
Abstract
Comparative effectiveness of behavioral interventions to mitigate the impacts of degeneration-based cognitive decline is not well understood. To better address this gap, we summarize the studies from the Healthy Action to Benefit Independence & Thinking (HABIT®) program, developed for persons with mild cognitive impairment (pwMCI) and their partners. HABIT® includes memory compensation training, computerized cognitive training (CCT), yoga, patient and partner support groups, and wellness education. Studies cited include (i) a survey of clinical program completers to establish outcome priorities; (ii) a five-arm, multi-site cluster randomized, comparative effectiveness trial; (iii) and a three-arm ancillary study. PwMCI quality of life (QoL) was considered a high-priority outcome. Across datasets, findings suggest that quality of life was most affected in groups where wellness education was included and CCT withheld. Wellness education also had greater impact on mood than CCT. Yoga had a greater impact on memory-dependent functional status than support groups. Yoga was associated with better functional status and improved caregiver burden relative to wellness education. CCT had the greatest impact on cognition compared to yoga. Taken together, comparisons of groups of program components suggest that knowledge-based interventions like wellness education benefit patient well-being (e.g., QoL and mood). Skill-based interventions like yoga and memory compensation training aid the maintenance of functional status. Notably, better adherence produced better outcomes. Future personalized intervention approaches for pwMCI may include different combinations of behavioral strategies selected to optimize outcomes prioritized by patient values and preferences.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Support for Behavioral Interventions
There have been significant advances towards the early identification of Alzheimer’s disease (AD) with the diagnosis of mild cognitive impairment (MCI) due to Alzheimer’s disease or a related disorder (ADRD) becoming fairly common [1, 2]. Amnestic MCI is defined as memory abnormality beyond normal age-related decline with relatively intact functional capacity, in other words, not (yet) dementia [3]. Fifteen to twenty percent of those 65 or older have MCI and approximately one-third of these individuals develop dementia related to Alzheimer’s disease in 5 years [4].
While the FDA recently approved aducanumab for early stages of AD, no medical therapy has yet proven robust in impacting patient function or patient wellness in MCI [5]. Moreover, the vast majority of clinical trials ignore partner or caregiver outcomes in spite of the significant impact AD has on their well-being [6]. Based on seminal studies [7, 8], nascent research [9], and consensus statements [10], patients and families are increasingly receiving recommendations to engage in nonpharmacological treatments, aka behavioral interventions (e.g., physical exercise, note taking, social engagement, and computerized cognitive training). The evidence is indeed promising that such behavioral interventions can be beneficial in MCI. Namely, recent meta-analyses suggest that cognitive interventions have significant, small to medium effect sizes (Hedges’ g ranging from 0.23 to 0.40) for persons with MCI (pwMCI) on multiple cognitive domains, including memory, attention, and processing speed [11]. Meta-analysis of non-cognitive effects of cognitive interventions in pwMCI demonstrates significant though small effects for activities of daily living (ADLs; Cohen’s d = 0.23), mood (d = 0.16) and metacognitive outcomes (i.e., how one thinks/feels about one’s memory; d = 0.30) [12]. Physical exercise meta-analysis outcomes in individuals over 50 have provided similar overall effect sizes on cognition (mean effect size = 0.29) [13].
To date, most studies and consequently most meta-analyses have focused on single interventions, such as cognitive rehabilitation, physical exercise training, or psychotherapy. Yet, these reviews are hampered by significant variations in the interventional approaches. Within a category like physical exercise [12], there is no consensus about best intervention type, intensity, or duration [14]. Even as ascertainment of appropriate methods and “doses” for these behavioral methods lags, there is increasing support for the use of multi-component interventions in dementia prevention efforts [8]. This could reflect how great the needs of patients and caregivers are when curative treatments remain so elusive [15]. For example, the Alzheimer’s Association is currently funding a $20 million study of physical exercise, diet, cognitive and social stimulation, and improved self-management of blood pressure in healthy elderly. Finally, while studies comparing single and multi-component interventions to “placebo” are accumulating, there is a dearth of literature examining the effectiveness of various behavioral interventions in comparison to each other.
Grounding Behavioral Interventions in Rehabilitation Approaches
The focus in rehabilitation can be to improve the impaired ability itself (remediation), to learn methods to adapt to the changed ability without attempting to improve the ability itself (compensation), or both simultaneously. Computerized brain training often adopts a remediation approach to cognitive loss in MCI. In contrast, compensation for cognitive loss in MCI is many times taught through therapist-based training in which the patient is taught strategies, such as mnemonic techniques or an adaptive system of taking notes or keeping calendars or lists. Previously, we compared outcomes for a compensatory memory calendar training intervention, known as the memory support system (MSS), to a computerized cognitive exercise intervention, as well as to no-treatment control groups in randomized trials [16, 17]. This comparison pitted the two approaches against one another (with comparison to a no-treatment control) in a study of an intervention seeking to mitigate the functional impact of cognitive loss measured as patient memory-related activities of daily living (mADLs). mADLs were significantly improved over no treatment groups in those randomized to the MSS condition. Moreover, sense of memory self-efficacy significantly improved for those trained in use of the MSS but not in those receiving computerized cognitive exercise or no treatment conditions [16, 17]. Furthermore, care partners in both treatment groups showed stable mood and anxiety, while partners in the untreated group showed worsening depression and anxiety over 6 months [18]. Similarly, a systematic review of the literature found that various computerized interventions aimed at improving cognition may reduce anxiety and depression in pwMCI, and those trained with therapists in compensatory strategies (like the MSS training highlighted above) have better ADLs, self-beliefs about memory, and confidence [12].
Grounding Behavioral Approaches in Learning Theory
The behavioral interventions described above are predicated on the capacity of pwMCI to learn new patterns of behavior in the interest of remediation and compensation. This, however, seems a paradox since the hallmark impairment of common amnestic MCI is impairment in learning and memory. However, it is well known that humans possess multiple memory systems, including distinct declarative vs non-declarative memory processes [19]. Different functional neuroanatomy underlies these systems, such that procedural learning (one form of non-declarative memory) appears to remain intact even as declarative memory declines [19]. This appears to be true during the early course of AD (see Fig. 1). Indeed, a systematic review and meta-analysis of studies (k = 17) comparing procedural learning between individuals with aMCI or AD dementia and healthy controls [20] demonstrated that while procedural learning performance was not statistically identical between individuals with aMCI or AD dementia, and healthy older adults, the difference was clinically and statistically trivial. This preservation of procedural learning contributes to the training of compensatory techniques, as done in the HABIT® program [20]. In this paper, we summarize studies from HABIT®, a large, longstanding, multi-dimensional behavioral intervention program for pwMCI and their partners.

Conceptual model of multisystem memory decline in Alzheimer’s disease
The HABIT (Healthy Action to Benefit Independence &Thinking®) Program
Participants
The ongoing clinical HABIT® program targets people with amnestic forms of MCI and their partners. These pairs or dyads of people are typically identified for referral to the HABIT® program from Neuropsychology and Behavioral Neurology clinics but can come from other referral sources including via self-referral. Neuropsychologists review patients’ medical history, symptom profile, physical exam, and neuropsychological testing. Eligible patients are required to have a clinical diagnosis of amnestic MCI (either single domain or multi-domain). Partners are required to be cognitively normal (MMSE > 24) without severe major depression that would prioritize their own mental health treatment first. For associated research studies, a MCI diagnosis is based on NIA-Alzheimer Association criteria [3].
Interventions
The goal of the HABIT® program, as the name hopefully conveys, is to initiate new healthy behavioral habits that slow functional loss and maximize coping and adaptation to cognitive loss so pwMCI can do as well as possible for as long as possible, even if brain disease progresses. The program consists of 10 days of intervention. Historically, these 10 days are delivered over 2 weeks. There are 5 components, so each participant and care partner received 50 h (5 components, each for 1 h, for 10 days) of intervention.
-
1.
Physical exercise: Participants engaged daily in 45–60 min of physical exercise via yoga. Hatha yoga requires no machinery and limited equipment and is suited to the different levels of baseline physical activity of our participants and partners. Adapted Hatha Yoga is practiced so participants can sit on chairs for some asana (poses) and use the chair for support for balance during other standing poses and for other parts of the sequence. This adapted Hatha Yoga style is accessible even for those who have limited mobility, including those who use walkers or wheelchairs. HABIT® yoga also incorporates breathing and meditation and cultivates an overall sense of connection and support. Instructors have at least 200 h of training and are certified. The yoga intervention is intended to initiate and sustain a schedule of physical activity rather than ultimately prescribing a type of physical activity. Post-program, participants and partners are encouraged to maintain a schedule of 150 min of their preferred exercise per week. Post-program, we consider yoga, swimming, walking, running, or formal exercise programming like water aerobics, resistance training, etc. to count equivalently towards this total. We nevertheless provide a customized DVD as a supplement for continued practice after the program to those that opt to continue yoga. The DVD includes sections on the following: poses, modifications, benefits, breathing, and meditation practices.
-
2.
Computerized cognitive training (CCT): The HABIT® program uses the commercially available Posit Science product BrainHQ® on tablets (e.g., iPads). This product is the latest generation of the program studied by Smith et al. [21] and Zelinski et al. [22]. Participants complete 45–60 min of training daily in the program and are encouraged to accumulate at least 40 h of computerized brain training post-program. Participants are provided a 1-year subscription to the program. All participants’ adherence and progress, amount of usage, and number of levels gained can now be tracked as their account is registered through the clinician portal provided by Posit Science.
-
3.
Wellness education: The wellness education program involves daily 45–60-min group lecture sessions with topics including Introduction to the Program, Living with MCI, Changes in Roles and Relationships, Sleep Hygiene, Steps to Healthy Brain Aging, Preventing Dementia, MCI and Depression, Nutrition and Exercise, Assistive Technologies, Participating in Research, and Community Resources.
-
4.
Support groups: Concurrent but separate daily 45–60-min support group sessions are provided for patients and their partners. The goal in each session is to provide emotional support and education about cognitive loss associated with MCI.
Patient: The patient support group is reminiscence focused. Homework assignments are given in the LifeBio Memory Journal© and used as a basis for group sessions the next day. Patients also accomplish emotional processing around the MCI diagnosis and lifestyle impact with a goal toward acceptance and healthy dialog with partners.
Partner: The care partner support group is a traditional caregiver support group with no set curriculum, but common caregiving themes that emerge include ambiguity of the diagnosis, denial, disclosure to friends and family, role changes, communication, emotional adjustment, behavior changes in our loved one, safety, driving issues, planning for the future, caregiver health, manufacturing success, dementia and relationships, communication skills, defense mechanisms, dimensions of wellness, effects on emotions, family roles, grief and loss, healthy relationships, intimacy needs, introduction to self-help, ongoing care needs, spirituality, stages of change, and thought restructuring. Trained group facilitators provide emotional support, offer guidance about communication approaches, and address denial as well as the grief and loss associated with the diagnosis of MCI in a loved one.
-
5.
Memory support system (MSS) training: This intervention for MCI, pioneered by Greenaway et al. [23, 24], involves intensive training to use a calendaring/notetaking/tracking system. Of note, a key finding established that when memory support is given alone versus control, there are improvements in memory-based activities of daily living, especially for those that are most adherent [23, 24]. Each member of the dyad is provided a set of specifically designed day-at-a-glance monthly calendars and receives 45–60 min of daily MSS training throughout the program. The three stages of the MSS are grounded in learning theory [25]: (1) an acquisition phase in which use of the MSS is learned, (2) an application phase in which a participant is taught to apply the MSS to his/her daily life, and (3) an adaptation phase in which a participant practices incorporating the MSS into his/her daily life so as to make its use habitual.
A specific set of MSS training questions is used in each daily session. These questions cover the topics to be learned in each phase of training. Participants progress to the next training phase after demonstrating 100% accuracy on questions in a given stage for two consecutive days. Homework is given at the end of each session to focus on the practice of MSS skills. At home, the care partners play the role of asking the MSS training questions. Even for cognitively intact people, 10 h of direct training may be insufficient for the acquisition of a new procedural learning skill. Care partners are thus included in the training to provide additional cuing and practice outside of the therapy sessions.
Outcomes
Grounding the Program in Patient Preference
There is significant debate within the field as to which behavioral intervention outcomes to measure and how to consistently measure them. Most studies of behavioral interventions have focused on the impact on cognition itself for cognitively normal older adults or for those with MCI. However, the growing culture of patient-centered care considers patients to be members of the healthcare team with an active voice in their treatment and care. Researchers are increasingly aware of the need to ask patients and caregivers what they want from an intervention. Thus, the first aim of our largest study was to obtain input from pwMCI and their partners about the outcomes they value most.
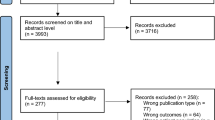
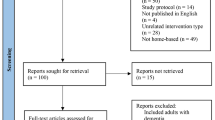
An online survey tool was used to expand prior interview-based patient/partner preference analyses [13]. The survey was conducted in 2014 and used to select the primary outcome measure for the subsequent comparative effectiveness trial. Two-hundred thirty HABIT® program completers (from 2008 to 2014) who provided emails for subsequent contact were eligible to participate. This included dyads who completed the full HABIT® program at the Mayo Clinic in Minnesota, Arizona, or Florida. Their emails were used to send a Qualtrics survey to the partnerships. Usable data on outcome importance came from 88 respondents, including 29 patients, 54 partners, and 13 cases where the patient and partner worked together to complete the survey. Sixty-nine percent of the patient respondents were male. Spouses constituted 87% of partners, 9% were adult children of the patient, and 4% were friends of the patient. Mean (standard deviation) age of the patient and partner groups were 72.9 (8.3) and 67.1 (8.2) years, respectively. Mean (standard deviation) years of education for the patient and partner groups were 16.8 (2.3) and 16.5 (2.3) years, respectively. Patients and partners had completed all of the measures listed in the survey. They were thus familiar with the constructs they were asked to prioritize. We found that they rated patient quality of life (QoL), patient self-efficacy, patient mood, and mADLs to be the most important outcomes to target with behavioral interventions (in that order) [42, 43]. However, review of 442 active MCI clinical trials listed on ClinicalTrials.gov at that time revealed that less than 10% of these studies included a QoL outcome and only 9 studies used QoL as a primary outcome measure [43]. Only 4 studies included self-efficacy as an outcome. Based on the survey, pwMCI QoL was selected as one of the primary outcomes of the comparative effectiveness trial.
A common set of clinical assessments has been utilized across all HABIT®-related studies and in the clinical HABIT® program. This includes 12–14 measures with 7 completed by the pwMCI about him or herself, 3 completed by the partner about the pwMCI, and 5 completed by the partner about his or her own experience. We describe these below.
Measures completed by the pwMCI
Quality of Life-AD (QoL-AD) [26]
A 13-item measure developed to assess quality of life with high criterion, concurrent, and construct validity as well as a interrater reliability > 0.7. Each pwMCI was asked to rate their overall quality of life, aspects of daily living, memory, mood, energy level, physical condition, concerns about finances, and relationships.
Center for Epidemiologic Studies Depression Scale (CES-D) [27]
PwMCI were asked to complete a 20-item scale to assess the frequency of depressive feelings and behaviors over the past week. The frequency of depressive symptoms (e.g., loneliness, decreased appetite) is rated on a scale ranging from 0 (rarely or none of the time) to 3 (most or almost all the time). CES-D has an adequate factorial validity but low discriminant validity [28].
REACH Anxiety Inventory Form (REACH-anx) [29]
Anxiety symptoms were assessed through the REACH-anx, a 10-item scale modified from the State-Trait Anxiety Inventory questionnaire by the Resources for Enhancing Alzheimer’s Caregiver Health (REACH) project.
Self-efficacy for Managing MCI Scale (Sem-MCI) [30]
PwMCI self-efficacy, with emphasis on memory self-efficacy, was assessed using a modified 9-item version of the chronic disease Self-Efficacy Scales. This modified version included the Do Chores scale, Social/Recreational Activities scale, and 4 of the 5 items in the Manage Disease in General Scale, given their relevance to MCI. Wording on the original form was adapted to represent memory/cognitive difficulties. Sem-MCI has good construct validity and test–retest reliability (ranging from r = 0.55–0.69).
Dementia Rating Scale-2 (DRS-2) [31]
To assess the overall level of cognitive functioning at baseline, pwMCI were administered the DRS-2, a brief cognitive battery that allows for objective assessment of global cognitive functioning in several cognitive domains.
Cogstate [32]
The Cogstate brief battery consists of four tasks: Detection (DET), Identification (IDN), One Card Learning (OCL), and One Back Task (ONB). Detection (DET) is a reaction time task where the participant touches “Yes” when they see the playing card presented on the screen has been turned over. Identification (IDN) is a task of visual attention and reaction time where the participant is shown playing cards and asked to respond to the question, “Is the card red?” One Card Learning (OCL) is a visual attention and learning task. Participants are shown various playing cards and asked to respond to the question, “Have you seen this card before in this task?” The task yields the primary score of accuracy and a secondary score for reaction time. One Back Task (ONB) is a task of working memory. Participants are shown various playing cards and asked to respond to the question, “Is the previous card the same?” Participants have a dichotomous choice of “Yes” or “No” response. This task yields both reaction time and accuracy. A psychomotor/simple attention composite score is derived from IDN and DET speed scores. A learning/working memory composite score is based on OCL and ONB accuracy scores. This computerized assessment is not part of the routine clinical assessment portfolio.
Measure Completed by Both the pwMCI and the Partner About the pwMCI
Clinical Dementia Rating (CDR) [33]
The CDR scale yields a score representative of a stage of dementia, as ascertained through a mental status evaluation of the pwMCI and a clinical interview with care partner. Following the interview, the interviewer rates the severity of cognitive impairment of the pwMCI across 6 dimensions: Memory, Orientation, Judgement and Problem Solving, Community Affairs, Home and Hobbies, and Personal Care. Given their level of functioning in each of these domains, they are assigned a global score generated via algorithm. For the purposes of these analyses, CDR sum of boxes (CDR-SOB) was utilized due to its wider range, which allows for increased sensitivity in tracking more subtle changes both between and within dementia rating stages [34]. This structured interview assessment is not part of the routine clinical assessment portfolio.
Measures completed by the partner about the pwMCI
Functional Assessment Questionnaire (FAQ) [35]
The FAQ is a 10-item informant-based questionnaire that assesses instrumental activities of daily living (IADLs) with high convergent and discriminant validity and an interrater reliability of 0.97. The questionnaire asks care partners to assess pwMCI’s ability to perform instrumental everyday tasks independently in the past 4 weeks. This is a widely used measure for IADLs and has been shown to discriminate between cognitively normal controls and pwMCI [36].
Everyday Cognition (Ecog) [37]
Care partners were asked to complete a 39-item measure that assesses pwMCI’s cognitively mediated impairments in IADLs in several areas, such as memory, language, visuospatial abilities, planning, organization, and divided attention. Ecog has a test–retest reliability of 0.82 and strong convergent and external validity.
Measures Completed by the Partner About Themselves
Center for Epidemiologic Studies Depression Scale (CES-D)
Partners were also asked to complete this scale to assess the frequency of their depressive feelings and behaviors over the past week.
REACH Anxiety Inventory Form (REACH-anx)
Partners’ anxiety symptoms were also assessed through the REACH-anx.
Quality of Life-AD (QoL-AD)
To assess partner perception of their own quality of life as impacted by MCI within their loved one, the partner also completed the QoL-AD. This is a novel application of this instrument.
Partner Self-Efficacy
The Pearlin Mastery Scale [38, 39] was used to assess partners’ own caregiving competence and mastery. The Pearlin scale was designed to assess an individual’s perceived locus of control and coping strategies with a reliability of 0.7[40]. We used only the 7-item Mastery scale, which had partners rate how much they agree or disagree about statements pertaining to themselves, including “feeling in control of life events,” “ability to change important things,” and “feeling helpless about dealing with life’s problems.” Responses include a 4-point Likert scale (1 = strongly disagree; 4 = strongly agree).
Zarit Caregiver Burden Questionnaire, Short Form [41]
To assess the level of caregiver-related stress, care partners completed the short form of the Zarit Caregiver Burden Inventory. This 12-item questionnaire addresses issues such as stress, anger, embarrassment, fear about the future, and financial strain with a test–retest reliability of 0.89 and strong correlation (Pearson’s correlation coefficient: 0.53 to 0.73) with other caregiver well-being measurements.
HABIT®: Study Design and Procedure
Early studies sought to compare one intervention to controls or to a comparative intervention, for example, MSS to CCT [44]. Later studies have used a comparative effective design [45, 46]. Smith and colleagues’ (2017) five-arm comparative effective study sought to compare the effectiveness of the five behavioral interventions that comprise the HABIT® program on the highly valued outcomes in pwMCI. Specifically, the impact of withholding each one of the five interventions in turn was examined. As noted previously, the five components are yoga, computerized cognitive training (CCT), wellness education, support groups, and cognitive rehabilitation with a compensatory memory support system (MSS). Each of these interventions was originally chosen because each was shown to be effective when compared to no treatment controls across a variety of outcomes (e.g., cognitive functioning, QOL, mood, and partner burden) [11,12,13, 47].
As described elsewhere [45], this study used the recruitment, intervention, and evaluation infrastructure of the HABIT program but included more rigorous participant selection criteria. The contribution of each of the 5 components to delivering those patient centered outcomes were assessed and compared. Use of four centers (Mayo Clinic in MN, AZ, and FL as well as University of Washington) enhanced recruitment, scalability of the intervention, and generalization of results. Furthermore, patient and partner advisors encouraged the use of a non-traditional study design. Traditional randomized controlled trials (RCTs) can be thought of as “additive” trials where randomization leads to the addition of treatments beyond placebo or standard-of-care (which may be no treatment). Because potential participants are confronted with a significant probability of receiving no treatment, many decline to participate or withdraw after learning that they will not receive active treatment. In contrast, in this comparative effectiveness trial, randomization was to one of five arms, each of which involved the withholding of one of the five interventions but receiving the other four. That is, this innovative randomization involved suppression of just 1 of the 5 treatment components. Thus, all participants received at least 80% of the menu of interventions offered in this trial. This is referred to as a “subtraction” design, a type of fractional factorial design [48, 49].
In the program, individualized randomization posed significant risk for diffusion of treatment effects, as the group nature of HABIT® permits participants to compare their experiences. Thus, cluster randomization was used, with a cluster defined as one 2-week program. The program was typically offered four times per year at each of 4 sites. Thus, in 16 months, 20 HABIT® programs (5 each at the 4 sites) were randomized. Block randomization was performed at the group level by the principal study statistician; the initial 5 groups of patients and their partners at each site were randomly assigned to one of the 5 arms (withholding of one of the 5 components of HABIT®), with the blocking constraint that each site had at least one (but no more than two) groups/sessions assigned to each of the arms. Study assignments were masked from patients, partners, and clinicians until the first day of that session. The randomization assignment of a group was concealed from participants until the first day of the HABIT® program. Thereafter, blinding of participants was not possible.
All measures were completed at baseline, treatment end, 6 months, and 12 months post intervention. Six-month and 12-month data collection was part of a 1-day booster session that included a refresher for each of the 4 interventions originally provided [45]. Measures that could be completed at a distance were also collected at 18-month follow-up. The schedule was specifically chosen to match follow-up clinical data collection in the full clinical HABIT® program. This permitted the comparison of certain outcomes from the full program to those of the reduced comparative effectiveness program in a pseudo-randomized analyses.
While pairwise differences in group effects on QoL at 12 months were the pre-defined primary outcome of the study, impacts on mood, self-efficacy, and mADLs and partner outcomes at 12 months and functional outcomes at 18 months were also examined. The significance of each pairwise comparison of each outcome was assessed accounting for multiple testing with Westfall stepwise adjustment.
Latent Structure of the Outcome Variables
Subsequent to publishing the planned primary and secondary outcome analysis, how the separate measures might covary were considered. Factor analyses determined what latent constructs might be reflected in the outcome measurements [50]. These analyses initially involved an exploratory factor analysis (EFA) conducted with the comparative effectiveness sample’s baseline data. This analysis revealed that the 13 main measures (excluding Cogstate) used in the HABIT® program are likely tapping 3 main constructs, described as pwMCI impairment level, pwMCI adjustment, and partner adjustment.
Subsequent confirmatory factor analysis was completed with all other data in the HABIT® registry, which is our IRB-approved database for clinical dyads from HABIT® approving use of their clinical data for research and participating in follow-up data collection.. These analyses confirmed that with minor modifications to the factor loadings and accounting for some scale overlap (between the depression and anxiety measures) the factor structure seen in the EFA was a good fit for this validation sample, not only at baseline but post-intervention as well [50]. The final factor model for the post-intervention data is presented in Fig. 2.

Post-intervention confirmatory factor analysis model. Reproduced with permission
HABIT®: Study Results
The results of this major comparative effectiveness study have been reported in a series of manuscripts [51,52,53,54]. Two hundred seventy-two participants were enrolled, seven of whom withdrew consent, and thus, their data was suppressed per IRB requirements. Figures 3, 4, and 5 and Table 1 depict and summarize the trajectories of the various outcomes in the studies organized according to the latent factor structure of the outcome data set described above.

Effect sizes on impacts related to pwMCI adjustment. a Quality of life (QOL), b mood, and c self-efficacy by study arm. Effect sizes were estimated from linear mixed effects regression models where a 1-unit increase in the effect size corresponds to 1 standard deviation (SD) improvement in patient outcome. BL = baseline; EOT = end of treatment. Baseline SDs were 5.59 (QOL), 8.11 (mood), 14.0 (self-efficacy)

Effect sizes by study arm on patient impairment. Effect sizes on were estimated from linear mixed effects regression models, in which a 1-unit increase in the effect size corresponds to a 1 standard deviation (SD) improvement in outcome. a FAQ and b CDR-SOB. Abbreviations: EOT, end of treatment; CCT, computerized cognitive training; MSS, memory support system. Error bars represent 95% confidence intervals for the effect sizes

a Impact of CCT and yoga on psychomotor/visual attention outcome; b Impact of CCT and yoga on learning/working memory outcome
pwMCI adjustment
Figure 3 depicts impacts on pwMCI adjustment. The largest ES for QOL (0.34) was for wellness education to have more impact than CCT (unadjusted p = 0.02). For the mood (CES-D) outcome at 12 months, the largest ES (0.54) again favored wellness education over CCT, (p = 0.01).
pwMCI impairment
Regarding impacts on impairment level for pwMCI, Chandler et al. [51] found, for the Ecog memory measure of mADLs, there was significant benefit of yoga over support group (ES = 0.43, p = 0.04). Shandera et al. [52] subsequently reported comparable findings at the 18-month follow-up for more general functional measures (see Fig. 4). Specifically, functional outcomes as measured by the FAQ and CDR-SOB were benefited when yoga replaced either support group (FAQ ES = 0.53, p = 0.01; CDR-SOB ES = 0.67, p = 0.03) or wellness education (FAQ ES = 0.44, p = 0.03; CDR-SOB ES = 0.67, p = 0.03).
Cognition
Analyses of cognitive outcomes from the program focused on composite psychomotor speed/simple attention and learning/working memory indices from the Cogstate battery (as previously described). Here, study colleagues pursued the specific hypothesis that CCT and yoga would independently, and when combined, provide beneficial impact to processing speed and visual attention at 12-month post-training period in pwMCI. They further hypothesized that the benefit of CCT and yoga as independent and combined interventions would be more evident on processing speed and visual attention outcomes compared to learning and working memory outcomes. They did not anticipate any benefit to cognitive testing outcomes from the other interventions of HABIT (memory support system (mss), wellness education, and support groups). Thus, they partitioned the 5 treatment arms from the comparative effectiveness trial into three arms. One arm included CCT, MSS, wellness, and support groups but not yoga. A second arm included yoga, MSS, wellness education, and support groups but not CCT. The remaining arm pooled the remaining 3 cohorts, which all received yoga and CCT, as well as two other interventions.
As reflected in Fig. 5, arms which included CCT but not yoga were superior to the arm that did not receive CCT [54]. Contrary to the hypothesis, yoga did not independently or in combination with CCT facilitate cognitive function. In fact, when combined with CCT, yoga seemed to weaken the impact of CCT when compared to arms with CCT but not yoga. This led to the speculation that yoga and CCT may have competed with one another in post-program adherence efforts. The target for program participants in cohorts that received CCT was to sustain regular use of the program continuously for at least get to 40 h of total usage (10 h in program and 30 h post-program) to align with prior studies(21). In direct analysis of at-home CCT adherence after the supervised intervention, there was a median of just 3 h of CCT participation post program over the course of 12 months. Nevertheless, total raw time spent on at-home CCT post-intervention was associated with improvement in psychomotor/attention composite (z score = 0.215; 95% CI 0.015 to 0.412, p = 0.035) at 12 months. This boosts confidence that CCT was the “active ingredient” in moderating the rate of decline in processing speed/attention.
Partner Adjustment
Outcomes at 12 months for five partner adjustment outcomes were also examined [53]. Preliminary analyses suggested no group differences within the 5 arms of the comparative effectiveness trial examining these caregiver outcomes. The analyses were then broadened to make use of the robust data available from the full HABIT® clinical sample. Data interpretation when comparing each of the arms in the comparative effectiveness trial to data previously collected in the full HABIT® clinical sample is more direct because the clinical sample received all five interventions. Therefore, differences between any comparative effectiveness arms and the full HABIT® clinical sample are more directly a function of the withholding of the single intervention in that arm.
Table 1 shows the mixed effects models of 12-month outcomes for each arm compared to the full HABIT® clinical sample. It appeared that missing yoga or wellness education produced a statistically significant negative impact on partner anxiety (ES = 0.44 AND 0.55, respectively). Withholding yoga produced a high cost in terms of burden (ES = 0.32) and mood (ES = 0.36), although not statistically significant when adjusting for multiple comparisons. There was no impact on quality of life and self-efficacy when intervention components were withheld (results not shown).
Physical Functioning
Yoga is the single HABIT® intervention expected to impact physical function. The comparative effectiveness study measured physical functioning using the Short Physical Performance Battery (SPPB; [55]) at baseline and at 1-year post-intervention. The impact of receiving yoga or no yoga on change in the SPPB was compared. For pwMCI, there was a general pattern of physical decline regardless of yoga training (yoga vs. no yoga d = 0.06, p = 0.79). However, among care partners, those who received yoga had better physical function at 12 months compared to those who did not (d = 0.39 points, p = 0.041). Thus, participation in yoga had a positive impact on physical performance outcomes at 12-month follow-up for care partners but did not counteract general physical decline in pwMCI.
Integrating/Consolidating/Summarizing Treatment Outcomes
There have been numerous analyses conducted across HABIT® studies. Tables 2 and 3 consolidate information on the impact of the components of HABIT® on a range of outcomes in pwMCI and their care partners.
Treatment Uptake and Adherence: The Importance of Earliest Possible Intervention
The crucial importance of uptake and treatment adherence is well understood in clinical drug trials. A drug that is not absorbed or routinely taken cannot be effective. The same issue attaches to behavioral interventions. PwMCI must be able to demonstrate the capacity to engage the target behaviors and must maintain adherence to these target behaviors overtime. Therefore, it is important to understand the factors associated with treatment uptake and subsequent adherence. Initial analyses of treatment uptake focused particularly on MSS training where approximately 40% of pwMCI reach mastery of the system within the 10-day initial intervention period [56] and the majority of pwMCI at least make it into the final stage of training. Baseline cognitive impairment as measured by the Dementia Rating Scale (DRS) predicts treatment uptake (p < 0.001). Additionally, aspects of personality, namely, openness in both the pwMCI and the partner associate with MSS treatment uptake [57]. Further analyses reveal that beyond global cognitive functioning, greater integrity of both declarative and aspects of procedural memory associate with better MSS learning efficiency [58]. In turn treatment uptake predicts adherence to the MSS at 18-month follow-up (p = 0.008) [56].
In general, adherence to behavioral-lifestyle interventions like HABIT® may be even more effortful than medication compliance. Relative to adherence to a single intervention like MSS, adherence to a full multicomponent program may be even more challenging. In the comparative effectiveness trial, the ideal was that participants would adhere to four interventions in an ongoing manner after the treatment program. However, the median number of interventions (out of 4) adhered to was 2 at 6- and 12-month follow-up and 1.5 (credit given for partial adherence) at 18 months [59]. Baseline DRS was again a significant predictor of 12-month adherence (ß = 0.16, p = 0.02). Adherence level was associated again with functional outcomes (as measured by the FAQ) at 6 (ß = − 0.14, p = 0.03) and 12 months (ß = − 0.29, p = 0.001) [59]. These findings, though relevant only to the interventions included in the HABIT program, perhaps lend support to the importance of early intervention for individuals with cognitive impairment. They also provide an example of both the challenges and importance of adherence in behavioral interventions.
Conclusion
Note that in the trials described here, it was common for most treatment groups to demonstrate evidence of within-group improvement on most outcome measures by treatment end. For example, in the large comparative effectiveness trial, all combinations of interventions led to reported improvements in QOL at treatment end. However, these within-group findings must be interpreted cautiously as there was no untreated active control group by which to account for the mere passage of time and provision of attention in this comparative effectiveness study. Still, spontaneous improvement in MCI samples has not been observed in previous work with no treatment controls, who showed deterioration of functional status over 6 months of follow-up [23].
There was evidence of differences in study arms with respect to mood at 12 months. Namely, those who had all program components except wellness education had worsened mood, while those who did not have computerized cognitive training had improved mood. Thus, not receiving wellness education appears to be more detrimental to mood by 12 months post-intervention than the other interventions. Conversely, it is possible that participating in computerized cognitive training may be detrimental to long-term mood outcome.
Replacing yoga with either support group or wellness education led to the poorest results on measures of daily function. Similarly, withholding yoga came at a cost to burden and mood outcomes for care partners, while withholding wellness education or yoga was detrimental to care partner anxiety. Collectively these findings generally align with prior research suggesting the importance of physical exercise to functional outcomes for patients and some caregiver outcomes while wellness education is important to other caregiver outcomes.
Taken together, the HABIT® studies reviewed herein have advanced knowledge relevant to behavioral intervention research in MCI due to ADRD in several ways through (1) identification of which outcomes are most important to patients and their partners, (2) use of novel study designs that allow analysis of a multi-component intervention while assuring all participants receive some form of intervention, (3) delineation of the latent constructs measured by a broad battery of commonly used outcome measures, (4) provision of valuable data on trajectories of these outcome measures for pwMCI and partners, and (5) empirical findings for the expectable observation that the different behavioral interventions in a multicomponent program have differential impacts on different outcome measures (see Tables 2 and 3). This constellation of findings provides preliminary support for the notion that knowledge-based interventions like wellness education may be more impactful on patient and partner well-being (e.g., QoL and mood), while active engagement in skill-based interventions like yoga and compensation-based calendar training (the MSS) is necessary to assist with the maintenance of functional status.
While the studies reviewed here all used components of the Mayo Clinic’s HABIT® versions of these interventions, similar behavioral interventions (e.g., therapy-based cognitive rehabilitation, CCT programs, physical exercise, psychotherapy/group therapy, and education programs for memory loss) are being offered in various combinations in medical and research centers around the world [12]. The conclusions may not generalize to other forms of the behavioral intervention (e.g., resistance training or walking versus yoga), but these results add to the rapidly accumulating corpus of information that suggests these multicomponent behavioral interventions are efficacious and effective in impacting the trajectory of MCI due to ADRD. In spite of this rapid accumulation of empirical support, additional research is clearly needed to improve our understanding of “active ingredients” and “optimal doses” for these behavioral interventions pertinent to various valued outcomes in MCI.
Limitations
This research program suffers from various limitations. Unfortunately, the cohorts recruited are not racially or ethnically diverse and are highly educated. This limits potential generalizability of the results. There have been increased efforts to diversify the cohorts through growing community engagement efforts with dedicated and trained staff. Notably, there have been recent efforts in adapting components of HABIT® (i.e., MSS) for linguistically diverse participants with subjective cognitive impairment [60]. Nevertheless, these samples are likely biased in at least two additional ways. First, the cohorts by default are comprised of people that pursue active coping approaches to manage chronic illnesses like MCI. Additionally, the program requires participants and partners to dedicate 40–50 h over 2 weeks to the program, including daily travel to and from the program, or in some cases requiring self-funded hotel stays. This biases the samples to higher SES. In fact, time and distance were primary reasons that eligible candidates cited for not enrolling in this type of intervention [44]. There have been efforts to reduce the financial and time burden of the program through developing and trialing a telehealth HABIT clinical program.
Many of the studies reported herein have a comparative effectiveness design. Interpretation of results from this type of design is a challenge compared to traditional placebo-controlled studies. In an attempt to simplify the explanation of the results, pairwise comparisons of multiple component interventions were used that differed in which single intervention was withheld. This approach assumes negligible interaction between interventions. It is probable, however, that there are synergies between various interventions in the program, and that a single intervention delivered alone would produce similar results. Next, although the sample size in the main trial was large relative to other behavioral intervention trials in MCI, the trial was only powered to detect within group change over time. It was underpowered to detect pairwise differences between arms of the study. This means that the significant findings observed are likely to be reliable, but other important impacts may not have reached statistical significance. Awareness of this limitation led to the report of effect sizes as well as statistical significance. However, it was noted that comparative effectiveness trials will generate smaller effect sizes than placebo-controlled studies, and treatments are compared to either other rather than to no treatment at all [61].
References
Smith G, Petersen R, Parisi J, Ivnik R, Kokmen E, Tangalos E, et al. Definition, course and outcome of mild cognitive impairment. Aging Neuropsychol Cogn. 1996;3:141–7.
Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Mild cognitive impairment: clinical characterization and outcome. Arch Neurol. 1999;56(3):303–8.
Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270–9.
As A. Alzheimer’s disease facts and figures. Alzheimer’s dement. 2017;13:325–73.
Alexander GC, Knopman DS, Emerson SS, Ovbiagele B, Kryscio RJ, Perlmutter JS, et al. Revisiting FDA Approval of Aducanumab. N Engl J Med. 2021;385(9):769–71.
Richardson TJ, Lee SJ, Berg-Weger M, Grossberg GT. Caregiver health: health of caregivers of Alzheimer’s and other dementia patients. Curr Psychiatry Rep. 2013;15(7):367.
Mittelman M, Ferris S, Steinberg G, Shulman E, Mackell J, Ambinder A, et al. An intervention that delays institutionalization of Alzheimer’s disease patients: treatment of spouse-caregivers. Gerontologist. 1993;33(6):730–40.
Ngandu T, Lehtisalo J, Solomon A, Levalahti E, Ahtiluoto S, Antikainen R, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015;385(9984):2255–63.
Schmitter-Edgecombe M, Dyck DG. Cognitive rehabilitation multi-family group intervention for individuals with mild cognitive impairment and their care-partners. J Int Neuropsychol Soc. 2014;20(9):897–908.
National Academies of Sciences EaM. In: Downey A, Stroud C, Landis S, Leshner AI, editors. Preventing cognitive decline and dementia: a way forward. Washington (DC): The National Academies Press; 2017.
Sherman DS, Mauser J, Nuno M, Sherzai D. The efficacy of cognitive intervention in mild cognitive impairment (MCI): a meta-analysis of outcomes on neuropsychological measures. Neuropsychol Rev. 2017;27(4):440–84.
Chandler MJ, Parks AC, Marsiske M, Rotblatt LJ, Smith GE. Everyday impact of cognitive interventions in mild cognitive impairment: a systematic review and meta-analysis. Neuropsychol Rev. 2016;26(3):225–51.
Northey JM, Cherbuin N, Pumpa KL, Smee DJ, Rattray B. Exercise interventions for cognitive function in adults older than 50: a systematic review with meta-analysis. Br J Sports Med. 2018;52(3):154–60.
Smith GE, Okonkwo OC. Truly Cross-fit: The association of exercise and clinical outcomes: introduction to a JINS Special Section. J Int Neuropsychol Soc. 2021;27(8):757–60.
Cummings JL, Morstorf T, Zhong K. Alzheimer’s disease drug-development pipeline: few candidates, frequent failures. Alzheimers Res Ther. 2014;6(4):37.
Chandler MJ, Locke DEC, Duncan NL, Hanna SM, Cuc AV, Fields JA, et al. Computer versus compensatory calendar training in individuals with mild cognitive impairment: functional impact in a pilot study. Brain Sci. 2017;7(9).
Greenaway MC, Duncan NL, Smith GE. The memory support system for mild cognitive impairment: randomized trial of a cognitive rehabilitation intervention. Int J Geriatr Psychiatry. 2013;28(4):402–9.
Cuc AV, Locke DEC, Duncan N, Fields JA, Snyder CH, Hanna S, et al. A pilot randomized trial of two cognitive rehabilitation interventions for mild cognitive impairment: caregiver outcomes. Int J Geriatr Psychiatry. 2017;32(12):e180–7.
Squire LR. Memory and brain systems: 1969–2009. J Neurosci. 2009;29(41):12711–6.
De Wit L, Marsiske M, O’Shea D, Kessels RPC, Kurasz AM, DeFeis B, et al. Procedural Learning in individuals with amnestic mild cognitive impairment and Alzheimer’s dementia: a systematic review and meta-analysis. Neuropsychol Rev. 2021;31(1):103–14.
Smith GE, Housen P, Yaffe K, Ruff R, Kennison RF, Mahncke HW, et al. A cognitive training program based on principles of brain plasticity: results from the Improvement in Memory with Plasticity-based Adaptive Cognitive Training (IMPACT) study. J Am Geriatr Soc. 2009;57(4):594–603.
Zelinski EM, Spina LM, Yaffe K, Ruff R, Kennison RF, Mahncke HW, et al. Improvement in memory with plasticity-based adaptive cognitive training: results of the 3-month follow-up. J Am Geriatr Soc. 2011;59(2):258–65.
Greenaway MC, Hanna SM, Lepore SW, Smith GE. A behavioral rehabilitation intervention for amnestic mild cognitive impairment. Am J Alzheimers Dis Other Demen. 2008;23(5):451–61.
Sohlberg MM, Mateer CA. Training use of compensatory memory books: a three stage behavioral approach. J Clin Exp Neuropsychol. 1989;11(6):871–91.
Logsdon RG, Gibbons LE, McCurry SM, Teri L. Assessing quality of life in older adults with cognitive impairment. Psychosom Med. 2002;64(3):510–9.
Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401.
Orme JG, Reis J, Herz EJ. Factorial and discriminant validity of the Center for Epidemiological Studies Depression (CES-D) scale. J Clin Psychol. 1986;42(1):28–33.
Wisniewski SR, Belle SH, Coon DW, Marcus SM, Ory MG, Burgio LD, et al. The Resources for Enhancing Alzheimer’s Caregiver Health (REACH): project design and baseline characteristics. Psychol Aging. 2003;18(3):375–84.
Kurasz AM, DeFeis B, Locke DEC, De Wit L, Amofa P, Smith G, et al. Psychometric properties of the self-efficacy for managing mild cognitive impairment scale. Int J Geriatr Psychiatry. 2021;36(1):174–81.
Jurica PJ LC, Mattis S Dementia Rating Scale-2: Professional manual. 2001.
Farias S Tomaszewski, Mungas D, Reed B, Cahn-Weiner D, Jagust W, Baynes K, et al. The measurement of everyday cognition (ECog): Scale development and psychometric properties. Neuropsychology. 2008;22:531–544.
Maruff P, Lim YY, Darby D, Ellis KA, Pietrzak RH, Snyder PJ, et al. Clinical utility of the cogstate brief battery in identifying cognitive impairment in mild cognitive impairment and Alzheimer’s disease. BMC Psychol. 2013;1(1):30.
Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology. 1993;43(11):2412–4.
O’Bryant SE, Lacritz LH, Hall J, Waring SC, Chan W, Khodr ZG, et al. Validation of the new interpretive guidelines for the clinical dementia rating scale sum of boxes score in the national Alzheimer’s coordinating center database. Arch Neurol. 2010;67(6):746–9.
Pfeffer RI, Kurosaki TT, Harrah CH Jr, Chance JM, Filos S. Measurement of functional activities in older adults in the community. J Gerontol. 1982;37(3):323–9.
Teng E, Becker BW, Woo E, Knopman DS, Cummings JL, Lu PH. Utility of the functional activities questionnaire for distinguishing mild cognitive impairment from very mild Alzheimer disease. Alzheimer Dis Assoc Disord. 2010;24(4):348–53.
Farias ST, Mungas D, Reed BR, Cahn-Weiner D, Jagust W, Baynes K, et al. The measurement of everyday cognition (ECog): scale development and psychometric properties. Neuropsychology. 2008;22(4):531–44.
Pearlin LI, Mullan JT, Semple SJ, Skaff MM. Caregiving and the stress process: an overview of concepts and their measures. Gerontologist. 1990;30(5):583–94.
Pearlin LI, Schooler C. The structure of coping. J Health Soc Behav. 1978;19(1):2–21.
Eklund M, Erlandsson LK, Hagell P. Psychometric properties of a Swedish version of the Pearlin Mastery Scale in people with mental illness and healthy people. Nord J Psychiatry. 2012;66(6):380–8.
Bedard M, Molloy DW, Squire L, Dubois S, Lever JA, O’Donnell M. The Zarit Burden Interview: a new short version and screening version. Gerontologist. 2001;41(5):652–7.
Barrios PG, Gonzalez RP, Hanna SM, Lunde AM, Fields JA, Locke DE, et al. Priority of treatment outcomes for caregivers and patients with mild cognitive impairment: preliminary analyses. Neurol Ther. 2016;5(2):183–92.
Smith GE, Chandler M, Fields JA, Aakre J, Locke DEC. A survey of patient and partner outcome and treatment preferences in mild cognitive impairment. J Alzheimers Dis. 2018;63(4):1459–68.
Locke DE, Greenaway MC, Duncan N, Fields JA, Cuc AV, Snyder CH, et al. A patient-centered analysis of enrollment and retention in a randomized behavioral trial of two cognitive rehabilitation interventions for Mild Cognitive Impairment. J Prev Alzheimers Dis. 2014;1(3):143–50.
Smith G, Chandler M, Locke DE, Fields J, Phatak V, Crook J, et al. Behavioral interventions to prevent or delay dementia: protocol for a randomized comparative effectiveness study. JMIR Res Protoc. 2017;6(11):e223.
De Wit L, O’Shea D, Chandler M, Bhaskar T, Tanner J, Vemuri P, et al. Physical exercise and cognitive engagement outcomes for mild neurocognitive disorder: a group-randomized pilot trial. Trials. 2018;19(1):573.
Rodakowski J, Saghafi E, Butters MA, Skidmore ER. Non-pharmacological interventions for adults with mild cognitive impairment and early stage dementia: an updated scoping review. Mol Aspects Med. 2015;43–44:38–53.
Collins LM, Dziak JJ, Kugler KC, Trail JB. Factorial experiments: efficient tools for evaluation of intervention components. Am J Prev Med. 2014;47(4):498–504.
Chakraborty B, Collins LM, Strecher VJ, Murphy SA. Developing multicomponent interventions using fractional factorial designs. Stat Med. 2009;28(21):2687–708.
DeFeis B, Ying G, Kurasz AM, De Wit L, Amofa P, Chandler M, et al. Latent Factor Structure of Outcome Measures Used in the HABIT(R) Mild Cognitive Impairment Intervention Programs. J Alzheimers Dis. 2021.
Chandler MJ, Locke DE, Crook JE, Fields JA, Ball CT, Phatak VS, et al. Comparative effectiveness of behavioral interventions on quality of life for older adults with mild cognitive impairment: a randomized clinical trial. JAMA Netw Open. 2019;2(5):e193016.
Shandera-Ochsner AL, Chandler MJ, Locke DE, Ball CT, Crook JE, Phatak VS, et al. Comparative effects of physical exercise and other behavioral interventions on functional status outcomes in mild cognitive impairment. J Int Neuropsychol Soc. 2021:1–8.
Amofa PA, Locke DEC, Chandler M, Crook JE, Ball CT, Phatak V, et al. Comparative effectiveness of behavioral interventions to prevent or delay dementia: one-year partner outcomes. J Prev Alzheimers Dis. 2021;8(1):33–40.
Phatak VS, Smith GE, Locke D, Shandera-Ochsner A, Dean PM, Ball C, et al. Computerized Cognitive Training (CCT) versus Yoga Impact on 12 Month Post Intervention Cognitive Outcome in Individuals with Mild Cognitive Impairment. Brain Sci. 2021;11(8).
Chandler M, Locke DE, Thomas CS, Crook JE, Graff‐Radford M, Lucas PH, et al. Yoga training impacts physical function 12 months post intervention for care partners of those with mild cognitive impairment: dementia care research: Behavioral interventions. Alzheimer's & Dementia. 2020;16:e045418.
De Wit L, Chandler M, Amofa P, DeFeis B, Mejia A, O’Shea D, et al. Memory support system training in mild cognitive impairment: predictors of learning and adherence. Neuropsychol Rehabil. 2021;31(1):92–104.
Khayoun R, Devick KL, Chandler MJ, Shandera-Ochsner AL, De Wit L, Cuc A, et al. The impact of patient and partner personality traits on learning success for a cognitive rehabilitation intervention for patients with MCI. Neuropsychol Rehabil. 2021:1–13.
De Wit L, Levy S, Kurasz AM, Amofa P, DeFeis B, O’Shea DM, Chandler MJ, Smith GE. Procedural Learning, declarative learning, and working memory as predictors of learning the use of a memory compensation tool in persons with amnestic mild cognitive impairment. Journal of the International Neuropsychological Society. 2022.
Sr PAA, DeFeis B, De Wit L, O'Shea D, Mejia A, Chandler M, et al. Functional ability is associated with higher adherence to behavioral interventions in mild cognitive impairment. Clin Neuropsychol. 2019:1–19.
Santos OA, Rios-Rosales A, Pedraza O, Bergeron CD, Chandler M. Memory support system in spanish: a pilot study. Brain Sci. 2021;11(11).
Sox HC, Goodman SN. The methods of comparative effectiveness research. Annu Rev Public Health. 2012;33:425–45.
Acknowledgements
Research reported in this manuscript was partially funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (CER-1306-01897). The statements in this publication are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee. Trial Registration: ClinicalTrials.gov Identifier, NCT02265757, and peace of mind studies.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The Mayo Clinic and the University of Florida offer the HABIT® program as a clinical service, billing for and collecting revenues from this program. While several of the authors are salaried employees of one of these organizations, none of the study authors or PIs receives direct, financial benefit from this service. Furthermore, none of the authors holds equity in or benefit financially from the vendors of the products used in the HABIT program.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Levy, SA., Smith, G., De Wit, L. et al. Behavioral Interventions in Mild Cognitive Impairment (MCI): Lessons from a Multicomponent Program. Neurotherapeutics 19, 117–131 (2022). https://doi.org/10.1007/s13311-022-01225-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13311-022-01225-8