
Abstract
Introduction
Monopolar radiofrequency (MRF) is a valuable modality for tightening and contouring mild-to-moderate facial skin laxity. Few studies have evaluated new-generation MRF devices for lower facial laxity in Asians. This study aims to evaluate the efficacy and safety of MRF for treating lower facial laxity in Asians.
Methods
This prospective cohort study enrolled 30 volunteers with Fitzpatrick Skin Types III–V and mild-to-moderate skin laxity. Subjects received a single MRF treatment. Self-assessments and adverse events were recorded. Two blinded dermatologists graded improvements (6-point scale) after treatment and 1, 3, and 6 months later.
Results
All subjects completed the study. Treatment energy levels ranged from 2 to 4. The average number of shots was 412 ± 49, delivered in 3–4 passes with 15–30% overlap. All patients reported improvement in lower facial laxity immediately after treatment. Most patients had mild-to-moderate improvement over the 6-month follow-up. Continuous improvement was observed at the 1-, 3-, and 6-month follow-ups (P < 0.01). Significant improvement was seen at the 6-month follow-up compared with the 1-month follow-up (P < 0.01). Subjects tolerated the procedure well: the average pain score was 3.13 out of 10, and no serious adverse events were observed.
Conclusions
The new-generation MRF device we tested was effective and safe for mild-to-moderate lower facial laxity in Asian skin. The latest MRF technology offers improved safety to prevent complications. Appropriate patient selection, setting, and protocols are mandatory to achieve optimal clinical outcomes.
The Trial Registration Number
TCTR20210326002.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
Monopolar radiofrequency (MRF) is a valuable modality to tighten and contour mild-to-moderate skin laxity of the lower face and neck. |
Few studies have examined the effects of the latest generation of MRF devices in Asians. |
This study aims to evaluate the efficacy and safety of MRF for treating lower facial laxity in Asians. |
What was learned from the study? |
MRF treatment appears to give mild-to-moderate improvement, with statistically significant improvement over time. |
The newer technologies of the latest MRF devices offer improved levels of safety that prevent complications. |
Introduction
The face transforms throughout time. The alterations occur at every anatomic level due to a dynamic interaction between extrinsic and intrinsic factors and the activities of the facial musculature [1]. Gradual deterioration of these layers manifests clinically as excessive skin laxity [2]. Lower face wrinkles and excessive skin laxity make people look “older.” Various modalities have been utilized to treat skin laxity and wrinkles of the lower face. These include surgical procedures, chemical peeling, lasers, injectables, intense pulsed light, and radiofrequency (RF) [3].
Over time, the designs of RF devices have advanced so that they can now tighten and contour the skin and body effectively. Depending on the area of concern, they provide customizable results with little to no downtime [4]. The devices can be classified as monopolar, unipolar, bipolar, and multipolar, depending on the number of electrodes and the method used to transmit energy to subcutaneous tissues. The polarity of the RF affects the treatment’s comfort, effectiveness, and frequency [4]. Monopolar radiofrequency (MRF) is a valuable modality to tighten and contour mild-to-moderate skin laxity of the lower face and neck. Treatment with MRF is still one of the gold standards and a popular method for skin tightening [2]. Since the introduction of the first MRF device in the early 2000s, different companies have developed RF platforms that utilize innovative and novel technologies to enhance therapeutic outcomes [4].
Few studies have examined the effects of the newest (fourth) generation of MRF devices in Asians. The present investigation assessed the efficacy and safety of monopolar radiofrequency for lower facial laxity in Asians. This evaluation of the latest-generation MRF devices will improve clinicians’ understanding of the technology.
Methods
This prospective, cohort, evaluator-blinded study was conducted at a tertiary university hospital. The study enrolled 30 Thai volunteers (29 women; 1 man). They had Fitzpatrick Skin Types III–V with mild-to-moderate facial laxity (1.5–2.5 points, according to a 4-point quantitative grading scale for laxity). The inclusion criteria were a body mass index < 30 kg/m2, male or female, and < 45 years of age. The exclusion criteria were as follows: a history of hypertrophic scar or keloid, showing signs of active infection, a herpes simplex infection, smoking regularly, immunocompromised, preexisting connective tissue disease, implanted electrical device of any kind, being pregnant, up to 3 months postpartum, breastfeeding, facial treatment with monopolar radiofrequency, microfocused ultrasonography, botulinum toxin, or laser during the previous 6 months, and treatment with facial fillers during the previous 12 months.
Subjects received a single treatment on day 0 and returned for follow-up assessments on days 30, 90, and 180. At each session, photographic documentation with frontal, left-oblique, right-oblique, left-lateral, and right-lateral views was captured. The protocol was approved by the Institutional Review Board of the university hospital in Bangkok, Thailand (Si 146/2021). Before enrollment, all patients were informed of the therapeutic benefits, risks, and possible complications. Prior to the study-related procedures, the patients gave their written informed consent to the treatment and the later publication of any patient images. This research was performed per the Helsinki Declaration of 1964 and subsequent amendments.
The study used a monopolar radiofrequency device (Oligio; Won Tech Co., Ltd., Seongnam, Gyeonggi, Korea) with a frequency of 6.78 MHz, maximum power of 400 W, and impedance range of 75–400 Ω. The RF emission depends on the energy level (set from 0.5 to 8). The device has a hand piece connected to a disposable treatment tip with a working area of 2 × 2 cm2 (4 cm2). A hand switch controls the treatment shot. A sensor in the treatment tip continuously monitors skin temperature and a contact pressure sensor, and a skin impedance checking system in the tip confirms that there is proper contact between the tip and the skin. The system generates deep-tissue heating (40–60 °C). Contact cooling from a cryogen spray on the inner surface of the treatment tip occurs before, during, and after each energy pulse.
Preoperatively, patients were instructed to remove all makeup and metallic accessories, and wash the treatment areas with a mild cleanser. Before treatment, a topical mixture of 2.5% lidocaine and 2.5% prilocaine cream (a eutectic mixture of local anesthetic; AstraZeneca LP, Wilmington, DE, USA) was applied under occlusion to the treatment area for 1 h. Immediately before treatment, the patients were disinfected with 70% isopropyl alcohol, and the tip condition was checked, appropriately positioned, and grounded. The return pad was thoroughly attached on the right side of the upper back. The treatment area was marked with a provided marker. The tip membrane was thoroughly disinfected with a 70% alcohol swab and checked for dirt or scratches. Coupling oil fluid was applied to the treatment site to ensure uniform conduction of the MRF energy from the tip electrode to the skin. Treatment then commenced.
Machine-controlled pressure, temperature sensors, and skin-impedance checking in the MRF treatment tip automatically aborted energy delivery if uniform contact was not maintained with the skin or if the temperature at the skin surface rose above a set threshold. The treatment started with a test shot at the standard level, and the level was then varied according to patient feedback. The thermal sensation goal was a score of 3 (from 0 to 10) “hot but tolerable.” The hand piece was kept perpendicular (90 °C) to the skin to ensure that the tip fully contacted the skin. The following settings were used over the treatment area: 4 cm2 tip, energy levels 2–4, and 3–4 passes with 15–30% overlapped. The treatment area includes the middle and lower face, extended from the nasolabial fold medially to the preauricular region laterally to the inferior margins of the submental and submandibular regions inferiorly. Treatment with multiple passes was continued as tolerated until visible tightening or erythema was evident.
Patients could resume normal activities immediately after the procedure. However, they were instructed to apply a UVA/B sunscreen with an SPF > 30 daily and avoid direct sun exposure. No other supplementary products or special instructions on skin care were given. Due to their limited penetration depths, all patients may continue their regular skincare routine at home without worrying about any negative effects. To maximize the healing response within the dermis and promote collagen formation, the patients were advised to avoid using anti-inflammatory medications (steroids and nonsteroidal anti-inflammatory drugs).
Photographic documentation was obtained at baseline; immediately after treatment; and at 1, 3, and 6 months afterward. Identical camera settings and lighting were used, and standard photographic images were obtained of the face at five corners prior to n-axis 90º, 45°, 0º, −45º, and −90º. All digital photographs were shot using a Canon PowerShot G9 standoff camera (OMNIA Imaging System; Canfield Scientific, Inc., Fairfield, NJ, USA). The fixture ensured a set distance and fixed angles between the patient and the camera. Flashlamps placed in fixed positions relative to the camera ensured even illumination of all parts of the face and the ability to examine subjects under controlled lighting.
The study’s outcome was the clinical improvement of the lower face using a 6-point scale. Clinical evaluations were obtained immediately after treatment and 1, 3, and 6 months later. The “before” and “after” photographs were evaluated. Two blinded non-treating board-certified dermatologists graded the clinical improvement using a 6-point scale, with −1 = worse, 0 = no change, 1 = mild improvement (1–25%), 2 = moderate improvement (26–50%), 3 = marked improvement (51–75%), and 4 = excellent improvement (76–100%). Patients also performed self-assessments using the same 6-point scale. Any adverse events arising from the MRF treatment were collected.
The descriptive-analytic method was employed to evaluate data on clinical improvements to lower facial laxity. Categorical variables were summarized by count and percentage, while continuous variables were summarized by mean, median, minimum, and maximum percentiles with standard error. The dermatologists’ assessments of improvements at 1, 3, and 6 months after treatment were analyzed with the Wilcoxon signed-rank test and the Friedman test. The statistical analyses were processed using SPSS Statistics for Windows, version 18.0 (SPSS Inc., Chicago, IL, USA). Significance was set at P ≤ 0.05.
Results
All 30 subjects completed the study and attended the final 6-month follow-up assessment. Twenty-nine patients were female (96.6%; n = 29), and one patient was male. The age of the participants ranged from 43 to 53 years (mean, 48 years). Eleven had Fitzpatrick skin type III (36.6%), 13 had type IV (43.3%), and 6 had type V (20.1%). Patient demographics are detailed in Table 1.
Treatment was delivered in 3–4 passes with a 15–30% overlap. During the treatment session, subjects received a mean of 412 ± 49 shots. The energy level ranged from 2 to 4, and the total energy delivered in a session was 31 ± 4.7 kJ.
The dermatologists’ assessments of improvement in lower facial laxity using the 6-point scale are summarized in Fig. 1. Immediately after treatment, 65% of the patients showed a 1–25% improvement, and 33.33% showed a 26–50% improvement. Some patients became worse (5%) or had no change (26.67%) relative to baseline.

Dermatologists’ assessments of the improvements immediately after the treatments, and 1, 3, and 6 months following the treatments
Steady improvements were observed at the 1-, 3-, and 6-month follow-ups (P < 0.01; Table 2). At the 1-month follow-up, 86.67% of patients showed improvement, with 1–25%, 26–50%, and 51–75% improvements in 61.67%, 16.67%, and 8.33% of the patients, respectively. Noticeable improvements were seen at the 3-month follow-up: 85% of patients showed improvement, and more patients had 26–50% and 51–75% improvements (40.00% and 3.33%, respectively; Fig. 1). Most patients maintained their improvement until the 6-month follow-up (86.67%). At that time, the majority of patients showed moderate improvement (38.33%), while some patients had marked (8.33%) and excellent improvements (3.33%). Moreover, significant improvement was found at the 6-month follow-up compared with the 1-month follow-up (P < 0.01; Table 3).
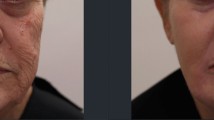
Patient self-assessments were recorded at all follow-ups (Fig. 2). All patients reported improvement immediately after treatment, with 1–25%, 26–50%, 51–75%, and 76–100% improvement in 23.33%, 30.00%, 33.33%, and 13.33% of cases, respectively. At the 1-month follow-up, 73.3% reported improvement, with 1–25%, 26–50%, and 51–75% improvement in 16.67%, 23.33%, and 33.33% of patients, respectively. An increase in improvement was again found at the 3-month follow-up. Most patients (90%) perceived mild, moderate, and excellent improvements (30.00%, 33.33%, and 26.67% of patients, respectively). The improvement remained consistent until the 6-month follow-up, with 76.67% of patients reporting improvement. Most patients perceived a 51–75% improvement (36.67%), while a few (6.67%) reported a 76–100% improvement. Representative clinical improvements in lower facial laxity at baseline and follow-up visits are shown in Fig. 3.

Patients’ assessments of the improvements immediately after the treatments, and 1, 3, and 6 months following the treatments

A representative clinical photograph at baseline (A); immediately after the treatment (B); and 1 (C), 3 (D), and 6 (E) months after the treatment
All patients tolerated the procedure well. Reporting a mean pain score of 3.13 during the procedure, 25 patients (83.3%) experienced erythema immediately after treatment that resolved in 1–2 days. One month after treatment, one patient (3.3%) experienced facial dryness; however, it had resolved by the 3-month follow-up. No complications were observed 3 or 6 months after the therapy.
Discussion
Restoring balance and harmony to the lower face without surgery requires a thorough patient history and assessment to identify treatment areas [1]. MRF treatment softens the nasolabial folds, lifts the jowl skin, and enhances the cervicomental angle [5]. Mild-to-moderate facial skin laxity can be tightened and lifted using RF [6]. Generally, the modality is used for people in their mid-thirties through to their early fifties, but older patients also use RF. Asians in their forties have been identified as receiving the most benefit from MRF [7].
Most patients in the present investigation reported a mild-to-moderate improvement in lower facial skin laxity. The outcome of this study may have benefited from proper patient selection since good patient selection is required for MRF procedures. Kilmer et al. [8] reported that most appropriately selected patients exhibit visible improvements after a single treatment with new-generation MRF devices.
Monopolar RF devices generate volumetric heat through a high-frequency electric current that travels through a transducer and returns to a grounding pad on the patient’s body. Volumetric heating heats the deep dermis, fat, fibrous septae, and fascia [9], resulting in skin tightening for 4–6 months [10]. The middle and lower faces may respond more immediately to RF because they typically contain a higher proportion of subcutaneous fat [11]. Interestingly, compared with baseline, all patients in our study experienced an immediate improvement after the treatment procedure. A possible explanation for the current findings is immediate collagen denaturation that leads to fibril contraction and tissue thickening [12]. An additional possible mechanism for the immediate improvements in contour that were visible is that the MRF energy was conducted to collagen-based fibrous septa. Between 10% and 30% of subcutaneous tissue has collagen-based fibrous septa, which form a connective tissue network between fat locules.
The subjective nature of patient outcomes regarding skin tightening must be considered. Our patients’ self-assessment scores were higher than the physicians’ evaluation scores. Nevertheless, the patients’ subjective reporting is still pertinent because it reflects patient satisfaction and perception of improvement after the treatment. This view is consistent with the work of Dover et al. [13]: their 5700-patient satisfaction survey revealed that 87% of patients experienced immediate tightening.
The present study also demonstrated continued clinical improvement over time. At the 1-month follow-up, we observed that 86.67% of patients showed improvement, with mild, moderate, and marked improvements in 61.67%, 16.67%, and 8.33% of patients, respectively. Alhaddad et al. [14] demonstrated that MRF significantly improved cheek laxity, nasolabial folds, jowls, and upper neck laxity as early as 30 days after the procedure. Furthermore, Angra et al. [2] showed that 80% and 73% of subjects improved by months 3 and 6, respectively. In the current investigation, we observed greater degrees of improvement at the 3- and 6-month follow-ups, and more moderate-to-marked improvements were seen. A similar pattern was seen with the patients’ self-assessments. An improvement was perceived by 90.00% of the patients at the 3-month follow-up and 76.60% at the 6-month follow-up.
Previous research revealed that collagen fibril alterations were noticeable 8 weeks after MRF therapy. Their presence could result from the natural healing mechanism [15]. The treated skin also had elevated collagen messenger RNA (mRNA), with a collagen Type I mRNA steady-state expression that was 2.4-fold higher on day 2 and 1.7-fold higher 1 week after treatment. However, 3 and 8 weeks after treatment, the mRNA levels were slightly below control levels [15]. In our investigation, steady clinical improvement was observed at the 1-, 3-, and 6-month follow-ups (P < 0.01; Table 2). Significant improvement was also found at the 6-month follow-up compared with the 1-month follow-up (P < 0.01; Table 3).
Newer generations of MRF devices have improved by incorporating larger tips for greater efficacy and efficiency, vibration for added comfort, cooling for greater comfort and ability to endure high energy levels, and impedance checking technology to increase safety [2]. Fourth-generation MRF devices use a high-frequency generator that produces a 400 W, 6.78 MHz monopolar current signal. MRF devices stimulate volumetric tissue heating, with dermal temperatures reaching between 65 and 75 °C [16]. Our study used an MRF of 6.78 MHz, a power of 400 W, a 4-cm2 disposable tip, and a coupling fluid to generate 40–60 °C tissue heating. The device used also had an optional vibration mode. The sensor in the tip continuously monitored skin temperature and the contact pressure sensor, and the skin impedance checking system (measured by the tip) confirmed proper tip contact with the skin. This new-generation MRF device proved efficient and convenient during the study treatment sessions.
The treatment parameters provide valuable insights that enable clinical results to be optimized [17], and a proper technique is mandatory to deliver the energy efficiently. The treatment settings of the newer generation of MRF devices are lower than those of earlier models [18]. Suh et al. reported treatment levels of 2–2.5 (82.7%) for the cheek, 2–2.5 (55.8%) for the forehead, and 1–1.5 (65.4%) for the eyelid [7]. In our study, subjects received treatment energy levels ranging from 2 to 4. Energy-level selection is best determined by continuously evaluating the heat tolerance level of individual patients during the procedure. According to our patient feedback, we set the energy at a level that kept the thermal sensation at a score of 3 (“hot but tolerable”), on the scale of 0–10. Not only do patients have different pain tolerances, but their skin compositions also vary. These differences affect the degree of RF penetration, resistance, and thermal deposition within the tissue. Drawing upon patient feedback on heat sensation is imperative to determine proper device settings, and this method has proven to be valid for optimal energy selection [8].
The number of treatment passes was previously found to affect the collagen fibril change [19]. The current study delivered treatment in 3–4 passes with a 15% to 30% overlap, and a clinical endpoint of erythema or visible skin tightening. Using a multiple-pass algorithm, Dover et al. reported that 87% of their patients reported immediate skin tightening, while 92% noted skin tightening 6 months following the procedure [13]. Our study had similar results to those of Dover et al.: all of our patients reported immediate skin tightening, and 86.67% were improved at the 6-month follow-up. Bogle et al. [11] evaluated the pulse count of MRF using a low pulse range (76–149 pulses), a medium pulse range (150–193 pulses), and a high pulse range (194–368 pulses). The data trended toward more improvement with more pulses per treatment. In the present work, the subjects received an energy level ranging from 2 to 4, and the average number of shots was 412 ± 49. Tailoring the number of pulses might increase efficacy.
Newer generations of MRF technology and multiple-pass treatment algorithms have markedly improved the modality’s efficiency and safety [2, 20]. The complication rate of recent-generation MRF devices was reported to be under 10% [7]. Of the patients with adverse events, 23.5% had severe pain, 33.3% had erythema for more than 24 h, 49% reported blisters or vesicles, and 51% had edema for 24–48 h. The same research found that most dermatologists considered pulse staking (37.3%), problematic tip (37.3%), and using high energy (58.8%) as the cause of complications [7]. The most significant safety concern associated with the MRF procedure is the need to avoid superficial injuries [17].
Based on our clinical data, MRF is safe to use on Asian skin. All patients tolerated the procedure well, reporting a mean pain score of 3.13 during the procedure. Although 25 patients (83.3%) experienced erythema immediately after treatment, the condition resolved in 1–2 days. In addition, 1 patient (3.3%) experienced facial dryness 1 month after treatment; the dryness had resolved before the 3-month follow-up assessment. Moreover, no complications were observed 3 or 6 months after treatment. The real-time temperature feedback built into the MRF device and its cryogen gas cooling helped the operator avoid thermal injuries.
Limitations
The limitations of this study were the lack of a control group, and the evaluations were mainly subjective. It is not easy to quantify the degree of skin lifting because it is three-dimensional. Further studies with longer follow-up and multiple treatment algorithms will add more clinical information about the technology that will be of value to clinicians.
Conclusions
Our prospective clinical trial demonstrated that the new-generation MRF device we investigated is effective and safe for mild-to-moderate lower facial laxity in Asian skin. MRF treatment appears to give mild-to-moderate improvement, with statistically significant improvement over time. Additionally, the newer technologies of the latest MRF devices offer improved levels of safety that prevent complications. Appropriate patient selection, a proper setting, and suitable treatment protocols are mandatory to achieve optimal clinical outcomes.
References
Carruthers J, Carruthers A. A multimodal approach to rejuvenation of the lower face. Dermatol Surg. 2016;42:S89–93.
Angra K, Alhaddad M, Boen M, Lipp MB, Kollipara R, Hoss E, et al. Prospective clinical trial of the latest generation of noninvasive monopolar radiofrequency for the treatment of facial and upper neck skin laxity. Dermatol Surg. 2021;47(6):762–6.
Rabe JH, Mamelak AJ, McElgunn PJ, Morison WL, Sauder DN. Photoaging: mechanisms and repair. J Am Acad Dermatol. 2006;55(1):1–19.
Lee C, Gold MH. Updates on radiofrequency devices for skin tightening and body contouring. Dermatol Rev. 2020;1(3):75–83.
Alster TS, Tanzi E. Improvement of neck and cheek laxity with a nonablative radiofrequency device: a lifting experience. Dermatol Surg. 2004;30(4):503–7.
Waibel JS. Photorejuvenation. Dermatol Clin. 2009;27(4):445–57.
Suh DH, Hong ES, Kim HJ, Lee SJ, Kim HS. A survey on monopolar radiofrequency treatment: the latest update. Dermatol Ther. 2020;33(6): e14284.
Kilmer SL, Lupo MP, Marmur E, Dyke SV. Consensus recommendations for 4th generation non-microneedling monopolar radiofrequency for skin tightening: a Delphi consensus panel. J Drugs Dermatol. 2020;19(1):20–6.
Beasley K, Weiss RA. Radiofrequency in cosmetic dermatology. Dermatol Clin. 2014;32:79–90.
Dierickx CC. The role of deep heating for noninvasive skin rejuvenation. Lasers Surg Med. 2006;38(9):799–807.
Bogle MA, Ubelhoer N, Weiss RA, Mayoral F, Kaminer MS. Evaluation of the multiple pass, low fluence algorithm for radiofrequency tightening of the lower face. Lasers Surg Med. 2007;39(3):210–7.
Fritz M, Counters JT, Zelickson BD. Radiofrequency treatment for middle and lower face laxity. Arch Facial Plast Surg. 2004;6:370–3.
Dover JS, Zelickson B, Panel PMC. Results of a survey of 5700 patient monopolar radiofrequency facial skin tightening treatments: assessment of a low-energy multiple-pass technique leading to a clinical end point algorithm. Dermatol Surg. 2007;33(8):900–7.
Alhaddad M, Wu DC, Bolton J, Wilson MJ, Jones IT, Boen M, et al. A randomized, split-face, evaluator-blind clinical trial comparing monopolar radiofrequency versus microfocused ultrasound with visualization for lifting and tightening of the face and upper neck. Dermatol Surg. 2019;45(1):131–9.
Zelickson BD, Kist D, Bernstein E, Brown DB, Ksenzenko S, Burns J, et al. Histological and ultrastructural evaluation of the effects of a radiofrequency-based nonablative dermal remodeling device: a pilot study. Arch Dermatol. 2004;140(2):204–9.
Weiss RA. Noninvasive radio frequency for skin tightening and body contouring. Semin Cutan Med Surg. 2013;32(1):9–17.
Alexiades-Armenakas M, Rosenberg D, Renton B, Dover J, Arndt K. Blinded, randomized, quantitative grading comparison of minimally invasive, fractional radiofrequency and surgical face-lift to treat skin laxity. Arch Dermatol. 2010;146(4):396–405.
Suh DH, Hong ES, Kim HJ, Lee SJ, Kim HS. A survey on monopolar radiofrequency treatment. Dermatol Ther. 2017;30(5): e12536.
Kist D, Burns AJ, Sanner R, Counters J, Zelickson B. Ultrastructural evaluation of multiple pass low energy versus single pass high energy radio-frequency treatment. Lasers Surg Med. 2006;38(2):150–4.
Abraham MT, Ross EV. Current concepts in nonablative radiofrequency rejuvenation of the lower face and neck. Facial Plast Surg. 2005;21(01):65–73.
Acknowledgements
Funding
This research project is supported by the Faculty of Medicine Siriraj Hospital, Mahidol University. The device was supported by Quantum Healthcare (Thailand) Co., Ltd. The rapid service fee and open access fee were funded by Won Tech (South Korea) Co., Ltd.
Authorship
All named authors meet the International Committee of Medical Journal Editors criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Phumithep Phumariyapong, Yanisorn Nanchaipruek, Panwadee Thongjaroensirikul, Pitchaya Maneeprasopchoke, and Chadakan Yan. Data interpretation and critical revision were performed by Rungsima Wanitphakdeedecha, Thanya Techapichetvanich, Sasima Eimpunth, and Woraphong Manuskiatti. Rungsima Wanitphakdeedecha had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The first draft of the manuscript was written by Yuri Yogya and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Medical Writing, Editorial, and Other Assistance
The authors thank Ms Phonsuk Yamlexnoi, Ms Chutikan Kiatphansodsai, Ms Apichaya Jutaphonrakul, and Dr Thanyaporn Leesanguankul for their assistance in recruiting subjects and managing the database. The authors express their gratitude to Mr Suthipol Udompunthurak for his assistance with the statistical analyses. The authors are also indebted to Mr David Park for English-language editing.
Disclosures
Rungsima Wanitphakdeedecha, Yuri Yogya, Chadakan Yan, Phumithep Phumariyapong, Yanisorn Nanchaipruek, Panwadee Thongjaroensirikul, Pitchaya Maneeprasopchoke, Thanya Techapichetvanich, Sasima Eimpunth, and Woraphong Manuskiatti, declare that they have no personal, financial, commercial, or academic conflicts of interest.
Compliance with Ethics Guidelines
The study was approved by the ethics committee of the Siriraj Institutional Review Board (Certificate of Approval No. Si146/2021). Written informed consent was obtained for the publication and use of all patients’ images prior to their enrollment in the study. This study was performed in accordance with the Helsinki Declaration of 1964 and its subsequent amendments and was registered at ClinicalTrials.gov (NCT number TCTR20210326002).
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Thanking Patient Participant(s)
We thank the patients who participated in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Wanitphakdeedecha, R., Yogya, Y., Yan, C. et al. Efficacy and Safety of Monopolar Radiofrequency for Treatment of Lower Facial Laxity in Asians. Dermatol Ther (Heidelb) 12, 2563–2573 (2022). https://doi.org/10.1007/s13555-022-00817-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-022-00817-8