled, phase 3 trial, patient-reported assessments of itch were lower in patients with AD treated with asivatrep cream than those receiving vehicle at week 1 and maintained until the end of the study (week 8). Moreover, the mean change in patient-reported pruritus VAS scores from baseline were significantly greater in the asivatrep-treated patients compared to those receiving vehicle (− 2.3 points vs. − 1.5 points), indicating significant improvement in itch [33]. Additionally, asivatrep appears to optimize skin barrier function through its production of epidermal differentiation markers, which may contribute to its antipruritic effect [33].
Topical Cannabinoids (Cannabidiol)
Cannabinoids are compounds that act on the endocannabinoid system to elicit a range of physiologic effects. Recently, topical cannabinoids have garnered attention for their potential role in managing cutaneous pathologies, namely AD, as they have been shown to have antipruritic and anti-inflammatory properties through activity on neurons, inflammatory cytokines, and mast cells [35]. The antipruritic mechanism of action is likely multifactorial, including peripheral and central modulation of cannabinoid receptors 1 (CB1) and 2 (CB2) and TRP channels [35]. The central effect is predominantly mediated via CB1, and the peripheral effect likely involves an analgesic effect mediated by both CB1 and CB2 [35].
Cannabidiol
A recent study investigated the effects of topical cannabidiol on 14 patients with AD aged 25–73 years old [36]. Patients completed surveys before and after 14-day application [36]. Pruritus was assessed using VAS-pruritus, which assessed patients’ itch on a scale of 0 (no itch) to 10 (worst itch of their life), and the 5-D pruritus scale, which assesses the degree, duration, disability, and distribution of itch within the prior 2 weeks [36]. Patients experienced a statistically significant reductions in pruritus on both, the VAS-pruritus (pre-treatment, 5.78; post-treatment, 4.01) and the 5-D pruritus scale (pre-treatment, 13.2; post-treatment, 10.86) [36].
Another study evaluated the effects of topical cannabinoid gel in patients with self-reported eczema. Twenty individuals consented to participate, of whom 16 completed the Patient Oriented Eczema Measure to assess disease severity and the emotional domain of the Quality-of-Life Hand Eczema Questionnaire to assess the psychosocial burden of disease [37]; 67% of participants reported a decrease in itch and more than 60% had a perceived improvement in their eczema [37].
Additionally, a role for topical cannabinoids has been suggested in uremic pruritus. There is some evidence to show their effect on TRPV1, which is implicated in the pathogenesis of uremic pruritus [38]. In one non-randomized study, 21 individuals with uremic pruritus were treated with a cream containing the endogenous cannabinoid acetylethanolamide and a related noncannabinoid, palmitoylethanolamide, which resulted in 38% of participants experiencing complete relief of pruritus [38, 39]. More studies are needed to further elucidate the role of cannabinoids for pruritus.
Drugs in Early Phase of Testing (B244, Detomidine, KM001, Topical Acetaminophen)
B244
B244 is a live biotherapeutic currently under investigation for a role in the management of AD (Table 2). B244 consists of a purified strain of Nitrosomonas eutropha [40]. This is an bacteria that oxidizes ammonia to nitrite and nitric oxide, which is thought to promote antimicrobial and anti-inflammatory activity, respectively [40]. In vitro analysis found B244 to reduce Th2 cytokines associated with AD including IL-4, IL-5, and IL-13 [40]. A randomized, double-blind, placebo-controlled, dose-ranging, phase 2b trial of B244 enrolled 547 patients 18–65 years old with mild to moderate AD and moderate to severe pruritus [40]. Optical density (OD) at 600 nm was used to divide patients into a low dose group (OD 5.0), a high dose group (OD 20.0), or a vehicle group for a 4-week treatment period and 4-week follow-up period [40]. Patients were to apply a topical spray twice daily during the treatment weeks [40]. Pruritus was assessed using the WI-NRS at 4 weeks [40]. Patients treated with B244 saw a 34% reduction in WI-NRS score (B244, − 2.8; placebo, − 2.1) from a baseline score greater than 8; this was statistically significant [40].
Topical Detomidine (CLE 400)
CLE-400 is a topical gel that contains detomidine, an activator of skin nociceptor α2-adrenergic receptors, which is proposed to inhibit receptor excitability and ultimately reduce neuropathic itch signaling [41]. CLE-400 is undergoing phase 2 studies for notalgia paresthetica [41].
KM001
There is evidence to suggest the involvement of TRPV3 in pruritus pathways. As such, this receptor has garnered attention as a potential therapeutic target for itch. Notably, KM001 has emerged as a novel topical small-molecule inhibitor of TRPV3 and is currently undergoing phase II trials for the treatment of lichen simplex chronicus [30].
Topical Acetaminophen
Topical acetaminophen has recently been studied for a possible role in treating itch. Traditionally, the mechanism of action is thought to involve inhibition of the cyclooxygenase pathway and prostaglandin synthesis, although the exact mechanism is not entirely known [42]. In a double-blind, vehicle-controlled pilot study, 17 healthy volunteers 19–50 years of age (average age of 26.4 years) were evaluated for treatment response with 1%, 2.5%, and 5% acetaminophen gels and a vehicle gel that was applied to the skin prior to the induction of itch with histaminergic (with histamine) and non-histaminergic (with cowhage) stimuli. Individuals treated with the 2.5% and 5% acetaminophen gel formulations had significant reductions in itch for histamine and cowhage compared to vehicle [42]. Moreover, the mean peak itch intensity was significantly reduced with the 2.5% gel formulation by 32% compared to the vehicle [42].
Conclusion
Topical treatments are the mainstay of therapies used by dermatologists; however, there were limited developments of novel topical antipruritics. The significant advancement in our understanding of the mechanisms of itch is leading to the development of novel topical therapies for itch, namely localized itch. The therapies highlighted carry a wide range of mechanisms and varying degrees of efficacy in their respective phases of study, inspiring continued innovation to target itch pathways. Comparisons between the drug therapies discussed may be limited by differences in study methods, phases of clinical trials, and pruritus assessment tools. For this reason, it is difficult to determine if one drug is more efficacious than another without being tested in a head-to-head trial. Furthermore, AD is the most studied condition in this review, and there is more room to test these topicals in the management of other itchy conditions. Ultimately, as research in the field continues to grow, increasing therapeutics are becoming available, allowing for more patient options and increasingly nuanced modalities of clinical practice.
References
Vander Does A, Ju T, Mohsin N, Chopra D, Yosipovitch G. How to get rid of itching. Pharmacol Ther. 2023;243:108355.
Lin CM, Cooles FA, Isaacs JD. Basic mechanisms of JAK Inhibition. Mediterr J Rheumatol. 2020;31(Suppl 1):100–4.
Papp K, Szepietowski JC, Kircik L, et al. Efficacy and safety of ruxolitinib cream for the treatment of atopic dermatitis: results from 2 phase 3, randomized, double-blind studies. J Am Acad Dermatol. 2021;85(4):863–72.
Słuczanowska-Głąbowska S, Ziegler-Krawczyk A, Szumilas K, Pawlik A. Role of Janus kinase inhibitors in therapy of psoriasis. J Clin Med. 2021;10(19):4307.
Brumfiel CM, Patel MH, Severson KJ, et al. Ruxolitinib cream in the treatment of cutaneous lichen planus: a prospective, open-label study. J Invest Dermatol. 2022;142(8):2109-2116.e4.
Oetjen LK, Mack MR, Feng J, et al. Sensory neurons co-opt classical immune signaling pathways to mediate chronic itch. Cell. 2017;171(1):217–228.e13.
Markova A, Pan A, Dusza S, et al. Interim results of a pilot, prospective, randomized, double-blinded, vehicle- and comparator-controlled trial on safety and efficacy of a topical inhibitor of Janus kinase 1/2 (Ruxolitinib INCB018424 Phosphate 1.5% Cream) for non-sclerotic and superficially sclerotic chronic cutaneous graft-versus-host disease. Blood. 2021;138:3915.
Zhu J, Navarini AA, Halter JP, Mueller SM. Pruritus in cutaneous graft-versus-host disease: a systematic review. J Eur Acad Dermatol Venereol. 2023;37(7):1276–83. https://doi.org/10.1111/jdv.19057.
Palmer J, Chai X, Pidala J, et al. Predictors of survival, nonrelapse mortality, and failure-free survival in patients treated for chronic graft-versus-host disease. Blood. 2016;127(1):160–6.
Landis MN, Arya M, Smith S, et al. Efficacy and safety of topical brepocitinib for the treatment of mild-to-moderate atopic dermatitis: a phase IIb, randomized, double-blind, vehicle-controlled, dose-ranging and parallel-group study. Br J Dermatol. 2022;187(6):878–87.
Yosipovitch G, Reaney M, Mastey V, et al. Peak Pruritus Numerical Rating Scale: psychometric validation and responder definition for assessing itch in moderate-to-severe atopic dermatitis. Br J Dermatol. 2019;181(4):761–9.
Chovatiya R, Paller AS. JAK inhibitors in the treatment of atopic dermatitis. J Allergy Clin Immunol. 2021;148(4):927–40.
Nakagawa H, Nemoto O, Igarashi A, Saeki H, Kaino H, Nagata T. Delgocitinib ointment, a topical Janus kinase inhibitor, in adult patients with moderate to severe atopic dermatitis: a phase 3, randomized, double-blind, vehicle-controlled study and an open-label, long-term extension study. J Am Acad Dermatol. 2020;82(4):823–31.
Labib A, Ju T, Yosipovitch G. Emerging treatments for itch in atopic dermatitis: a review. J Am Acad Dermatol. 2023;89(2):338–44.
Bauer A, Thyssen JP, Buhl T, et al. Treatment with delgocitinib cream improves itch, pain and other signs and symptoms of chronic hand eczema: results from the Hand Eczema Symptom Diary in a phase IIb randomized clinical trial. Contact Dermatitis. 2023;89(1):46–53.
Gold LS, Alonso-Llamazares J, Draelos ZD, et al. 27874 Correlation of itch response to roflumilast cream with disease severity and patient-reported outcomes in patients with chronic plaque psoriasis. J Am Acad Dermatol. 2021;85(3):AB164. https://doi.org/10.1016/j.jaad.2021.06.669.
Stein Gold L, Alonso-Llamazares J, Draelos ZD, et al. Effect of roflumilast cream (ARQ-151) on itch and itch-related sleep loss in adults with chronic plaque psoriasis: patient-reported itch outcomes of a phase 2b trial. Am J Clin Dermatol. 2023;24(2):305–13.
Lebwohl MG, Kircik LH, Moore AY, et al. Effect of roflumilast cream vs vehicle cream on chronic plaque psoriasis: the DERMIS-1 and DERMIS-2 randomized clinical trials. JAMA. 2022;328(11):1073–84.
Blauvelt A, Draelos ZD, Stein Gold L, et al. Roflumilast foam 0.3% for adolescent and adult patients with seborrheic dermatitis: a randomized, double-blinded, vehicle-controlled, phase 3 trial. J Am Acad Dermatol. 2024. https://doi.org/10.1016/j.jaad.2023.12.065.
Simpson E, Eichenfield L, Gooderham M, et al. Efficacy and safety of Roflumilast cream 0.15% in adults and children aged ≥6 years with mild to moderate atopic dermatitis in two phase 3 trials (INTEGUMENT-1 and INTEGUMENT-2). SKIN J Cutaneous Med. 2023;7(4):220.
Hanifin JM, Ellis CN, Frieden IJ, et al. OPA-15406, a novel, topical, nonsteroidal, selective phosphodiesterase-4 (PDE4) inhibitor, in the treatment of adult and adolescent patients with mild to moderate atopic dermatitis (AD): a phase-II randomized, double-blind, placebo-controlled study. J Am Acad Dermatol. 2016;75(2):297–305.
Saeki H, Baba N, Oshiden K, Abe Y, Tsubouchi H. Phase 2, randomized, double-blind, placebo-controlled, 4-week study to evaluate the safety and efficacy of OPA- 15406 (difamilast), a new topical selective phosphodiesterase type-4 inhibitor, in Japanese pediatric patients aged 2–14 years with atopic dermatitis. J Dermatol. 2020;47(1):17–24.
Saeki H, Baba N, Ito K, Yokota D, Tsubouchi H. Difamilast, a selective phosphodiesterase 4 inhibitor, ointment in paediatric patients with atopic dermatitis: a phase III randomized double-blind, vehicle-controlled trial. Br J Dermatol. 2022;186(1):40–9.
Furue M, Kitahara Y, Akama H, et al. Safety and efficacy of topical E6005, a phosphodiesterase 4 inhibitor, in Japanese adult patients with atopic dermatitis: results of a randomized, vehicle-controlled, multicenter clinical trial. J Dermatol. 2014;41(7):577–85.
Nemoto O, Hayashi N, Kitahara Y, et al. Effect of topical phosphodiesterase 4 inhibitor E6005 on Japanese children with atopic dermatitis: results from a randomized, vehicle-controlled exploratory trial. J Dermatol. 2016;43(8):881–7.
van den Bogaard EH, Bergboer JG, Vonk-Bergers M, et al. Coal tar induces AHR-dependent skin barrier repair in atopic dermatitis. J Clin Invest. 2013;123(2):917–27.
Kircik L, Zirwas M, Kwatra SG, et al. Rapid improvements in itch with tapinarof cream 1% once daily in two phase 3 trials in adults with mild to severe plaque psoriasis. Dermatol Ther (Heidelb). 2024;14(1):201–11.
Andrus E. Trial of VTAMA® (tapinarof) Cream, 1% Once Daily in Adults and Children as Young as 2 Years Old [Press Release]. https://www.dermatologytimes.com/view/adoring-1-study-reveals-promising-results-for-tapinarof-in-atopic-dermatitis. Accessed 9 Apr 2024.
Dermavant reports positive topline results from adoring 1, the second atopic dermatitis phase 3 trial of VTAMA® (tapinarof) cream, 1% in adults and children as young as 2 years old. Business Wire [Press Release]. https://www.dermavant.com/dermavant-reports-positive-topline-results-from-adoring-1-the-second-atopic-dermatitis-phase-3-trial-of-vtama-tapinarof-cream-1-in-adults-and-children-as-young-as-2-years-old/. Accessed 9 Apr 2024.
Mahmoud O, Soares GB, Yosipovitch G. Transient receptor potential channels and itch. Int J Mol Sci. 2022;24(1):420.
Nakagawa H, Hiura A. Four possible itching pathways related to the TRPV1 channel, histamine, PAR-2 and serotonin. Malays J Med Sci. 2013;20(4):5–12.
Shirolkar P, Mishra SK. Role of TRP ion channels in pruritus. Neurosci Lett. 2022;18(768): 136379.
Park CW, Kim BJ, Lee YW, et al. Asivatrep, a TRPV1 antagonist, for the topical treatment of atopic dermatitis: phase 3, randomized, vehicle-controlled study (CAPTAIN-AD). J Allergy Clin Immunol. 2022;149(4):1340–7(e4).
Lee YW, Won CH, Jung K, et al. Efficacy and safety of PAC-14028 cream—a novel, topical, nonsteroidal, selective TRPV1 antagonist in patients with mild-to-moderate atopic dermatitis: a phase IIb randomized trial. Br J Dermatol. 2019;180(5):1030–8.
Avila C, Massick S, Kaffenberger BH, Kwatra SG, Bechtel M. Cannabinoids for the treatment of chronic pruritus: a review. J Am Acad Dermatol. 2020;82(5):1205–12.
Maghfour J, Rundle CW, Rietcheck HR, et al. Assessing the effects of topical cannabidiol in patients with atopic dermatitis. Dermatol Online J. 2021. https://doi.org/10.5070/D3272052393.
Maghfour J, Rietcheck HR, Rundle CW, et al. An observational study of the application of a topical cannabinoid gel on sensitive dry skin. J Drugs Dermatol. 2020;19(12):1204–8.
Worth H, O’Hara DV, Agarwal N, Collister D, Brennan F, Smyth B. Cannabinoids for symptom management in patients with kidney failure: a narrative review. Clin J Am Soc Nephrol. 2022;17(6):911–21.
Szepietowski JC, Szepietowski T, Reich A. Efficacy and tolerance of the cream containing structured physiological lipids with endocannabinoids in the treatment of uremic pruritus: a preliminary study. Acta Dermatovenerol Croat. 2005;13(2):97–103.
Silverberg JI, Lio PA, Simpson EL, et al. Efficacy and safety of topically applied therapeutic ammonia oxidising bacteria in adults with mild-to-moderate atopic dermatitis and moderate-to-severe pruritus: a randomised, double-blind, placebo-controlled, dose-ranging, phase 2b trial. EClinicalMedicine. 2023;60:102002.
CLE-400 Pruritus 2022. https://www.clexio.com/pipeline/cle-400-pruritus/#:~:text=CLE%2D400%20is%20a%20topical,attenuation%20of%20neural%20itch%20signaling. Accessed 9 Apr 2024.
Nattkemper LA, Zhi K, Romero KE, et al. Antipruritic effect of topical acetaminophen gel in histaminergic and non-histaminergic itch provocation: a double-blind, vehicle-controlled pilot study. Acta Derm Venereol. 2022;102:adv00640.
Funding
No funding or sponsorship was received for this study or publication of this article.
Author information
Authors and Affiliations
Contributions
Rami H. Mahmoud—writing and editing of the manuscript, creation of the figure; Omar Mahmoud—writing and editing of the manuscript, creation of the figure; Georgia Biazus Soares—writing and editing of the manuscript; Gil Yosipovitch—concept design, reviewing and editing of the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Rami H. Mahmoud, Omar Mahmoud, and Georgia Biazus Soares have nothing to disclose. Dr. Gil Yosipovitch serves as an advisory board member for Abbvie, Arcutis, BMS, Cara Therapuetics, GSK. Escient Health, Eli Lilly, Galderma, Kiniksa Pharmaceuticals, LEO Pharma, Novartis, Pfizer, Pierre Fabre, Regeneron Pharmaceuticals, Inc., Sanofi, TreviTherapeutics, and Vifor; Dr. Gil Yosipovitch receives grants/research funding from Eli Lilly, Kiniksa Pharmaceuticals, LEO Pharma, Novartis, Pfizer, Galderma, Escient, Sanofi Regeneron, and Celldex; Dr. Gil Yosipovitch Received Pathways grants as Investigator for Regeneron Pharmaceuticals, Inc. Sanofi. Gil Yosipovitch is an Editorial Board member of Dermtology and Therapy. Gil Yosipovitch was not involved in the selection of peer reviewers for the manuscript nor any of the subsequent editorial decisions.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Mahmoud, R.H., Mahmoud, O., Biazus Soares, G. et al. Novel Topical Treatments for Itch. Dermatol Ther (Heidelb) 14, 829–840 (2024). https://doi.org/10.1007/s13555-024-01144-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-024-01144-w