
Abstract
Introduction
Cardiovascular disease (CVD) is the leading cause of death in Chinese adults with type 2 diabetes (T2D), and treatment guidelines have increasingly focused on the comprehensive management of T2D and CVD. Here, we report data from the Chinese population within the CAPTURE study, including CVD prevalence in patients with T2D and insights into their management.
Methods
CAPTURE (a multinational, non-interventional, cross-sectional study in adults with T2D) included data from eight centers in China from July to September 2019. Overall CVD prevalence estimates were calculated, and descriptive data regarding CVD subtypes and treatment were collected and reported here.
Results
Of 805 adults with T2D enrolled in China (61.9% male, median age 59 years), 273 had established CVD, with an estimated prevalence (95% CI) of 33.9% (30.6%, 37.3%). Most CVD cases were atherosclerotic (94.9%). Coronary heart disease had the highest estimated prevalence (16.0%), followed by carotid artery disease (9.6%) and cerebrovascular disease (7.7%). Use of glucose-lowering agents (GLAs) with proven cardiovascular benefits (glucagon-like peptide-1 receptor agonists and/or sodium-glucose cotransporter-2 inhibitors) was low in the China sample (7.7%). Approximately half of the CVD subgroup in the China sample was receiving cardiovascular medication, but use of guideline-directed agents was low (e.g., statins: 35.9%; angiotensin II receptor blockers: 15%; angiotensin-converting enzyme inhibitors: 2.6%).
Conclusions
In the Chinese CAPTURE population, one-third of patients had established CVD, with atherosclerotic CVD largely accounting for the CVD burden; use of GLAs with proven cardiovascular benefits and cardiovascular medications was low, suggesting an unmet need for optimal management in this group.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
Cardiovascular disease (CVD) is the leading cause of death in adults with type 2 diabetes (T2D) in China |
This study reports contemporary CVD prevalence data from the Chinese sites of the CAPTURE study and provides insights into how patients with T2D and CVD are being managed in China |
What was learned from the study? |
One-third of patients with T2D in China within the secondary care (diabetology setting) had established CVD, with atherosclerotic CVD largely accounting for CVD burden |
Use of glucose-lowering agents with proven cardiovascular benefits and cardiovascular medications was low in the Chinese CAPTURE population in 2019, suggesting an unmet need for optimal management in this group |
Introduction
Cardiovascular disease (CVD) is the leading cause of death in China and is responsible for 40% of deaths in the Chinese population [1]. Individuals with diabetes have an approximately two-fold increased risk of CVD compared with individuals without diabetes [2, 3]. With the latest data for mainland China showing an increasing prevalence over time (12.8% in 2017 compared with 11.6% in 2010) [4, 5], diabetes is recognized as an important determinant in the prevention of CVD [1]. China has the largest number of adults with diabetes worldwide, and figures are predicted to rise from 116.4 million in 2019 to 147.2 million by 2045 [6].
Among people with type 2 diabetes (T2D), CVD is reported to account for approximately half of all deaths [7]. Hence, diabetes treatment guidelines have increasingly focused on the comprehensive management of T2D and CVD, and many regulatory agencies require that diabetes medications demonstrate cardiovascular (CV) safety (or even benefits in terms of CV risk reduction), especially for major adverse CV events [8,9,10]. A number of newer blood glucose-lowering agents (GLAs), including glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and sodium-glucose co-transporter-2 (SGLT2) inhibitors, have demonstrated superiority versus placebo in CV outcomes trials (CVOTs) in individuals with T2D and established CVD or high CV risk (e.g., the LEADER and EMPA-REG OUTCOMES trials) [11, 12]. Thus, international guidelines now recommend the GLAs with evidence of CV risk reduction as first- or second-line treatment in this population [8,9,10]. Although specific guidelines focused on co-management of patients with both T2D and CVD are lacking in China, there is consensus regarding the CV benefits of these GLAs, based on the results of CVOTs, from the Chinese Diabetes Society and Chinese Society of Endocrinology [13, 14].
A systematic literature review exploring the prevalence of CVD worldwide among adults with T2D has reported that CVD affects approximately 32.2% of all persons with T2D and 28.4% of adults with T2D in China [7]. However, there is a paucity of representative cross-sectional data estimating the prevalence of CVD in patients with T2D using standardized methodology, particularly following the introduction of GLAs with proven CV risk reductions. It is important to identify current prevalence figures based on the data of daily clinical practice and understand how the patients are being managed. The CAPTURE study estimated the contemporary prevalence of established CVD and its management in adults with T2D across 13 countries from five continents using standardized methodology [15]. Here, we report prevalence results from the Chinese sites of the CAPTURE study and provide insights into how patients with T2D and CVD are being managed in China.
Methods
The study design of CAPTURE, a non-interventional, cross-sectional study conducted at 214 centers across 13 countries, was described previously [15]. Eight centers were in China. The present analysis focuses on the study data in China.
The study was approved by all participating institutions, registered with ClinicalTrials.gov (NCT03786406 and NCT03811288) and conducted in accordance with the Declaration of Helsinki [16], Guidelines for Good Pharmacoepidemiology Practices issued by International Society for Pharmacoepidemiology [17] and Chinese regulations for clinical research. The study protocol was approved by the Ethics Committee of Peking University Third Hospital and other appropriate clinical research ethics committees in each participating site in China and relevant institutional review boards at each site (Electronic Supplementary Material [ESM] Table 1). Informed consent was obtained prior to study participation.
Site Selection
Information on the management of people with T2D in China was obtained from sponsor-employed local medical affairs personnel. The information, which included the types of physicians (endocrinologists or diabetologists) managing T2D in routine clinical practice and types of practices, was used to inform which sites could be considered as representative. Since individuals with T2D in China do not consult primary care practitioners as their initial contact and are primarily managed in specialist care, only secondary care sites were selected.
Participants
Consecutive adults aged ≥ 18 years at the time of informed consent and with a diagnosis of T2D ≥ 180 days prior to providing informed consent were invited to participate by their managing physician, within a 90-day time period (from July to September 2019) at each participating site. Exclusion criteria were: prior participation in this study (to prevent patients being included more than once); a diagnosis of type 1 diabetes; mental incapacity, unwillingness or language barriers precluding an adequate understanding of, or cooperation with, study requirements; or known congenital heart disease or malformation.
Objectives and Endpoints of the Study
The primary objective was to assess the prevalence of CVD in adults with T2D in China using a standardized methodology. Patients were considered to have established CVD if any of the following conditions were recorded: coronary heart disease (CHD), carotid artery disease, cerebrovascular disease, cardiac arrhythmia, peripheral artery disease, heart failure or aortic disease. The definitions of these conditions are provided in the ESM Methods.
Data Collection
The study was based on primary collection of data from patients’ medical records by physicians or an appropriately qualified and trained delegate. The following data were collected: demographic, anthropometric and clinical parameters, selected medical history, GLAs and CV medications. Only current medications (or those discontinued within ≤ 3 months) were recorded. GLAs were further classified according to demonstrated CV benefit in CVOTs and based on the 2020 American Diabetes Association guidelines, in which the GLAs with CV benefit included three GLP-1 RAs (dulaglutide, liraglutide and semaglutide) and three SGLT2 inhibitors (canagliflozin, dapagliflozin and empagliflozin) [8].
Statistical Analysis
The prevalence (95% confidence interval [CI]) of CVD, atherosclerotic cardiovascular disease (ASCVD) and CVD subtypes and diagnoses were calculated. Due to the descriptive nature of this study, P values were not calculated to assess the statistical significance of any differences. Descriptive data for the study sample characteristics were not weighted and are presented for the overall China study sample and stratified according to CVD.
For secondary analysis, patients were stratified according to the presence or absence of established CVD. The CVD was further classified as ASCVD if there was a diagnosis of CHD, carotid artery disease, cerebrovascular disease or peripheral artery disease [9]. Furthermore, the use of CV medications in patients with T2D and CVD across 12 countries (excluding China) and in China was analyzed.
Results
Study Population
There were a total of 805 adults with T2D enrolled across eight sites in the CAPTURE study in China. The average number of patients per site was 101 (range: 20–160). Among the study sample in China, 38.1% were female and median (interquartile range [IQR]) age was 59 (51–67) years. The median (IQR) diabetes duration was 9.2 (4.2–14.4) years and glycated hemoglobin (HbA1c) was 7.3% (6.4–8.5%). Median (IQR) body mass index was 24.5 (22.6–26.7) kg/m2 and 49.3% had diagnosed hypertension (Table 1).
CVD Prevalence
Among patients in the China study sample, 273 had established CVD, and the estimated prevalence (95% CI) was 33.9% (30.6%, 37.3%). Most cases of CVD in the China sample were ASCVD (94.9%), and its estimated prevalence (95% CI) was 32.2% (29.0%, 35.5%) (Table 2).
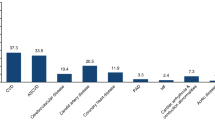
The CVD subtypes with the highest estimated prevalence in the China sample were CHD, carotid artery disease and cerebrovascular disease (16.0%, 9.6% and 7.7%, respectively) (Table 2). Within these three subtypes, the highest estimates by diagnosis were stable coronary artery disease (13.4%), carotid artery disease (9.6%) and ischemic stroke (5.5%) (Fig. 1). Two CVD subtypes had a low estimated prevalence of 0.2%, namely heart failure and aortic disease (Table 2).

Prevalence of CVD in people with T2D by CVD subtype and diagnoses in China in 2019. Data are overall prevalence estimates (95% CI). Diagnoses are not mutually exclusive, and one participant may have multiple diagnoses. †Categorized as ASCVD. ‡Included conduction abnormalities. ASCVD atherosclerotic cardiovascular disease, AV atrioventricular, CHD coronary heart disease, CI confidence interval, CVD cardiovascular disease, PAD peripheral artery disease, SND sinus node dysfunction, T2D type 2 diabetes
Characteristics of the Study Population Stratified by CVD Status
Analysis of demographic and clinical characteristics of the China study sample according to CVD status revealed that both the CVD and ASCVD subgroups versus the non-CVD subgroup appeared to be older (median age: 64 years and 64 years vs. 57 years, respectively), with more females (43.6% and 43.2% vs. 35.3%), higher HbA1c (7.7% and 7.7% vs. 7.0%) and triglyceride levels (1.52 mmol/L and 1.52 mmol/L vs. 1.34 mmol/L) and a longer duration of diabetes (median duration: 11.2 years and 11.2 years vs. 7.3 years) (Table 1; not statistically analyzed).
The proportions of participants in both the CVD and ASCVD subgroups, compared with the non-CVD subgroup, appeared to be different in terms of diagnosed hypertension (69.1% and 69.7% vs. 38.9%, respectively), familial hypercholesterolemia (6.4% and 6.4% vs. 5.0%), retinopathy (23.3% and 24.1% vs. 9.4%), nephropathy (14.7% and 14.7% vs. 7.3%) and neuropathy (41.5% and 41.6% vs. 12.8%), although no statistical testing was completed on these proportions. Furthermore, differences also appeared in both the CVD and ASCVD subgroups versus the non-CVD subgroup for markers of renal dysfunction (microalbuminuria: 34.5% and 34.8% vs. 26.5%; macroalbuminuria: 9.7% and 10.1% vs. 8.4%; eGFR ≤ 59 mL/min/1.73 m2: 16.8% and 16.5% vs. 4.0%) and reported low physical activity (0–1 day of physical activity per week: 23.9% and 24.5% vs. 16.8%) (Table 1; not statistically analyzed).
Use of GLAs with Proven CV Benefit
Among patients in the China study sample, 779 (96.8%) were receiving any type of GLA. The proportion of patients using any oral antidiabetic drug seemed similar among the CVD, ASCVD and non-CVD subgroups in the CAPTURE China study population (89.0%, 89.2% and 88.3%, respectively; not statistically analyzed), although differences appeared in the type of oral antidiabetic drug being used. For example, biguanide (metformin) use in the CVD and ASCVD subgroups was 56.0% and 57.1%, respectively, while it was 66.9% in the non-CVD subgroup. In contrast, use of alpha glucosidase inhibitors was 52.4% and 52.5% for the CVD and ASCVD subgroups, but 35.0% for the non-CVD subgroup. Similarly, insulin was used by approximately half of the CVD and ASCVD subgroups (55.3% and 56.4%, respectively), but by under a third of the non-CVD subgroup (30.5%) (ESM Table 2).
In the China study sample, use of any GLA with proven CV benefit (GLP-1 RA and/or SGLT2 inhibitor: 6.2% and 5.8% vs. 8.5%) and use of GLP-1 RA (1.5% and 1.5% vs. 5.1%) appeared to be somewhat lower in the CVD and ASCVD subgroups than the non-CVD subgroup, while use of SGLT2 inhibitor seemed comparable among the CVD, ASCVD and non-CVD subgroups (5.9% and 5.4% vs. 5.1%) (Fig. 2; not statistically analyzed). Compared with the overall multinational study population, the use of GLAs with proven CV benefit was lower in the overall China study sample (7.7% vs. 21.9% for GLP-1 RA and/or SGLT2 inhibitor) [15].

Use of GLAs with proven CV risk reduction in the CAPTURE population stratified by CVD status in China in 2019. Data are proportion of participants using a GLA with proven CV risk reduction per ADA guidelines (GLP-1 RAs: dulaglutide, liraglutide and semaglutide; SGLT2 inhibitors: canagliflozin, dapagliflozin and empagliflozin). ADA American Diabetes Association, ASCVD atherosclerotic cardiovascular disease, CV cardiovascular, CVD cardiovascular disease, GLA glucose-lowering agent, GLP-1 RA glucagon-like peptide-1 receptor agonist, SGLT2 sodium-glucose co-transporter-2
Use of CV Medications
A total of 32.3% patients of the overall study sample from China were receiving a CV medication, with use being more common among the CVD and ASCVD subgroups than the non-CVD subgroup (55.3% and 58.3% vs. 20.5%). The most frequently used CV medications in the CVD, ASCVD and non-CVD subgroups were statins (35.9%, 37.8% and 13.5%) followed by acetylsalicylic acid (24.9%, 26.3% and 6.2%) (ESM Table 3). Compared with the multinational population (excluding China), there was less use of guideline-directed agents in patients with T2D and CVD in China, including statins (35.9% vs. 66.5%), angiotensin-converting enzyme inhibitors (2.6% vs. 28.3%), angiotensin II receptor blockers (15.0% vs. 37.7%) and platelet-aggregation inhibitors (34.4% vs. 59.0%) (ESM Table 4; not statistically analyzed).
Discussion
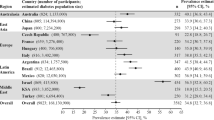
The CAPTURE study estimated the prevalence of CVD in patients with T2D who were enrolled from routine clinical practice in 13 selected countries in 2019. The results for China showed an overall estimated prevalence of 33.9% for CVD and 32.2% for ASCVD, which was comparable to the overall prevalence based on data pooled from all 13 countries of 34.8% and 31.8%, respectively [15].
Among patients with T2D in the CAPTURE China population, ASCVD accounted for a large proportion of the CVD burden (similar to the multinational study sample) [15], the leading causes of which were stable coronary artery disease, carotid artery disease and stroke. There was a low prevalence of heart failure in this study compared with a systematic literature review that included five studies from China with 39,934 patients and reported a prevalence of congestive heart failure of 4.3% [7]. Furthermore, the prevalence of heart failure in the CAPTURE China sample was lower than in the multinational study sample (0.2% vs. 2.4%) [15]. This low prevalence of heart failure may not reflect the real picture in China, as all the investigators in Chinese sites were endocrinologists. In other words, cardiologists, who were more likely to manage patients with established heart failure than an endocrinologist in China, were not included in this study.
The findings of the current study demonstrate a higher prevalence of CVD (33.9%) among patients with T2D than the above-mentioned systematic literature review (28.4%) [7], but the current results are comparable to those of a cross-sectional hospital-based study conducted in four major Chinese cities that reported a CVD prevalence of 30.1% [18]. Nonetheless, differences in the study design used to collect CVD prevalence data (e.g., site and participant selection, timing and definition of CVD) can make it difficult to compare the results between studies. In the CAPTURE study, the standardized approach used to collect CVD prevalence data would enable the direct comparison of data relating to the CVD burden between regions and countries.
The triglyceride level appeared higher in the CVD and ASCVD subgroups than in the non-CVD subgroup (not statistically analyzed), which indicated that it might be a risk factor for CVD in adults with T2D in this Chinese study population. Similarly, triglyceride level has been shown as a potential risk factor for CHD in Japanese patients with T2D, which is comparable to low-density lipoprotein cholesterol [19].
The prevalence of cerebrovascular disease in the current study (7.7%) is in contrast to a study that reported an age-standardized prevalence of 1.79% for stroke in 219,522 Chinese patients with T2D [20]. The lower prevalence in the latter study could be attributed to the use of data from the China National HbA1c Surveillance System in 2012 compared with CAPTURE data collection in 2019. Furthermore, the prevalence of 1.79% did not include transient ischemic attack or unspecified stroke. A different study, which included 4629 patients with T2D in China, found a slightly higher prevalence of 5.5% for stroke [21]. It is important to note that in the clinic in China, stroke may be considered a result of carotid artery disease as well as cerebrovascular disease, since the former is considered a major cause of stroke. This could explain the higher estimates of both carotid artery disease and cerebrovascular disease in the China study sample compared with the multinational sample [15].
Based on evidence from CVOTs, international guidelines now recommend measures (including use of GLAs with demonstrated CV risk reduction as first- or second-line GLA) to reduce the burden of ASCVD, a largely preventable disease [8,9,10]. Indeed, targeting ASCVD is considered a key priority for prevention of CVD in China [13, 14, 22]. Previous reports have suggested that many individuals diagnosed with diabetes in China are not adequately managed, particularly in rural areas, thereby increasing the risk of premature death [23]. The findings of the current study demonstrate that these international recommendations have not yet been translated into daily clinical practice in China, with fewer than 1 in 15 patients with T2D and established CVD receiving a GLA with proven CV risk reduction, while this figure is lower than the 1 in 5 adults in the multinational study sample [15]. However, it should be remembered that these GLAs with demonstrated CV risk reduction were either not licensed with a CV indication or even not reimbursed for a diabetes indication in China in 2019, and were therefore less accessible when these data were collected.
Approximately one-third of the China study sample (32.3%) was receiving CV medications (55.3% in the CVD subgroup and 20.5% in the non-CVD subgroup). The proportions of patients receiving CV medications in the China study sample are lower than those reported for the multinational study population (China study sample: 32.3% overall, with 55.3%, 55.3% and 20.5% in the CVD, ASCVD and non-CVD subgroups, respectively, compared with 76.0% in the overall pooled CAPTURE study sample) [15]. The most frequently used medications in the China study sample were statins and acetylsalicylic acid. Data from this study showed that there was less use of guideline-directed agents (e.g., statins, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers and platelet-aggregation inhibitors) in patients with T2D and CVD in China compared with the multinational population (excluding China). This indicates that there may be an unmet need for optimal management of this sub-population in China.
The current study has several strengths, including the enrollment of consecutive patients at routine clinical visits. The study was cross-sectional and multinational, using a standardized methodology to collect CVD prevalence data facilitating comparative analysis. With the formal approval of a CV indication for GLAs with demonstrated CV risk reductions in China, this study will serve as a useful reference point for those wishing to monitor the use of these GLAs.
Limitations of this study include that the selected sites and the small sample size may not be fully representative of the target population of China and thus may not reflect the specific prevalence of CVD in Chinese adults with T2D. Additionally, this was a non-interventional study and did not require adjudication for the presence of complications, and therefore there is a possibility that CVD was underdiagnosed or misdiagnosed. Furthermore, the study was descriptive in design and thus no statistical comparisons were completed. The low prevalence of heart failure reported in the China study population may have resulted from selection bias. For example, it is possible that patients with both T2D and heart failure in China are more likely to visit a cardiologist than an endocrinologist compared with patients in other countries (where cardiologists also participated in the study) and therefore would not have been included in the CAPTURE study.
Conclusions
This study, which to our knowledge represents the first contemporary data on CVD prevalence in patients with T2D in China, shows that one-third of patients with T2D in China have established CVD, but this may be limited to the type of sites selected to participate in the CAPTURE study. The CVD burden is largely accounted for by ASCVD, with the leading causes being stable coronary artery disease, carotid artery disease and stroke. Usage of GLAs with proven CV benefits has been found to be low in Chinese diabetology practice compared with the pooled multinational analysis in the CAPTURE study, suggesting an unmet need for optimal management in this group.
References
Zhao D, Liu J, Wang M, Zhang X, Zhou M. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol. 2019;16:203–12.
Rao Kondapally Seshasai S, Kaptoge S, Thompson A, et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med. 2011;364:829–41.
Sarwar N, Gao P, Seshasai SR, et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375:2215–22.
Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997.
Xu Y, Wang L, He J, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310:948–59.
International Diabetes Federation. IDF Diabetes Atlas. 9th ed. In: International Diabetes Federation, ed. Brussels, Belgium: International Diabetes Federation. 2019
Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc Diabetol. 2018;17:83.
American Diabetes Association. 10. Cardiovascular disease and risk management: standards of medical care in diabetes-2020. Diabetes Care. 2020;43:S111-S34.
Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2019;140:e596–646.
Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41:255–323.
Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375:311–22.
Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373:2117–28.
Chinese Diabetes Society and Chinese Society of Endocrinology of Chinese Medical Association. Expert consensus on glucose-lowering pharmacotherapies in Chinese adults with type 2 diabetes and cardiovascular disease or chronic kidney disease [Chinese]. Chin J Diabetes Mellitus. 2020;12:369–81.
Hong T, Su Q, Li X, et al. Glucose-lowering pharmacotherapies in Chinese adults with type 2 diabetes and cardiovascular disease or chronic kidney disease. An expert consensus reported by the Chinese Diabetes Society and the Chinese Society of Endocrinology. Diabetes Metab Res Rev. 2020;37:e3416.
Mosenzon O, Alguwaihes A, Leon JLA, et al. CAPTURE: a multinational, cross-sectional study of cardiovascular disease prevalence in adults with type 2 diabetes across 13 countries. Cardiovasc Diabetol. 2021;20:154.
World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–4.
International Society for Pharmacoepidemiology (ISPE). Guidelines for Good Pharmacoepidemiology Practices (GPP). 2015. Available from URL: https://www.pharmacoepi.org/resources/policies/guidelines-08027/. Accessed 23-Sept-2020.
Liu Z, Fu C, Wang W, Xu B. Prevalence of chronic complications of type 2 diabetes mellitus in outpatients—a cross-sectional hospital based survey in urban China. Health Qual Life Outcomes. 2010;8:62.
Sone H, Tanaka S, Tanaka S, et al. Serum level of triglycerides is a potent risk factor comparable to LDL cholesterol for coronary heart disease in Japanese patients with type 2 diabetes: subanalysis of the Japan Diabetes Complications Study (JDCS). J Clin Endocrinol Metab. 2011;96:3448–56.
Lyu Y, Luo Y, Li C, et al. Regional differences in the prevalence of coronary heart disease and stroke in patients with type 2 diabetes in China. J Clin Endocrinol Metab. 2018;103:3319–30.
Zhang X, Mu Y, Yan W, Ba J, Li H. Prevalence of stroke and metabolic disorders in the middle-aged and elderly Chinese with type 2 diabetes. Chin Med J (Engl). 2014;127:3537–42.
Task Force on Chinese Guidelines for the Prevention of Cardiovascular Diseases (2017); Editorial Board of Chinese Journal of Cardiology. Chinese guidelines for the prevention of cardiovascular diseases (2017) [Chinese]. Zhonghua Xin Xue Guan Bing Za Zhi. 2018;46:10-25
Bragg F, Holmes MV, Iona A, et al. Association between diabetes and cause-specific mortality in rural and urban areas of China. JAMA. 2017;317:280–9.
Acknowledgements
The primary CAPTURE study reporting the CVD prevalence in adults with T2D across 13 countries has been previously published (Mosenzon et al. Cardiovasc Diabetol. 2021;20:154. https://doi.org/10.1186/s12933-021-01344-0). The authors would like to thank the CAPTURE study participants, investigators and coordinators. The authors would also like to thank Ke Cao, who worked for Novo Nordisk at the time of the manuscript development, and Wenyan Liu, a Novo Nordisk employee, for reviewing the manuscript. Medical writing support was provided by Gillian Groeger, PhD, of Ashfield MedComms, an Ashfield Health company, funded by Novo Nordisk A/S.
Funding
The funding source (Novo Nordisk A/S) of the CAPTURE study participated in the study design, site selection (in collaboration with a contract research organization), study coordination, data management, data analysis (including the country-level data analysis) and study report preparation. The Rapid Service fee was also paid for by Novo Nordisk A/S.
Prior Publication
Part of the data in the current manuscript has been presented as a poster at the 31st Great Wall International Congress of Cardiology, 19–25 Oct 2021, virtual congress.
Authorship
All authors contributed to critically reviewing and editing the manuscript drafts. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship in this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Tianpei Hong, Zongxun Yan, Li Li, Wei Tang, Lin Qi, Jianhua Ye, Jiangong Ren, Qin Wan and Wenhua Xiao were investigators in the study and collected study data. Tianpei Hong contributed to the data interpretation.
Disclosures
Tianpei Hong declares speaker’s bureau honoraria and advisory board membership from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Serono, Merck Sharp & Dohme, Novartis, Novo Nordisk and Sanofi. Di Zhao works for Novo Nordisk China Pharmaceutical Co. Ltd as a medical advisor. Zongxun Yan, Li Li, Wei Tang, Lin Qi, Jianhua Ye, Jiangong Ren, Qin Wan and Wenhua Xiao have no competing interests to declare.
Compliance with Ethics Guidelines
Approval of the protocol by the Ethics Committee of Peking University Third Hospital and other relevant Independent Ethics Committee/appropriate body (ESM Table 1) was provided by each investigator prior to undertaking any study-related activities (study-related activities are any procedures related to recording of data according to protocol). Informed consent was recorded from each patient on their first study visit, but prior to undertaking any study-related activities. The registration number and approval date of registry of the studies are NCT03786406 (26 December 2018) and NCT03811288 (22 January 2019). The studies were conducted in accordance with the Declaration of Helsinki, Guidelines for Good Pharmacoepidemiology Practices issued by International Society for Pharmacoepidemiology and Chinese regulations for clinical research.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Hong, T., Yan, Z., Li, L. et al. The Prevalence of Cardiovascular Disease in Adults with Type 2 Diabetes in China: Results from the Cross-Sectional CAPTURE Study. Diabetes Ther 13, 969–981 (2022). https://doi.org/10.1007/s13300-022-01243-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-022-01243-x