
Abstract
Background
Gastric Cancer (GC) presents poor outcome, which is consequence of the high incidence of recurrence and metastasis at early stages. GC patients presenting recurrent or metastatic disease display a median life expectancy of only 8 months. The mechanisms underlying GC progression remain poorly understood.
Methods
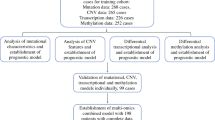
We took advantage of public available GC datasets from TCGA using GEPIA, and identified the matched genes among the 100 genes most significantly associated with overall survival (OS) and disease free survival (DFS). Results were confirmed in ACRG cohort and in over 2000 GC cases obtained from several cohorts integrated using our own analysis pipeline. The Kaplan-Meier method and multivariate Cox regression analyses were used for prognostic significance and linear modelling and correlation analyses for association with clinic-pathological parameters and biological hallmarks. In vitro and in vivo functional studies were performed in GC cells with candidate genes and the related molecular pathways were studied by RNA sequencing.
Results
High expression of ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 individually and as a signature was associated with poor prognosis and recurrent disease in GC. Moreover, the expression of ANKRD6 and ITIH3 was significantly higher in metastasis and their levels associated to Epithelial to Mesenchymal Transition (EMT) and stemness markers. In line with this, RNAseq analysis revealed genes involved in EMT differentially expressed in ANKRD6 silencing cells. Finally, ANKRD6 silencing in GC metastatic cells showed impairment in GC tumorigenic and metastatic traits in vitro and in vivo.
Conclusions
Our study identified a novel signature involved in GC malignancy and prognosis, and revealed a novel pro-metastatic role of ANKRD6 in GC.
Similar content being viewed by others


1 Introduction
Gastric cancer (GC) is the fifth most common cancer and the third leading cause of cancer death worldwide [1, 2]. Although the clinical management of GC has improved in the last decades and currently consists of surgical resection, chemoradiotherapy and targeted therapy [3], the prognosis is still dismal, with an average 5-year survival rate of around 20% [2]. This poor outcome is consequence of the high incidence of recurrence and metastasis. In this sense, around 30% of patients undergoing curative resection experiences recurrence within a year [4]. Moreover, a high proportion of patients (60%) undergoing resection display lymph node metastasis [5], even in early GC cases [6], whereas the 30–35% of the patients presents distant metastases spreading to the liver, peritoneum, lung, or bone at the time of diagnosis [7]. GC patients presenting recurrent or metastatic disease display a median life expectancy of only 8 months [8]. Altogether, this scenario points out the need of understanding the underlying molecular mechanisms of recurrence and metastasis in order to identify biomarkers for monitoring and suitable targets for prevention and inhibition.
GC is a heterogeneous disease influenced by different environmental factors and several genetic and epigenetic alterations. Traditionally, GC has been classified into intestinal and diffuse histological subtypes on the basis of the Lauren’s classification [9]. Over the past decade, advances in sequencing technology and high-throughput analysis delivered new insights and unravelled that GC presents high genetic and epigenetic molecular heterogeneity. Indeed, different consortiums, such as The Cancer Genome Atlas (TCGA) or the Asian Cancer Research Group (ACRG) carried out large scope studies, identifying critical driver genes and proposing molecular classifications of GC [10, 11 ]. Both consortiums identified four different molecular subtypes of GC and, in the case of the ACRG classification, the subtypes were associated with different survival rates and recurrence patterns [11]. These molecular studies helped to understand the biology of GC and represent very useful tools in basic research. However, although this knowledge exhibits potentially important clinical implications for disease diagnosis and treatment, the comprehension of its clinical connotations is a complex matter and these molecular classifications have not been translated in its current format into the clinic yet.
The main known risk factors for GC recurrence and metastasis are still related to the tumor stage, the extension of the surgery, the lymph node affectation, the tumor size and other non-molecular aspects [12,13,14], remaining the molecular determinants of GC progression unknown. In this scenario, we used the publicly available dataset of the GC patients from the TCGA cohort and identified the genes most significantly associated with GC prognosis. From this, and taking advantage of computational biology tools, additional patient datasets, clinical information and functional studies, we identified a novel gene signature related to recurrence and metastasis in GC, highlighting the special relevance of ANKRD6 and ITIH3, which represent novel potential biomarkers for GC progression, EMT and metastasis, as well as suitable targets for the improvement of the management of the disease.
2 Experimental procedures
2.1 Patient cohorts
The GEPIA tool was used to identify the genes most associated with survival in GC patients (http://gepia.cancer-pku.cn/detail.php?clicktag=survival2). We have analyzed data from GC patients cohorts previously published by the TCGA, Cristescu et al. (ACRG cohort) [11], Oh SC et al. (MDACC, KUCM, KUGH and MDACC cohorts) [15], Ooi CH et al. (Singapore cohort) [16], Lee et al. (SMC cohort) [17], Cheong JH et al. (Yonsei cohort) [18], and Cho JY et al. (YUSH cohort) [19]. We downloaded the public raw expression data and clinical data from the Gene Expression Omnibus (GEO) repository.
2.2 Processing of patient gene expression data
Processed Transcripts Per Million (TPM) expression data of the TCGA were downloaded with the TCGAbiolinks R package [20] prior to log2-normalization. Clinical data curated by the Genomic Data Commons (GDC) Data Portal were downloaded from Xena Browser [21]. Samples without OS data available were not included in the analyses.
All microarray data sets were pre-processed either by the Robust Multichip Average method for Affymetrix data with the oligo R package [22] or by quantile normalization for Illumina data before log2-transformation. Gene annotation data was obtained from BioMart, using the biomaRt R package [23], and for each data set and gene only the probe/bead that yielded the highest signal intensity value was used.
Microarray data were integrated first by sample-level standardization. Genes detected in at least 50% of the samples were kept, and missing expression data were imputed using nearest neighbour averaging with the R package impute. Those imputed values were subsequently eliminated after data set-derived batch effect removal using ComBat function of the sva R package. Standarized (Z-score) values were used in all patient analyses. Additionally, we downloaded log2(TPM+1) protein coding gene expression data from the DepMap Portal version 22Q2 [24].
2.3 Cell culture
The gastric cancer cell line MKN45 was cultured as an adherent monolayer with some single round cells or clumps in suspension at 37 °C and 5% CO2 in RPMI medium (Gibco) supplemented with 10% FBS (Gibco), 100 U/ml penicillin and 100 µg/mL streptomycin. For experiments, the adherent monolayer cells were used. Cultures were regularly tested for Mycoplasma.
2.4 ANKRD6 silencing
For ANKRD6 silencing by short hairpin RNA (shRNA), cells were infected with lentivirus harboring the TRCN0000158616 and TRCN0000162328 shANKRD6 plasmids (Sigma, St. Louis, MO, USA) and the corresponding pLKO.1 puro control plasmid #8453 (pLKO) from Addgene, a gift from Dr. Bob Weinberg. Lentiviral infections were performed for 6 h and selected with puromycin.
2.5 mRNA expression analysis
Total RNA was isolated using trizol (Life Technologies, Carlsbad, CA, USA). Reverse transcription was performed using the Maxima First Strand cDNA Synthesis Kit (ThermoFisher, Waltham, MA, USA) according to the manufacturer’s guidelines. Quantitative real-time PCR was performed in a CFX384 Thermal Cycler (Bio-Rad, Hercules, CA, USA) using Power SYBR® Green Master Mix (ThermoFisher), 10 mmol/L of primers and 20 ng of cDNA. GAPDH was used as housekeeping gene. Statistical analysis was performed based on ΔCT values.
2.6 Western blot
Protein lysates were resolved using sodium dodecyl sulfate-polyacrylamide gel electrophoresis and transferred to nitrocellulose membranes. The membranes were blocked and incubated overnight at 4 °C with primary antibodies against E-Cadherin (610181, BD Biosciences, San Jose, CA, USA), KRT18 (#4548, Cell Signaling Technology, Danvers, MA, USA) and β-actin (A5441, Sigma, St. Louis, MO, USA). Then, membranes were incubated with the corresponding secondary antibodies conjugated to horseradish peroxidase (HRP), and protein detection was performed using the NOVEX® ECL system (Invitrogen, Carlsbad, CA, USA) and the iBright Imaging system (ThermoFisher).
2.7 Immunofluorescence
Immunofluorescence was performed following standard procedures. Cells were seeded in 8-well immunofluorescence chamber slides (154534, LabTek ThermoFisher) and fixed with 4% PFA. Primary antibodies used were: cleaved-Caspase-3 (AF835, R&D Systems, Minneapolis, MN, USA), cleaved-PARP1 (ab32064, Abcam, Waltham, MA, USA), E-Cadherin (610181, BD Biosciences, San Jose, CA, USA) and KRT18 (#4548, Cell Signaling Technology). Secondary antibodies conjugated to fluorochromes were incubated and chromatin staining was performed with DAPI (D9542, Sigma). Cleaved-Caspase-3 and cleaved-PARP1 positive cells were counted manually and total number of cells were automatically quantified using the software for Bioimage Analysis QuPath v.0.4.3.
2.8 Immunohistochemistry
Subcutaneous tumors were fixed with 3.7% formaldehyde and embedded in paraffin blocks that were cut into 5-µm-thick sections. Primary antibodies used were: E-Cadherin (610181, BD Biosciences, San Jose, CA, USA), active Caspase-3 (AF835, R&D Systems, Minneapolis, MN, USA) and Ki67 (ab15580, Abcam, Waltham, MA, USA). Sections were incubated with secondary antibodies and the stains were visualized using 3,3′-diaminobenzidine (DAB, ab64238, Abcam, Waltham, MA, USA). Nuclei were counterstained with hematoxylin. Images were captured with a ZEISS Axioscan 7 slide scanner, and image analyses were performed using Qupath v.0.4.3. All nuclei were detected automatically. E-Cadherin intensity means were obtained and averaged per tumor for statistical analysis, active Caspase-3 positive cells were quantified manually, and Ki67 staining was detected automatically by setting an optical density threshold.
2.9 Proliferation
2·5×104 cells were plated in duplicate in 6-well-treated plates. At days 1, 3 and 5 after seeding, cells were harvested using 0.05% trypsin-EDTA and counted using a Neubauer chamber and an inverted optical microscope.
2.10 Migration and invasion
For migration and invasion transwell assays were used. Cells were starved for 24 h in serum-free medium. After that, migration was analyzed using Corning® Transwell® polycarbonate membrane inserts (#3422, Corning, NY, USA), and invasion was evaluated using the QCM™ Collagen Cell Invasion Assay of Millipore (ECM551, Burlington, MA, USA). Cells (10·104 cells for migration and 25·104 cells for invasion) were seeded into the upper compartment in medium without serum, and the inserts were placed in wells of 24-well flat bottom plates containing medium with 10% of a fetal bovine serum as chemo-attractant. After 96 h, the migrated and invading cells were fixed and stained according to the manufacturer’s protocol. Cells on the upper side of the chambers were wiped off using cotton swaps, and for quantification, the staining of cells situated in the undersurface of the membranes was dissolved and the absorbance was measured at 560 nm.
2.11 Cell cycle analysis by flow cytometry
The experiment was carried out immediately after antibiotic selection was complete. Cells were harvested using trypsin, washed with PBS and counted using a Neubauer chamber. 1·106 cells were fixed with 75% cold ethanol at −20 °C for at least 1 h, and incubated with 0.5% Triton X-100 and 25 µg/mL RNase A in PBS for 30 min at room temperature. Then, DNA was stained with 25 ng/mL propidium iodide for 15 min and samples were analyzed using a CytoFLEX flow cytometer (Beckman Coulter Co., Miami, FL, USA).
2.12 In vivo carcinogenesis assays
For subcutaneous xenografts, MKN45 cells were harvested with trypsin/EDTA and resuspended in PBS. 1 × 105 cells were injected subcutaneously into both flanks of Foxn1nu/Foxn1nu nude mice (8 weeks old). An external calliper was used to measure tumor size at the indicated time points, from which tumor volume was calculated according to the formula ½ (length × width2). Wilcoxon rank sum test was used to test the dimensions of the tumors independently for each day, and the global impact of ANKRD6 silencing with either of the shANKRD6 plasmids was assessed by a longitudinal linear mixed model.
2.13 RNA sequencing
Total RNA from pLKO and shANKRD6 MKN45 cells was isolated using trizol. For library preparation, the DNBSEQ Eukaryotic Stranded Transcriptome library preparation pipeline was followed. Sequencing data filtering was performed using the SOAPnuke software [25], developed by BGI. Data were aligned to the GRCh38.p13 reference genome using Bowtie2.
2.14 Functional enrichment analysis
The Gene Set Variation Analysis (GSVA) method [26] was used to assess the prognostic value of the gene signatures evaluated. The GSVA method was also applied to estimate the relative enrichment of the hallmark gene sets from the Molecular Signature Database [27] in the TCGA and ACRG cohorts. Differential enrichment analysis (DEA) was performed using DESeq2 [28], adjusting for the first principal component to remove unwanted variation and using the likelihood ratio test. Then hallmark Gene Set Enrichment Analysis was performed with the R package clusterProfiler [29].
2.15 Statistical analysis
The top-100 genes most correlated with OS and DFS in GC were identified using GEPIA (http://gepia.cancer-pku.cn/index.html) [30]. The prognostic value of ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 expression in GC was explored in the GC cohorts through Kaplan-Meier and multivariate Cox regression analyses. In the former, we used the best cut-off method implemented in the package survminer (https://cran.r-project.org/web/packages/survminer/index.html) to distribute the samples into high and low expression and GSVA score groups. In the latter, we used the uncut values in a model adjusted for age and TNM stage. The prognostic value of ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 expression in the different cancer types from the TCGA was assessed in a Cox univariate regression independently for each cohort without expression level grouping.
We used parametric (T-test or pairwise T-test p-value adjustment for variables with more than 2 groups) and non-parametric (Wilcoxon rank sum test or Dunnett’s test) tests to assess the relevance of the five genes in relation to the different clinic-pathological characteristics. We also used a paired T-test to analyse the differences in expression between GC tissue and normal gastric tissue in the ACRG cohort (N = 100).
The correlation between the expression of ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178, and the correlation of each with the expression of epithelial and mesenchymal markers, EMT inductors, stem cell regulators and hallmark enrichment scores were determined using the Spearman’s rank correlation test in GC tissue from patients of the TCGA and the ACRG cohorts. Correlation coefficients were grouped by hierarchical clustering based on Euclidean distance.
The p values were adjusted with the Benjamini-Hoichberg (BH) method when necessary, and statistical significance was considered when p < 0.05 (*p < 0.05, **p < 0.01, ***p < 0.001). All statistical analyses were conducted using R Statistical Software (v4.3.1; R Core Team 2023).
3 Results
3.1 Six transcripts match among the 100 most correlated with OS and DFS in GC
Using the GEPIA tool, we identified the top-100 transcripts most significantly associated with overall survival (OS) and disease-free survival (DFS) in the GC patients from the TCGA (n = 408) (Supplementary file 1). Among them, 6 were associated with both OS and DFS (Fig. 1A). These include the coding genes ANKRD6 (Ankyrin Repeat Domain 6), ITIH3 (inter-alpha-trypsin inhibitor heavy chain 3), SORCS3 (sortilin related VPS10 domain containing receptor 3), NPY1R (neuropeptide Y receptor Y1), CCDC178 (coiled-coil domain containing 178), and the long non-coding RNA AC002480.3. In particular, we focused on the 5 genes and we confirmed that their high individual expression was associated with reduced OS and DFS in the TCGA (Fig. 1B), results that were extended to the ACRG cohort (n = 299) (Fig. 1C). To further characterize their impact on survival, we performed a multivariate Cox proportional hazards regression model, adjusting for relevant factors including age and TNM tumor stage. This analysis revealed that the expression of the 5 genes represented an increased risk for OS in the TCGA patients (Fig. 1D), and these results were confirmed for ANKRD6, ITIH3, SORCS3 and NPY1R in the ACRG cohort (Fig. S1A). In relation to DFS, ANKRD6, ITIH3, NPY1R and CCDC178 represented also an increased risk for DFS in TCGA (Fig. S1B), and ANKRD6, ITIH3 and NPY1R in ACRG (Fig. S1C).

Prognostic potential of ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 in GC. A ANKRD6, ITIH3, SORCS3, NPY1R, CCDC178 and the lncRNA AC002480 are the common transcripts among the top-100 transcripts most significantly associated with OS and DFS in the GC TCGA cohort (STAD dataset analyzed in GEPIA). Kaplan-Meier plots of OS and DFS according to the expression of the 5 cited coding genes in the TCGA (B) and ACRG (C) cohorts using the best cut-off method for expression level stratification. D Forest plots showing multivariate Cox regression analysis for ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 expression in association with OS in the TCGA cohort, adjusting for age and TNM stage. E Expression of the identified genes in normal gastric tissue versus the corresponding paired GC tissue in ACRG patients stratified into high and low expression subgroups according to the cut-offs used in the OS analysis from C (N = 100). Kaplan-Meier plots of OS (F) and DFS (G) according to the score of the 5-gene GSVA signature composed by ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 in the TCGA (left) and ACRG (right) cohorts using the best cut-off method for GSVA score stratification. H Forest plot showing multivariate Cox regression analysis for the 5-gene GSVA score in association with OS in the TCGA cohort, adjusting for age and TNM stage (I). 5-gene GSVA score in normal gastric tissue versus the corresponding paired GC tissue in ACRG patients stratified into high and low score subgroups defined in the OS analysis from F (right) (N = 100)
We next compared their expression in tumor and normal gastric samples. For this, we distributed the cases between patients with high or low tumor expression of the genes according to the cut-offs used for survival. For the 5 genes, the expression in normal tissue was similar between the groups of low or high survival, but the trend observed in the tumor samples was different between these groups. Noteworthy, overexpression of ANKRD6, ITIH3 and SORCS3 was detected in tumor compared with control tissue in the patients presenting poor survival (Fig. 1E). On the contrary, cases with extended survival displayed lower levels of the 5 genes in the tumor compared to healthy tissue (Fig. 1E).
We wondered whether the identified genes could represent a malignant signature associated to cancer and studied their prognostic potential in additional cancer types. For this, we took advantage of publicly available datasets of TCGA studies, and analyzed 32 cancer types. This analysis revealed interesting results, as some of the genes were associated with poor prognosis in several cancer types (Fig. S2). For instance, the expression of ANKRD6 and ITIH3 was associated with reduced OS in colon carcinoma (COAD) and kidney renal papillary cell carcinoma (KIRP), and the expression of CCDC178 in bladder urothelial carcinoma (BLCA) and thyroid carcinoma (THCA).
Next, we performed a Gene Set Variation Analysis (GSVA) to obtain a global score corresponding to the combined expression of the 5 genes in GC. We explored the potential of the score to predict prognosis in both TCGA and ACRG cohorts, and using Kaplan-Meier estimator, we identified that the high score of the signature was associated to reduced OS (Fig. 1F) and DFS (Fig. 1G). Besides, multivariate Cox regression analyses showed that the score of the signature constituted an independent prognostic factor for OS after adjusting for the risk factors age and tumor stage in both cohorts. Notably, the Hazard Ratios (HRs) of the signature were superior to those of the 5 genes individually (Figs. 1H and S1D). Similar results were obtained with DFS (Fig. S1E, F). Moreover, when we analyzed paired tumor versus gastric healthy tissue samples, the signature score was significantly higher in those subsets of patients presenting poor outcome (Fig. 1I). Concerning the other cancer types, there was not a general pattern linking the expression of the 5 genes to survival in additional cancer types (Fig. S2). These results reveal that the 5 identified genes individually or as a signature serve as age- and tumor stage- independent prognostic factors in GC.
3.2 High expression of the identified genes correlated with tumor recurrence and metastasis in GC
Next, we analyzed the expression of the identified genes in the different TNM stages of the disease. Overall, the expression of the 5 genes individually increased gradually according to the stage, being the differences in expression among stages significant for ANKRD6, ITIH3 and NPY1R (Figs. 2A and S3A). Similarly, the signature also displayed significant differences (Figs. 2B and S3B). We also studied the expression of the genes in relation to recurrence and found that the expression of all of them individually or as a signature was significantly higher in the biopsies of those patients that underwent recurrence (Fig. 2C, D). Then, we explored their expression in the different molecular subtypes of GC proposed by the TCGA and the ACRG. This study unveiled that for all the genes, the MSI subtype presented the lowest expression in both cohorts (Fig. 2E). Of note, this subtype displayed the best prognosis in the ACRG classification, further indicating the link of the 5 genes with GC malignancy. Consistent with this idea, the highest expression of the 5 genes in the ACRG was registered in the MSS/EMT subtype, that with the poorest outcome and more prone to recur [10]. In the TCGA, the highest expression was detected in the genomically stable (GS) subtype (Fig. 2E), the one which is classified principally as MSS/EMT when the ACRG criteria are applied to the TCGA patients [10]. These results were reproduced by the 5-gene signature (Fig. 2F) and suggest a link with the process of EMT.

Association of ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 expression with clinic-pathological characteristics in TCGA and ACRG GC cohorts. Expression of the 5 genes individually (A) and as a GSVA signature (B) in the different tumor stages in the ACRG cohort (NI = 30, NII = 96, NIII = 95, NIV = 77). Expression of the 5 genes individually (C) and as a GSVA signature (D) in primary tumor tissue of patients who recurred (Yes) or not (No) after the primary therapy in the TCGA and ACRG cohorts (TCGA: NNo = 216, NYes = 58; ACRG: NNo = 157, NYes = 125). Expression of the 5 genes individually (E) and as a GSVA signature (F) in the different molecular subtypes of GC identified by the TCGA (top) and the ACRG (bottom). TCGA classification: MSI: GC with microsatellite instability (N = 55); EBV: Epstein-Barr virus-positive GC (N = 26) CIN: GC with chromosomal instability (N = 195), and GS: genomically stable GC (N = 42). ACRG classification: MSI: GC with microsatellite instability (N = 68); MSS/TP53+: microsatellite-stable with active TP53 (N = 79), MSS/TP53-: microsatellite-stable with inactive TP53 (N = 107); and EMT: microsatellite stable with epithelial-to-mesenchymal transition phenotype (N = 46). Expression of the 5 genes individually (G) and as a GSVA signature (H) in primary tumor tissue of patients presenting nodal dissemination (Node invasion) or not (N0) in ACRG. Node invasion group includes samples from N1 to N4 (NN0 = 38, NNode invasion = 262). I Spearman correlation between ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 in TCGA (left) and ACRG (right). Genes are grouped by hierarchical clustering. Red colour represents positive correlations (Colour figure online)
To characterize a potential interaction with metastasis, we investigated their link with lymph node dissemination and ascertained that the expression of the identified genes was higher in the patients of the ACRG exhibiting lymph node affectation, being the difference significant for ANKRD6 and ITIH3 (Fig. 2G). In the TCGA cohort, the differences, although less remarkable, confirmed the higher expression of ANKRD6 when the nodes are invaded (Fig. S3C). For the 5-gene signature we found a significantly higher expression in samples from patients exhibiting positive nodes in the ACRG cohort (Figs. 2H and S3D).
To further explore the association between the identified genes, we analyzed the Spearman correlation between the 5 genes in the TCGA and ACRG cohorts, finding a positive correlation for all the pairs of genes in both of them (Fig. 2I). Moreover, the highest correlations were observed between ANKRD6 with ITIH3 and NPY1R (Fig. 2I). Overall, these results reveal an association of the identified genes with metastasis, and postulate ANKRD6 and ITIH3 as the strongest genes within the signature.
3.3 Integrated analysis with data from 2000 GC patients across 9 independent cohorts confirms association with metastasis and recurrence
Next, with the aim of extending the study of the 5 genes in GC metastasis, we developed an analysis pipeline and we jointly analyzed available datasets corresponding to a total of 1908 GC patients from 9 independent cohorts (Table 1). We assessed the expression of the 5 genes in relation to metastasis, detecting significantly higher expression of ANKRD6 and ITIH3 in the samples belonging to patients suffering from metastatic disease (Fig. 3A). Furthermore, higher expression of ANKRD6, ITIH3 and NPY1R was also detected in the samples of the patients exhibiting recurrent disease (Fig. 3B). Since recurrence and therapy resistance are related processes, we explored the association of the genes with the survival specifically in treated patients, revealing reduced OS in treated patients with high ANKRD6, ITIH3 and NPY1R expression (Fig. 3C), and being the expression of ANKRD6 and NPY1R independent prognostic factors in treated patients (Fig. S4). We also studied in this large set of patients the association with survival and tumor stage to confirm the data obtained in the TCGA and ACRG cohorts. Notably, high levels of ANKRD6, ITIH3 and NPY1R significantly correlated with reduced OS, whilst high expression of ANKRD6, ITIH3, SORCS3 and NPY1R was associated with lower DFS (Fig. 3D). Moreover, the multivariate Cox regression analysis showed that ANKRD6, ITIH3 and NPY1R constituted independent prognostic factors for OS (Fig. S5) and DFS (Fig. S6). In relation to expression, we observed a progressive and significant increase of ANKRD6 and ITIH3 across the tumor stages (Fig. 3E). These results highlight the usefulness of the pipeline, validate the results obtained in TCGA and ACRG, and denote the clinical impact of the identified genes, with special emphasis for ANKRD6 and ITIH3 in GC malignancy, recurrence and metastasis.

Association of ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 expression with metastasis, recurrence and survival on a total of 1908 GC patients from 9 publicly available GC data sets. A Expression of the 5 genes in primary tumor tissue of GC patients presenting distant metastasis (M) or not (M0) (NM0 = 513, NM1 = 45). B Expression of the 5 genes individually in primary tumor tissue of patients who recurred (Yes) or not (No) after the primary therapy (NNo = 573, NYes = 423). C Kaplan-Meier plots of OS according to the expression of the 5 genes in patients treated with adjuvant chemotherapy (N = 1036). The best cut-off method was used for expression level stratification. D Kaplan-Meier plots of OS (top) and DFS (bottom) according to the expression of the 5 genes. The best cut-off method was used for expression level stratification. E Expression of the 5 genes in the different tumor stages (NI = 217, NII = 495, NIII = 879, NIV = 316)
3.4 ANKRD6 and ITIH3 in GC progression, metastasis and EMT
Given the higher clinical impact of ANKRD6 and ITIH3, we explored the score of their combined expression and compared its potential with respect to the 5 genes individually and the 5-gene signature. First, we detected that a high score of this 2-gene signature in ACRG and TCGA cohorts predicted worse prognosis (Figs. 4A and S7A), and was an age- and stage- independent prognostic factor (Figs. 4B and S7B), in the former cohort with HRs higher than those obtained with the genes individually. The 2-gene score was significantly higher in tumor versus paired normal gastric tissue in patients presenting poor outcome (Fig. 4C), and was also higher in advanced disease stages (Figs. 4D and S7C) and in patients with recurrence (Figs. 4E and S7D). Moreover, the score was higher in the MSS/EMT and GS molecular subtypes (Figs. 4F and S7E), in samples from patients presenting node invasion (Figs. 4G and S7F), and in metastatic cases in TCGA and ACRG (Figs. 4H and S7G). In the metastatic patients, the score of the 5-gene signature was not significantly higher neither in the TCGA cohort nor in the ACRG cohort (Fig. S8A), reinforcing the relevance of ANKRD6 and ITIH3 in metastasis. Moreover, using the Cancer Cell Line Encyclopedia (CCLE), we determined that among our identified genes, in GC cells, ANKRD6 showed the highest levels on average, with the metastatic cell lines displaying higher expression than those cells derived from primary cases (Fig. S8B, S8C).

Association of the GSVA score of ANKRD6 and ITIH3 with prognosis and clinic-pathological characteristics, and correlation of the 5 genes with hallmark gene sets in the ACRG cohort. A Kaplan-Meier plots of OS and DFS according to the ANKRD6 and ITIH3 GSVA score in the ACRG cohort using the best cut-off method for GSVA score stratification. B Forest plots showing multivariate Cox regression analysis for the ANKRD6 and ITIH3 GSVA score in association with OS (left) and DFS (right), adjusting for age and TNM stage, in the and ACRG cohort. C ANKRD6 and ITIH3 GSVA score in normal gastric tissue versus the corresponding paired GC tissue in ACRG patients stratified into high and low score subgroups according to the cut-off defined in (A). ANKRD6 and ITIH3 GSVA score according to tumor stage (D), recurrence (E), molecular subtype (F), N stage (G), and M stage (H). I Correlation of ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 with the GSVA scores of the 50 hallmark gene sets defining biological states or processes from The Molecular Signatures Database (MSigDB) in the ACRG cohort. Genes and hallmarks are grouped by hierarchical clustering. Blue colour represents negative correlations and red colour positive correlations. Spearman’s rho correlation coefficient is indicated in significant correlations. Correlation of ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178 with epithelial and mesenchymal markers, and EMT inductors (J), and with CSC markers (K) in the ACRG cohort. In (J), markers are clustered within each marker category, and in (K), genes in columns and rows are grouped by hierarchical clustering. Blue colour represents negative correlations and red colour positive correlations. Spearman’s rho correlation coefficient is indicated in significant correlations (Colour figure online)
Then, with the aim of exploring the biological significance of the identified genes in GC, we studied their relationship with described pathways. For this, we took advantage of the GSVA signature score of the hallmark gene sets included in MsigDb (https://www.gsea-msigdb.org/gsea/msigdb/). The Spearman correlation analysis showed that the 5 genes presented positive correlation with the hallmarks of Epithelial mesenchymal transition (EMT), KRAS, Hedgehog signaling, or myogenesis in both TCGA and ACRG cohorts (Figs. 4I and S7H). In contrast, there was negative correlation with G2M checkpoint or DNA repair hallmarks (Figs. 4I and S7H). These analyses also showed differences in the pattern of correlations of the genes, differentiating ANKRD6 and ITIH3 in one side, from SORCS3, NPY1R and CCDC178. Thus, TGF beta, STAT3 and TNFA signaling and apoptosis were pathways specifically correlated with ANKRD6 and ITIH3 (Figs. 4I and S7H). Moreover, ANKRD6 and ITIH3 were the genes most positively correlated with the hallmark of EMT in both cohorts, with Spearman coefficients of 0.46 and 0.35 for ANKRD6 in ACRG and TCGA; and coefficients of 0.44 and 0.49 for ITIH3 in the corresponding cohorts (p-value < 0.001 in all cases) (Figs. 4I and S7H).
To further characterize the connection of these genes with the process of EMT, we explored the correlations established between them and canonical epithelial and mesenchymal markers, whose expression decrease and increase in cells undergoing EMT respectively, as well as with EMT inducers. This study revealed negative correlations with epithelial genes, such as the epithelial cell adhesion protein E-Cadherin (CDH1), the cytoskeletal genes coding the keratins 8, 18 and 19 (KRT8, KRT18 and KRT19) and desmoglein 3 (DSG3) in both ACRG and TCGA cohorts (Figs. 4J and S7I). On the contrary, positive correlations with mesenchymal markers such as N-Cadherin (CDH2), the cytoskeletal protein Vimentin (VIM), the matrix metallopeptidase 2 (MMP2), proteins belonging to the extracellular matrix (ECM) such as Fibronectin 1 (FN1) and Matrilin-3 (MATN3), or related to its composition such as the serpin family H member 1 (SERPINH1), were detected (Figs. 4J and S7I). Finally, positive correlations were found between the 5 genes with the expression of different EMT inducers including ZEB1/2, SNAI1/2, TWIST1/2, PRRX1 and STAT3 (Figs. 4J and S7I). Notably, the strongest correlations and with the highest number of markers of each group were detected for ANKRD6 and ITIH3.
Since metastasis and EMT, as well as recurrence and therapy resistance, are attributed to cancer stem cells (CSCs) [31, 32], we studied the correlation of the 5 genes with regulators of CSCs. This analysis revealed that several stem cell markers were positively and significantly correlated with the 5 genes in both cohorts (Figs. 4K and S7J). As in the case of biological pathways and EMT markers/inducers, ANKRD6 and ITIH3 were the genes, specially the first one, presenting the strongest patterns of correlation and with a higher number of stem markers, exhibiting ANKRD6 significant correlations with SOX2, BMI1, KLF8, LINGO2, CXCR4, CD90 and YAP1 (Figs. 4K and S7J). These results associate high levels of ANKRD6 and ITIH3 with the EMT process.
3.5 ANKRD6 is required for gastric cancer cell activity
ANKRD6 was the most robustly associated with poor outcome, recurrence and metastasis among the 5 genes. Moreover, its impact on GC cell activity remained unexplored. Therefore, we selected this gene in order to address its functional role in GC cells. For this, we silenced the expression of ANKRD6 using 2 independent short hairpin RNAs in the metastatic GC cell line MKN45, which expresses high levels of ANKRD6, as observed in CCLE (Fig. S8B). Once we validated the significant inhibition of ANKRD6 using both short hairpins (Fig. 5A), we analyzed the phenotype of the ANKRD6-silenced cells, detecting multiple cells de-attached in sh1 and sh2 conditions, indicative that they could undergo apoptosis. To confirm this idea, immunofluorescence of the apoptosis markers active Caspase-3 and proteolyzed PARP-1 were performed. Noteworthy, we detected an increase of around 5–10 fold in ANKRD6-silenced cells compared to control cells. In particular, the proportion of cells positive for active Caspase-3 was 3.37% ± 0.31 and 4.61% ± 0.54 in sh1 and sh2 cells compared to 0.56% ± 0.14 in controls (Fig. 5B). Similarly, proteolyzed PARP-1-positive cells were 2.64% ± 0.55 and 4.00% ± 0.32 in ANKRD6-silenced compared to 1.03% ± 0.27 in controls (Fig. 5C). Additionally, flow cytometry analysis unveiled a significant increase in the proportion of cells in the subG1 phase in ANKRD6-silenced cells (sh1; 11.87% ± 0.25; sh2: 13.39% ± 0.99) respect to control cells (0.77% ± 0.45) (Fig. 5D). Moreover, we observed an increase in the percentage of cells in the G2M phase, whilst the proportion of cells decreased in G1 and S phases (Fig. 5D), suggesting cell cycle arrest. To test the effect on cell proliferation, we performed cell count experiments, which revealed a significant and progressive reduction in the number of cells over time in both sh conditions compared to control cells (Fig. 5E). Concretely, at day 5, the number of sh1 and sh2 cells was reduced by ~60% (Fig. 5E).

Role of ANKRD6 in gastric cancer cell activity. A ANKRD6 mRNA expression in MKN45 GC cell line lentivirally transduced with pLKO (control) or ANKRD6 silencing (sh1 and sh2) plasmids (n ≥ 3). Quantification and representative images of active Caspase-3-positive cells (B) and proteolyzed PARP-1-positive cells (C) in pLKO and shANKRD6 MKN45 cells analyzed by immunofluorescence (n = 3). D Cell cycle distribution in pLKO and shANKRD6 MKN45 cells assessed through the study of cell DNA content by flow cytometry (n = 3). E Growth curves representing the number of pLKO and shANKRD6 MKN45 cells counted at days 1, 3 and 5 after seeding (n ≥ 3). F Volume at the indicated time points and image of subcutaneous tumors generated by pLKO (control) and shANKRD6 MKN45 cells in immunodeficient FOXn1nu (nu/nu) mice. G Mass of subcutaneous tumors represented in (F). Representative images and quantification of cells presenting active Caspase-3 (H) and Ki67 positive staining (I) assessed by IHC in subcutaneous tumors from (F). Scale bar: 100 µm
Then, we moved to the in vivo setting and established subcutaneous xenografts of control and ANKRD6-silenced cells in immunodeficient mice. ANKRD6-silenced cells displayed a significant reduction in tumor growth with respect to control cells (Fig. 5F). The decrease in tumor volume was 67.2% in sh1 tumors and 66.8% in sh2 at day 18. Consistent with this, the tumor weight was significantly lower in those derived from ANKRD6-silenced cells (Fig. 5G). Furthermore, we explored Caspase-3 and the proliferation marker Ki67 in these tumors by IHC, finding a 2–3 fold increase in the number of active Caspase-3 positive cells (Fig. 5H), and a decrease in the proportion of Ki67-positive cells (Fig. 5I) in sh conditions, which confirmed in vivo the requirement of ANKRD6 for tumor cell survival and proliferation. Overall, these results demonstrate that ANKRD6 is required for GC metastatic cell activity and malignancy.
3.6 ANKRD6 is required for GC metastatic traits
Then, to unravel the molecular mechanisms associated to the activity of ANKRD6, we performed RNA sequencing in control and ANKRD6-silenced cells. 450 genes were differentially expressed with respect to control cells, with a fold-change cut-off of >1.5 and p-adjusted values <0.05. Among them, 198 genes were up-regulated and 252 down-regulated. The gene set enrichment analysis (GSEA) identified statistically significant downregulation of 11 pathways in ANKRD6-silenced cells (Fig. 6A). Among them, the hallmark of EMT was identified, as well as other hallmarks such as G2M checkpoint or KRAS signaling up, which is in agreement with the results obtained above. Consequently, we studied functional and molecular events linked to EMT and metastasis in ANKRD6-silenced cells. First, we detected an increased expression of the epithelial markers E-Cadherin and Keratin-18 (KRT18) in ANKRD6-silenced cells using IHC, western blot and immunofluorescence techniques in vivo and in vitro (Fig. 6B–D). In line with these findings at cellular level, the expression of ANKRD6 inversely correlated with both epithelial markers in the GC samples from the ACRG and TCGA patients (Figs. 4J and S7I). Moreover, the capacity of GC cells for migration and invasion was significantly impaired by ANKRD6 silencing (Fig. 6E, F). Thus, the migration capacity of ANKRD6-silenced cells compared to controls represented the 60.8 ± 11.2% and the 43.7 ± 4.3% for sh1 and sh2 cells, respectively (Fig. 6E). Similarly, the invasive potential of sh cells was reduced in around 30% (Fig. 6F).

Pro-metastatic role of ANKRD6 in gastric cancer. A GSEA ridge plots depicting the enrichment of signal pathways altered in shANKRD6 cells respect to pLKO cells. B Representative image and quantification of E-Cadherin determined by IHC in subcutaneous tumors derived from pLKO and shANKRD6 MKN45 cells. Scale bar: 100 µm. Representative western blot (C) and immunofluorescence (D) of E-Cadherin and KRT18 in pLKO and sh2 ANKRD6 MKN45 cells. Scale bar: 100 µm. Representative images and relative migration (E) and invasion (F) of ANKRD6-silenced cells respect to control cells determined by transwell assays (n ≥ 3). G Genes belonging to the Epithelial mesenchymal transition (EMT) hallmark gene set that are differentially expressed in shANKRD6 cells respect to pLKO cells. Genes down-regulated are represented in purple and up-regulated in green. H Correlation in TCGA and ACRG cohorts between the expression of ANKRD6 and the DEGs from the EMT hallmark. I Expression of MATN3, GPC1, TIMP1 and DKK1 in normal gastric tissue (grey) versus the corresponding paired GC tissue (red) in TCGA (Ntumor = 32, Nnormal = 375) and ACRG (Ntumor = 98, Nnormal = 98). J Kaplan-Meier plots of OS (left) and DFS (right) according to the expression of MATN3, TIMP1 and DKK1 in TCGA, ACRG and the integrated cohort. K Expression of MATN3, TIMP1 and DKK1 according to M stage in the integrated cohort (NM0 = 513, NM1 = 45). L mRNA expression of MATN3, GPC1, TIMP1 and DKK1 determined by qPCR in shANKRD6 respect to pLKO cells (n ≥ 3) (Colour figure online)
We observed that within the hallmark of EMT, 8 genes were significantly down-regulated and 4 were up-regulated in ANKRD6-silenced cells (Fig. 6G). The down-regulated genes were PMEPA1, a native regulator of TGF-beta; DKK1, an antagonist of the canonical Wnt signaling pathway; CAPG, which is involved in actin dynamics; and genes coding components of the ECM (MATN3 and LAMC2) or ECM-interacting proteins (ITGA2, GPC1 and TIMP1) (Fig. 6G). We moved back to the patients and found that MATN3, GPC1, TIMP1 and DKK1 were positively and significantly correlated with the expression of ANKRD6 in the GC patients from both the TCGA and the ACRG cohorts (Fig. 6H). Additionally, their expression was higher in GC tissue respect to normal gastric tissue in both cohorts (Fig. 6I), whereas high expression of MATN3, TIMP1 and DKK1 was significantly associated with reduced OS and DFS in GC patients from the TCGA, ACRG and the additional cohorts used in this study (Fig. 6J), their expression being also significantly elevated in the samples of those patients presenting metastasis (Fig. 6K). Finally, we detected that the expression of the four genes was significantly downregulated in shANKRD6 cells validating the in silico results (Fig. 6L). These findings, overall, reveal a role of ANKRD6 in GC progression, metastasis and EMT.
4 Discussion
Our work identified the top-genes most significantly associated with reduced, both OS and DFS of GC patients from the TCGA. These genes are ANKRD6, ITIH3, SORCS3, NPY1R and CCDC178, which form a signature associated to adverse clinic-pathological features such as advanced tumor stage, poor prognosis and disease recurrence in GC. Among them, ANKRD6 and ITIH3 are the most significant genes within the signature. ANKRD6, also called Diversin, belongs to the ankyrin repeat domain protein family and is the homolog of the Diego protein of Drosophila [33], whilst ITIH3 encodes a protein that binds hyaluronic acid and stabilizes the ECM [34]. Very little is known regarding their expression and activity in GC and those findings complement our results. Thus, a recent work proposed a cuproptosis-related prognostic 3-gene signature including ANKRD6 [35], whereas in relation to ITIH3, higher levels were detected in the plasma of GC patients respect to healthy individuals [36, 37], and it was part of a 8-gene signature associated with poor outcome [58]. Additionally, a few works connected their expression with outcome in additional types of cancer. In this sense, ANKRD6 is overexpressed in breast cancer, wherein its high level is associated with advanced TNM stages and nodal invasion [38]. In gliomas, the positive expression of ANKRD6 is associated with advanced tumor grade [39], whereas in non-small cell lung cancer (NSCLC) and colorectal cancer (CRC) is correlated with poor prognosis, advanced stages and poor differentiation [40,41,42]. Referring to ITIH3, higher levels of ITIH3 in the plasma were reported in lung [43], pancreatic [44], and breast cancer [45], whereas opposite findings have been detected in colorectal cancer [46, 47]. In tumor biopsies, ITIH3 mRNA is reduced in tumor versus normal tissue in breast, uterus, colon, ovary, lung, rectum, and prostate cancer [48, 49], and low protein levels were significantly associated with poor prognosis and platinum resistance in ovarian cancer [49]. These results suggest that the effect of ITIH3 in cancer is context-dependent, acting as a tumor suppressor in some cancer types, whilst it may exhibit an oncogenic role in others including GC. Indeed, our work has shown that high ITIH3 expression is associated with reduced survival also in adrenocortical carcinoma, colon adenocarcinoma, kidney renal clear cell carcinoma, kidney renal papillary cell carcinoma and mesothelioma. Moreover, our results confirm that ANKRD6 is commonly overexpressed in cancer where it is associated to poor outcome and malignancy.
Regarding the other 3 genes of the signature little is known about their expression and role in cancer. NPY1R encodes a G protein-coupled receptor that mediates the function of the neurotransmitter neuropeptide Y (NPY), and the peptide YY (PYY), which is a gastrointestinal hormone that controls appetite [50]. CCDC178 encodes a protein located in the ciliary basal body, whilst SORCS3 encodes a receptor transmembrane protein of the vacuolar protein sorting 10 family, which acts as a postsynaptic modulator of synaptic depression [51]. Specifically in GC, NPY1R is more highly expressed in the subgroup of gastric tumors presenting MUC16 mutations, and, in agreement with our results, the high expression of NPY1R was associated with dismal prognosis in the GC patients from the TCGA and ACRG cohorts [52]. In the case of SORCS3, it has been detected its methylation [53] and this epigenetic modification has been associated with the progression of gastric precancerous lesions [54]. In the case of CCDC178, an study that performed whole genome sequencing in samples from a GC patient, identified in the primary GC tumor a somatic nonsynonymous single nucleotide variation affecting CCDC178 [55], and another study identified in GC mutations (mainly missense mutations and frame shift deletions) in CCDC178 that were significantly associated with poor survival [56].
We report the potential of the 2-gene signature composed by ANKRD6 and ITIH3, which predicts survival regardless of the tumor stage and the patients’ age, exhibiting HRs higher than those of the 5 genes individually, and whose score is higher in patients presenting recurrent disease. Additionally, we have also identified that both are involved in metastasis and EMT process. These results have been obtained taking advantage of public databases and bioinformatics from TCGA and ACRG cohorts, but also generating a new analysis pipeline allowing the study of almost 2000 CG patients derived from 9 independent cohorts. This pipeline represents a useful tool to analyze recurrence, therapy resistance and metastasis. Since no previous studies have explored the role of the identified genes in GC, we went deeper into the analysis of the relevance of the novel signature and characterized the role of ANKRD6 in GC through functional studies in vitro and in vivo, and transcriptomic analysis to unravel downstream targets. These experiments complemented the results obtained in the bioinformatic analyses and unraveled that ANKRD6 confers pro-metastatic and tumorigenic properties to GC cells, preventing apoptosis, promoting GC cell migration and invasion, fostering tumor growth, and regulating EMT related pathways but also hallmarks such as G2M checkpoint or KRAS signaling. In this sense, ANKRD6 has been previously linked to WNT signaling, a critical pathway in GC, where it promotes the non-canonical Wnt/Planar cell polarity pathway [57].
Overall, our work identifies a novel signature of 5 genes associated with adverse outcomes in GC, driven specially by 2 of them, ANKRD6 and ITIH3, and reveals for the first time the role of ANKRD6 in metastasis and EMT process, pointing out their potential as a prognostic signature and molecular target in cancer.
Data availability
RNAseq data are deposited in NCBI’s Gene Expression Omnibus (GSE238103).
Bibliography
H. Sung, J. Ferlay, R.L. Siegel, M. Laversanne, I. Soerjomataram, A. Jemal, et al., Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 71, 209–249 (2021)
J. Ferlay, M. Colombet, I. Soerjomataram, D.M. Parkin, M. Pineros, A. Znaor, et al., Cancer statistics for the year 2020: an overview. Int. J. Cancer (2021)
D.H. Ilson, Advances in the treatment of gastric cancer: 2019. Curr. Opin. Gastroenterol. 35, 551–554 (2019)
Y. Li, H. Zhao, Postoperative recurrence of gastric cancer depends on whether the chemotherapy cycle was more than 9 cycles: based on a retrospective and observational study of follow-up within 3 years of 843 patients. Medicine (Baltimore) 101, e28620 (2022)
C. de Jongh, L. Triemstra, A. van der Veen, L.A.A. Brosens, M.D.P. Luyer, J. Stoot, et al., Pattern of lymph node metastases in gastric cancer: a side-study of the multicenter LOGICA-trial. Gastric Cancer 25, 1060–1072 (2022)
S. Kinami, N. Nakamura, Y. Tomita, T. Miyata, H. Fujita, N. Ueda, et al., Precision surgical approach with lymph-node dissection in early gastric cancer. World J. Gastroenterol. 25, 1640–1652 (2019)
G. Marte, A. Tufo, F. Steccanella, E. Marra, P. Federico, A. Petrillo, et al., Efficacy of Surgery for the Treatment of Gastric Cancer Liver Metastases: a Systematic Review of the Literature and Meta-Analysis of Prognostic Factors. J. Clin. Med. 10(5), 1141 (2021)
J. Ferlay, M. Colombet, I. Soerjomataram, C. Mathers, D.M. Parkin, M. Pineros, et al., Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 144, 1941–1953 (2019)
P. Lauren, The Two Histological Main Types of Gastric Carcinoma: diffuse and So-Called Intestinal-Type Carcinoma. An Attempt at a Histo-Clinical Classification. Acta Pathol. Microbiol. Scand. 64, 31–49 (1965)
Cancer Genome Atlas Research N, Comprehensive molecular characterization of gastric adenocarcinoma. Nature 513, 202–209 (2014)
R. Cristescu, J. Lee, M. Nebozhyn, K.M. Kim, J.C. Ting, S.S. Wong, et al., Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 21, 449–456 (2015)
F. Seyfried, B.H. von Rahden, A.D. Miras, M. Gasser, U. Maeder, V. Kunzmann, et al., Incidence, time course and independent risk factors for metachronous peritoneal carcinomatosis of gastric origin–a longitudinal experience from a prospectively collected database of 1108 patients. BMC Cancer 15, 73 (2015)
T. Arigami, D. Matsushita, M. Shimonosono, Y. Tsuruda, K. Sasaki, K. Baba, et al., Clinical Significance of Recurrence Risk Score for Conversion Surgery in Patients With Advanced Gastric Cancer. Anticancer Res. 43, 3305–3310 (2023)
K. Fujikawa, T. Omori, N. Shinno, H. Hara, M. Yamamoto, M. Yasui, et al., Tumor Deposit Is an Independent Factor Predicting Early Recurrence and Poor Prognosis in Gastric Cancer. J. Gastrointest. Surg. 27(7), 1336–1344 (2023)
S.C. Oh, B.H. Sohn, J.H. Cheong, S.B. Kim, J.E. Lee, K.C. Park, et al., Clinical and genomic landscape of gastric cancer with a mesenchymal phenotype. Nat. Commun. 9, 1777 (2018)
C.H. Ooi, T. Ivanova, J. Wu, M. Lee, I.B. Tan, J. Tao, et al., Oncogenic pathway combinations predict clinical prognosis in gastric cancer. PLoS Genet. 5, e1000676 (2009)
J. Lee, I. Sohn, I.G. Do, K.M. Kim, S.H. Park, J.O. Park, et al., Nanostring-based multigene assay to predict recurrence for gastric cancer patients after surgery. PLoS One 9, e90133 (2014)
J.H. Cheong, S.C. Wang, S. Park, M.R. Porembka, A.L. Christie, H. Kim, et al., Development and validation of a prognostic and predictive 32-gene signature for gastric cancer. Nat. Commun. 13, 774 (2022)
J.Y. Cho, J.Y. Lim, J.H. Cheong, Y.Y. Park, S.L. Yoon, S.M. Kim, et al., Gene expression signature-based prognostic risk score in gastric cancer. Clin. Cancer Res. 17, 1850–1857 (2011)
M. Mounir, M. Lucchetta, T.C. Silva, C. Olsen, G. Bontempi, X. Chen, et al., New functionalities in the TCGAbiolinks package for the study and integration of cancer data from GDC and GTEx. PLoS Comput. Biol. 15, e1006701 (2019)
M.J. Goldman, B. Craft, M. Hastie, K. Repecka, F. McDade, A. Kamath, et al., Visualizing and interpreting cancer genomics data via the Xena platform. Nat. Biotechnol. 38, 675–678 (2020)
B.S. Carvalho, R.A. Irizarry, A framework for oligonucleotide microarray preprocessing. Bioinformatics 26, 2363–2367 (2010)
S. Durinck, P.T. Spellman, E. Birney, W. Huber, Mapping identifiers for the integration of genomic datasets with the R/Bioconductor package biomaRt. Nat. Protoc. 4, 1184–1191 (2009)
M. Ghandi, F.W. Huang, J. Jane-Valbuena, G.V. Kryukov, C.C. Lo, E.R. McDonald 3rd, et al., Next-generation characterization of the Cancer Cell Line Encyclopedia. Nature 569, 503–508 (2019)
P.J. Cock, C.J. Fields, N. Goto, M.L. Heuer, P.M. Rice, The Sanger FASTQ file format for sequences with quality scores, and the Solexa/Illumina FASTQ variants. Nucleic Acids Res. 38, 1767–1771 (2010)
S. Hanzelmann, R. Castelo, J. Guinney, GSVA: gene set variation analysis for microarray and RNA-seq data. BMC Bioinf. 14, 7 (2013)
A. Liberzon, C. Birger, H. Thorvaldsdottir, M. Ghandi, J.P. Mesirov, P. Tamayo, The Molecular Signatures Database (MSigDB) hallmark gene set collection. Cell Syst. 1, 417–425 (2015)
M.I. Love, W. Huber, S. Anders, Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 15, 550 (2014)
T. Wu, E. Hu, S. Xu, M. Chen, P. Guo, Z. Dai, et al., clusterProfiler 4.0: a universal enrichment tool for interpreting omics data. Innovation (Camb.) 2, 100141 (2021)
Z. Tang, C. Li, B. Kang, G. Gao, C. Li, Z. Zhang, GEPIA: a web server for cancer and normal gene expression profiling and interactive analyses. Nucleic Acids Res. 45, W98–W102 (2017)
T. Nairuz, Z. Mahmud, R.K. Manik, Y. Kabir, Cancer stem cells: an insight into the development of metastatic tumors and therapy resistance. Stem. Cell Rev. Rep. 19(6), 1577–1595 (2023)
M. Otaegi-Ugartemendia, A. Matheu, E. Carrasco-Garcia, Impact of Cancer Stem Cells on Therapy Resistance in Gastric Cancer. Cancers (Basel) 14(6), 1457 (2022)
F. Feiguin, M. Hannus, M. Mlodzik, S. Eaton, The ankyrin repeat protein Diego mediates Frizzled-dependent planar polarization. Dev. Cell 1, 93–101 (2001)
M.S. Lord, J. Melrose, A.J. Day, J.M. Whitelock, The Inter-alpha-Trypsin Inhibitor Family: versatile Molecules in Biology and Pathology. J. Histochem. Cytochem. 68, 907–927 (2020)
X.X. Wang, S.Z. Deng, L.H. Wu, Q.Q. Liu, G. Zheng, K. Du, et al., Cuproptosis-Mediated Patterns Characterized by Distinct Tumor Microenvironment and Predicted the Immunotherapy Response for Gastric Cancer. ACS Omega 8, 10851–10862 (2023)
P.K. Chong, H. Lee, J. Zhou, S.C. Liu, M.C. Loh, T.T. Wang, et al., ITIH3 is a potential biomarker for early detection of gastric cancer. J. Proteome Res. 9, 3671–3679 (2010)
Y.H. Uen, K.Y. Lin, D.P. Sun, C.C. Liao, M.S. Hsieh, Y.K. Huang, et al., Comparative proteomics, network analysis and post-translational modification identification reveal differential profiles of plasma Con A-bound glycoprotein biomarkers in gastric cancer. J. Proteomics 83, 197–213 (2013)
X. Yu, M. Wang, Q. Dong, F. Jin, Diversin is overexpressed in breast cancer and accelerates cell proliferation and invasion. PLoS One 9, e98591 (2014)
M. Wang, X. Yu, Q. Dong, Y. Wang, Diversin is overexpressed in human gliomas and its depletion inhibits proliferation and invasion. Tumour Biol. 35, 7905–7909 (2014)
L. Luan, N. Li, K. Zhang, X. Wang, H. Pan, Diversin upregulates the proliferative ability of colorectal cancer by inducing cell cycle proteins. Exp. Mol. Pathol. 129, 104850 (2023)
R. Bai, D. Wu, Z. Shi, W. Hu, J. Li, Y. Chen, et al., Pan-cancer analyses demonstrate that ANKRD6 is associated with a poor prognosis and correlates with M2 macrophage infiltration in colon cancer. Chin. J. Cancer Res. 33, 93–102 (2021)
L. Luan, Y. Zhao, Z. Xu, G. Jiang, X. Zhang, C. Fan, et al., Diversin increases the proliferation and invasion ability of non-small-cell lung cancer cells via JNK pathway. Cancer Lett. 344, 232–238 (2014)
S.H. Heo, S.J. Lee, H.M. Ryoo, J.Y. Park, J.Y. Cho, Identification of putative serum glycoprotein biomarkers for human lung adenocarcinoma by multilectin affinity chromatography and LC-MS/MS. Proteomics 7, 4292–4302 (2007)
X. Liu, W. Zheng, W. Wang, H. Shen, L. Liu, W. Lou, et al., A new panel of pancreatic cancer biomarkers discovered using a mass spectrometry-based pipeline. Br. J. Cancer 117, 1846–1854 (2017)
J. Dufresne, P. Bowden, T. Thavarajah, A. Florentinus-Mefailoski, Z.Z. Chen, M. Tucholska, et al., The plasma peptides of breast versus ovarian cancer. Clin. Proteomics 16, 43 (2019)
X. Jiang, X.Y. Bai, B. Li, Y. Li, K. Xia, M. Wang, et al., Plasma Inter-Alpha-Trypsin Inhibitor Heavy Chains H3 and H4 Serve as Novel Diagnostic Biomarkers in Human Colorectal Cancer. Dis. Markers 2019, 5069614 (2019)
A.T. Kopylov, A.A. Stepanov, K.A. Malsagova, D. Soni, N.E. Kushlinsky, D.V. Enikeev, et al., Revelation of Proteomic Indicators for Colorectal Cancer in Initial Stages of Development. Molecules 25(3), 619 (2020)
A. Hamm, J. Veeck, N. Bektas, P.J. Wild, A. Hartmann, U. Heindrichs, et al., Frequent expression loss of Inter-alpha-trypsin inhibitor heavy chain (ITIH) genes in multiple human solid tumors: a systematic expression analysis. BMC Cancer 8, 25 (2008)
Y. Liu, L. Shi, C. Yuan, Y. Feng, M. Li, H. Liu, et al., Downregulation of ITIH3 contributes to cisplatin-based chemotherapy resistance in ovarian carcinoma via the Bcl-2 mediated anti-apoptosis signaling pathway. Oncol. Lett. 25, 61 (2023)
R.L. Batterham, M.A. Cowley, C.J. Small, H. Herzog, M.A. Cohen, C.L. Dakin, et al., Gut hormone PYY(3-36) physiologically inhibits food intake. Nature 418, 650–654 (2002)
T. Breiderhoff, G.B. Christiansen, L.T. Pallesen, C. Vaegter, A. Nykjaer, M.M. Holm, et al., Sortilin-related receptor SORCS3 is a postsynaptic modulator of synaptic depression and fear extinction. PLoS One 8, e75006 (2013)
Y.J. Huang, Z.F. Cao, J. Wang, J. Yang, Y.J. Wei, Y.C. Tang, et al., Why MUC16 mutations lead to a better prognosis: a study based on The Cancer Genome Atlas gastric cancer cohort. World J. Clin. Cases 9, 4143–4158 (2021)
K. Matsusaka, A. Kaneda, G. Nagae, T. Ushiku, Y. Kikuchi, R. Hino, et al., Classification of Epstein-Barr virus-positive gastric cancers by definition of DNA methylation epigenotypes. Cancer Res. 71, 7187–7197 (2011)
B.G. Schneider, R. Mera, M.B. Piazuelo, J.C. Bravo, J. Zabaleta, A.G. Delgado, et al., DNA Methylation Predicts Progression of Human Gastric Lesions. Cancer Epidemiol. Biomarkers Prev. 24, 1607–1613 (2015)
J. Zhang, J.Y. Huang, Y.N. Chen, F. Yuan, H. Zhang, F.H. Yan, et al., Whole genome and transcriptome sequencing of matched primary and peritoneal metastatic gastric carcinoma. Sci. Rep. 5, 13750 (2015)
B. Zhang, Y. Li, L. Yang, Y. Chen, A Four-Gene-Based Risk Score With High Prognostic Value in Gastric Cancer. Front. Oncol. 11, 584213 (2021)
T. Schwarz-Romond, C. Asbrand, J. Bakkers, M. Kuhl, H.J. Schaeffer, J. Huelsken, et al., The ankyrin repeat protein Diversin recruits Casein kinase Iepsilon to the beta-catenin degradation complex and acts in both canonical Wnt and Wnt/JNK signaling. Genes Dev. 16, 2073–2084 (2002)
F. Shang, Y. Wang, Z. Shi, Z. Deng, J. Ma, Development of a signature based on eight metastatic-related genes for prognosis of GC patients abstract. Mol. Biotechnol. 65(11), 1796–1808 (2023). https://doi.org/10.1007/s12033-023-00671-9
Acknowledgements
M.O-U and A.A-Z were recipient of predoctoral fellowships from the FPU call from MINECO (FPU18/04540) and Basque Government (PRE_2020_1_0130) respectively. E.C-G was a recipient of a Stop Fuga de Cerebros postdoctoral fellowship and holds a Miguel Servet contract (CP19/00085) from the Instituto de Salud Carlos III (ISCIII). This work was supported by grants from ISCIII and FEDER Funds (PI18/01612, PI19/01355, DTS20/00179, PI22/01905), Diputacion Foral Gipuzkoa (2020-CIEN-000061-01 and 2022-CIEN-000012-01), and Health Department of the Basque Country (2022333033).
Funding
EC-G received a Miguel Servet grant from Instituto de Salud Carlos III (ISCIII) (CP19/00085). The work was supported by grants from the ISCIII co-financed by the European Union (PI22/00168 and PI22/01905), the Gipuzkoa City Council (2022-CIEN-000012-01), and the Health Department of the Basque Country (2022333034 and 2022333033).
Author information
Authors and Affiliations
Contributions
JE completed the bioinformatic analysis, performed the experiments and analyzed the results with the help of A. A-Z and M.O-U; V.M-A helped with the in vivo experiments; M. M-V helped with the evaluation of IHCs; AM and EC-G directed the project, contributed to data analysis, obtained funds and wrote the manuscript.
Corresponding authors
Ethics declarations
Ethical approval
Not applicable.
Competing interests
The authors declare that no competing interest exists.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elizazu, J., Artetxe-Zurutuza, A., Otaegi-Ugartemendia, M. et al. Identification of a novel gene signature related to prognosis and metastasis in gastric cancer. Cell Oncol. (2024). https://doi.org/10.1007/s13402-024-00932-y
Accepted:
Published:
DOI: https://doi.org/10.1007/s13402-024-00932-y