
Abstract
Objectives
To investigate clinical characteristics and risk factors for atypical community-acquired pneumonia (CAP) in children.
Methods
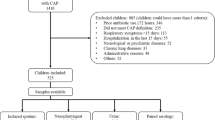
Multiplex polymerase chain reaction and specific IgM determination were used to detect atypical bacteria in 661 hospitalized children aged 1–15 years with CAP. Clinical and epidemiological patterns were compared between typical and atypical CAP.
Results
Children in atypical CAP group manifested significantly lower rates of wheezing, bronchial rales, and interstitial pneumonia and showed higher rates of asthma history, headache, chest pain, and lobar pneumonia. Age group, season of disease onset, asthma history, duration of symptom onset to hospital admission, and radiological findings were the significant risk factors for atypical CAP on multivariate logistic regression analysis.
Conclusions
The clinical characteristics and risk factors can be used to identify a child at high risk of atypical CAP.
Similar content being viewed by others


References
Nair H, Simões EA, Rudan I, et al. Global and regional burden of hospital admissions for severe acute lower respiratory infections in young children in 2010: A systematic analysis. Lancet. 2013;381:1380–90.
Hammerschlag MR. Pneumonia due to Chlamydia pneumoniae in children: Epidemiology, diagnosis and treatment. Pediatr Pulmonol. 2003;36:384–90.
Cunha BA. The atypical pneumonia: Clinical diagnosis and Importance. Clin Microbiol Infect. 2006;2:12–24.
Huong PLT, Hien PT, Lan NTP, Binh TQ, Tuan DM, Anh DD First report on prevalence and risk factors of severe atypical pneumonia in Vietnamese children aged 1–15 years. BMC Public Health. 2014;14:1304.
Salaria M, Singh M. Atypical pneumonia in children. Indian Pediatr. 2002:39:259–66.
Bradley JS, Byington CL, Shah SS, et al. The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53:617–30.
Miyashita N, Fukano H, Yoshida K, Niki Y, Matsushima T. Is it possible to distinguish between atypical pneumonia and bacterial pneumonia?: Evaluation of the guidelines for community-acquired pneumonia in Japan. Respir Med. 2004;98:952–60.
Takaki M, Nakama T, Ishida M, et al. High incidence of community-acquired pneumonia among rapidly aging population in Japan: A prospective hospital-based surveillance. Jpn J Infect Dis. 2014;67:269–75.
Campbell LA, Perez Melgosa M, Hamilton DJ, Kuo CC, Grayston JT Detection of chlamydia pneumoniae by polymerase chain reaction. J Clin Microbiol. 1992;30:434.
Nagai T, Sobajima H, Iwasa M, et al. Neonatal sudden death due to Legionella pneumoniae associated with water birth in a domestic spa bath. J Clin Microbiol. 2003; 41:2227–29.
Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143:29–36.
Fluss R, Faraggi D, Reiser B Estimation of the Youden Index and its associated cutoff point. Bio J. 2005;47:458–72.
R Development Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, 2008.
Mikasa K, Aoki N, Aoki Y, et al. JAID/JSC Guidelines for the Treatment of Respiratory Infectious Diseases: The Japanese Association for Infectious Diseases/Japanese Society of Chemotherapy — The JAID/JSC Guide to Clinical Management of Infectious Disease/Guideline-preparing Committee Respiratory Infectious Disease WG. J Infect Chemother. 2016;22:S1–S65.
Huong PL, Thi NT, Nguyet NT, Van TK, Hang DT, Huong VT, et al. First report on clinical features of Mycoplasma pneumoniae infections in Vietnamese children. Jpn J Infect Dis. 2007;60:370–3.
Prapphal N, Suwanjutha S, Durongkaveroj P, et al. Prevalence and clinical presentations of atypical pathogens infection in community acquired pneumonia in Thailand. J Med Assoc Thai. 2006;89:1412–9.
Ma YJ, Wang SM, Cho YH, et al Taiwan Pediatric Infectious Disease Alliance. Clinical and epidemiological characteristics in children with community-acquired Mycoplasma pneumonia in Taiwan: A nationwide surveillance. J Microbiol Immunol Infect. 2015;48:632–8.
Acknowledgements
Prof. Nguyen Thanh Liem — Former Director of the Vietnam National Children’s Hospital for helpfully supporting the study, Ms. Do Thi Bich Ngoc and to our colleagues at National Institute of Hygiene & Epidemiology and Vietnam National Children’s Hospital for technical help.
Funding
Funding: National Foundation for Science and Technology Development (NAFOSTED), grant no. 106.03-2010.36 from The Ministry of Science and Technology, Vietnam. Competing interest: None stated.
Author information
Authors and Affiliations
Contributions
PLTH: conceptualized and designed the study, designed and performed laboratory analyses, drafted the initial manuscript, reviewed and revised the manuscript; PTH: recruited patients, collected and entered data, follow-up patients; NTPL: participated in laboratory analyses, reviewed the manuscript; DMT: designed the study, recruited patients, follow-up patients, participated in discussion and interpretation of the findings; DDA: had a substantial contribution in experimental design and interpretation of ELISA and multiplex PCR, critically reviewed the manuscript; TQB: cleaned data, supervised data collection, performed statistical analyses and interpretation of findings, critically reviewed and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Research Ethics Committee Vietnam National Children’s Hospital; No. 1124/HDDD, dated 2 June, 2010.
Electronic Supplementary Material
Rights and permissions
About this article

Cite this article
Huong, P.L.T., Hien, P.T., Lan, N.T.P. et al. Clinical Patterns and Risk Factors for Pneumonia Caused by Atypical Bacteria in Vietnamese Children. Indian Pediatr 58, 1056–1058 (2021). https://doi.org/10.1007/s13312-021-2373-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13312-021-2373-5