
Abstract
Objectives
The aim of this study is to evaluate the prevalence, associated factors, and time for diabetic retinopathy (DR) development in Ecuadorian patients with type 2 diabetes (DM2) followed for 10 years.
Methods
A retrospective cohort study between 2007 and 2017 included 487 patients with DM2 who had at least one dilated fundus eye examination in Diabetes Center in a primary-health-care level followed up for ten years. Data was collected from clinical records. Sociodemographic and laboratory variables were analysed, determining their association (mean difference and bivariate logistic regression) with DR. Survival time was calculated through life tables and Kaplan-Meier analysis.
Results
The prevalence of DR was 19.95% during the 10-year follow-up period. The median time for developing DR was 28.53 (95% CI: 26.89–27.05), showing that 50% of patients have the risk (HR: 4.57) to develop DR in the third decade of DM disease diagnosis. The significant risk factors for progression of DR were duration of DM2, high glycosylated hemoglobin level > 7% (HbA1c Expβ: 1.709, 95% CI: 1.00–2.89), systemic hypertension (HNT Expβ: 2.348 Expβ: 2.348 95% CI: 1.17–4.70%) 95% CI: 1.17–4.70%), low glomerular filtration rate (Expβ: 1.805, GFR, < 60 ml/min/sc1.73) (95% CI: 1.10–2.94) and albuminuria (Expβ: 2.48 Expβ: 2.48 95% CI: 1.49–4.13).
Conclusions
Half of the patients with DM2 treated in a primary level of care will develop DR in the third decade of the disease. There are risk factors related to development of DR, such as low GFR, high HbA1c, albuminuria and HTN. Low GFR, high HbA1c, albuminuria and high blood pressure are related with the presence of retinopathy in diabetes patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Diabetic retinopathy (DR) is a complication present in 30% of the people diagnosed with diabetes, and it is the leading cause of vision loss in working-age adults. In Ecuador, the prevalence of type 2 diabetes mellitus (DM2) is between 3.5 and 8.5% [1], and a local study has reported that the prevalence of DR is 14.8% approximately [2].
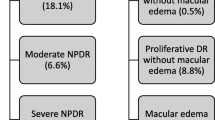
DR is caused by chronic hyperglycemia damaging the retinal microvasculature. The microvascular repercussion at the retinal capillary level (loss of pericytes, basement membrane thickness, and microaneurysms) is the most common consequence of DM2 in the eyes. DR can be classified as non-proliferative diabetic retinopathy (NPDR), proliferative diabetic retinopathy (PDR), and diabetic macular edema (DME) [3].
This study aimed to determine the prevalence and associated DR factors, and the survival time for developing DR in an Ecuadorian population with DM2 at the primary level of care.
Materials and methods
This retrospective cohort study included 697 patients with DM2 followed for 10 years from January 2007 to December 2017 registered at the Chimbacalle Primary Care Health Center in Quito, Ecuador. Participants were included if they were diagnosed with DM2 by the American Diabetes Association (ADA) criteria [4]. Additionally, participants must have medical and laboratory records for a minimum period of 1 year from the baseline, including total cholesterol (TC), high-density lipoproteins (HDL), low-density lipoproteins (LDL), triglycerides (Tg), glycated hemoglobin (HbA1c), urea, creatinine and albuminuria. Moreover, electrocardiogram [EKG] exam, glomerular filtration rate, calculated with the CKD-EPI formula, and at least one ocular fundus during the study should have been recorded. Participants with type 1 diabetes mellitus diagnosis, under 18 years old, pregnant women, incomplete data in clinical records (n = 48), patients without ocular fundus exam (n = 157) and those previously diagnosed with any chronic ocular disease or blindness were excluded. After exclusion criteria, 487 (69.87%) participants with DM2 remained in the study (Fig. 1).

Flow diagram of eligible participants in the study
Retinopathy ascertainment
The ophthalmological examination included visual acuity with and without correction, ocular movements, intraocular pressure, biomicroscopy with a slit lamp, ocular fundus with 78 Dp lenses and indirect ophthalmoscopy. Both retina and vitreous were examined, and DR was diagnosed if signs of capillary microaneurysms, cotton-wool spots, dots or blot retinal hemorrhages, hard exudates, macular edema, venous dilation and intraretinal microvascular abnormalities were found in the ophthalmoscopic exam by a trained ophthalmologist.
Diabetes-related variables
Covariates were selected based on the previously published evidence of their relationship with DR. Covariates included sex, age at DM2 diagnosis, DM duration length in years, smoking status (non-smoker, former or current smoker), hypertension status, body mass index (BMI) calculated as weight divided by height squared in meters (kg/m2) and categorized using 25 kg/m2 as cut-off point. Biochemical test information included HbA1c (> 7%), albuminuria (normal/high), TC (> 200 mg/dl) and HDL (> 45 mg/dl for men and > 50 mg/dl for women). Additionally, glomerular filtration rate (GFR) was calculated and categorized (< 60 ml/min/m2). Systolic and diastolic blood pressure were measured in mmHg by trained personal and arterial hypertension (HTN) was defined according to the Eighth Joint National Committee criteria [5].
Statistical analysis
Participant’s characteristics were summarized according to sex. The mean and standard deviation were calculated for quantitative variables, and the relative and absolute frequencies were calculated for qualitative variables.
Furthermore, participants were divided into two groups according to their DR diagnosis status (Retinopathy Yes/No). The statistical differences were calculated using t Student for parametric, and the Mann-Whitney U for non-parametric quantitative variables, and the χ2 was used for qualitative variables.
For survival analysis, the survival time for the development of DR was the interval between the index time (age at diagnosis of DM2) and the occurrence of the event of interest (diagnosis of DR) or the end of follow-up (December 31, 2017). Life tables were used to estimate the survival time for developing DR.
Binary logistic regression analysis included those variables that were statistically significant in the univariate analysis. All statistical analyses were considered p values < .05 statistically significant and were performed using the statistical software package IBM SPSS Statistics version 23.
Results
Among the 487 patients included in the study, the mean age was 65.82 years, ranging from 31 to 97 years. The mean DM duration was 13.16 years, with 55% (n = 268) of individuals showing a history of DM over 10 years. Additionally, 73.6% (n = 358) had high blood pressure as comorbidity (Table 1).
Overweight was found in 42.5% (n = 207) of the patients, and 38.2% (n = 186) presented some degree of obesity according to their BMI. Regarding glucose levels, 62.4% (n = 304) presented HbA1c higher than 7%. Additionally, concerning lipid profile components, 72.7% (n = 354) individuals showed TC levels under 200 mg/dl, 69.8% (n = 340) had LDL levels less than 100 mg/dl and 51.3% (n = 250) presented inadequate triglyceride values (above 150 mg/dl). On contrast, 83.8% (n = 408) presented HDL values within normal parameters (Table 1).
The behavior of DR was analysed with the sociodemographic characteristics and risk factors. For the year 2017, the prevalence of retinopathy was of 19.95% (n = 96); within the bivariate analysis, we found that the time of disease and time of appearance of DR were significant as well as the presentation of AHT (95% CI: 1.17–4.70%) and control of HbA1c (95% CI: 1.00–2.89), also show a significant association with decreased renal function (Table 2).
Among all patients, 96 (19.95%) participants developed DR (n = 96) in the follow-up time. Comparing patients with DR with patients without DR, statistically significant differences were found in age at DM diagnosis, renal function, HBA1c, HDL, blood pressure and categorized TC (Table 2).
In the survival analysis to determine the presence of DR by 10-year period, results showed that 50% of patients would develop DR in the third decade of DM disease (28.56 years) with a 4.57 times increased risk (HR:4.57) (Table 3 and Fig. 2).

Survival curve
Among the variables statistically significant in the univariate analysis, the binary logistic regression results showed an association between DR and renal function TFG_CKD < 60 ml/min (Expβ: 1.805, 95% CI: 1.04–2.949, p value: < .018), HbA1c (Expβ: 1.709, 95% CI: 1.01–2.89, p: .047), HTN (Expβ: 2.348, 95% CI: 1.17–4.71, p value .016), and albuminuria (Expβ: 2.48, 95% CI: 1.495–4.139, p value:.000) (Table 4).
Discussion
Globally, the mean prevalence of DR is 25.2%, with the highest among Hispanic countries which range around 30% [6]. Epidemiological studies showing the prevalence of DR have not been conducted in Ecuador, highlighting the importance of this study, focusing on reliable data in a population diagnosed with DM2 at a primary level of care.
This study has shown that the prevalence of DR was 19.5% in a DM2 population, with a mean DM2 duration of 13.16 years. This prevalence is lower than other Latin American countries’ reported prevalence of 30% [6]. An analysis of 35 studies conducted in 22,896 people with diabetes on several continents reported a DR global prevalence of 25.2% [6]. In some European countries, the prevalence is slightly higher, ranging from 30 to 40% [7]. According to Varma et al., the prevalence is higher in the Hispanic population [8]. Furthermore, the prevalence in Peru and Chile has been reported at 25.9% and 24.78%, respectively. The authors of these studies have theorized that the reasons may be due to some genetic or obesogenic factors [9, 10].
Factors such as duration of DM, presence of HTN, decrease in GFR, and high values of HbA1c were found significantly associated with DR, as previous evidence has been published.
Therefore, the longer the time of being with DM2, is more likely to develop DR. A study by Zhang et al. conducted in the USA reported that each year of DM2 represents a 6% increase in the likelihood of DR [11].
Furthermore, increased systolic and diastolic blood pressure measurements, regardless of the type of diabetes, were found to increase the risk of DR [12]. Diastolic blood pressure was also an independent predictor of DR in patients with DM2. The United Kingdom Prospective Diabetes Study (UKPDS) showed reduced microvascular complications and visual loss when lowering blood pressure [13, 14].
The prevalence of albuminuria in diabetic patients is 15% to 20%: it is a risk marker for renal and cardiovascular disease and severe ocular morbidity [15]. Evidence has shown that DM2 patients with microalbuminuria were more likely to have retinopathy than those without microalbuminuria [16]. Also, it has been reported that about 45% of diabetic patients with albuminuria have some degree of DR [17].
Adequate and continuous control of blood glucose levels in DM2 patients might directly reduce the risk of long-term DR shown in the UKPDS study [12]. In contrast, inadequate glucose control, measured by HbA1c, increases the risk of early DR development, as shown in the ACCORD and ADVANCE studies [18].
To the best of our knowledge, this is the first study conducted in the Ecuadorian DM2 population at the primary level of care and has the potential of becoming a reference retinopathy study in a developing country like Ecuador due to the sociodemographic characteristics of the population. The study also emphasizes the need to have a good and comprehensive care of DM2 to prevent the development of microvascular complications like DR. For this purpose, strict control of the metabolic profile and blood pressure from the moment of diagnosis according to the recommendations of the guidelines is necessary. Furthermore, the authors highlight the importance of having a reliable method to identify patients at the highest risk of DR. Periodic visual controls allow an effective intervention before vision loss occurs.
Among the limitations, we found that it is not a prospective design work of a single cohort, and that the data was gathered in a primary care clinic; therefore, these findings cannot be extrapolated to the general population. However, the results could be applied in patients with a similar context, as the one in the present study. This means a primary care center of the public health system, which focuses on national and international diabetes control recommendations. However, the study has the strength of being a reference in a developing country like Ecuador because of the population and sociodemographic characteristics.
It should be noted that these results could also be attributed mainly to the fact that patients were permanently treated with first-line drugs (ODA) for treatment, including insulin, which in this country are distributed free of charge, thus affordable to all patients.
In conclusion, a low rate of DR is observed due to adequate follow-up and compliance with therapeutic goals in a diabetes clinic. In a primary level of care diabetes clinic, half of its patients will develop DR by the end of the third decade of disease. Important factors to consider when analysing the risk of developing DR include AHT, HbA1c, renal function, age at diagnosis, and time with DM2.
References
Cho NH, Shaw JE, Karuranga S, Huang Y, da Rocha Fernandes JD, Ohlrogge AW, Malanda B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–81. https://doi.org/10.1016/j.diabres.2018.02.023.
Romero-Naranjo F, Espinosa-Uquillas C, Gordillo-Altamirano F, Barrera-Guarderas F. Which Factors may reduce the health-related quality of life of ecuadorian patients with diabetes? P R Health Sci J. 2019;38(2):102–8. PMID: 31260554
Wu L, Fernandez-Loaiza P, Sauma J, Hernandez-Bogantes E, Masis M. Classification of diabetic retinopathy and diabetic macular edema. World J Diabetes [Internet]. 2013;4(6):290–4. https://doi.org/10.4239/wjd.v4.i6.29.
American Diabetes Association. Standards of Medical in Diabetes. Diabetes Care. 2017;40(January):s33–43. PMID:27979885
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E. 2014 Evidence-based guideline for the management of high blood pressure in adults. JAMA. 2014;311:507. https://doi.org/10.1001/jama.2013.284427.
Ting DS, Cheung GC, Wong TY. Diabetic retinopathy: global prevalence, major risk factors, screening practices and public health challenges: a review. Clin Exp Ophthalmol. 2016;44(4):260–77. https://doi.org/10.1111/ceo.12696.
Yau JW, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–64. https://doi.org/10.2337/dc11-1909.
Varma R, Paz SH, Azen SP, et al. The Los Angeles Latino Eye Study: design, methods, and baseline data. Ophthalmology. 2004;111(6):1121–31. https://doi.org/10.1016/j.ophtha.2004.02.001.
Adrianzén RE, Rioja M, Manrique A. Frequency and severity of diabetic retinopathy in patients with type 2 diabetes mellitus at the regional institute of Ophthalmology. Rev Peru Med Exp Salud Publica. 2019;36(2):260–4. https://doi.org/10.17843/rpmesp.2019.362.4076.
Abuauad S, Guzmán P, Urzúa C. Prevalencia de retinopatía diabética y edema macular en población diabética del CESFAM Cordillera Andina de Los Andes. Rev Chil Salud Pública. 2014;18(1):81. https://doi.org/10.5354/0719-5281.2014.30759.
Zhang X, Saaddine J, Chou C, et al. Prevalence of diabetic retinopathy in the United States, 2005-2008. JAMA - J Am Med Assoc. 2010;304:649–56. https://doi.org/10.1001/jama.2010.1111.
King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br. J. Clin. Pharmacol. 1999;48(5):643–8. https://doi.org/10.1046/j.1365-2125.1999.00092.x.
Klein R, Klein BE. Blood pressure control and diabetic retinopathy. The British journal of ophthalmology. 2002;86(4):365–7. https://doi.org/10.1136/bjo.86.4.365.
Rajalakshmi R, Amutha A, Ranjani H, et al. Prevalence and risk factors for diabetic retinopathy in Asian Indians with young onset Type 1 and Type 2 Diabetes. J Diabetes Complications. 2014;28(3):291–7. https://doi.org/10.1016/j.jdiacomp.2013.12.008.
Asensio-Sánchez VM, Rodríguez-Delgado B, García-Herrero E, Cabo-Vaquera V, García-Loygorri C. Microalbuminuria y retinopatía diabética [Microalbuminuria and diabetic retinopathy]. Arch Soc Esp Oftalmol. 2008;Feb;83(2):85–8. Spanish. https://doi.org/10.4321/s0365-66912008000200005.
Cruickshanks K, Ritter L, Klein R, et al. The association of microalbuminuria with diabetic retinopathy. The Wisconsin Epidemiologic Study of Diabetic Retinopathy. Ophthalmology. 1993;100(6):862–7. https://doi.org/10.1016/s0161-6420(93)31562-9.
Trevisan R, Vedovato M, Mazzon C, et al. Concomitance of diabetic retinopathy and proteinuria accelerates the rate of decline of kidney function in type 2 diabetic patients. Diabetes Care. 2002;25(11):2026–31. https://doi.org/10.2337/diacare.25.11.2026.
Stitt A, Curtis T, Chen M, et al. The progress in understanding and treatment of diabetic retinopathy. Prog Retin Eye Res. 2016;51:156–86. https://doi.org/10.1016/j.preteyeres.2015.08.001.
Acknowledgments
The authors thank the staff and the patients of Chimbacalle Medical Centre for their valuable contributions and trust throughout all these years.
Funding
The authors do not disclose receipt of the following financial support for the research, authorship, and publication of this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
This study was approved by the Institutional Review Board (IRB) of Central University of Ecuador (IRB ref number: 279-CE-UCE-2015). The study adhered to the tenets of the Declaration of Helsinki. All the patients gave their informed consent before the Ophthalmological Control was performed.
Conflict of interests
The authors declare no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Barrera-Guarderas, F., Flor, A.P., Coba-Loor, S. et al. Diabetic retinopathy: long-term follow-up of Ecuadorian patients with type 2 diabetes in primary care. Int J Diabetes Dev Ctries 43, 441–447 (2023). https://doi.org/10.1007/s13410-022-01109-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13410-022-01109-9