
Abstract
Introduction
Persistent facial erythema associated with rosacea may negatively impact quality of life (QoL), self-esteem, and self-confidence. We evaluated burden and health-related QoL (HRQoL) impacts of centrofacial erythema of rosacea.
Methods
A cross-sectional, Web-based survey conducted in collaboration with the National Rosacea Society enrolled adults who self-reported having received a physician diagnosis of rosacea and self-evaluated their current erythema as mild to severe on the validated Subject Self-Assessment for Rosacea Facial Redness. Sociodemographic and clinical characteristics, rosacea symptoms, and their impacts on QoL [validated Impact Assessment for Rosacea Facial Redness (IA-RFR)] and HRQoL [validated Dermatology Life Quality Index (DLQI)] were recorded.
Results
A total of 708 eligible respondents completed the survey (white/Caucasian, 93.5%; female, 83.1%; mean age, 52.4 years). Respondents had mild (59.2%), moderate (33.2%), or severe (7.6%) erythema. The most bothersome symptoms were persistent facial erythema (69.2%) and blushing/flushing (60.9%). Mean IA-RFR scores showed negative impacts across all severities of erythema. The mean (standard deviation) total DLQI score was 5.2 (6.0) overall [mild erythema, 3.8 (4.9); moderate, 5.7 (5.4); severe, 13.4 (8.9); P < 0.0001].
Conclusion
Centrofacial erythema of rosacea represents a substantial HRQoL burden, especially for those with more severe erythema.
Funding
Allergan plc, Dublin, Ireland.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rosacea is a chronic skin condition that has an estimated prevalence of approximately 5.5% among adults globally [1], although the prevalence may be higher because of underdiagnosis [2]. Centrofacial erythema is a hallmark of rosacea; patients frequently present with a combination of individual features such as persistent erythema, flushing, papules or pustules, and telangiectasia [3,4,5]. Rosacea has been shown to have negative effects on psychosocial health factors such as self-esteem, confidence, and the ability to socialize [6,7,8]. However, limited literature exists on the impact of facial erythema due to rosacea on the self-perception, grooming, social, and emotional impacts as well as health-related quality of life (HRQoL).
A previous cross-sectional survey of 600 participants compared HRQoL of participants with erythematotelangiectatic vs papulopustular rosacea. It demonstrated that rosacea had an overall negative impact on HRQoL in both cohorts using the Rosacea-specific Quality-of-Life questionnaire and overall QoL assessed by the Impact Assessment for Rosacea Facial Redness (IA-RFR) [9, 10]. The current survey was conducted in collaboration with the National Rosacea Society (NRS) and sought to further explore the symptom profile and burden of centrofacial erythema in adults with differing severities of erythema due to rosacea using the IA-RFR and the Dermatology Life Quality Index (DLQI). The DLQI also was included to allow comparison of erythema of rosacea to other skin conditions.
Methods
This cross-sectional, direct-to-patient, Web-based survey was administered from March 13 to May 26, 2017 to patients who visited the NRS website or received the NRS Rosacea Review newsletter and agreed to participate. Respondents were required to provide informed consent through a Web link opt-in process prior to completing a series of demographic and screening questions that assessed eligibility. Survey enrollment was open until the targeted number of completed surveys (600) was met. Participants received a US$15 gift card for completing the survey. United BioSource Corporation (Kansas City, Missouri) monitored the conduct of the survey, which was administered by Ipsos Observer (New York, New York). The Chesapeake Institutional Review Board (IRB) determined that this study met the regulatory criteria for exemption from IRB oversight using the Department of Health and Human Services regulations Title 45 CFR Part 46.101(b) (2). The study was conducted in accordance with the requirements for studies involving human respondents and regulatory guidelines.
Participant Eligibility
Eligible participants were at least 18 years of age, self-reported that they had received a physician’s diagnosis of rosacea, were able to read and understand United States (US) English, and had current mild, moderate, or severe centrofacial erythema of rosacea based on the validated Subject Self-Assessment for Rosacea Facial Redness with photo guide. Participants were excluded if they had a clinical diagnosis of telangiectasia and/or visible blood vessels covering more than 25% of the facial area where rosacea occurs, a clinical diagnosis of sun damage and/or sun-damaged skin (irregular coloring or pigmentation of the skin with a mottled wrinkled appearance and liver spots or age spots) covering more than 25% of the face, or a clinical diagnosis of facial acne and/or facial acne covering more than 25% of the face. There was a temporary cap on the number of mild severity patients eligible to participate in the survey for 18 days during survey fielding to ensure adequate recruitment of respondents with moderate and severe erythema. Respondents who indicated that they had mild facial erythema during this timeframe were excluded.
Data Collection
Information on sociodemographic characteristics was collected from respondents, including age, gender, ethnicity, race, marital status, living area (suburban/rural/urban), education level, height and weight (to calculate body mass index), primary medical insurance, and prescription drug coverage. Clinical characteristics of rosacea included age of onset, date of diagnosis, presence of papulopustular rosacea, type of provider who diagnosed rosacea, age when rosacea became bothersome, troublesome factors about rosacea, symptoms, location, behavioral factors and triggers of rosacea, presence of other co-occurring skin conditions, and Fitzpatrick skin phototype [11]. Respondents were asked about the severity of current symptoms associated with facial erythema of rosacea on the validated Symptom Assessment for Rosacea Facial Redness scale [12], which comprises four items (degree of redness, amount of face that is red, sensation of warmth, and sensation of burning) rated on a 5-point scale (0, absence of symptoms, to 4, most severe symptoms).
The survey included one instrument that assesses QoL, the IA-RFR, and one instrument that assesses HRQoL, the DLQI. The IA-RFR scale is a validated [13] instrument that consists of four domains (self-perception, emotional, grooming, and social) derived from eight individual items (i.e., questions) that ask participants to rate the impacts of their facial redness over the past 7 days on a 5-point scale (0, no negative impact, to 4, high negative impact). Scores for all IA-RFR items were transformed to a scale from 0 (no negative impact) to 100 (highest negative impact). The overall impact score for the IA-RFR was calculated as the mean of all individual item scores. The DLQI is a validated 10-item questionnaire that assesses the impact of dermatological conditions on HRQoL over the last week [14] across six domains (symptoms and feelings, daily activities, leisure, personal relationships, work and school, and treatment). The total DLQI score, which uses a scale of 0–30, is calculated by summing the scores of all individual items. Total DLQI score ranges reflect the following levels of impact on skin-related HRQoL: score of 0–1, no effect; 2–5, small effect; 6–10, moderate effect; 11–20, very large effect; and 21–30, extremely large effect on skin-related HRQoL [15, 16].
Statistical Analysis
Analyses were performed on the population of evaluable respondents, which included eligible respondents who completed the entire survey. Sociodemographic and clinical characteristics and IA-RFR and DLQI scores were summarized descriptively for the evaluable analysis population as well as by severity of erythema (mild, moderate, or severe redness on face at screening). P values were calculated from analysis of variance for continuous outcomes, the Pearson chi-squared test for categorical outcomes with expected cell counts greater than 5, and the Fisher exact test for categorical outcomes with expected counts of 5 or less. Limited inferential analyses were conducted for key outcomes, with statistical significance for all comparisons set at P < 0.05.
Results
Participants
A total of 6967 invitees responded to the survey invitations, of whom 921 respondents were eligible to participate in the survey and 708 completed the survey. Of those respondents who did not qualify to participate, 62.4% (3773/6046) dropped out of the survey prior to completing the screening questions and 30.9% (1871/6046) met an exclusion criterion.
Survey respondents were primarily white/Caucasian, female, and had a mean [standard deviation (SD)] age of 52.4 (14.7) years. Most of the respondents reported an education level exceeding that of a high school diploma. The majority had private medical insurance. Ninety percent of participants reported having a Fitzpatrick skin phototype of I (very fair skin) to III (medium skin) (Table 1).
Symptoms
The mean reported age of first awareness of rosacea symptoms was 36.6 years (range 3–74 years) and the mean (SD) time since diagnosis of rosacea was 11.9 (8.5) years. The majority of respondents reported that the severity of their facial erythema was mild [59.2% (419/708)] or moderate [33.2% (235/708)]; 7.6% (54/708) reported that erythema was severe. Approximately one-third of respondents reported having four or more inflammatory bumps or pimples.
The most commonly reported rosacea symptoms were flushing that lasts longer than 10 min (84.0%) and persistent facial erythema in the central part of the face (69.1%). The most bothersome rosacea symptoms were persistent facial redness (69.2%), blushing or flushing (60.9%), and bumps or pimples (53.5%). Among respondents with moderate or severe erythema, nearly all reported that persistent facial redness was their most bothersome symptom (Fig. 1). Burning or stinging skin was the most bothersome symptom for over half of respondents with severe erythema and nearly half of those with moderate severity erythema.

Most bothersome symptoms of rosacea by severity of erythema. Respondents could report multiple bothersome symptoms
Respondents with severe facial erythema reported greater severity of symptoms in response to all questions on the Symptom Assessment for Rosacea Facial Redness, including degree of redness, amount of face that is red, and sensations of warmth and burning (P < 0.0001 for effect of severity category; Fig. 2). Facial warmness was rated “quite a bit” or “very” severe by 4.3% of respondents with mild erythema, 15.7% of respondents with moderate erythema, and 38.9% of respondents with severe erythema. Facial burning was rated “quite a bit” or “a lot” by 3.6% of respondents with mild erythema, 8.9% of respondents with moderate erythema, and 37.0% of respondents with severe erythema.

Symptom Assessment for Rosacea Facial Redness responses by severity of erythema (mild, n = 419; moderate, n = 235; severe, n = 54). *P < 0.0001 for effect of erythema severity category, based on the Fisher exact test
Quality of Life
Mean IA-RFR scores showed the impacts of erythema across all levels of severity (Fig. 3). Total and individual domain IA-RFR scores (self-perception, emotional, grooming, social) showed a significant impact of severity of erythema of rosacea, with an upward trend in score with increasing level of erythema severity (P < 0.0001 for total and all individual domains).

Mean scores from the Impact Assessment for Rosacea Facial Redness scale by severity of erythema. *P < 0.0001 for effect of erythema severity category, based on ANOVA type III sums of squares by severity
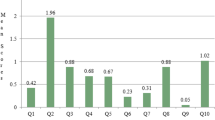
Total DLQI scores showed that rosacea had negative impacts on HRQoL in respondents with mild to severe erythema, with greatest impacts observed in those with severe erythema (Fig. 4). The mean (SD) total DLQI score was 5.2 (6.0) for all respondents and was significantly different between respondents with severe [13.4 (8.9)], moderate [5.7 (5.4)], and mild erythema [3.8 (4.9); P < 0.0001]. Among those with severe erythema, the majority had a total DLQI value that indicated a very large effect (31.5%) or extremely large effect (29.6%) of rosacea on their HRQoL. Mean scores for all individual DLQI domains were significantly different across erythema severity categories (P < 0.0001), and scores increased with increasing level of erythema severity (Fig. 4).

Mean overall and individual domain scores from the Dermatology Life Quality Index based on the severity of erythema. HRQoL health-related quality of life. *P < 0.0001 for effect of erythema severity category based on ANOVA type III sums of squares by severity. aOverall score ranges from 0 to 30. bDomain score ranges from 0 to 6. cDomain score ranges from 0 to 3
Discussion
With the outreach and recruitment efforts of the NRS, this study exceeded its recruitment goal, obtaining completed surveys from more than 700 respondents with self-reported physician-diagnosed rosacea and mild to severe facial erythema. Results from two assessment instruments, the IA-RFR and the DLQI, showed that rosacea has substantial negative impacts on several aspects of the quality of patients’ lives.
Responses to the IA-RFR scale demonstrated QoL impacts of facial erythema associated with rosacea in respondents with mild, moderate, and severe erythema, with the highest impacts observed in the self-perception, emotional, and grooming domains. A similar pattern of IA-RFR scores was reported in a previous Web-based survey study of patients with erythematotelangiectatic and papulopustular rosacea [9]. In the current study, respondents with more severe erythema reported greater impact across all IA-RFR scale domains. Thus, this study provides further evidence that facial erythema of rosacea has a substantial impact on QoL, with even greater impacts associated with greater severity.
The DLQI results showed that rosacea has substantial impacts on daily HRQoL. The mean total DLQI in all respondents was 5.2, indicating that facial erythema of rosacea has a small to moderate impact on skin-related HRQoL in the overall population of respondents with mild, moderate, or severe erythema [15, 16]. This DLQI value is generally within the range of values previously reported in populations that included patients with all severities of rosacea (4.1–7.6) [17,18,19,20] and is comparable to mean DLQIs reported in patients with acne (5.1–6.1) [21,22,23,24].
Mean DLQI values increased with increasing severity of erythema and approximately two-thirds of respondents with severe erythema had total DLQI scores that indicated a “very large” or “extremely large” effect of rosacea on HRQoL. The mean total DLQI in respondents with severe erythema (13.4) reflects a very large effect on HRQoL [15, 16] and is higher than values previously reported in patients with severe rosacea (8.6–10.0) [19, 25]. The level of HRQoL impact observed in patients with severe erythema is comparable to that observed in patients with eczema (mean DLQI, 7.1–11.3) [22, 26,27,28,29], atopic dermatitis (8.5–10.7) [30,31,32,33], and psoriasis (7.8–12.0) [22, 34,35,36,37,38,39].
This survey cohort tended to be better educated than the general population. More than 90% of survey participants had a level of education that exceeded a high school diploma, whereas fewer than 60% of US adults aged older than 25 years had at least some college education in 2015 [40]. However the observed educational profile is comparable to that reported in a previous survey of a large cohort of adults with rosacea, which found that more that 91% of participants had education beyond a high school diploma [10]. The reasons for these sociodemographic differences are unclear, but may be attributable to possible selection bias that could have been introduced by the Web-based recruitment methodology.
A possible limitation of this study is that the study placed a temporary cap on the number of mild severity patients eligible to participate in the survey during survey fielding to ensure adequate recruitment of respondents with moderate and severe erythema. Therefore, the prevalence of mild, moderate, and severe erythema is not reflective of the prevalence in the general population of patients with rosacea. In addition, clinical information was collected from respondent self-reports; neither physician records nor diagnostic information was available to confirm information reported by respondents (e.g., physician diagnosis and severity of erythema). Finally, the recruitment method for the survey may have favored patients who found their erythema bothersome, as evidenced by their visits to the NRS website.
Conclusions
Rosacea has wide-ranging negative effects on HRQoL, including psychosocial well-being in individuals who have mild, moderate, or severe facial erythema of rosacea. These effects, including impacts on self-perception and emotional, social, and overall well-being, were significantly greater in respondents with severe erythema of rosacea. These findings may provide insight and guidance to encourage physicians to consider QoL outcomes when treating patients with rosacea.
Abbreviations
- ANOVA:
-
Analysis of variance
- DLQI:
-
Dermatology Life Quality Index
- HRQoL:
-
Health-related quality of life
- IA-RFR:
-
Impact Assessment for Rosacea Facial Redness
- NRS:
-
National Rosacea Society
- QoL:
-
Quality of life
- SD:
-
Standard deviation
- US:
-
United States
References
Gether L, Overgaard LK, Egeberg A, Thyssen JP. Incidence and prevalence of rosacea: a systematic review and meta-analysis. Br J Dermatol. 2018;179:282–9.
Tan J, Schofer H, Araviiskaia E, Audibert F, Kerrouche N, Berg M. Prevalence of rosacea in the general population of Germany and Russia—the RISE study. J Eur Acad Dermatol Venereol. 2016;30:428–34.
Baldwin HE. Diagnosis and treatment of rosacea: state of the art. J Drugs Dermatol. 2012;11:725–30.
Del Rosso JQ, Thiboutot D, Gallo R, et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 1: a status report on the disease state, general measures, and adjunctive skin care. Cutis. 2013;92:234–40.
Tan J, Berg M. Rosacea: current state of epidemiology. J Am Acad Dermatol. 2013;69:S27–35.
Su D, Drummond PD. Blushing propensity and psychological distress in people with rosacea. Clin Psychol Psychother. 2012;19:488–95.
National Rosacea Society. Coping with rosacea. 2016. http://www.rosacea.org/patients/materials/coping/managing.php#Managing. Accessed 29 Mar 2016.
Huynh TT. Burden of disease: the psychosocial impact of rosacea on a patient’s quality of life. Am Health Drug Benefits. 2013;6:348–54.
Zeichner JA, Eichenfield LF, Feldman SR, Kasteler JS, Ferrusi IL. Quality of life in individuals with erythematotelangiectatic and papulopustular rosacea: findings from a web-based survey. J Clin Aesth Dermatol. 2018;11:47–52.
Del Rosso JQ, Tanghetti EA, Baldwin HE, Rodriguez DA, Ferrusi IL. The burden of illness of erythematotelangiectatic rosacea and papulopustular rosacea: findings from a web-based survey. J Clin Aesth Dermatol. 2017;10:17–31.
Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869–71.
Ferrusi IL, Ahluwalia G, Andrae DA. Development and validation of the symptom assessment for rosacea facial redness (SA-RFR) [abstract 5677]. J Am Acad Dermatol. 2017;76:AB99.
Ferrusi IL, Ahluwalia G, Andrae DA. Patient-rated impact assessment for rosacea facial redness (IA-RFR): results of two phase 3 pivotal trials of oxymetazoline cream 1% vs vehicle [abstract PSS26]. Value Health. 2017;20:A160.
Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)—a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19:210–6.
Basra MK, Fenech R, Gatt RM, Salek MS, Finlay AY. The Dermatology Life Quality Index 1994-2007: a comprehensive review of validation data and clinical results. Br J Dermatol. 2008;159:997–1035.
Hongbo Y, Thomas CL, Harrison MA, Salek MS, Finlay AY. Translating the science of quality of life into practice: what do Dermatology Life Quality Index scores mean? J Invest Dermatol. 2005;125:659–64.
Bohm D, Schwanitz P, Stock GS, Schmid-Ott G, Schulz W. Symptom severity and psychological sequelae in rosacea: results of a survey. Psychol Health Med. 2014;19:586–91.
Beikert FC, Langenbruch AK, Radtke MA, Augustin M. Willingness to pay and quality of life in patients with rosacea. J Eur Acad Dermatol Venereol. 2013;27:734–8.
Aksoy B, Altaykan-Hapa A, Egemen D, Karagoz F, Atakan N. The impact of rosacea on quality of life: effects of demographic and clinical characteristics and various treatment modalities. Br J Dermatol. 2010;163:719–25.
Wu Y, Fu C, Zhang W, Li C, Zhang J. The Dermatology Life Quality Index (DLQI) and the hospital anxiety and depression (HADS) in Chinese rosacea patients. Psychol Health Med. 2018;23:369–74.
Zachariae R, Zachariae C, Ibsen H, Mortensen JT, Wulf HC. Dermatology life quality index: data from Danish inpatients and outpatients. Acta Derm Venereol. 2000;80:272–6.
Parna E, Aluoja A, Kingo K. Quality of life and emotional state in chronic skin disease. Acta Derm Venereol. 2015;95:312–6.
Richter C, Trojahn C, Hillmann K, et al. Sensitivity to change of the Dermatology Life Quality Index in adult females with facial acne vulgaris: a validation study. J Eur Acad Dermatol Venereol. 2017;31:169–74.
Alanazi MS, Hammad SM, Mohamed AE. Prevalence and psychological impact of Acne vulgaris among female secondary school students in Arar city, Saudi Arabia, in 2018. Electron Phys. 2018;10:7224–9.
Bewley A, Fowler J, Schofer H, Kerrouche N, Rives V. Erythema of rosacea impairs health-related quality of life: results of a meta-analysis. Dermatol Ther (Heidelb). 2016;6:237–47.
Boehm D, Schmid-Ott G, Finkeldey F, et al. Anxiety, depression and impaired health-related quality of life in patients with occupational hand eczema. Contact Dermat. 2012;67:184–92.
Ghaderi R, Saadatjoo A. Quality of life in patients with hand eczema as health promotion: a case control study. Acta Dermatovenerol Croat. 2014;22:32–9.
Cortesi PA, Scalone L, Belisari A, et al. Cost and quality of life in patients with severe chronic hand eczema refractory to standard therapy with topical potent corticosteroids. Contact Dermat. 2014;70:158–68.
Lindberg M, Bingefors K, Meding B, Berg M. Hand eczema and health-related quality of life; a comparison of EQ-5D and the Dermatology Life Quality Index (DLQI) in relation to the Hand Eczema Extent Score (HEES). Contact Dermatitis. 2013;69:138–43.
Beikert FC, Langenbruch AK, Radtke MA, Kornek T, Purwins S, Augustin M. Willingness to pay and quality of life in patients with atopic dermatitis. Arch Dermatol Res. 2014;306:279–86.
Kim DH, Li K, Seo SJ, et al. Quality of life and disease severity are correlated in patients with atopic dermatitis. J Korean Med Sci. 2012;27:1327–32.
Misery L, Finlay AY, Martin N, et al. Atopic dermatitis: impact on the quality of life of patients and their partners. Dermatology. 2007;215:123–9.
Holm EA, Esmann S, Jemec GB. Does visible atopic dermatitis affect quality of life more in women than in men? Gend Med. 2004;1:125–30.
Moradi M, Rencz F, Brodszky V, Moradi A, Balogh O, Gulacsi L. Health status and quality of life in patients with psoriasis: an Iranian cross-sectional survey. Arch Iran Med. 2015;18:153–9.
Palotai T, Szepietowski JC, Pec J, et al. A survey of disease severity, quality of life, and treatment patterns of biologically naive patients with psoriasis in central and eastern Europe. Acta Dermatovenerol Croat. 2010;18:151–61.
Schoffski O, Augustin M, Prinz J, et al. Costs and quality of life in patients with moderate to severe plaque-type psoriasis in Germany: a multi-center study. J Dtsch Dermatol Ges. 2007;5:209–18.
Martinez-Garcia E, Arias-Santiago S, Valenzuela-Salas I, Garrido-Colmenero C, Garcia-Mellado V, Buendia-Eisman A. Quality of life in persons living with psoriasis patients. J Am Acad Dermatol. 2014;71:302–7.
Cakmur H, Dervis E. The relationship between quality of life and the severity of psoriasis in Turkey. Eur J Dermatol. 2015;25:169–76.
Mohd Affandi A, Khan I, Ngah Saaya N. Epidemiology and clinical features of adult patients with psoriasis in Malaysia: 10-year review from the Malaysian Psoriasis Registry (2007–2016). Dermatol Res Pract. 2018;2018:4371471.
Ryan CL, Bauman K. Educational attainment in the United States: 2015. https://www.census.gov/content/dam/Census/library/publications/2016/demo/p20-578.pdf. Accessed 12 Apr 2016.
Acknowledgements
The authors thank the National Rosacea Society for their collaboration in conducting the survey, and the patients who participated.
Funding
This study and the journal’s Rapid Service Fee were sponsored by Allergan plc, Dublin, Ireland. Neither honoraria nor other forms of payments were made for authorship.
Medical Writing Assistance
Writing and editorial assistance was provided to the authors by Jennifer Darby of Peloton Advantage, Parsippany, NJ, and was funded by Allergan plc.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis, and have given their approval for this version to be published.
Disclosures
Julie Harper serves as an investigator for Allergan plc. Hilary E. Baldwin serves as an investigator for Allergan plc. Sarah Baradaran is an employee of Allergan plc and may own stock/stock options in the company. Vaishali Patel is an employee of Allergan plc and may own stock/stock options in the company.
Compliance with Ethics Guidelines
The Chesapeake Institutional Review Board (IRB) determined that this study met the regulatory criteria for exemption from IRB oversight using the Department of Health and Human Services regulations Title 45 CFR Part 46.101(b)(2). The study was conducted in accordance with the requirements for studies involving human respondents and regulatory guidelines. Respondents were required to provide informed consent through a Web link opt-in process prior to completing a series of demographic and screening questions that assessed eligibility.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Digital Features
To view enhanced digital features for this article go to https://doi.org/10.6084/m9.figshare.9746240.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License ( http://creativecommons.org/licenses/by-nc/4.0/ ), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Baldwin, H.E., Harper, J., Baradaran, S. et al. Erythema of Rosacea Affects Health-Related Quality of Life: Results of a Survey Conducted in Collaboration with the National Rosacea Society. Dermatol Ther (Heidelb) 9, 725–734 (2019). https://doi.org/10.1007/s13555-019-00322-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-019-00322-5