
Abstract
Elucidation of physical-chemical characteristics of investigational medicinal products should be established with suitable methodology. Characterization of nanomedicines and nanocarriers in clinical trials may require the definition of additional specific properties depending on the nature of the nanostructures or nanomaterials composing the investigational medicinal product. The availability of regulatory requirements and guidelines is investigated focusing on critical quality attributes for nanomedicines and nanocarriers, mapping them in a clinical trial setting. Current regulatory challenges and issues are highlighted. The increasing complexity of nanostructures, the innovative connotation of applied nanotechnology, and the lack in capillarity or misalignment of relevant guidelines and terminology may lead to a potential not standardized approach in the characterization of nanomedicines and nanocarriers in clinical trials and delays in the approval process. Further efforts and a proactive approach from a regulatory standpoint would be desirable to surf the wave of innovation that impact nanomedicines and nanocarriers in clinical trials, in order to support clinical drug development capitalizing on technological advances and still ensuring a strong regulatory framework.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Requirements for a dossier to be submitted to the regulatory authorities (RAs) for a request of authorization of clinical trials (CTs) may differ from those required for the submission of a marketing authorization of a medicinal product. Information and data needed in the assessment of investigational medicinal products (IMPs) are mainly focused on the potential risks, inherent the specific nature of the product, and take into deep consideration, among others, the status of the drug development, the phase of the CT (phase I to IV) and its duration, the characteristics of the population in study (e.g., pediatric, vulnerable group of patients), the therapeutic area, and the specificity of the diseases, like in case of rare ones, or their pathology. The specifications set for the control of the drug substances used in the CTs, including the tests and their acceptance criteria foreseen for phase I or phase II CTs, may be reviewed and strengthened when the IMP is further tested in phase III CTs. Furthermore, additional parameters may need to be adjusted according to the clinical development stage. Detailed data on the IMPs manufacturing process may not be required unless critical new processes are implemented such as non-standard sterilization ones, which may not be reported in the Pharmacopoeia. However, when complex manufacturing processes are involved and the relationship between quality characteristics and in vivo performance is not perfectly demonstrated or even understood, such as with nanomedicines or nanocarriers, the manufacturing process and characterization of IMPs are critical information that is expected to be provided in the quality section of the investigational medicinal product dossier (IMPD) as part of the submission of an application for a request of a CT authorization [1].
On the other hand, in a marketing authorization, the expected use of the medicinal product in a wider number of patients implies that the state of the art of its quality must be ensured, illustrated in detail, including a consolidated and validated manufacturing process. Liposomal, micellar, and nanoparticulate preparations are considered specialized pharmaceutical dose forms deriving from non-standard processes and therefore requiring production scale validation data to be provided in the marketing authorization application dossier unless otherwise justified [2].
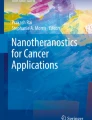
It is acknowledged that it may be challenging to set requirements able to cover into specific details every possible nature of a drug product. As an example, in the EU, general quality guidelines are available [3] and others also cover specific types of drug products such as IMPs [4], or multidisciplinary ones [5] including nanomedicines. During the benefit-risk assessment of CTs, dedicated guidelines for the evaluation of the quality of IMPs are taken into consideration; however, assessors at the RAs also refer to scientific guidelines on the quality of human medicinal products. This may be due to the lack of dedicated guideline intended to be applicable in a CT setting or due to the need of a more conservative approach because of the intrinsic characteristics of the IMP. It is not easy to identify CTs involving nanomedicines or nanocarriers in the public databases due to missing dedicated structured data fields in the clinical trial application (CTA) [6], able to code information on a nanomedicine, nanocarrier, or nanodevice and related characteristics. The sponsor of a CT is not prompted to declare if the IMP is a nanomedicine and to elucidate if the composition of the IMP includes nanocarriers, if due to the formulation of the IMP nanostructures or nanomaterials are involved, or if any nanotechnology is applied. Even now that the Clinical Trial Regulation (EU) No 536/2014 [7] is fully applicable in the EEA, the clinical trials information system [8] has no fields where the sponsor can state if the IMP is impacted by a nanotechnology. However, in the EMA pre-submission request form for a marketing authorization application [9], a checkbox is instead available to indicate if any nanotechnology applies. For CTs, the information can be only deduced by the description fields and by the text entered by sponsors in the databases, such as ClinicalTrials.gov [10], during the submission of a new application. This procedure has been used to retrieve the number of interventional CTs including the term “nano” and the trend in the number of submissions (Fig. 1) during the last 10 years.

Interventional clinical trials including the term “nano” with a study start date from 2010 to 2021. Searching criteria: other terms field, with interventional filter applied. Source: ClinicalTrials.gov (accessed 03 April 2022)
It is not possible to distinguish how many CTs involve a nanomedicine rather than a nanodevice, if a nanocarrier is concerned, or if a specific nanotechnology is used; moreover, other databases [11] are even less informative. However, the growing trend in human drug product submissions to FDA containing nanomaterials [12] is confirmed, as also evidenced by the number of nanomedicines on the market [13, 14]. The increasing impact of nanotechnology in the manufacturing processes of nanomedicines and nanodevices is bringing along an increase in efficacy and accuracy and at the same time additional regulatory discussions and concerns on safety to human health and the environment [15].
Characterization of nanomedicines, their future perspectives, and a better understanding of the correlation between their physico-chemical properties and their pharmacokinetics need to be and are being widely investigated [16,17,18,19]. However, there is limited information on the regulatory framework and quality assessment associated to the clinical development phase of a nanomedicine or nanocarrier. Missing full description or not standardized characterization of nanomedicines tested in CTs may jeopardize the safety profile or represent weak development data, and may not considered sufficient to support the marketing authorization stage. We therefore investigate the current availability of regulatory requirements and guidelines on nanomedicines and nanocarriers and focus on potential critical quality attributes (CQAs), mapping them in a CT setting, where additional regulatory guidance and alignment across RAs of different regions is strongly needed so that during drug development phase, the safety of subjects in CTs is ensured and an early consistent approach to proper description and characterization is envisaged by sponsors limiting inconsistencies between early batches and commercial ones.
The need of an improvement of the regulatory protocols is commonly recognized to be of fundamental importance to increase the industrial and clinical applications of nanomedicines. This is evidenced by a large number of papers addressing this issue in the recent years [20,21,22], including the Refine project [23], all attempting to support regulatory advances in the nanomedicine field.
Regulatory requirements
One of the most important regulatory steps in establishing the initial safety and efficacy profile of an IMP is the conduction of CTs. Such studies, carried out in humans, provide an opportunity to assess, for the first time, advances in pharmaceutical nanotechnology and the latest scientific innovations and advances in health care and prevention. During this crucial process, the quality of IMPs is assessed to confirm the physical-chemical characterization, the critical quality parameters, and function impacting the drug product performance and safety.
The characteristics of nanotechnology-based products are challenging for regulatory approval processes and there are still many open questions in the regulation of nanomedicines and nanomaterials, starting from their assessment in a CT setting. Examples are related to not standard pharmacokinetics, environmental and accumulation issues, genotoxicity, representativeness of in vitro nanotoxicology tests, increased permeation, stability and manufacturing scale-up, nanomorphology and characterization, non-standardized terminology, and regulations [24]. In addition, limited dedicated guidelines are available to support quality, safety, and efficacy assessment of nanomedicines or nanocarriers in the specific context of CTs.
A list of most relevant guidelines available to support medicinal product developers and CT sponsors in the preparation of the quality documentation presented in a request for authorization of CTs is reported in Fig. 2; the required information should be included in the chemistry manufacture and control (CMC) part of the IMPD for the evaluation of nanomedicines and nanocarriers. Looking at the incremental number of guidelines issued in the last 10 years, it is evident the attention and efforts that regulators dedicated to nanotechnology and its application to the pharmaceutical sector, even if it is also noted that RAs adopted different approaches and reacted with different timing. The trend in guidelines production reflects the impulse in sponsors’ submissions of CT applications containing nanotechnology-based products and highlights how the regulatory environment reacted to innovation when it has already reached the clinical trial stage.

Relevant guidelines on quality documentation and regulatory requirements for clinical trials, nanomedicines, and nanocarriers
European Union (EU)
Since 2012, the European Commission (EC) proposed in Europe a case-by-case approach to the assessment of nanomaterials [25]; however, in the document, there is no reference to CTs; a few opinions were also generated through the EC scientific committees on risk assessment of products of nanotechnologies and effects of nanosilver compounds [26, 27]. After the elaboration of a reflection paper on nanotechnology-based medicinal products for human use [28], EMA had a very productive period (2012–2016) in terms of reflection papers elaboration, on intravenous micellar systems [29], block copolymer micelle [30], intravenous liposomal products [31], coated nanomedicine products [32], and intravenous iron-based nano-colloidal products [33], followed by a break during the last 5 years. No general guideline on nanomedicines was ever developed, or a discussion launched on the need of a dedicated one in a CT context, which represents the front line where nanotechnology innovations applied to IMPs are facing for the first time a regulatory assessment process. The evaluation of innovation has been mandated to the innovation task force (ITF) in 2014 [34], and there are no signals that EMA intends to develop any further detailed guidelines or to review its own approach. Nevertheless, it is acknowledged that dedicated guidelines for CTs were developed and recently also updated, such as the guidelines on the requirements for the chemical and pharmaceutical or biological quality documentation concerning IMPs in CTs [35, 36]. The guideline for the chemical and pharmaceutical quality introduced in its scope, during one of the last updates, synthetic oligonucleotides, but the update did not incorporate any specific guidance on nanomedicines or nanocarriers, which are not cited. Even if huge efforts and progresses have been done, the regulatory framework for nanomedicines and nanocarriers in the EU remains fragmented and stratified [37] and would benefit from a harmonization process, including dedicated guidelines for early stages development and assessment in CTs.
USA
After the elaboration of a guidance to set the content and format of investigational new drug applications for phase I studies, the FDA elaborated in the first decade of the century also a guidance for industry to support with the use of current good manufacturing practice, for phase I investigational drugs [38, 39], and to support with the chemistry, manufacturing, and control information that would be submitted for phase II and phase III studies [40]. However, no reference to nanotechnology can be found in these documents. The increasing attention to nanotechnology products led to the publication in 2014 of an important guidance to discern whether an FDA-regulated product involves the application of nanotechnology [41] even if CTs were not specifically covered. There is no dedicated regulatory framework on nanomedicines, and the FDA assessment follows a product specific path, relying on consultation with sponsors to identify potential regulatory issues and on the assumption that the available requirements are sufficient to determine any potential toxicity profile. Consistent with other agencies, also, FDA privileges a case-by-case approach to the assessment of nanotechnology. However, it must be recognized that FDA reacted to the emerging application of nanotechnology with the publication of a fundamental guidance on drug products, including biological products that contain nanomaterials [42]. With this guidance, nanomaterial quality attributes and structural characterization of drug products containing nanomaterials were addressed, including in the scope eventually also CTs. A proportionate approach in the description and characterization of the IMP depending on the development stage is acknowledged, as far as it ensures safety during use in clinical trials. This represents a major step in the attempt to set a general framework for the identification of CQAs of the drug product, acknowledging also that the nanomaterial’s CQAs should be determined with regard to its function and potential impact on product performance. Recently, also, a guidance on liposome drug products was published [43].
Japan
There is no evidence that a definition or a specific framework was ever adopted for nanomedicines in Japan that are regulated under the general framework of the pharmaceutical affairs law and seems to be evaluated on a case-by-case basis approach. However, a nanomedicine initiative working group is in place for discussions on regulatory requirements for nanomedicine development. The Pharmaceuticals and Medical Devices Agency (PMDA) and the Ministry of Heath Labour and Welfare (MHLW) collaborated in the preparation of the joint MHLW/EMA reflection paper on the development of block copolymer micelle medicinal products [30]. PMDA also assisted MHLW in the preparation of two management guidance on CT notifications containing the points to consider in case of some nanotechnology-based medicines [44]. A reflection paper on nucleic acids (siRNA)-loaded nanotechnology-based drug products [45] and a guideline for the development of liposome drug products [46] were issued in 2016 by MHLW. There is not a dedicated regulatory framework for the assessment of nanomedicines and nanocarriers in CTs.
Canada
Issues with nanomedicines in Canada are acknowledged since 2010 [47]. Benefit-risk evaluation and approval of nanomedicines are currently performed within the existing legislative and regulatory frameworks, there is in fact no explicit reference to nanomaterial in acts and regulations, and there is no dedicated guideline for the submission of nanotechnology products in CTs. However, Health Canada implemented a working definition of nanomaterials [48]. This is allowing to request specific information to improve the understanding of nanomaterials and for the assessment of potential risks and benefits or risk management purposes, of regulated product or substances, including therefore those in CT applications that may be or that may contain a nanomaterial. The types of information required are the intended use, function and purpose of the nanomaterial, and information regarding any end product in which it will be used; manufacturing methods; toxicological, eco-toxicological, metabolism, and environmental fate data that may be both generic and specific to the nanomaterial if applicable; and risk assessment and risk management strategies, if considered or implemented. The characteristics and physico-chemical properties that can be required on nanomaterials by Health Canada are available online [49]; however, there is no structured or dedicated approach for CTs.
India
An innovative and extremely interesting approach is the one adopted in India with the recent publication of the guidelines for evaluation of nanopharmaceuticals [50]. A definition of nanopharmaceutical and nanomaterial is provided (material having particle size in the range of 1 to 100 nm in at least one dimension), extending the range up to 1000 nm if the material exhibits physical, chemical, or biological phenomenon or activity, which are attributable to its dimension. An attempt to categorize nanopharmaceuticals either according to the degradability and nature of the nanomaterial or the nanoform of the ingredient is also presented. The guideline is listing a set of data that should be submitted to the RA in the submission of an application for a CT. In particular, data for the physico-chemical characterization of nanopharmaceuticals are defined, specifying that some of them need to be identified as CQAs, and that they should be listed along with the product specifications. In the specifications, moreover, apart from criteria for unique identification, identity and quantification of impurities, and stability data, it is explicitly required to provide in vitro/in vivo release kinetics of the drug/active ingredient (as applicable) and in vitro/in vivo degradation kinetics of the nanopharmaceutical in various simulated media. The added value with this approach resides in having a comprehensive list of general regulatory requirements for the evaluation of nanopharmaceutics and nanocarriers, applicable to CTs. However, and in alignment with the other RAs, it is recognized that information required for nanopharmaceuticals should be decided on case-by-case basis approach.
Difficulties in the translation of nanotechnology health products into clinical application pass through several potential challenges such as the understanding of biological interaction, manufacturing complexity and costs, safety issues, and also facing regulatory standards [18], and dedicated efforts should be made in all these sectors. From a regulatory perspective, scientific challenges and regulatory needs for nanotechnology-enabled health products are well known, as discussed by the Joint Research Centre (JRC) [51]; however, additional guidelines particularly in a CT setting, where nanotechnology-impacted IMP would be assessed for the first time, would help in streamlining the overall process and in anticipating regulatory challenges that may be expected during the marketing authorization step. Developing a dedicated guidance for CTs would help to ensure that sponsors acknowledge the submission of any nanotechnology-impacted IMP, nanomaterial, or nanostructure associated with an IMP, such as innovative nanocarriers or supramolecular structures, that may affect the stability, the PK/PD properties, the size, the drug encapsulation efficiency, or the targeting properties, and that may carry along with innovation also unknown risks. In the case of non-ionic surfactant-based nanocarriers (e.g., niosomes, nanoemulsions, micelles), the elucidation of excipients and surfactant role in the IMP formulation should be explored and reported, focusing on in vivo stability or safety issues, and potential toxicity issues could be investigated in ad hoc designed CTs [52]. Coding in a guideline the minimum set of requirements to control the potential impact of nanotechnology on the safety profile of nanomedicines or nanocarriers would help to ensure that a sufficient and transparent level of data are submitted in a CT application and that chemistry manufacturing and control information meet regulatory requirements starting from an early-stage clinical development. The final desired scope would be to support the manufacturing process to achieve a desired quality drug product focusing on CQAs. Envisaging a risk-based approach or exploring other regulatory strategies could support a more proactive and dynamic regulatory framework, able to support innovation in nanotechnology, and drive efforts towards a personalized approach to medicine. But it still would need to ensure that a strong regulatory framework is in place. The question to address is if the current static regulatory framework is still able to support the emerging technology development or if a regulatory conceptual evolution is needed.
Critical quality attributes
A CQA is defined as a physical, chemical, biological, or microbiological property or characteristic that should be within an appropriate limit, range, or distribution to ensure the desired product quality of a drug substance, excipients, intermediates (in-process materials), and drug product [53]. But how can we expect to define CQAs for nanomedicines or nanocarriers if there is still no consensus on the definition of the used terms? There is no standardization in the use of scientific terminology; many different terms are used as synonyms such as nanomedicines, nanoparticles, nanodrugs, or nanopharmaceuticals [54]. Even when the same term is used, in a regulatory environment, there are still misalignments in the adoption by different regulatory bodies. In 2011, the EC published a recommendation on the definition of a nanomaterial [55, 56]; however, EMA issued a definition of nanomedicines [28] and, in relation to quality aspects of nano-based medicines, adopted a working definition [57, 58]. The EC recently updated the definition of nanomaterial in a new recommendation [59] with the aim to support a coherent EU regulatory framework for nanomaterials and help to align legislation across all sectors. However, it is still not aligned with RAs in other regions, as it sets the size limits for the size range to 100 nm in contrast to the FDA guidance. The use of the term nanomaterial in FDA guidance documents does not represent a regulatory definition, and neither a definition is available for the term nanotechnology, nanoscale, or other related terms; in Canada, a working definition of nanomaterial is adopted [60]; a definition of nanomaterial can instead be found for India in the guidelines for evaluation of nanopharmaceuticals [50]. Even when a definition is provided, such as in the case of ISO standards [61], an approximate terminology is adopted when defining the nanoscale (approximately from 1 to 100 nm). Size limit adoption in the definitions is arbitrarily used and definitely not appropriate, at least in a CT setting and for medicinal products, where physical and chemical properties dependent on size continue to apply across regulatory imposed definitions [62]. Divergent descriptions or definitions of the term nanomaterial or nanomedicine are reported in Table 1.
To identify regulatory needs and to enhance any static communication, sharing best practices and knowhow across regulatory agencies, a survey was recently conducted to identify regulatory experience with nanomedicines, information needs of regulators for the categorization and characterization of nanomaterials, and further steps that could support the acceptance of nanotechnology-based products in health care [63]. It was confirmed that regions have a different level of expertise in marketing nanomedicines, and that sharing experience and collaboration of regulatory bodies in the assessment of nanotechnology-based products would be an added value to face the foreseen increasing number of nanotechnology applications. However, to follow such a path, the prerequisite is a consistent terminology and categorization of nanomedicines, supporting communication and collaboration among regulatory bodies. When a list of nano-specific characteristics is proposed as relevant for the approval of CTs, even if not exhaustive, there is clear evidence that there is still not full alignment in the identification of crucial characteristics across regulatory bodies; this is not supporting sponsors in compiling quality data for the purpose of submitting international CTs in different regions. The consolidated takeaway message is that there is a strong need of an accurate characterization of physico-chemical properties by appropriate analytical methods of toxicity assessments including in vitro and in vivo testing, and that crucial to ensure the quality of nanomedicines is to focus on better understanding CQAs. The availability of a global list of CQAs and of a dedicated guideline would support the submission of quality data for nanomedicines and nanocarriers in CTs, and potential early access to nanotechnology health products would be streamlined, as detailed in Fig. 3.

Regulatory path forward for a CQA consolidation and nanotechnology health products potential early access
Innovation in nanotechnology is a very fast evolving field, and regulatory frameworks are not always able to keep up with the speed of the ultimate nano-construct and potential application to the health sector, some are even creating new paradigms such as evolvable platforms for programmable nanoparticle-based therapies [64]. An evident contradiction is highlighted when these valuable projects are receiving public funding, but it is on the other hand clear that the final outcome could not be potentially supported by an equally dynamic and receptive regulatory framework. Even if many efforts have been spent by regulatory bodies so far in the field of nanomedicines and nanocarriers, the combination of speed of technology evolution and the increasing complexity of innovation seems to be an obstacle for regulators, unless a different approach and mindset are adopted by involving all potential stakeholders in the definition of a fit-for-purpose regulatory system [65]. Additional approaches are also proposed by stakeholders in the EU, including a centralized regulatory procedure, the harmonization of requirements to characterize nanomedicines, a scientific consensus on definitions, improved education, and a fostering of awareness on the complexity of nanomedicines [66]. However, regulatory acknowledge of innovation in the healthcare nanotechnology setting is definitely possible, as the Covid-19 emergency is showing, with the bursting introduction of the new technology based on lipid nanoparticles for mRNA vaccine delivery [67, 68]. There is a clear identification by EMA as a regulatory science research need, the one to develop an understanding of, and regulatory response to, nanotechnology and new materials in pharmaceuticals anticipated to be used in the coming 10 years [69]. Even if a fervent activity is noted across stakeholders as evidenced by the recent results of the Refine project in terms of future perspectives for advancing regulatory science of nanotechnology-enabled health products [70], it is still missing a dedicated discussion on the impact of nanotechnology innovation in the assessment of CTs. Nevertheless, there is a current activity carried out in the context of the EU innovation network horizon scanning with a topic proposal on nanotechnology, where hopefully this issue may emerge.
To start supporting with such a process, stemming from the physical and chemical characterization of general nanomaterials-nanomedicines-nanopharmaceuticals and potential CQAs [71], we report in Table 2 the main critical parameters required in CTs for general types of nanomedicine as required by different regulatory bodies [42, 49, 50].
There is alignment in terms of most critical parameters: composition/entrapment efficacy drug loading, size, morphology, stability, structure/surface charge/nomenclature/general properties, and impurities. However, a different level of detail is provided by regulatory bodies in the requested information. This should not be read as a missing scrutiny of details in terms of characterization required by the RAs, as the assessor would require additional information if needed to guarantee the safety and positive benefit-risk balance. However, the approval process may be slowed down and not all required and updated information may be provided by the sponsor during the initial submission, particularly for multi-regional international CTs. Not all regulatory bodies instead are fully aligned with requests on sterility/apyrogenicity and especially drug release. Other requirements such as catalytic activity or GMP process description are also reported.
CQAs are identified also for specific types of nanomaterials-nanomedicines-nanopharmaceuticals [29,30,31,32,33, 43, 45, 46], and even if parameters cannot be generalized, they should be taken into deep consideration as additional input on data and/or methods that can support or accelerate the process of identification of adequate characterization for new or forthcoming nanotechnologies. Among data to be considered and characteristics to be described also for general types of nanomedicines, particularly in terms of additional stability data and carrier functionality, the following not exhaustive list of features that are already coded for specific types of nanomedicines guidelines, such as liposomes or nucleic acid-loaded nanocarriers, could be in our opinion expanded in their scope and suggested as supportive also for general types of nanomedicines, as reported in Table 3.
Conclusion
There is no evidence of a unique rather than standardized approach in the development of guidelines and reflection papers for the evaluation of nanomedicines and nanocarriers, especially when focusing on IMPs in a CT setting. RAs are reluctant to adopt definitions of related terms such as nanomaterial, and prefer to rely on descriptions or working definitions that differ each other. The first step in removing obstacles through a potential standardization process would be the mutual recognition of terms used as synonyms in the same regulatory context. Regulatory bodies have been reacting with different timing and approaches to the emerging innovation of nanotechnology applied to the manufacture of medicinal products. Even if numerous guidelines have been recently developed and profound efforts have been made, it has not been possible to establish a consolidated and valid global platform to frame, from the point of view of the characterization in CTs, all the types of known nanomedicines and nanocarriers but especially those in development or yet to be discovered. Even if there is evidence of an attempt to provide a comprehensive list of requirements for the characterization of nanomedicines and nanocarriers in CTs, the common denominator across regulatory bodies is still a case-by-case basis approach.
Available guidelines are fragmented and not aligned across different regulatory bodies. Additional efforts in the definition of the CQAs and the requirements for the characterization of nanomedicines and nanocarriers should be pursued and would be of benefit to encode them in the regulatory framework dedicated to CTs. CQAs should consider physico-chemical but also technological and biological attributes deriving from the potential transformations and fate of the product in the human body, including those that are function of their performance, or deriving from potential interactions and degradation processes in subjects. However, there will never be a convergence in CQAs if a semantic definition of what should be characterized is not achieved first. The high level of alignment actually available across regulatory bodies of different countries, in the use of a case-by-case basis approach during the evaluation process of a nanomedicine or nanocarrier, reflects the need to deal with continuous scientific, technological, and academic advances and increasing knowledge and expertise in manufacturing processes. Regulatory bodies should capitalize on the experience already acquired to envisage a more global and structured approach, potentially encompassing a renewed risk-based methodology or risk proportionate approaches in clinical trials [72, 73].
Current regulatory challenges and issues are highlighted, mainly due to the speed and complexity of innovation of nanotechnology applied to the health sector. The current lack in capillarity of relevant guidelines, particularly in a CT setting, can lead to a potential missing standardized approach in the characterization, and therefore not fully addressing CQAs, or in delays in the CT authorization process. Among major challenges for regulators in the coming years is the missing uniformity of regulations and guidelines and standardization of requirements for the characterization and control of nanomedicines and nanocarriers in CTs. To surf through the waves of the current and upcoming healthcare innovation and applied nanotechnology, a change of pace and approach to the evaluation of nanomedicines, nanocarriers, and nanotechnology health products is needed, starting from the CT setting. There is probably need to re-think how an already strong regulatory framework can increase efficiency by adapting itself, passing through its own innovation, encompassing for example a more inclusive strategy, with a higher level of involvement and early collaboration with stakeholders so that facing regulatory challenges would be part of the nanotechnology design and development phase.
Availability of data and materials
Data sharing is not applicable to this review article as no new data were created or analyzed in this study.
References
EMA. European Medicines Agency (EMA) - Quality of medicines questions and answers: Part 1. 2022. https://www.ema.europa.eu/en/human-regulatory/research-development/scientific-guidelines/qa-quality/quality-medicines-questions-answers-part-1#variation-section. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA) - Guideline on process validation for finished products - information and data to be provided in regulatory submissions. 2016. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-process-validation-finished-products-information-data-be-provided-regulatory-submissions_en.pdf. Accessed 22 Apr 2022.
EMA. European Medicines Agency (EMA) - Quality guidelines. 2022. https://www.ema.europa.eu/en/human-regulatory/research-development/scientific-guidelines/quality-guidelines. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA) - Quality guidelines: specific types of products. 2022. https://www.ema.europa.eu/en/human-regulatory/research-development/scientific-guidelines/quality/quality-specific-types-products. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA) - Multidisciplinary quality guidelines: nanomedicines. 2022. https://www.ema.europa.eu/en/human-regulatory/research-development/scientific-guidelines/multidisciplinary/multidisciplinary-nanomedicines. Accessed 3 Apr 2022.
EC. European Commission (EC) - Annex 1: Clinical trial application form request for authorisation of a clinical trial on a medicinal product for human use to the competent authorities and for opinion of the ethics committees in the community (revision 4 of November 2009; updated on 22 of November 2019). 2019. https://ec.europa.eu/health/system/files/2019-11/application-form_en_0.pdf. Accessed 3 Apr 2022.
Regulation (EU) No 536/2014. 2014. Regulation (EU) No 536/2014 of the European Parliament and of the Council of 16 April 2014 on Clinical Trials on Medicinal Products for Human Use, and Repealing Directive 2001/20/EC. 2014. https://eur-lex.europa.eu/eli/reg/2014/536/oj. Accessed 3 Apr 2022.
CTIS. Clinical Trials Information System (CTIS) - Clinical trials in the European Union. 2022. https://euclinicaltrials.eu/home. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA) - Marketing Authorisation Application (MAA) Pre-submission meeting request form. 13 October 2020, EMA/571057/2010. 2020. https://www.ema.europa.eu/documents/template-form/marketing-authorisation-application-maa-pre-submission-meeting-request-form-human_en.docx. Accessed 3 Apr 2022.
Clinicaltrials.gov. 2022. https://clinicaltrials.gov. Accessed 3 Apr 2022.
EU Clinical Trials Register. 2022. https://www.clinicaltrialsregister.eu. Accessed 3 Apr 2022.
FDA. Food and Drug Administration (FDA) - Nanotechnology - Over a Decade of Progress and Innovation. A report by the U.S. Food and Drug Administration. 2020. https://www.fda.gov/media/140395/download. Accessed 3 Apr 2022.
Anselmo AC, Mitragotri S. Nanoparticles in the clinic: An update. Bioeng Transl Med. 2019;4(3):e10143. https://doi.org/10.1002/btm2.10143.
Farjadian F, Ghasemi A, Gohari O, Roointan A, Karimi M, Hamblin MR. Nanopharmaceuticals and nanomedicines currently on the market: challenges and opportunities. Nanomedicine. 2019;14:93–126. https://doi.org/10.2217/nnm-2018-0120.
Vencken SF, Greene CM. Chapter 15 - A review of the regulatory framework for nanomedicines in the European Union. In: Inorganic Frameworks as Smart Nanomedicines. William Andrew Publishing; 2018. p. 641–79. https://doi.org/10.1016/B978-0-12-813661-4.00015-8.
Choi YH, Han HK. Nanomedicines: current status and future perspectives in aspect of drug delivery and pharmacokinetics. J Pharm Investig. 2018;48:43–60. https://doi.org/10.1007/s40005-017-0370-4.
Coty J-B, Vauthier C. Characterization of nanomedicines: A reflection on a field under construction needed for clinical translation success. J Control Release. 2018;275:254–68. https://doi.org/10.1016/j.jconrel.2018.02.013.
Hua S, de Matos MBC, Metselaar JM, Storm G. Current Trends and Challenges in the Clinical Translation of Nanoparticulate Nanomedicines: Pathways for Translational Development and Commercialization. Front Pharmacol. 2018;9:790. https://doi.org/10.3389/fphar.2018.00790.
Milane L, Amiji M. Clinical approval of nanotechnology-based SARS-CoV-2 mRNA vaccines: impact on translational nanomedicine. Drug Deliv and Transl Res. 2021;11:1309–15. https://doi.org/10.1007/s13346-021-00911-y.
Younis MA, Tawfeek HM, Abdellatif AAH, Abdel-Aleem JA, Harashima H. Clinical translation of nanomedicines: Challenges, opportunities, and keys. Adv Drug Deliv Rev. 2022;181:114083. https://doi.org/10.1016/j.addr.2021.114083.
Halamoda-Kenzaoui B, Vandebriel RJ, Howarth A, et al. Methodological needs in the quality and safety characterisation of nanotechnology-based health products: Priorities for method development and standardisation. J Control Release. 2021;336:192–206. https://doi.org/10.1016/j.jconrel.2021.06.016.
Shan X, Gong X, Li J, Wen J, Li Y, Zhang Z. Current approaches of nanomedicines in the market and various stage of clinical translation. Acta Pharm Sin B. 2022;12(7):3028–48. https://doi.org/10.1016/j.apsb.2022.02.025.
Refine Project. Regulatory Science Framework for Nano(bio)material-based Medical Products and Devices. http://refine-nanomed.eu/. Accessed 7 Nov 2022.
Foulkes R, Man E, Thind J, Yeung S, Joy A, Hoskins C. The regulation of nanomaterials and nanomedicines for clinical application: current and future perspectives. Biomater Sci. 2020;8:4653–64. https://doi.org/10.1039/D0BM00558D.
EC. European Commission (EC) - Nanomaterials: Commission proposes case by case approach to assessment (3 October 2012). 2012. https://ec.europa.eu/commission/presscorner/api/files/document/print/en/memo_12_732/MEMO_12_732_EN.pdf. Accessed 3 Apr 2022.
EC. European Commission (EC) - Scientific Committee on Emerging and Newly Identified Health Risks (2009). 19 January 2009. Risk Assessment of Products of Nanotechnologies. 2009. https://ec.europa.eu/health/ph_risk/committees/04_scenihr/docs/scenihr_o_023.pdf. Accessed 3 Apr 2022.
EC. European Commission (EC) - Scientific Committee on Emerging and Newly Identified Health Risks (2014). 10 -11 June 2014. Opinion on Nanosilver: safety, health and environmental effects and role in antimicrobial resistance. 2014. https://ec.europa.eu/health/scientific_committees/emerging/docs/scenihr_o_039.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMEA/CHMP/79769/2006. Reflection paper on nanotechnology-based medicinal products for human use. 2006. https://etp-nanomedicine.eu/wp-content/uploads/2018/10/reflection-paper-nanotechnology-based-medicinal-products-human-use_en-1.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMA/CHMP/QWP/799402/2011. Reflection Paper on the Pharmaceutical Development of Intravenous Medicinal Products Containing Active Substances Solubilised in Micellar Systems. 2012. https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-pharmaceutical-development-intravenous-medicinal-products-containing-active_en.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMA/CHMP/13099/2013. Joint MHLW/EMA reflection paper on the development of block copolymer micelle medicinal products. 2013. https://www.ema.europa.eu/en/documents/scientific-guideline/joint-mhlw/ema-reflection-paper-development-block-copolymer-micelle-medicinal-products_en.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMA/CHMP/806058/2009/Rev. 02. Reflection paper on the data requirements for intravenous liposomal products developed with reference to an innovator liposomal product. 2013. https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-data-requirements-intravenous-liposomal-products-developed-reference-innovator_en.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMA/325027/2013. Reflection paper on surface coatings: general issues for consideration regarding parenteral administration of coated nanomedicine products. 2013. https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-surface-coatings-general-issues-consideration-regarding-parenteral-administration_en.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMA/CHMP/SWP/620008/2012. Reflection paper on the data requirements for intravenous iron-based nano-colloidal products developed with reference to an innovator medicinal product. 2015. https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-data-requirements-intravenous-iron-based-nano-colloidal-products-developed_en.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMA/484400/2014. Mandate of the EMA Innovation Task Force (ITF). 2014. https://www.ema.europa.eu/en/documents/other/mandate-european-medcines-agency-innovation-task-force-itf_en.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMA/CHMP/QWP/545525/2017 Rev. 2. Committee for Medicinal Products for Human Use (CHMP) - Guideline on the requirements for the chemical and pharmaceutical quality documentation concerning investigational medicinal products in clinical trials. 2022. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-requirements-chemical-pharmaceutical-quality-documentation-concerning-investigational_en-1.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMA/CHMP/BWP/534898/2008 Rev. 2. Committee for Medicinal Products for Human Use (CHMP) - Guideline on the requirements for quality documentation concerning biological investigational medicinal products in clinical trials. 2022. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-requirements-quality-documentation-concerning-biological-investigational-medicinal_en-2.pdf. Accessed 3 Apr 2022.
Musazzi UM, Marini V, Casiraghi A, Minghetti P. Is the European regulatory framework sufficient to assure the safety of citizens using health products containing nanomaterials? Drug Discov Today. 2017;22:870–82. https://doi.org/10.1016/j.drudis.2017.01.016.
FDA. Food and Drug Administration (FDA) - Guidance for Industry CGMP for Phase 1 Investigational Drugs. 2008. https://www.fda.gov/media/70975/download. Accessed 3 Apr 2022.
FDA. Food and Drug Administration (FDA) - FDA’s guidance for industry Content and Format of Investigational New Drug Applications (INDs) for Phase 1 Studies of Drugs, Including Well-Characterized, Therapeutic, Biotechnology-derived Products. 1995. https://www.fda.gov/media/71203/download. Accessed 3 Apr 2022.
FDA. Food and Drug Administration (FDA) - Guidance for Industry - INDs for Phase 2 and Phase 3 Studies Chemistry, Manufacturing, and Controls Information. 2003. https://www.fda.gov/media/70822/download. Accessed 3 Apr 2022.
FDA. Food and Drug Administration (FDA) - Guidance for Industry Considering Whether an FDA-Regulated Product Involves the Application of Nanotechnology. 2014. https://www.fda.gov/media/88423/download. Accessed 3 Apr 2022.
FDA. Food and Drug Administration (FDA) - Draft Guidance - Drug Products, Including Biological Products, that Contain Nanomaterials. Guidance for Industry. 2022. https://www.fda.gov/media/157812/download. Accessed 13 Oct 2022.
FDA. Food and Drug Administration (FDA) - Liposome Drug Products Chemistry, Manufacturing, and Controls; Human Pharmacokinetics and Bioavailability; and Labeling Documentation. Guidance for Industry. 2018. https://www.fda.gov/media/70837/download. Accessed 3 Apr 2022.
PMDA. Pharmaceuticals and Medical Devices Agency. Nanomedicine Initiative Working Group. 2013. https://www.pmda.go.jp/english/rs-sb-std/rs/0010.html. Accessed 3 Apr 2022.
MHLW. Ministry of Health, Labour and Welfare (MHLW) - Reflection paper on nucleic acids (siRNA)-loaded nanotechnology-based drug products. 2016. https://www.nihs.go.jp/drug/section4/160328_MHLW_siRNA_RP.pdf. Accessed 3 Apr 2022.
MHLW. Ministry of Health, Labour and Welfare (MHLW) - Guideline for the Development of Liposome Drug Products. 2016. https://www.nihs.go.jp/drug/section4/160328_MHLW_liposome_guideline.pdf. Accessed 3 Apr 2022.
HC. Health Canada (HC) - Current Issues with Nanomedicines in Canada. 2010. https://www.ema.europa.eu/en/documents/presentation/presentation-nanomedicines-current-initiatives-canada-duc-vu-health-canada_en.pdf. Accessed 3 Apr 2022.
HC. Health Canada (HC) - Policy Statement on Health Canada's Working Definition for Nanomaterial. 2011. https://www.canada.ca/en/health-canada/services/science-research/reports-publications/nanomaterial/policy-statement-health-canada-working-definition.html. version 2. Accessed 3 April 2022.
HC. Health Canada (HC) - Frequently Asked Questions Related to the Policy Statement on Health Canada's Working Definition for Nanomaterial. 2011. https://www.canada.ca/en/health-canada/services/science-research/reports-publications/nanomaterial/policy-statement-working-definition-nanomaterial-frequently-asked-questions.html#a16. Accessed 3 Apr 2022.
DBT. Department of Biotechnology Government of India (DBT), New Delhi - Guidelines for Evaluation of Nanopharmaceuticals in India, Department of Biotechnology Government of India. 2019. http://dbtindia.gov.in/sites/default/files/uploadfiles/Guidelines_For_Evaluation_of_Nanopharmaceuticals_in_India_24.10.19.pdf. Accessed 3 Apr 2022.
EC. European Commission (EC), Joint Research Centre, Halamoda-Kenzaoui B, Box H, van Elk M, Gaitan S, Geertsma RE, Gainza Lafuente E, Owen A, Del Pozo A, Roesslein M, Bremer-Hoffmann S. Anticipation of regulatory needs for nanotechnology-enabled health products. Luxembourg: Publications Office of the European Union; 2019. https://doi.org/10.2760/596822. EUR 29919 EN; ISBN 978-92-76-12554-9.
Ge X, Wei M, He S, Yuan W. Advances of Non-Ionic Surfactant Vesicles (Niosomes) and Their Application in Drug Delivery. Pharmaceutics. 2019;11(2):55. https://doi.org/10.3390/pharmaceutics11020055.
EMA. European Medicines Agency (EMA) - EMA/CHMP/ICH/167068/2004 - Committee for Human Medicinal Products ICH guideline Q8 (R2) on pharmaceutical development, Step 5. 2017. https://www.ema.europa.eu/en/documents/scientific-guideline/international-conference-harmonisation-technical-requirements-registration-pharmaceuticals-human-use_en-11.pdf. Accessed 3 Apr 2022.
EC. European Commission (EC), Joint Research Centre, Quirós Pesudo L, Balahur A, Gottardo S, Rasmussen K, Wagner G, Joanny G, Bremer-Hoffmann S. Mapping Nano-medicine Terminology in the Regulatory Landscape. Luxembourg: Publications Office of the European Union; 2018. https://doi.org/10.2760/753829. ISBN 978-92-79-89872-3.
EC. European Commission (EC) - Commission Recommendation of 18 October 2011 on the definition of nanomaterial, text with EEA relevance (2011/696/EU). 2011. https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32011H0696&from=EN. Accessed 3 Apr 2022.
EC. European Commission (EC), JRC Science for Policy Report, Rauscher H, Roebben G, Mech A, Gibson N, Kestens V, Linsinger TPJ, Riego Sintes J. An overview of concepts and terms used in the European Commission’s definition of nanomaterial. JRC, Ispra: European Commission; 2019. https://doi.org/10.2760/459136. ISBN 978-92-79-99660-3.
EMA. European Medicines Agency (EMA), Papaluca M. Way forward. 1st International Workshop on Nanomedicine. London, United Kingdom; 2010. https://www.ema.europa.eu/en/documents/presentation/presentation-way-forward-marisa-papaluca-ema_en.pdf. Accessed 3 Apr 2022.
Pita R, Ehmann F, Papaluca M. Nanomedicines in the EU-Regulatory Overview. AAPS J. 2016;18(6):1576–82. https://doi.org/10.1208/s12248-016-9967-1.
EC. European Commission (EC) - Commission Recommendation on the definition of nanomaterial (2022). 2022. https://ec.europa.eu/environment/chemicals/nanotech/pdf/C_2022_3689_1_EN_ACT_part1_v6.pdf. C(2022) 3689 final. Accessed 13 Oct 2022.
HC. Health Canada (HC) - Policy Statement on Health Canada's Working Definition for Nanomaterial. 2011. https://www.canada.ca/en/health-canada/services/science-research/reports-publications/nanomaterial/policy-statement-health-canada-working-definition.html. Accessed 3 Apr 2022.
ISO. International Organization for Standardization (ISO) - Definition of nanomaterial. 2017. https://www.iso.org/obp/ui/#iso:std:iso:ts:21623:ed-1:v1:en:term:3.10. Accessed 3 Apr 2022.
Boverhof DR, Bramante CM, Butala JH, Clancy SF, Lafranconi M, West J, Gordon SC. Comparative assessment of nanomaterial definitions and safety evaluation considerations. Regul Toxicol Pharmacol. 2015;73(1):137–50. https://doi.org/10.1016/j.yrtph.2015.06.001.
EC. European Commission (EC), JRC Technical Reports - Bremer S, Halamoda-Kenzaoui B, Borgos SE. Identification of regulatory needs for nanomedicines: 1st EU-NCL survey with the “Nanomedicine” working group of the international pharmaceutical regulators. 2016. http://publications.jrc.ec.europa.eu/repository/bitstream/JRC103557/170412-report-identification_regulatory_needs_nanomedicines-final_05.12.16_online_version.pdf. Accessed 3 Apr 2022.
EvoNano. Evolvable platform for programmable nanoparticle-based cancer therapies (EvoNano). 2022. https://evonano.eu/. Accessed 3 Apr 2022.
Allan J, Belz S, Hoeveler A, Hugas M, Okuda H, Patri A, Rauscher H, Silva P, Slikker W, Sokull-Kluettgen B, Tong W, Anklam E. Regulatory landscape of nanotechnology and nanoplastics from a global perspective. Regul Toxicol Pharmacol. 2021;122:104885. https://doi.org/10.1016/j.yrtph.2021.104885.
Isles MP. Nanomedicines and Nanosimilars - Why a Robust Centralised Regulatory Framework Is Essential to Enhance Patient Safety. Front Pharmacol. 2022;12:787239. https://doi.org/10.3389/fphar.2021.787239.
Nanotechnology N. Nanomedicine and the COVID-19 vaccines. Nat Nanotechnol. 2020;2020(15):963. https://doi.org/10.1038/s41565-020-00820-0.
Schoenmaker L, Witzigmann D, Kulkarni JA, Verbeke R, Kersten G, Jiskoot W, Crommelin DJA. mRNA-lipid nanoparticle COVID-19 vaccines: Structure and stability. Int J Pharm. 2021;601:120586. https://doi.org/10.1016/j.ijpharm.2021.120586.
EMA. European Medicines Agency (EMA) - EMA/705364/2021, Regulatory Science and Innovation. Regulatory Science Research Needs (version 1.0). 2021. https://www.ema.europa.eu/en/documents/other/regulatory-science-research-needs_en.pdf. Accessed 3 Apr 2022.
Halamoda-Kenzaoui B, Geertsma R, Pouw J, et al. Future perspectives for advancing regulatory science of nanotechnology-enabled health products. Drug Deliv Transl Res. 2022;12:2145–56. https://doi.org/10.1007/s13346-022-01165-y.
Đorđević S, Gonzalez MM, Conejos-Sánchez I, Carreira B, Pozzi S, Acúrcio RC, Satchi-Fainaro R, Florindo HF, Vicental MJ. Current hurdles to the translation of nanomedicines from bench to the clinic. Drug Deliv Transl Res. 2021;12:500–25. https://doi.org/10.1007/s13346-021-01024-2.
Expert Group on CTs. Expert Group on Clinical Trials - Risk proportionate approaches in clinical trials. Recommendations of the expert group on clinical trials for the implementation of Regulation (EU) No 536/2014 on clinical trials on medicinal products for human use. 2017. https://ec.europa.eu/health/system/files/2017-08/2017_04_25_risk_proportionate_approaches_in_ct_0.pdf. Accessed 3 Apr 2022.
EMA. European Medicines Agency (EMA). EMEA/CHMP/SWP/28367/07 Rev. 1. Committee for Medicinal Products for Human Use (CHMP) - Guideline on strategies to identify and mitigate risks for first-in-human and early clinical trials with investigational medicinal products. 2017. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-strategies-identify-mitigate-risks-first-human-early-clinical-trials-investigational_en.pdf. Accessed 3 Apr 2022.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by Diego Alejandro Dri, Federica Rinaldi, Maria Carafa, and Carlotta Marianecci. The first draft of the manuscript was written by Diego Alejandro Dri and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Dri, D.A., Rinaldi, F., Carafa, M. et al. Nanomedicines and nanocarriers in clinical trials: surfing through regulatory requirements and physico-chemical critical quality attributes. Drug Deliv. and Transl. Res. 13, 757–769 (2023). https://doi.org/10.1007/s13346-022-01262-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13346-022-01262-y