
Abstract
Introduction
As atopic dermatitis (AD) grows increasingly prevalent in Asian populations worldwide, understanding how environmental, genetic, and cultural factors uniquely influence AD in Asians is essential for informing disease management. Our objectives were to characterize the epidemiology of AD in East Asian populations with sensitivity to the changing demographics of AD in these populations and the effects of urbanization and immigration.
Methods
A systematic review was performed on epidemiologic studies of AD in East Asian populations over the past 10 years.
Results
There is a rising prevalence of both pediatric and adult AD in Asian populations worldwide, particularly in Asians living in urban areas. Studies suggest that the children of Asian immigrants may be at higher risk for developing AD, potentially resulting from epigenetic phenomena unique to immigrant populations. A number of genetic polymorphisms implicated in AD are shared by Asian populations around the world and appear to be rare among other ethnic populations.
Conclusions
As the prevalence of AD continues to increase in Asian populations, it is important to understand its distinct genetic and pathophysiologic profile in these populations, as well as characterize the cultural beliefs and practices surrounding its treatment. Future research should aim to capitalize on our growing understanding of pathophysiologic differences to inform the most promising treatments for AD in Asians. Additionally, the impact of immigration on AD suggests that further investigation of these trends may lead to a greater understanding of the epigenetics of AD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Atopic dermatitis (AD) is increasing in prevalence in both pediatric and adult populations in East Asian countries. |
A complex interplay between genetics and environmental factors are likely to underlie the increasing burden of AD among Asians. |
Children of Asian immigrants may be at a particularly higher risk of developing AD. |
Genetic polymorphisms implicated in AD are common among Asian populations around the world, and different from those among other ethnic populations. |
There are unique and different pathophysiologic mechanisms underlying AD in Asians. |
Digital Features
This article is published with digital features, including a summary slide, to facilitate understanding of the article. To view digital features for this article go to https://doi.org/10.6084/m9.figshare.14152682 .
Introduction
Atopic dermatitis (AD) is a pruritic, chronic inflammatory skin condition that is becoming increasingly prevalent across the world. While AD was traditionally thought of as presenting most commonly in children, adult-onset AD is becoming a more common entity. AD prevalence varies across different countries and ethnicities, and the demographics of AD continue to evolve over time. Specifically in Asian populations, the epidemiology of AD has changed considerably over recent years.
Notably, AD prevalence in Asian populations appears to be increasing, which may be related in part to rapid urbanization in many major metropolitan areas in Asia; for example, the population inhabiting China’s urban areas has increased from 11.8% in 1950 to 49.2% by 2010 [1]. The actual epidemiology of AD among different Asian populations remains unclear, but a growing body of evidence supports that this is an increasingly prevalent disease in many Asian countries with shifting demographics. Some of the challenges in interpreting the data likely stem from variations in study design, patients’ understanding of the disease process, and a complex interplay between an evolving industrialized environment and AD.
Additionally, recent studies suggest that immigration may influence trends in AD prevalence among Asians, although more research is needed to parse out the precise impact. Research examining genetic and phenotypic presentations in AD in Asians distinct from AD in other ethnicities suggests that Ad in Asians may have unique pathophysiologic features.
The aim of this review is to provide an overview of existing research on the epidemiology of AD in Asian countries, the associations between immigration and AD risk, and pathophysiologic features that may be unique to AD in Asians.
Background: Epidemiology of AD in Asian Populations Worldwide
Reports of AD prevalence in different Asian populations have focused largely on pediatric patients, with the reported prevalance highly variable, ranging from under 5% to as high as 20%.
In a worldwide cross-sectional questionnaire survey conducted in 1999, the International Study of Asthma and Allergies in Childhood (ISAAC) reported that, in general, the prevalence of AD among children in Asia was higher than that among children of northern Europe [2], with rates of AD in China, Korea, and Japan of 1.2, 3.4, and 10.5%, respectively. Phase III of ISAAC published in 2009 revealed a rise in AD prevalence in children over the decade, reaching 10–20% in many of the developing industrialized countries of Asia [3].
Methods and Search Strategy
The eligibility criteria for the compiled studies included: (1) primary epidemiologic studies of AD in an East Asian population, (2) at least 5000 participants, and (3) published in 2010–2019.
For this systematic review, the PubMed and MEDLINE databases were used, with the time-frame set from inception to 2019. A combination of keywords and MeSH terms were used to create the search strategy. The Boolean operator “AND” was used to combine terms, keywords, and concepts. The keywords and MeSH terms used were: “Atopic dermatitis,” “Epidemiology,” “Asians,” “Japan,” “Korea,” “China.”
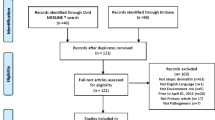
The search strategy is shown in Fig. 1, and details on the ten studies ultimately included in this review are given in Table 1.

PRISMA flow diagram of the search strategy and included studies
Ten studies were ultimately included in this review, as reported in Table 1.
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Results
AD in Asian Children and Adolescents
Korea
Several large studies in Korea have sought to evaluate the prevalence of AD in children based on data from physician examination, parent questionnaires, and large population-based studies.
A study conducted in Seoul, Korea used both clinical diagnosis and parent response questionnaires to assess AD prevalence in 2008 among children aged 0–6 years. Dermatologist examination of 6453 pre-school children yielded AD prevalence of 9.2%, with most patients having mild disease as measured by the Eczema Area and Severity Index (EASI) score. The ISAAC-based questionnaire yielded a higher AD prevalence of 19.1% [4].
Another cross-sectional study using parent response to the ISAAC questionnaire found that among 8750 children, 14.4% reported having AD within the previous 12 months [5]. Prevalence was significantly higher in pre-school children than in elementary school children, suggesting that younger age is associated with increased risk for AD. Interestingly, having pets was positively associated with AD among pre-school children, while among elementary school children, female gender, second-hand smoke, and moving to a newly built house within the first year of life was positively associated with AD [5].
AD prevalence among adolescents was assessed in a study using data from the Sixth Korean National Adolescent Health Behavior Survey, 2010, which was conducted by the Korea Center for Disease Control [6]. Of 37,570 adolescents who completed online self-report surveys, 22.6% reported an AD diagnosis within the past 12 months. The results of this study may be limited by its reliance on adolescent self-report; AD diagnosis was assessed based on response to a yes-or-no question written using wording from the ISAAC questionnaire. This study also found that prevalence of AD was 1.52-fold higher among female adolescents than among male students [6].
In a cross-sectional study using self-reported data from the 2008–2011 Korea National Health and Nutrition Examination Survey, the prevalence of AD among 8947 children aged 1–18 in Korea was 13.5%. Younger age, urban living, and higher household income were associated with greater risk for AD [7]. A study analyzing the frequency of AD-associated diagnosis codes submitted to the Korean National Health Insurance Service found a prevalence of AD of 5.8% among 9,992,581 children aged 0–18 in 2014. Of note, AD prevalence decreased from 20.8% in 2009 to 15.4% in 2014 among children 0–2 years of age [8]. The authors cite increased breastfeeding, vaginal deliveries, and consumption of probiotics as potential contributors to this decrease in AD prevalence.
Variations in study design and AD assessment methods make it difficult to ascertain the true prevalence of this disease in Korea. Even within a single study, dermatologist assessment based on EASI score and use of the ISAAC-based questionnaire yielded widely varying results [4]. Studies looking at the prevalence of physician-diagnosed AD, whether through direct skin examination or analysis of prior diagnosis codes, have found a lower rate of AD in Korea compared with AD reported using questionnaire-based methods. More research is needed to ascertain the actual epidemiology of AD in Korea.
China and Japan
In a study including kindergartens and vaccination clinics in 12 metropolitan areas of China, the prevalence of AD among 13,998 children aged 1–7 years in 2013–2014 was 12.94% based on clinical diagnosis by dermatologists and 4.76% based on UK Working Group criteria [9]. It should be noted that in this study, parents completed the surveys, and thus there is the potential that concepts were not well presented due to the translation and therefore not well understood. It has been noted that there are fundamental issues to consider when translating a survey to another language; it must not only be linguistically sound, but also culturally relevant and understandable [10] and that the process of translating a survey may introduce unintended biases depending on the type of questions asked.
A cross-sectional study spanning eight different districts in Shanghai, China asked parents to complete the UK Working Party questionnaire and found an AD prevalence of 8.3% among 10,436 children aged 3–6 years in 2010 [11]. An interesting finding from that study was that the rates of AD in the urban core of Shanghai were double that in the rural suburbs on the outskirts of the city. There are numerous hypotheses for this phenomenon, among them are urban development leading to pollution and the hygiene hypothesis whereby children in developed areas who are less exposed to allergens in early childhood have a higher propensity for developing allergic diseases.
Clinical investigations performed in elementary schools showed an AD prevalence of 0% in Lhasa, Tibet, 2.63% in Yixing, China, and 4.26% in Nishinomiya, Japan [12]. These represent three different environments: the first is a very rural environment where the bathing frequency is twice per month; the second is a medium-sized city in China; and the third is a relatively larger urban center in Japan. Both of the latter cities represent environoments that are more developed in terms of daily bathing frequencies, and while it is tempting to attribute the differing prevalence of AD to the aforementioned hygiene hypothesis, there may be other genetic and environmental factors contributing to this.
The prevalence of dermatologist-diagnosed AD among 7856 children aged 0–6 years on Ishigaki Island, a remote and warmer southern island belonging to Japan, was approximately 5–7%. The prevalence did not increase from 2001 to 2010 [13]. It is interesting to note that while the population should be rather similar ethnically to that of mainland Japanese, the prevalence of AD is only roughly half that in mainland Japan (12–13%) [13, 14].
Overall, studies in China and Japan to date have shown comparable rates of AD, although they did not include adolescents and focused more on younger children.
AD in Asian Adults and the General Population
While most research has focused on AD in pediatric patients, a number of studies have included adults in their investigations, and findings suggest that AD affects a subset of adults as well.
A 2014 cross-sectional study conducted among outpatients from 39 tertiary hospitals of 15 provinces in China reported the prevalence of AD in adults to be 7.8% based on dermatologist diagnosis using the UK Working Party criteria [15]. Among adults with AD, 59.7% experienced first onset of AD after the age of 18 years, while 40.3% experienced first onset of AD before age 18 years, suggesting that adult-onset AD was quite common in this population [15]. In a nationwide, cross-sectional study that included participants of all ages and spanned 170 clinics, the prevalence of AD in Japan was found to be 9.98% [16].
More research is needed to clarify the prevalence of AD in Asian adults, but existing evidence suggests that adult AD is not uncommon in many Asian countries, with prevalence rates approaching one in ten individuals.
Associations between Urbanization and AD in Asians
Potentially contributing to the evolving prevalence of AD is the rapid urbanization and increased pollution in many metropolitan areas in Asia. This environmental impact on AD is supported by research comparing AD rates in urban and rural areas of Asia.
A study spanning 12 metropolises in China found significantly lower rates of AD in children residing in rural areas (37.58%) compared to those in urban residence (62.42%; P < 0.001). Additionally, the prevalence of AD was higher (19.73%–24.69%) in inland China where recent accelerated industrialization had occurred [9].
Similarly, a cross-sectional study covering eigh different districts in Shanghai, China found the highest prevalence of AD among children in the core urban area (10.2%) and the lowest prevalence of AD in a district located far from the urban areas (4.6%) [11]. The study also categorized locations as urban, suburban, and rural to compare AD prevalence between them. The prevalence of AD was significantly higher in urban areas than in both the suburban and rural areas. Additionally, the prevalence of AD in suburban areas was significantly higher than that in rural areas [11].
Similar trends have been reported in Korea, where AD prevalence among children aged 1–18 years was 86.6% in urban areas and only 13.4% in rural areas (P = 0.0380) [7].
Research demonstrating the higher AD prevalence in urban areas as compared to rural areas points toward the possible role of rapid urbanization in the growing prevalence of AD in some Asian countries.
Impact of Immigration on AD in Asians
There is a growing body of literature examining AD among Asian immigrants in different countries, and research suggests that the children of Asian immigrants may be at particularly high risk of developing AD.
In a cross-sectional study in Australia, infants whose parents immigrated from East Asia had a higher prevalence (37.4%) of AD than infants of Australian-born parents (21.4%). Interestingly, the odds of infants developing AD increased linearly for each immigrant parent, combining to a multinomial odds ratio (OR) of 2.6 in cases of both parents haveing immigrated from East Asia. AD prevalence was lower among infants whose parents had immigrated to Australia recently (within 5 years) compared to those whose parents had immigrated less recently (> 5 years) (48.0 and 61.7%, respectively; P = 0.03). Interestingly, despite their children’s increased risk for developing AD, mothers born in East Asia were less likely to report having AD (10.3%) compared to mothers born in other regions worldwide (14.7%) (P = 0.008) [17], which suggests that Asian ethnicity serves as both a protective factor in parents and a risk factor in their children. Unique environmental effects may be at play in the children of Asian immigrants, but whether these trends can be attributed to immigration or the country of residence remains to be explored.
A survey study of adolescents in Israel found that Asian (OR 1.15) origins (defined as father’s country of birth) were associated with a higher prevalence of AD compared with African (OR 0.80) and Ethiopian (0.27) origins. Older age at time of immigration was also associated with a greater risk of AD in that immigrating to Israel after the age of 7 years was associated with significantly higher prevalence of AD in comparison to adolescents who were either born in Israel or who had immigrated before the age of 7 years (OR 1.88 vs. 1.41) [18]. These trends may point to increased risk factors associated with living in an Asian country or being of Asian descent; alternatively, living in Israel may provide protective effects.
A study in the USA revealed that among children with Asian parents, the OR of developing AD was lower (OR 0.23, 95% confidence interval 0.06–0.85) for children born outside the USA than those born within the USA [19].
In a cross-sectional study of children aged 0–17 years enrolled in the National Survey of Children’s Health in the USA, infants of Asian mothers were twice as likely to have been diagnosed with AD as infants of white or Hispanic mothers. Maternal country of birth, however, did not affect or alter the risk for AD [20]. In this case, Asian ethnicity increased risk for AD but parental immigration status did not.
Preliminary findings suggest an interesting trend where prevalence of AD appears to be stable among immigrants from Asian countries but higher among their children. Recent immigration and age at time of immigration also appear to be factors in AD risk among children. More research is needed to parse out the impact of immigration on AD risk.
Discussion
There is a great deal to unpack when considering what to make of one’s approach to AD in Asians. On one hand, it does seem that AD prevalence is consistently being found to be higher among Asian populations over the past few decades than previously thought (Fig. 2). However, there are numerous confounding factors that make it difficult to assess which factors may play a role in this, including a better understanding of the disease process itself.

Prevalence of AD in Asian populations by year across multiple studies. Populations in Asian countries (diamonds) are separated by age into categories of 0–18 years (red) and > 18 years (blue). Crosses indicate Asian patients who immigrated to other countries, also separated by age (0–18 years, in red; > 18 years, in blue)
One especially intriguing concept is the role of pollution and urbanization in the increased prevalence of AD. One of the studies cited above notes substantial differences in three Asian cities, with higher prevalence of AD coinciding with increased levels of urbanization [12]. This observaton was also supported in a recent meta-analysis which showed that urbanization in addition to maternal and personal history of smoking were the strongest environmental factors correlating with AD among Asians [21]. There is also basic science supporting this concept, with a potential link between pollution and AD found in the aryl hydrocarbon receptor [22]. In this framework, keratinocyte aryl hydrocarbon receptors sense lipophilic polycyclic aromatic hydrocarbons, which form the primary particulate matter found in air pollution, and activate the neurotrophic factor artemin, which in turn leads to epidermal hyper-innervation and formation of the itch–scratch cycle, even in an animal model. This may explain increases in AD prevalence not only in Asian countries, but also in countries where Asians have immigrated to.
In terms of clinical presentation, Asian patients with AD often show clearer demarcation of lesions with more prominent scaling and lichenification than patients of other ethnic groups [23]. These findings directly correlate with molecular and histological differences in Asian skin compared to the skin of their European/American counterparts, including more frequent parakeratosis, focal hypogranulosis, and more elongated rete ridges [23]. Further, histologic and molecular analyses have revealed significantly greater epidermal hyperplasia in Asian patients with AD compared to European/American patients, as measured based on greater thickness (P < 0.001) and a greater number of Ki671 cells in the basal layer of the epidermis (P < 0.001). Epidermal thickness measures of Asian patients with AD were similar to those seen in patients with psoriasis [23].
Compared to European/American patients, Asian patients with AD have higher IgE (P < 0.01) and eosinophil levels (P < 0.01), lower mean age (P < 0.001), and a higher rate of extrinsic AD (P = 0.004) [23], defined by increased levels of serum IgE [24]. In one study, 89% of Asian patients had extrinsic AD while only 56% of European American patients had this subtype. In addition, compared to European/American patients, Asian patients with extrinsic AD showed overall similar or lower expression of T-helper cell type 2 (Th2)-related chemokines (CCL17 and CCL22), lower levels of several Th1 markers, and significantly higher induction of Th17-related cytokines [23].
Certain genetic variations may uniquely contribute to AD in Asian skin. A number of mutations in the filaggrin (FLG) gene have been identified in Asian populations, most notably c.3321delA, which has been associated with AD in China, Korea and Japan [25,26,27,28,29], whereas R501X and 2282del4 mutations are commonly found in European populations [30]. Loss-of-function mutations in SPINK5 have been identified in several Asian populations as well, including those of Japan, China, and Taiwan [31,32,33,34]. Taken together, these findings suggest that the association between AD and certain genetic variations may be consistent across Asian populations worldwide and unique compared to other non-Asian ethnic groups.
Clearly, in terms of underscoring the differences in pathophysiology between Asian and European AD patients, there is still a great deal to understand about mechanistic influences in AD among these populations. The fillagrin mutations are common in individuals of European ancestry, being present in up to 50% of patients with AD; in Asians, that figure is closer to 25%. While a relatively small number of specific fillagrin mutations underlie the vast majority of cases of AD in Caucasians, there seems to be a higher number of specific mutations found in Asian populations [35]. Thus, it is not surprising that the cytokine profile of AD in patients of European and Asian descent seems to reflect some differences, although this has yet to result in any implications for treatment as targeting of the Th17 axis proved to be an ineffective treatment strategy for treating AD in a Japanese Phase II study [36].
Conclusion
Atopic dermatitis has a significant and increasing prevalence in both pediatric and adult Asian populations worldwide. In particular, AD disproportionately affects people living in urban areas, which raises the concern that the prevalence of AD will rise as Asian metropolises continue to increase in number and size. Further, results from preliminary studies on AD in Asian immigrants indicate that the children of immigrants may be at particularly high risk for developing AD, suggesting that the increased risk of AD is not isolated to location on the Asian continent, but rather to traits/genetics intrinsic to these populations. Several studies have investigated the genetics of AD in a number of different Asian countries and, taken together, their common findings suggest that certain genetic polymorphisms may not only be more common across all Asians with AD, but also unusual or absent in other ethnic populations.
Although few studies have directly compared AD in Asian and non-Asian populations, existing research suggests that AD in Asians may have unique pathophysiologic features and that identifying these differences may have important implications for the identification of at-risk individuals as well as prevention and treatment of the disease. Future studies should explore the unique pathophysiologic characteristics of Asians with AD in both children and adults, as well as unique environmental exposures, genetic polymorphisms, and cultural practices that may impact the development of AD and efficacy of currently available and new treatments. Focusing on Asian immigrant populations may provide new insight into the role of the environment and epigenetics on AD. Further, subanalyses of current pharmacologic treatments, including biologics and small molecules, may help generate bespoke treatment approaches targeted towards the root of the disease process in each patient.
References
Farrell K, Westlund H. China’s rapid urban ascent: an examination into the components of urban growth. Asian Geogr. 2018;35(1):85–106.
Williams H, Robertson C, Stewart A, et al. Worldwide variations in the prevalence of symptoms of atopic eczema in the International Study of Asthma and Allergies in Childhood. J Allergy Clin Immunol. 1999;103(1 Pt 1):125–38.
Odhiambo JA, Williams HC, Clayton TO, Robertson CF, Asher MI. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124(6):1251-1258.e1223.
Choi WJ, Ko JY, Kim JW, et al. Prevalence and risk factors for atopic dermatitis: a cross-sectional study of 6,453 Korean preschool children. Acta Derm Venereol. 2012;92(5):467–71.
Baek JO, Hong S, Son DK, Lee JR, Roh JY, Kwon HJ. Analysis of the prevalence of and risk factors for atopic dermatitis using an ISAAC questionnaire in 8,750 Korean children. Int Arch Allergy Immunol. 2013;162(1):79–85.
Oak JW, Lee HS. Prevalence rate and factors associated with atopic dermatitis among Korean middle school students. J Korean Acad Nurs. 2012;42(7):992–1000.
Lee JH, Han KD, Kim KM, Park YG, Lee JY, Park YM. Prevalence of atopic dermatitis in Korean children based on data From the 2008–2011 Korean National Health and Nutrition Examination Survey. Allergy Asthma Immunol Res. 2016;8(1):79–83.
Lee JY, Yang HK, Kim M, Kim J, Ahn K. Is the prevalence of atopic dermatitis in Korean children decreasing?: National Database 2009–2014. Asian Pac J Allergy Immunol. 2017;35(3):144–9.
Guo Y, Li P, Tang J, et al. Prevalence of atopic dermatitis in Chinese children aged 1–7 years. Sci Rep. 2016;6:29751.
McGorry SY. Measurement in a cross-cultural environment: survey translation issues. J Cetacean Res Manag. 2000;3(2):74–81.
Xu F, Yan S, Li F, et al. Prevalence of childhood atopic dermatitis: an urban and rural community-based study in Shanghai, China. PLoS ONE. 2012;7(5):e36174.
Sumikawa Y, Ueki Y, Miyoshi A, et al. Survey of atopic dermatitis and skin barrier functions in Japanese and Chinese school students. Arerugi. 2007;56(10):1270–5.
Takeuchi S, Esaki H, Furue M. Epidemiology of atopic dermatitis in Japan. J Dermatol. 2014;41(3):200–4.
Yamamoto S. Prevalence and exacerbation factors of atopic dermatitis. Skin Allergy Front. 2003;1:85–90.
Wang X, Shi XD, Li LF, Zhou P, Shen YW, Song QK. Prevalence and clinical features of adult atopic dermatitis in tertiary hospitals of China. Medicine. 2017;96(11):e6317.
Furue M, Yamazaki S, Jimbow K, et al. Prevalence of dermatological disorders in Japan: a nationwide, cross-sectional, seasonal, multicenter, hospital-based study. J Dermatol. 2011;38(4):310–20.
Martin PE, Koplin JJ, Eckert JK, et al. The prevalence and socio-demographic risk factors of clinical eczema in infancy: a population-based observational study. Clin Exp Allergy. 2013;43(6):642–51.
Wohl Y, Wainstein J, Bar-Dayan Y. Atopic dermatitis in Israeli adolescents—a large retrospective cohort study. Acta Derm Venereol. 2014;94(6):695–8.
Silverberg JI, Simpson EL, Durkin HG, Joks R. Prevalence of allergic disease in foreign-born American children. JAMA Pediatr. 2013;167(6):554–60.
Moore MM, Rifas-Shiman SL, Rich-Edwards JW, et al. Perinatal predictors of atopic dermatitis occurring in the first six months of life. Pediatrics. 2004;113(3 Pt 1):468–74.
Ng YT, Chew FT. A systematic review and meta-analysis of risk factors associated with atopic dermatitis in Asia. World Allergy Organ J. 2020;13(11):100477.
Hidaka T, Ogawa E, Kobayashi EH, et al. The aryl hydrocarbon receptor AhR links atopic dermatitis and air pollution via induction of the neurotrophic factor artemin. Nat Immunol. 2017;18(1):64–73.
Noda S, Suarez-Farinas M, Ungar B, et al. The Asian atopic dermatitis phenotype combines features of atopic dermatitis and psoriasis with increased TH17 polarization. J Allergy Clin Immunol. 2015;136(5):1254–64.
Tokura Y. Extrinsic and intrinsic types of atopic dermatitis. J Dermatol Sci. 2010;58(1):1–7.
On HR, Lee SE, Kim SE, et al. Filaggrin mutation in Korean patients with atopic dermatitis. Yonsei Med J. 2017;58(2):395–400.
Park J, Jekarl DW, Kim Y, Kim J, Kim M, Park YM. Novel FLG null mutations in Korean patients with atopic dermatitis and comparison of the mutational spectra in Asian populations. J Dermatol. 2015;42(9):867–73.
Meng L, Wang L, Tang H, et al. Filaggrin gene mutation c.3321delA is associated with various clinical features of atopic dermatitis in the Chinese Han population. PLoS ONE. 2014;9(5):e98235.
Zhong WL, Wu X, Yu B, et al. Filaggrin gene mutation c.3321delA is associated with dry phenotypes of atopic dermatitis in the Chinese Han population. Chin Med J. 2016;129(12):1498–500.
Li K, Oh WJ, Park KY, Kim KH, Seo SJ. FLG mutations in the East Asian atopic dermatitis patients: genetic and clinical implication. Exp Dermatol. 2016;25(10):816–8.
Rodriguez E, Baurecht H, Herberich E, et al. Meta-analysis of filaggrin polymorphisms in eczema and asthma: robust risk factors in atopic disease. J Allergy Clin Immunol. 2009;123(6):1361-1370.e1367.
Kato A, Fukai K, Oiso N, Hosomi N, Murakami T, Ishii M. Association of SPINK5 gene polymorphisms with atopic dermatitis in the Japanese population. Br J Dermatol. 2003;148(4):665–9.
Nishio Y, Noguchi E, Shibasaki M, et al. Association between polymorphisms in the SPINK5 gene and atopic dermatitis in the Japanese. Genes Immun. 2003;4(7):515–7.
Lan CC, Tu HP, Wu CS, et al. Distinct SPINK5 and IL-31 polymorphisms are associated with atopic eczema and non-atopic hand dermatitis in Taiwanese nursing population. Exp Dermatol. 2011;20(12):975–9.
Zhao LP, Di Z, Zhang L, et al. Association of SPINK5 gene polymorphisms with atopic dermatitis in Northeast China. J Eur Acad Dermatol Venereol. 2012;26(5):572–7.
Brown SJ, McLean WH. One remarkable molecule: filaggrin. J Invest Dermatol. 2012;132(3 Pt 2):751–62.
Saeki H, Kabashima K, Tokura Y, et al. Efficacy and safety of ustekinumab in Japanese patients with severe atopic dermatitis: a randomized, double-blind, placebo-controlled, phase II study. Br J Dermatol. 2017;177(2):419–27.
Acknowledgements
Funding
No funding or sponsorship was received for this study or publication of this article.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
Julia Cheng and Jashin J Wu have nothing to disclose. George Han is Editorial Board member of the journal.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Cheng, J., Wu, J.J. & Han, G. Epidemiology and Characterization of Atopic Dermatitis in East Asian Populations: A Systematic Review. Dermatol Ther (Heidelb) 11, 707–717 (2021). https://doi.org/10.1007/s13555-021-00516-w
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-021-00516-w